
Abstract
Background:
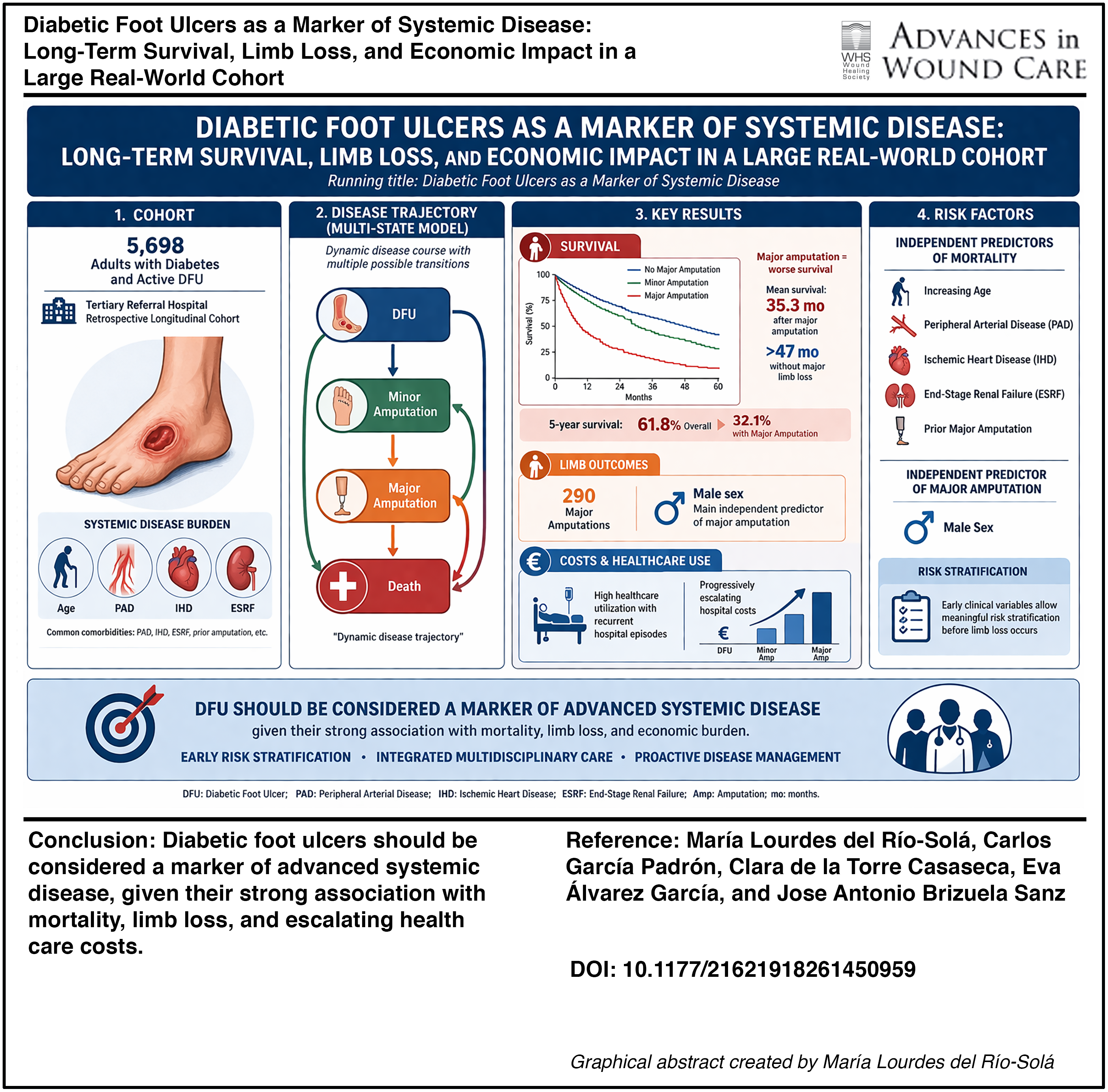
Diabetic foot ulcers (DFUs) represent one of the most severe complications of diabetes mellitus and are associated with limb loss, excess mortality, and substantial health care costs. Although DFUs are often approached as a localized wound condition, increasing evidence suggests that they reflect advanced systemic vascular and metabolic disease. However, large real-world longitudinal studies integrating wound outcomes, survival, and economic burden remain scarce.
Objectives:
The objective of this study is to evaluate long-term clinical outcomes, survival, and health care costs associated with DFUs in a large real-world cohort and to identify factors independently associated with mortality and limb loss.
Methods:
We conducted a retrospective longitudinal cohort study including 5,698 adult patients with diabetes treated for active DFUs at a tertiary referral hospital. Minor and major amputations, survival outcomes, health care utilization, and estimated direct hospital costs were analyzed. Time-to-event analyses included Kaplan–Meier estimation, competing-risk regression, and multivariable Cox proportional hazards models. Disease trajectories were further explored using multistate modeling.
Results:
During follow-up, 290 major amputations were recorded. Patients undergoing major amputation showed significantly worse survival compared with nonamputated patients or those with minor amputations (log-rank p < 0.001). Mean survival after major amputation was 35.3 months, compared with more than 47 months in patients without major limb loss. Five-year overall survival was 61.8%, decreasing to 32.1% among patients with major amputation. Increasing age, peripheral arterial disease, ischemic heart disease, end-stage renal failure, and prior major amputation were independently associated with mortality. Male sex emerged as the main independent predictor of major amputation in adjusted competing-risk models. DFU-related care was associated with high health care utilization and progressively escalating hospital costs.
Conclusions:
DFUs should be regarded as a marker of advanced systemic disease rather than an isolated wound condition, given their strong association with long-term mortality, limb loss, and economic burden. Early risk stratification and integrated multidisciplinary care strategies are essential to improve outcomes in this high-risk population.
Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.