
Abstract
Objectives:
Endogenous bioelectric signaling (including transepidermal potential [TEP] and the current of injury) plays a fundamental role in normal wound repair. Despite this, commonly used wound management frameworks do not consider this important driver of healing. The objectives of this review are to explore whether the patient characteristics/pathologies common in delayed healing are associated with weakened electrical properties of the skin and to consider whether compromised currents of injury are a barrier to healing that could be addressed with electrical stimulation therapy (EST) and incorporated into existing frameworks.
Approach:
This systematic review of PubMed was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and aimed to explore the impact of three characteristics associated with delayed healing (older age, diabetes, and chronic inflammation) on the electrical properties of skin/wounds.
Results:
Twelve relevant studies were identified, revealing that TEP in older or diabetic people is significantly lower, and the current of injury is approximately half that of young, healthy controls.
Innovation:
Lower currents of injury are associated with slower wound healing; therefore, the reduced current of injury/TEP identified here can be considered a barrier to healing. EST is designed to boost the weakened current of injury, back up to normal levels, stimulating a healing response. The incorporation of EST into existing wound management frameworks is therefore proposed.
Conclusion:
Endogenous bioelectrical signaling in the wound healing process appears to be compromised particularly in older people and those with diabetes. Patients may benefit from incorporating treatment with EST, which boosts bioelectrical signaling, into relevant wound treatment frameworks.
Jenny Smith, BSc, PhD
INTRODUCTION
The wound healing process is traditionally viewed as a complex interplay of cellular signaling mediated via a cocktail of growth factors, hormones, and cytokines released at the wound. 1 However, one fundamental aspect of the wound healing process, the role of bioelectrical signaling, is seldom mentioned when describing the physiology of wound healing or the pathophysiology of hard-to-heal wounds and is under-acknowledged in clinical practice.
Although bioelectric signaling is most commonly associated with excitable cells (neurons and muscle cells), in fact, all living cells generate and respond to bioelectricity through their ability to move charged particles (including ions and molecular ions) across cell membranes, thus generating electrical potential. Bioelectricity is necessary on a cellular level to regulate a wide range of fundamental cell-level behaviors, in all organ systems, including the skin. 2 Bioelectricity also coordinates how cells work together within organ systems. 3 In the human skin, not only do the resident cells generate and respond to bioelectricity but the epidermis itself generates an electrical potential as a result of the selected and directional transport of positively charged particles (e.g., Na+ ions) from the apical (outermost) side of the epidermis to the basolateral (innermost) side (Fig. 1A).1,4,5 This transepidermal potential (TEP), also referred to as the skin battery, in human skin, ranges between 15 and 60 mV1,6 (Table 1), with the innermost side of the epidermis being positive relative to the outside. This potential difference is found across other epithelial layers and can be referred to generically as the transepidermal potential (TEP). Tight junctions between the epithelial cells (keratinocytes in the epidermis) form a barrier for most particles, including those that carry an electrical charge, and prevent these charged ions and molecules from diffusing freely between the apical and basal sides. In this way a gradient of electrical charge, carried by concentrated positively charged particles, is maintained at the base of the epidermis in a manner which is dependent on the integrity of the tight junctions and the broader epidermal barrier (Fig. 1). 7 Indirect, experimental ways of measuring TEP include the assessment of skin barrier integrity by measuring transepidermal electrical resistance (TEER) and the detection of “leaked” electrically active molecules on the skin surface through the skin barrier by measuring skin surface electrical activity (Table 1).
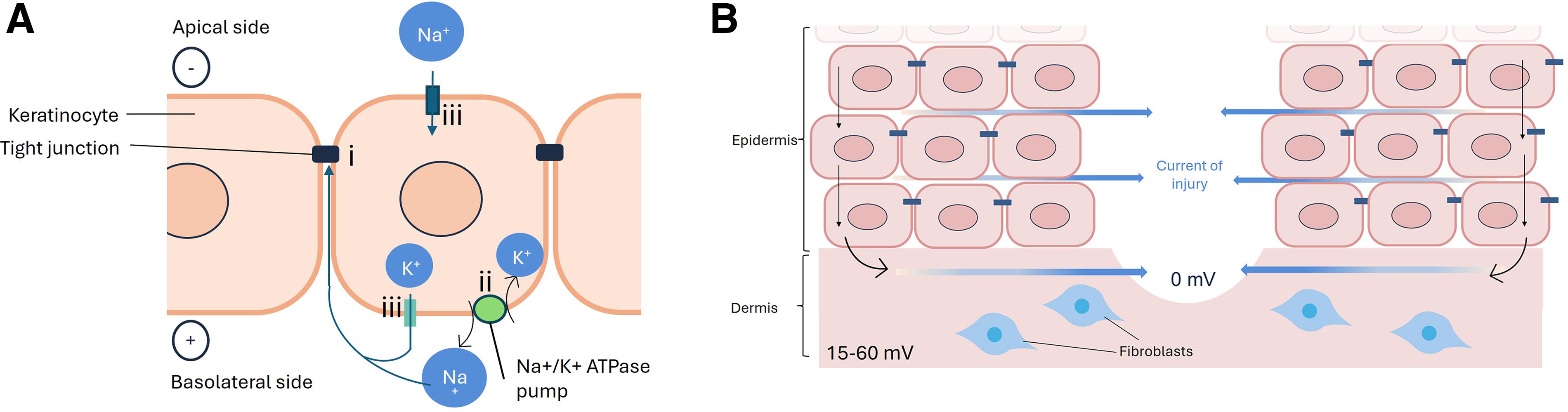
Mechanism of development of the transdermal potential
Methods used to measure and monitor electrical activity in intact skin and relevant in vitro models
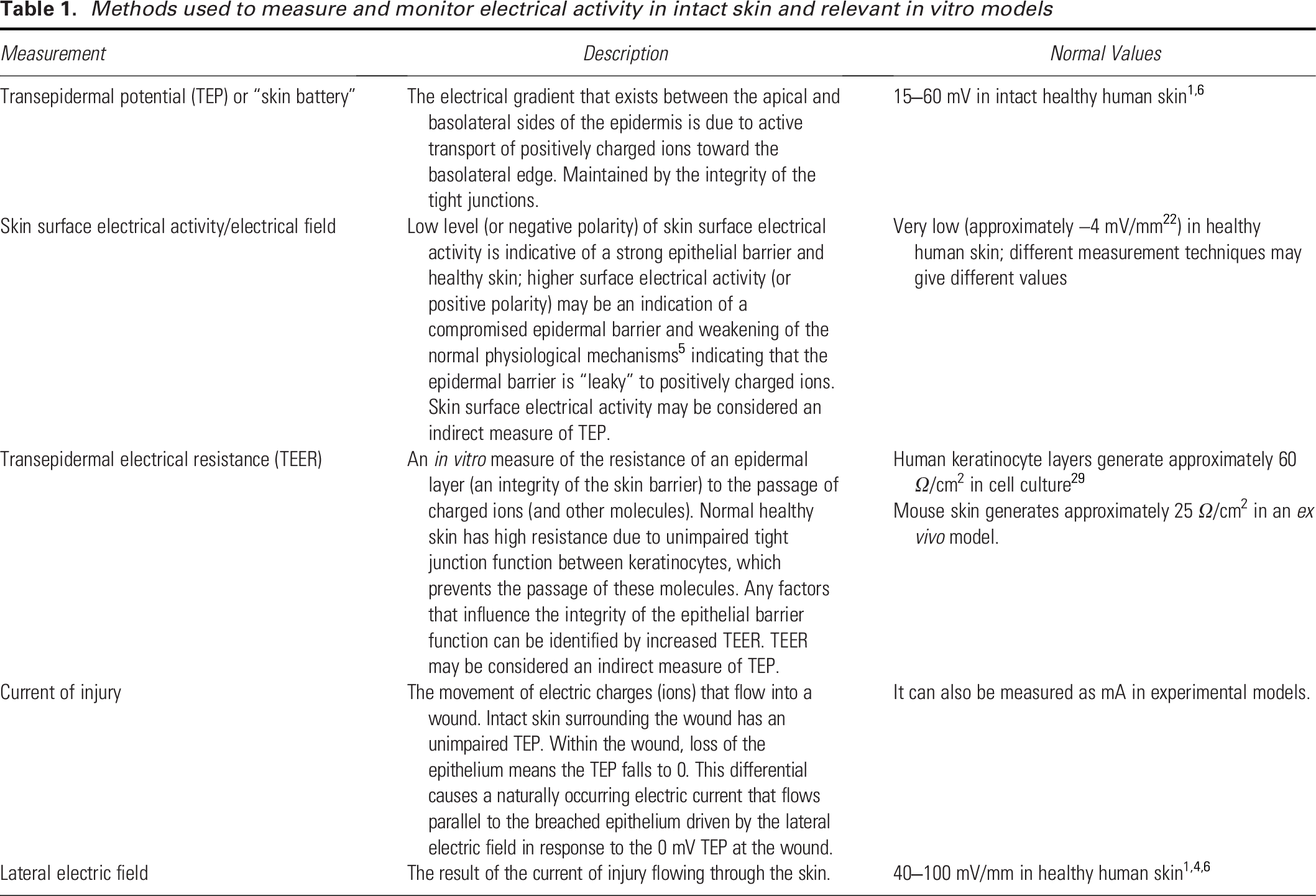
When the skin is wounded, there is an immediate collapse of the TEP in the wound bed caused by the complete loss of resistance resulting from the break in the epidermis. 8 In adjacent unwounded areas, ion transport mechanisms remain intact and positively charged ions continue to be actively transported toward the basolateral side of the epidermis, where they then flow toward the wound bed driven by the lateral electric field beneath the epidermis. This flow of positively charged ions is referred to as the current of injury (blue arrows Fig. 1B, Table 1, measured in micro-Amps), which generates a lateral electric field (which can be measured in mV/mm).1,4,6 This wound-related electric field stimulates many cellular processes, including cell proliferation, directional migration, and differentiation, and therefore is an important driver of healing.1,4 These cellular processes are stimulated in cells of the epidermis (e.g., keratinocytes that proliferate and migrate to close the wound) and the dermis (e.g., fibroblasts that proliferate, migrate, start to produce, and remodel collagen to repair the defect). In normal acute wound healing, the TEP is gradually restored over several days as re-epithelialization takes place and the new epithelium matures to form a continuous and differentiated layer.6,9,10 Experimental studies, which artificially alter the TEP, for example, by pharmacological blockade, or stimulation of ion channels or ion transport, have shown a strong and linear correlation between the magnitude of the wound electric current and the rate of wound healing.11–13 This raises the hypothesis that other, endogenous, nonpharmacological deficiencies in bioelectric signaling in the skin, for example, those caused by the pathogenic or age-related changes to skin physiology observed in people with hard-to-heal wounds, may also be associated with a deficient healing process.
CLINICAL PROBLEM ADDRESSED
Hard-to-heal wounds are increasingly prevalent and their management presents a large and growing socioeconomic burden globally. 14 Although many advanced wound management techniques, dressings, and devices can be deployed to improve the rate of healing, hard-to-heal wounds remain a major challenge to health care systems. Effective wound management is based on a combination of accurate diagnosis, treatment of the underlying cause, as well as treatment decisions relating to the wound itself, the latter often being guided by well-known frameworks, such as the TIME paradigm 15 first published in 2004 and updated in 2019 to TIMERS. 16 This framework postulates that if all barriers to healing (including tissue viability [T], infection/inflammation [I], appropriate levels of moisture [M], wound edge [E], regeneration [R], and social factors [S]) are overcome, then the wound should progress toward healing. However, around half of chronic wounds fail to heal within 1 year of treatment, leading to spiraling costs to health care systems and prolonged suffering for patients. 17
Clearly, further efforts are needed to reduce the burden of these wounds. This article proposes that one candidate for further investigation is the bioelectrical signaling associated with healing. An extensive body of scientific evidence loosely supports a hypothesis that deficient electric fields and dampened endogenous bioelectric signaling in patients at risk of delayed healing may contribute to compromised healing.4,18 The importance of bioelectric signals in normal wound healing is very well described; however, the role of bioelectricity in the deficient healing associated with hard-to-heal, or chronic, wounds, is less well understood. Furthermore, a clinically effective technology, specifically targeted to bioelectric wound signaling exists already, namely electrical stimulation therapy (EST). EST is one of the most highly evidenced advanced treatments in wound management that has been shown to have a consistently stimulatory effect on wound healing.19,20 EST is designed to boost the endogenous bioelectricity in patients with hard-to-heal wounds, with the aim of stimulating the healing process. However, although this technology is known to be effective, reflected in the high level of supporting evidence, the scientific rationale and clinical context for using it have not been well articulated—specifically, the extent to which deficient bioelectrical signaling may contribute toward wound chronicity or failure to heal has not been robustly explored. Also lacking are the inclusion of bioelectricity and its impact on healing in any widely used treatment protocols or frameworks. A clinical summary is provided in Box 1.
Box 1. Clinical Summary
What is the current of injury?
A flow of positively charged ions that flows from the edge of a wound into the center. The current of injury is strongest at the wound and gets weaker further away from the wound edge. The lateral electric field which drives the current of injury, is an essential part of the normal healing process and influences the behavior of cells in the epidermis (e.g., keratinocytes) and dermis (e.g., fibroblasts), promoting proliferation, directional migration (in the direction of the current toward the center of the wound, and differentiation.
Why does it matter in chronic wounds?
The magnitude of the current of injury has been shown to correlate with the speed of healing. Several studies have suggested that people with certain pathological states associated with failure to heal (e.g., diabetes, advanced age), also have a reduced current of injury, and that this might be one of the reasons why at-risk wounds heal more slowly in some people.
How can a deficient current of injury be corrected?
Electrical stimulation therapy (EST) is a well-evidenced and commercially available technology. It works by delivering small amounts of electrical current to the wound and peri-wound area, to boost the healing process, thus speeding up the rate of healing. EST also has a beneficial effect on wound-related pain.
When to consider EST?
EST may be a useful adjunct to existing standard care in patients whose wounds are 4 weeks or older, and are not responding well to standard care alone, showing either a stalled or deteriorating wound. If wound-related pain is a factor, then the use of EST is a nonpharmacological means to help reduce the pain.
Key takeaways from the evidence
Over 40 randomized controlled trials have been reviewed in 13 meta-analyses (Supplementary Table S3). EST compared with no EST is associated with several clinical benefits, including greater likelihood of healing, faster rate of wound size reduction, reduced wound-related pain, reduced nurse visits, reduced dressings, and overall reduced costs.
The primary objective of this systematic review is to explore the hypothesis that hard-to-heal wounds may have deficient or compromised skin battery and/or current of injury and that this may be considered a legitimate barrier to healing. A secondary aim is to consider whether it is feasible to incorporate bioelectricity and EST into an existing wound management framework, specifically the TIMERS paradigm. 16
MATERIALS AND METHODS
A systematic review of the literature was conducted on October 3, 2024, using PubMed in line with the PRISMA guidelines. 21 The review was not registered. For search terms and population, intervention, comparator, outcomes, and study type (PICOS) criteria, refer to Supplementary Tables S1 and S2. Briefly, three parallel searches were conducted all using the following terms: ((skin[Title/Abstract] OR dermal[Title/Abstract] OR cornea[Title/Abstract]) AND (“current of injury”[Title/Abstract] OR “electric field”[Title/Abstract] OR “electric potential”[Title/Abstract] OR “electric activity”[Title/Abstract] OR “electrical activity”[Title/Abstract] OR “electric signals”[Title/Abstract] OR “electrical potential”[Title/Abstract])) plus additional terms to identify papers relating to diabetes (AND [“diabetes”]), older age (AND [“age” OR “older” OR “elderly” OR “younger” OR “middle-aged”]) or inflammation (AND [inflamm*]). Bibliographies of highly relevant papers were reviewed for further relevant papers. Further ad hoc searches (Google, Google Scholar, and Elicit.com) were also conducted to identify any additional relevant information.
Hits were manually reviewed by one reviewer with experience in extracting data for systematic reviews, according to the inclusion/exclusion criteria (defined by the PICOS system). Papers with the following characteristics were removed: duplicates, papers describing tissues other than skin/cornea/retina, papers containing no primary data, papers that tested electrical devices or techniques (as opposed to measuring endogenous bioactivity), and papers with no relevant context to the research question under review. All included studies were progressed to the data extraction phase. A simple, predefined, structured data collection spreadsheet (Microsoft Excel) was used to obtain information from the full text of each included paper. No assessment of the quality or bias of included studies was carried out. Given that the majority of the identified data were experimental (in vitro, in vivo) and using a wide range of models and methods, with very little clinical research expected to be identified, it was determined that analysis of study bias and quality, which are largely defined by clinical study methodologies, were not relevant. No statistical analysis or data synthesis was possible given the highly variable nature of the data captured.
RESULTS
A total of 175 papers were identified, of which 168 were excluded, leaving 7 eligible for inclusion in this systematic review. This list was supplemented by an additional 5 papers identified from other sources (typically from the bibliography of the included papers or from additional ad hoc searches, Fig. 2). Included papers are listed in Table 2.
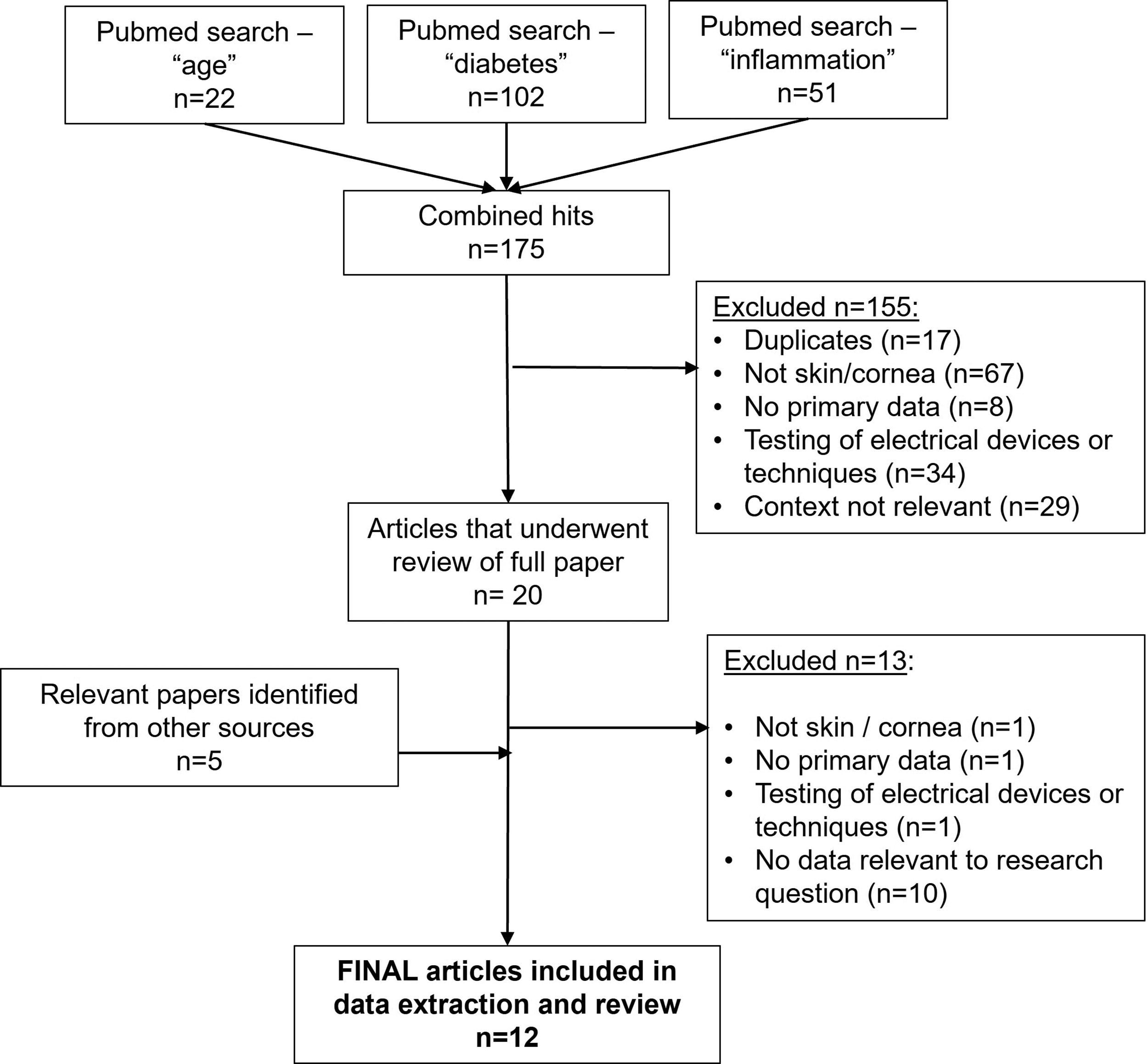
Systematic review flow chart.
Impact of older age, diabetes, and inflammation on electrical properties of the epidermis and other relevant epithelial layers
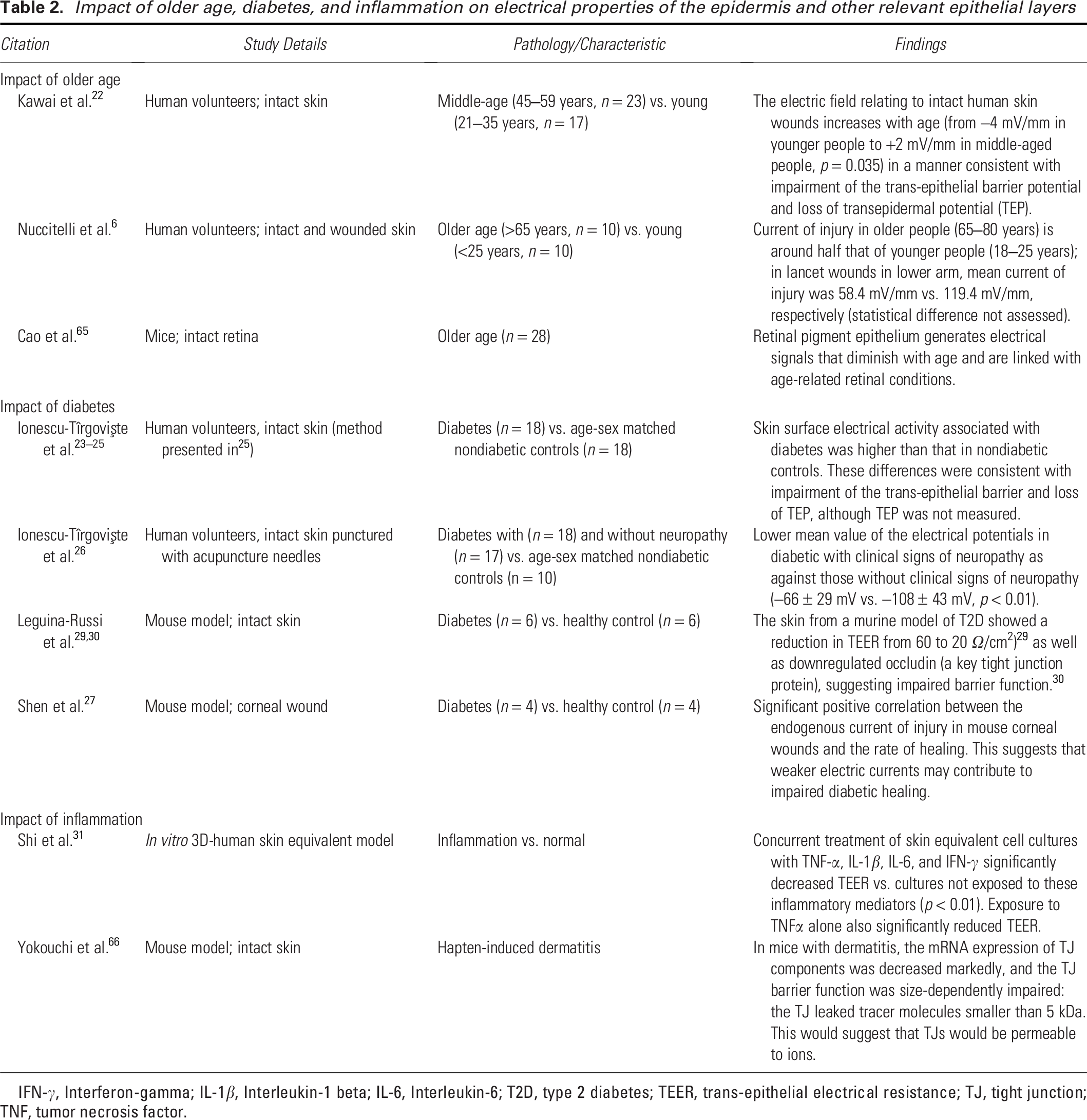
IFN-γ, Interferon-gamma; IL-1β, Interleukin-1 beta; IL-6, Interleukin-6; T2D, type 2 diabetes; TEER, trans-epithelial electrical resistance; TJ, tight junction; TNF, tumor necrosis factor.
The TEP/current of injury is compromised in older people or those with chronic conditions
Several scientific studies that either directly or indirectly report the status of the TEP or current of injury/lateral wound electric field have found anomalies in these phenomena in scenarios associated with delayed healing, including in older individuals (vs. younger), in diabetic individuals (vs. nondiabetic), and in the presence of chronic inflammation, all of which are discussed below.
The impact of aging on bioelectric signaling of the skin and wounds
Several studies have explored the impact of older age on skin bioelectricity (Table 2). Kawai et al. measured the skin surface electrical activity on intact skin in young (aged 21–35 years, n = 17) or middle-aged (aged 45–59 years, n = 23) volunteers. 22 They found that while young people showed the negative surface bioelectrical activity expected with healthy intact skin (measured at around −4 mV), the electrical activity in older people was statistically significantly higher, with a positive polarity at the skin surface (around 2 mV, p = 0.035). This positive polarity may be an indication of a compromised epidermal barrier and weakening of the normal physiological mechanisms, indicating that the epidermal barrier is “leaky” to positively charged particles (Table 1). They postulated that the changes observed in older skin could be due to a decline in the gradient of charged ions across the epidermis, which drives the generation of the TEP. 22
Using different methods, Nuccitelli et al. also explored the role of aging by comparing the intact skin of older people (aged 65–80 years, n = 10) with younger people (aged 18–25 years, n = 10). 6 This study confirmed that in unwounded skin, older people have a slightly higher skin surface electrical field than younger people (mean 41 vs. 21 mV/mm). This finding is again suggestive of an impaired transdermal barrier in older people, potentially failing to maintain a concentration of positively charged particles at the basolateral side of the epidermis. Following wounding, a surface lateral electric field, typically 100–200 mV more negative than adjacent intact skin, driven by the current of injury, was observable in both groups. However, the magnitude of this electric field was significantly lower in older people than in younger people (mean for all skin wounds of 65 mV/mm vs. 131 mm/mV, respectively). 6 This represented an approximate halving of the strength of the wound-related electrical field in older people, the population in whom nonhealing wounds are most concentrated, compared with younger people in whom nonhealing wounds are less prevalent. No differences were observed relating to the wound field in different body locations (lower limb vs. lower arm) or in males versus females. 6
These data suggest that TEP (skin battery) decreases with age, leading to increased electrical activity being measurable on the intact skin surface, and a smaller differential (electrical potential) between the apical and basolateral surfaces of the epidermis. The consequence of these changes observed in older people is that when a wound is incurred, this smaller TEP is only capable of driving a weaker current of injury, and consequently a weaker wound-related electrical field, resulting in a diminished cellular response to healing.
The impact of diabetes on bioelectric signaling of the skin and wounds
Research has shown impairments of skin bioelectricity in people and animal models with diabetes (Table 2). A series of studies have demonstrated that the surface electrical signals from intact skin are higher and “strongly different” in people with diabetes compared with healthy individuals.23–25 Detection of increased electrical activity on the surface of the skin in this context23–25 suggests reduced efficacy of the epidermal barrier, suggesting a lower TEP—a less powerful skin battery. This has been confirmed in a study comparing people with diabetes against age- and sex-matched healthy controls 26 in which TEP was lower in people with diabetes than people without diabetes (n = 18 in each group). In this study, the presence of neuropathy was associated with a further lowering of the TEP compared with diabetes with no neuropathy (p < 0.01). 26 This finding is consistent with the findings in older people described in the previous section.
No studies have been conducted to explore the current of injury or electric fields in wounded human diabetic skin, or diabetic foot ulcers, compared with healthy individuals, and this remains a major gap in the evidence base. However, in a model often used to represent skin, Shen et al. evaluated the corneal current of injury in three different mouse models of diabetes compared with age-matched, normal mice (n = 4 in each group). In this study, the current of injury was shown to be significantly lower in diabetic cornea compared with normal, peaking at 1.6 versus 3 µA/cm2, respectively. In all three mouse models of diabetes reported in this paper, the magnitude of the current of injury at the point of wounding was approximately half that of healthy controls. Whereas the current of injury in normal mice plateaued throughout the duration of the study (maximum of 300 mins evaluation period) the current of injury dissipated more rapidly in diabetic wounds. 27 This meant that the current of injury in diabetic mice became up to 5-times smaller compared with healthy mice over a relatively short-time frame of 5 h postwounding. This study also found that diabetic mice had a consistently reduced current of injury regardless of the level of glucose present, suggesting that the alteration of current of injury was not dependent on hyperglycemia but more likely to be due to a longer-term or systemic consequence of diabetes. The current of injury correlated significantly with the rate of healing; the higher the current of injury, the faster the rate of healing. The authors suggested several potential causes of the reduced current of injury in diabetes, including compromise of the epithelial tight junctions, downregulation of the ion channels and pumps responsible for generating the transepithelial potential, or abnormal cellular metabolism. Some support exists for some of these hypotheses. Several studies have shown that diabetic skin has lower levels of tight junction proteins than healthy skin.28–30 Studies in mouse models of diabetes (n = 6 in each group) have shown that the epidermal tight junction proteins zona occludens-1, occludin, and E-cadherin were all significantly downregulated compared with normal skin and that this was associated with a decreased skin barrier function.28–30 To date, this observation has not been directly associated with delayed healing. Studies in mouse models have also reported reduced TEER in the skin of diabetic mice compared with healthy controls.29,30 Whether these observations are directly or indirectly linked with the pathology of diabetes is unknown, and further research is required to explore these points.
The impact of inflammation on bioelectric signaling of the skin and wounds
The inflammatory phase is essential to the early wound healing process; however, chronic inflammation is associated with failure to heal. No direct evidence (direct measurement of TEP or current of injury) of the impact of chronic inflammation on the electrical activity of the skin was identified, and indirect evidence is limited to the impact of inflammation on the epidermal barrier measured by TEER (Table 2). It is known that the electrical resistance of the skin is lower in inflammatory situations. 31 Tumor necrosis factor-alpha and other inflammatory cytokines cause a reduction in TEER in a human skin equivalent cell culture model, consistent with a compromised skin barrier. 31 Studies have also shown that epidermal tight junction barrier function is altered by skin inflammation. These findings could be hypothesized to lead to impairment of the bioelectricity of inflamed skin (TEP) or current of injury when wounded. Although this remains to be robustly explored in inflammatory skin disease, inflammation in other epithelia, such as intestinal epithelium affected by inflammatory bowel disease,32,33 or lung epithelia affected by asthma, 34 is already known to be associated with impaired epithelial barrier function, reduced TEER, altered transepithelial ion transport, and reduced transepithelial potential.
DISCUSSION
This systematic review identified a body of evidence that taken together, suggest that scenarios associated with delayed healing, including older age, diabetes, and possibly chronic inflammation, all suffer from deficiencies in skin bioelectrical function, and most importantly, reduced current of injury. Boosting the deficient current of injury can be achieved through the use of EST, which is known to promote healing outcomes (Supplementary Table S3). This information should be considered for incorporation into treatment frameworks and educational material related to wound management.
The case for including compromised bioelectricity into the TIMERS framework
If compromised bioelectricity in the human skin in certain scenarios (e.g., older age, diabetes) is indeed a barrier to healing, and if a technology to address this barrier is available, then it may be logical to include it in the TIMERS framework. 16 Unless all barriers to healing are addressed, a chronic wound will not progress toward healing, and by ignoring the role of bioelectricity in healing, this barrier to healing may remain systematically unaddressed.
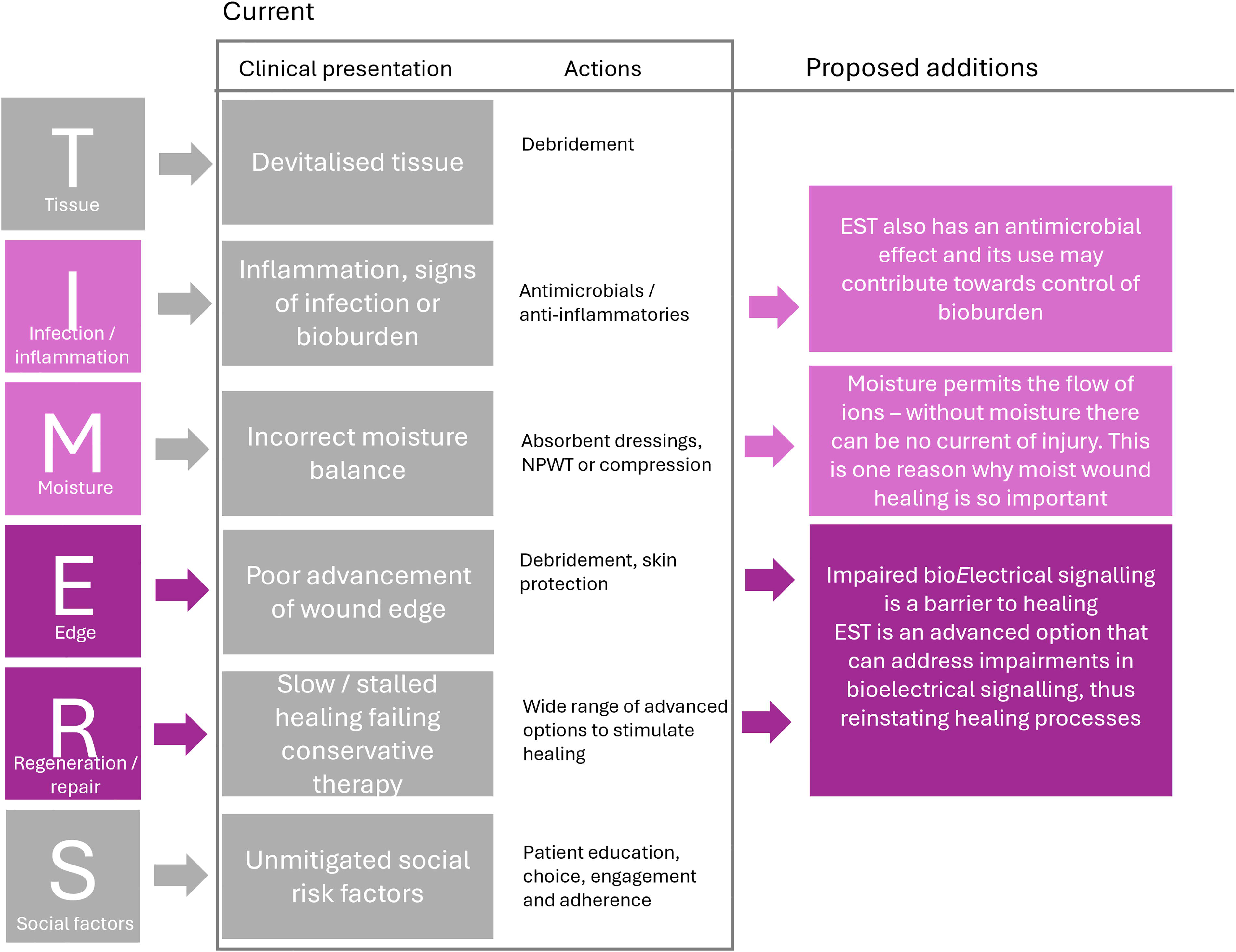
Wound management today is predominantly allopathic; this is exemplified by the TIMERS framework, which is a useful and widely recognized framework focused on management of specific, important barriers to healing and ways of overcoming those barriers (Fig. 4). Assuming that systemic issues have been addressed, the TIMERS framework alone, as currently defined, is clearly not enough to fully address or correct the pathology of a hard-to-heal wound—if this was the case then there would be no nonhealing wounds in any good quality care system. It may be that some fundamental elements necessary to the healing process have been overlooked in previous iterations.
Many commentators have stated that the endogenous current of injury is an important component of wound healing that has been largely ignored in the main narratives/education around the wound healing process. Given that the evidence points toward there being an impairment of the endogenous current of injury in people with diabetes and older age, and possibly in inflammation, it may be reasonable to position impaired bioelectricity as an additional “barrier to healing” that should be incorporated into the existing TIMERS framework.
Figure 3 proposes that the E in TIMERS could be adapted to include “[bio]Electricity” given the importance of the current of injury in migration/proliferative events that drive healing from the “edge” of the wound. In the past, there has been much difficulty in properly describing and communicating the “E” in the TIMERS acronym, with many of the actions listed under “E” could reasonably be included within other existing categories.
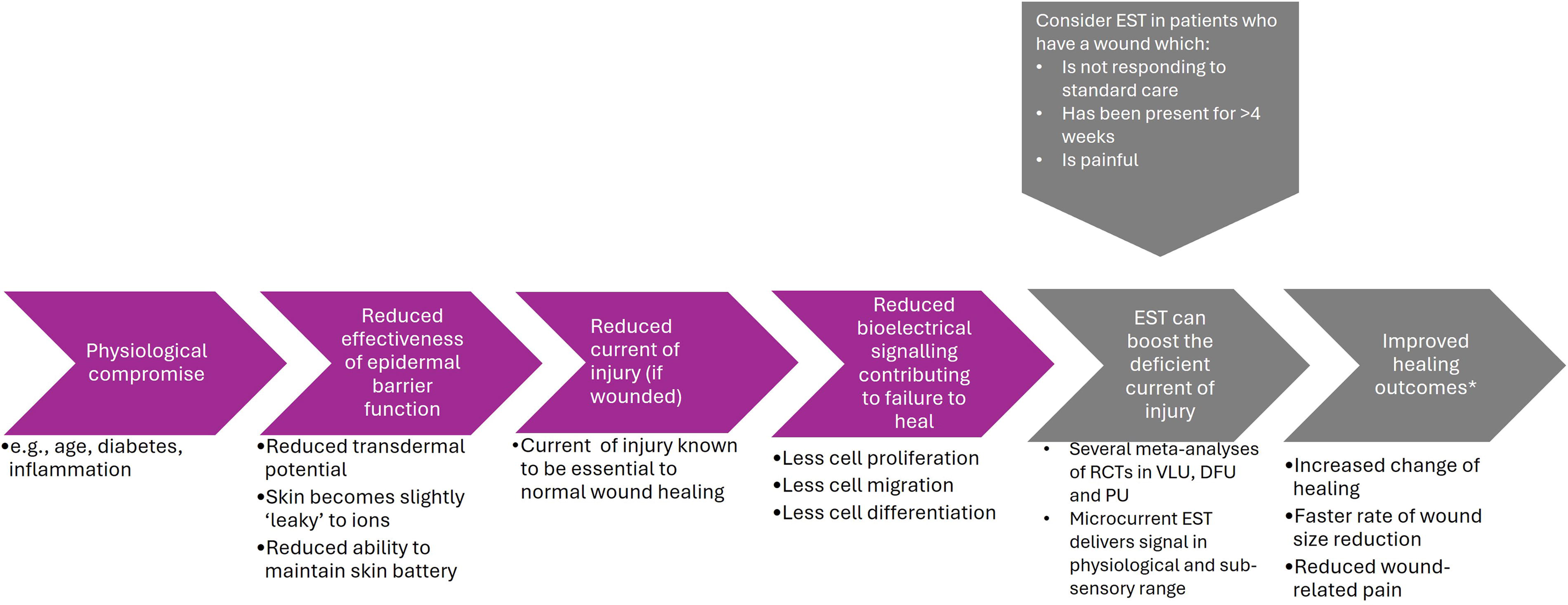
Innovation and clinical context. Although evidence supporting has been published, the innovation of this article is the rigorous collation of the information supporting the statements highlighted in purple, and its inclusion into a clinically relevant context. *Details of outcomes in response to EST are described in a series of meta-analyses, as shown in Supplementary Table S3. DFU, diabetic foot ulcer; EST, electrical stimulation therapy; PU, pressure ulcer; VLU, venous leg ulcer.
The link between moist wound healing and bioelectricity is clear. Preventing the wound from drying out permits the continued flow of ions around the wound bed, which is the fundamental driver of bioelectricty. 35 It has been shown that the current of injury is sustained by occlusive dressings. 36 In fact, this goes some way to explain the clinical benefit of moist wound healing; however, people with an impaired current of injury may still struggle to achieve healing. Incorporating this information into the TIMERS framework may also provide important context to explain why moist wound healing is such a fundamental enabler of the healing process (Fig. 4).
Proposal to define deficiencies in bioelectricity as a barrier to healing and to incorporate it into the TIMERS paradigm. 16 Pink boxes illustrate where new information may be incorporated. Recognition of compromised bioelectricity in hard-to-heal wounds may be incorporated within the “E” (currently representing wound edge). Recognition of the incorporation of EST as a treatment option could be incorporated not only to the “E” but also to the “R” (regeneration), as EST is a technology shown to promote healing. The impact of EST on microbes should be described within the “I” section of the TIMERS acronym. The ability of a moist wound environment, but not a dry wound environment, to support the current of injury (via the flow of charged ions in solution) should also be described within the “M” section of the TIMERS acronym.
Identifying a barrier to healing is not useful unless a procedure or treatment is available to overcome the barrier. Endogenous currents of injury can be boosted by EST, an existing technology that is ideally placed to overcome this newly proposed barrier to healing. EST has been shown to be a safe and effective treatment for hard-to-heal wounds.19,20,37,38 Several different types of EST have been successfully used in the clinic and are commercially available. Differences between options include the electrical parameters or treatment protocols used. Examples of differences in electrical parameters include the strength of the electrical signal delivered, ranging from subsensory, microcurrent EST, to high-voltage pulsed current, which can be felt as a tingling or prickling sensation, to neuromuscular electrical stimulation, which causes a muscle twitch. In particular, microcurrent levels of EST are believed to provide a physiologically relevant level of stimulation. 35 The practical delivery of EST can depend on the chosen technology, ranging from uninterrupted delivery of EST by means of pocket-sized, disposable, and portable devices managed at home by the patient, to large, capital equipment devices designed to be used for a set period per day in a clinic setting. Use of all devices requires a degree of training, which can often be provided by the manufacturer. Patient eligibility criteria that may suggest the use of EST include, presence of a chronic wound over 4 weeks in duration, failure of wound progression with standard care and wound-related pain which is affecting either aspects of wound management (e.g., ability to tolerate compression) or activities of daily living (Fig. 3). The benefits of EST in the management of hard-to-heal wounds are already recognized in wound care guidelines and recommendations including those published jointly by the National, European, and Pan Pacific Pressure Ulcer Advisory Panels, 39 the European Wound Management Association, 40 and the Wound Healing Society. 41 EST is one of the most highly evidenced therapy areas in wound management. Several meta-analyses of clinical studies have been published to date (listed in Supplementary Table S3), which are uniformly positive about the benefits of EST when used along with standard wound care (SWC), compared with SWC alone. Some of these benefits include a faster decrease in wound area,19,20,37,38,42–46 an increased proportion of patients healing,20,37,38,42–44,47 a faster time to healing19,48 a reduced risk of wound deterioration, 38 compared with control groups treated either with SWC alone or SWC plus a sham (nonactive) device.
Furthermore, EST can have a bactericidal and bacteriostatic effect on microbes and bacteria that commonly colonize or infect wounds, including Staphylococcus aureus, Escherichia coli, and Pseudomonas aeruginosa,49–52 including in biofilm.53,54 EST can also disrupt mixed-species biofilm 55 both in a porcine wound model 56 and in a randomized controlled trial (RCT) in patients with burns, in which EST significantly decreased biofilm incidence and severity compared with SWC. 57 Evidence has also shown that EST may be able to dampen down the expression of inflammatory mediators in the skin. 58 The evidence base suggests that use of EST in hard-to-heal wounds may also be able to contribute toward necessary actions within the “I” (infection/inflammation) section of the TIMERS framework and is also worthy of investigation in this context (Fig. 4).
The clinical benefits observed through the use of EST can also lead to a reduced resource burden. Wounds that are progressing well typically need fewer visits from health care professionals and fewer dressing changes, all of which take up valuable time. It is becoming more and more widely accepted that investing in evidence-based technologies that increase the likelihood of healing are more financially economical in the long run, than using cheap and ineffective products. Although advanced treatments may carry some upfront costs, these can easily be covered through the avoidance of future and long-term resource expenditure. Studies have shown that the financial benefits of using EST more than offset the costs of treatment, meaning that treatment can be financially beneficial overall to health care systems.59,60 In one study comparing the treatment-associated costs for the 12-months before and after use of a microcurrent EST device to manage leg ulcers, an 11% saving in overall costs of treatment was found. This included a 34% reduction in the number of nurse visits and a 26% reduction in the number of dressings needed per patient as a result of using EST. 59 In another study, an RCT-compared costs associated with Standard of Care (SoC) versus EST + SoC and found that EST + SoC not only had improved outcomes compared with SoC alone, but were also cheaper to manage, and so represented a dominant treatment. 60
EST can also reduce wound pain, often a key barrier to clinical improvement.19,61 Avendano-Coy et al. (2020) conducted a meta-analysis of eight RCTs and calculated that microcurrent EST reduced wound pain by a mean of 1.4 points (95% confidence interval [CI]: −2.7 to −0.2) on the 0–10 pain scale more than pain reduced with SWC alone. 19 Freedom from debilitating pain can transform the lives of patients but also transform their attitude toward wound treatments, allowing them to tolerate interventions they may otherwise have refused as being too painful (e.g., compression therapy, debridement). 62 EST may therefore also be viewed as an enabler of other effective wound management interventions. Reduced pain also fosters better sleep, improved well-being, and socialization—all essential factors in improving patients’ quality of life, as well as reducing the need for analgesics. 61 Reduced pain can also increase a patient’s mobility and level of activity, which in itself can be beneficial to wound healing, as activity can increase blood flow to the lower limb.
Limitations/opportunities for future research
Although a relevant body of evidence was identified in this systematic review, several gaps in the literature remain, which may represent areas for future research. While the current of injury and wound-related electric fields have been widely explored in the laboratory, their measurement in acute and chronic wounds, including any potential differences in different types of chronic wound, have not been explored. No monitoring of changes in the current of injury/electric fields over time in relation to healing status has been measured in patients. Studies exploring the impact of pathological states (e.g., ischemia, infection, hypertension) on the endogenous current of injury/electrical fields of the skin would strengthen the evidence base in this area, as would further exploration of the impact of inflammation in the skin on electrical fields associated with wound healing. In the absence of sufficient data specific to skin and wounding, some information presented in this review has been extracted from other epithelial tissues such as cornea and retina. The cornea is considered an acceptable model for cutaneous wounding 11 ; however, ideally, these studies should be replicated in dermal models or investigated in clinical subjects to confirm these findings. The inclusion of data from this wide range of models led to significant heterogeneity between the studies identified in the systematic review. Ideally, a diagnostic that would allow routine measurement of the TEP or current of injury in wounded tissue would be useful in identifying patients who would benefit from early use of EST to expedite healing; however, such tests are not currently easily available and some research and development is needed. Finally, several physiological changes associated with aging are well-characterized, for example, epidermal fragility, dryness, and thinning of the epidermal and dermal layers. 63 No research was found that linked these architectural changes to the reduction in the bioelectrical activity of the skin, although this association is plausible and may benefit from further investigation. The above points may represent evidence gaps that may benefit from further research.
INNOVATION
Results of the systematic review demonstrated that people with characteristics commonly associated with hard-to-heal wounds, in particular older age and diabetes, have impaired bioelectric properties in the skin, leading to lower TEP and current of injury compared with that of healthy or younger controls (Fig. 3). Given that the reduced current of injury is associated with slower healing,11,27,64 impaired bioelectricity may be considered a barrier to healing. EST can be applied as a simple adjunct to SWC and is well-placed as a treatment modality that can directly address this barrier through the application of an electrical signal to the wounded tissue and should be incorporated into wound treatment frameworks.
KEY FINDINGS
Results of this systematic review demonstrate that patients with comorbidities or characteristics associated with hard-to-heal wounds may have a deficient current of healing and that this is a clinically significant barrier to progression of their healing.
The means to address this issue, the clinical application of electrical stimulation therapy (EST), is already available and its use is supported by high level evidence; multiple meta-analyses of randomized controlled studies in different wound indications have already shown that microcurrent EST can significantly improve wound healing outcomes and also relieve wound-related pain.
Given this background, it is logical that clinicians should consider all factors that are now known to impact or impair healing, with the impairment of the current of injury being one of them.
Acknowledgement of the importance of bioelectricity in wound healing now provides the opportunity to update the TIMERS framework to incorporate the use of EST to address this deficiency in hard to heal wounds.
AUTHORS’ CONTRIBUTIONS
J.S.: Conceptualization, methodology, and writing—initial draft; R.M.: Conceptualization and writing—review and editing; E.W.: Project administration and writing—review and editing; All other authors contributed to writing—review and editing of all drafts. All authors approved the final draft.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
This article was funded through a unrestricted educational grant by Accel-Heal Technologies Limited, Kent, UK.
AUTHOR DISCLOSURE AND GHOSTWRITING
The content of this article was expressly written by the authors listed. No undisclosed individuals or ghostwriters contributed to the article. Authors J.S., E.W., and R.M., in their capacities as independent consultants and medical writers, received financial compensation for their contributions to the article from the project funder (Accel-Heal Technologies Limited, Kent, UK). No other authors have received any financial contribution for their role in contributing to this article. M.Z. is a member of the Scientific Advisory Board of Morphoceuticals, Inc. L.A. has previously received compensation from Accel-Heal Technologies Ltd for participation in an advisory board. K.C. is recruiting for an independent clinical trial investigating Accel-Heal. C.D. and H.M. have no relevant conflicts to declare.
ABOUT THE AUTHORS
Supplemental Material
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.