
Abstract
Transition into residential aged care (RAC) is a challenging process, often characterised by vulnerability, fear, and isolation. This study aimed to provide a contextualised description of transition within a care-facility in Australia to deepen our understanding of this major life event. A focused ethnography was conducted, which included formal interviews with residents during their first 6 months of living in RAC. The findings provide an account of the participants’ views on acceptance, highlight the challenges of loss, and showcase the coping practices new residents used. This paper provides a type of report card for the sector, which reveals that there is relatively slow progress with respect to supporting the needs of new residents during transition. There are opportunities for improvements regarding interventions, initiatives and practices to ensure residents are afforded a healthy transition.
Plain Language Summary
When older adults move into a residential aged care-facility (nursing home), it presents significant challenges for the individual, and is often marked by feelings of vulnerability, fear, and loneliness. This research sought to offer a detailed description of this transition to enhance our understanding of this significant life change. A focused ethnography research approach was used, which involved formal interviews with residents during their initial 6 months of living in the care-facility. The findings provide an account of the participants’ views on acceptance, highlight the challenges of loss, and showcase the coping practices new residents used. This paper provides a type of report card for the age care sector, which reveals that there is relatively slow progress with respect to supporting the needs of new residents during their transition. There are opportunities for improvement regarding interventions, initiatives, and practices to ensure residents are afforded a healthy transition.
Background and Objectives
In Australia older adults receive in-home aged care services from the government to assist them to live in their own homes (Australian Institute of Health and Welfare, 2023). Family members also play a key role in supporting their relative to remain at home; however, when the care needs of the individual become too complex for in-home services and family support, it may become necessary for them to move into a residential care-facility (commonly referred to as a nursing home).
Relocation into RAC is not just a physical move; it represents a transition between two life phases activated by some type of change, and is a time of ‘‘disequilibrium and upheaval’’ (Schumacher et al., 1999, p. 2). There are typically two triggers for transition: (1) hospitalisation (often due to a fall or other health issues), resulting in the need for a higher level of care than is possible through in-home services; and (2) a decline in an individual’s physical and/or cognitive health, adversely affecting their ability to carry out activities of daily living (McKechnie et al., 2018). Transition into RAC has been described as emotionally stressful, and a time of painful loss, grief and mourning (Sullivan & Williams, 2017; Zizzo et al., 2020), with feelings of abandonment, vulnerability, fear, isolation, and loneliness (Gardiner et al., 2020; Wilson, 1997; Zamanzadeh et al., 2017). Some clinicians have conceptualised the trauma of transition as Relocation Stress Syndrome (Manion & Rantz, 1995), the symptoms of which include depression, sadness, confusion, despair, sleep disturbance, withdrawal, and anger (Melrose, 2013). In particular, depression and loneliness – both prevalent among aged care residents (Amare et al., 2020; Gardiner et al., 2020) – can negatively impact quality of life, and cognitive and physical health (Gardiner et al., 2020; Hawkley & Cacioppo, 2010; Meeks et al., 2011). Given the potential harmful impact that transition can have on an individual’s health and well-being, it is important to identify and implement strategies to minimise negative outcomes and facilitate a positive transition for new residents.
Culturally, the way in which different societies care for older individuals differs around the world. For example, it is unusual and indeed quite rare, to find older adults living in nursing homes in the Philippines (de Guzman et al., 2012). In addition, what one country understands a residential care-facility to be, could be different from another country’s understanding of it. While a comparison of how various cultures around the world is likely a study within itself, a brief comparison of experiences from residents from long-term care in Ireland (Fraher & Coffey, 2011), a nursing home in Philippines (de Guzman et al., 2012), a care home in Slovenia (Križaj et al., 2016), a nursing home in Switzerland (Koppitz et al., 2017), an aged care home in Iran (Zamanzadeh et al., 2017), and a long-term care home in Canada (Sussman & Dupuis, 2014) indicated a few similarities. Residents in both the Philippines and Iran felt a strong sense of betrayal, resentment, abandonment, and rejection when they moved into a care-facility. A prevalent coping mechanism for individuals in the Philippines, Canada, Switzerland, and Slovenia was maintaining a sense of control over their lives, while both Slovenia and Canada also highlighted the significance of preserving a sense of self as a means to adapt to their new circumstances. Evaluating the experiences of residents across different countries poses a significant challenge, as it is crucial to take into account the cultural distinctions concerning older adults in each country, along with numerous other factors, such as when the study was conducted, the focus of the study, how long the participants had been living in the care-facility, the circumstances that led to their move, their involvement in decision-making regarding the move, as well as their family dynamics.
A large inquiry took place regarding the current status of aged care in Australia, with the final report from the Royal Commission into Aged Care Quality and Safety (RCAC) released in 2021. The report focused on the provision of high quality care and contained over 140 recommendations to improve the current system (Royal Commission into Aged Care Quality and Safety [RCAC], 2021). Amongst the many findings, the RCAC revealed that the care of older adults’ social and emotional needs were often ‘substandard’ (RCAC, 2021). Although this refers to all older adults in care, and not only new residents, this is concerning from a public health and human rights perspective, considering that transition into RAC is known to be a particularly difficult period for many residents.
The current study was supported by a large organisation with the aim of better understanding the needs of its new residents during the transition period and is an important piece of research which was undertaken shortly after the RCAC released its final report. The public learned of the many shortfalls of the aged care sector during the Royal Commission hearings due to the considerable media attention in the years leading up to the publication of the final report. The spotlight continued to shine on the aged care sector in the period following the publication of the RCAC’s findings, as stakeholders waited to learn of the many positive changes they hoped would be implemented.
Previous studies conducted in Australia have investigated the transition experience of older adults into RAC. These studies have differed in their methodology, as well as their focus. For example, a study by Larkey et al. (2024) used ‘appreciative inquiry’ – a method that does not necessarily highlight the barriers to a successful transition nor the negative experiences of new residents; instead, it creates ‘‘a sense of possibility rather than a sense of limitation’’ (Reed, 2007, p. 7), relying on the assumption that ‘‘what we focus on becomes our reality’’ (Reed, 2007, p. 7). Three other studies examined transition using a phenomenological approach (Marshall & Mackenzie, 2008; Nay, 1995; Polacsek & Woolford, 2022), and focused on describing the ‘‘essence’’ of the individuals’ experience – that is, ‘‘what’’ the individual experienced and ‘‘how’’ they experienced it (Creswell & Poth, 2018). Furthermore, Polacsek and Woolford (2022) concentrated on how to support the mental health needs of older adults during their transition into RAC, whilst Marshall and Mackenzie (2008) focused on residents living in low-care hostels, which differs from high-care RAC. Another study by Zizzo et al. (2020) used focus groups, which included residents and carer-relatives, as well as a staff forum, to collect data about experiences relating to loss and grief during transition.
This paper provides a rich ethnographic description of the current experiences of new residents who have recently moved into a residential care-facility following the Royal Commission. While there are some similarities between the earlier studies cited above and the study presented here, this study is the first to utilise a ‘focused ethnographic’ methodology, which relies on immersive and participatory practices in a particular setting to reveal lived experiences and purposefully disregards any pre-conceived conceptual frameworks in order to construct a provocative description of what is experienced within the setting ‘in focus’. Furthermore, this research provides the most recent ‘snapshot’ of transition in Australia, which RAC stakeholders should consider in their everyday practice and through their interactions with residents.
Research Design and Methods
Focused ethnography is ideal for research projects underpinned by a defined, pre-determined aim, which can be explored over a short time with intense ‘bursts’ of ethnographic engagement in a specific setting that is (somewhat) familiar to the researcher (Cruz & Higginbottom, 2013; Higginbottom et al., 2015). As per Roper and Shapira (2000), one of the primary strategies used in focused ethnography is participant observation, which is a process of collecting data through participation in the lives of the participants. This particular technique enabled the principal investigator, to become immersed in the culture of the care-facility, and thus identify and analyse the meanings that new residents constructed to make sense of their transition experience.
Purposive sampling was used to recruit participants and select the research site. The research team and the RAC organisation that managed the care-facility where the research took place had a mutualistic relationship with similar goals and values (i.e., the welfare of residents in RAC). The alignment of this partnership resulted in recruitment taking place in an ideal setting, a 160-bed care-facility located in Western Australia, which opened in May 2020. Participants had to be a permanent resident for between 1 and 6 months and have either no or mild cognitive impairment. The participants’ cognitive status was assessed using the Mini Mental State Examination (MMSE), which served as the basis for determining their eligibility for inclusion in the study. In addition, the Director of Nursing exercised clinical judgement to determine the overall suitability of potential participants. Progressive recruitment took place between August 2021 and November 2022, yielding 19 participants (16 females, 3 males) between the ages of 69 and 98 years (mean age = 91), with females (84%) being over-represented in this sample compared to the typical 66% of residents who live in RAC (Australian Institute of Health and Welfare, 2023). This mismatch of gender ratios was due to disproportionately more females meeting the inclusion criteria and agreeing to participate.
The first author met with eligible residents to explain the study, provide them with an Information Letter, and ensure they understood that participation was entirely voluntary and that they could withdraw at any time. Once residents had ample time to consider their decision to participate and they had no further questions about the study, written consent was obtained from all participants. The initial intent was to interview new residents three times – at the end of their first month as ‘new resident’, and again at 3 and 5 months post-admission into RAC; however, there was some attrition during the early stages of the project, which meant that some participants were not able to proceed to interviews at the 3 and 5 month timepoints. Hence, the recruitment strategy changed so that eligible participants who had been living in RAC for up to 6 months could be included in the study. A total of 27 interviews were conducted with 19 participants, with a duration of approximately 60 min per interview. Fourteen residents were interviewed once, two were interviewed twice and three were interviewed three times.
Data collection was conducted by the first author and took place between August 2021 and January 2023. Data collection included interviews, observations, informal conversations, and other documentation referred to during the interviews and informal conversations (e.g., the facility’s activity calendar and menu). The interviews consisted of semi-structured, open-ended questions to encourage participants to discuss topics that were meaningful to them. Questions were loosely organised around topics that related to: life before RAC; the decision to move; the actual move; and life after the move (an interview guide is provided in Appendix 1). It was important to ensure that participants felt they could safely recount their experience without fear of judgement or repercussions. Interviews took place in the participants’ rooms, with three participants preferring a communal lounge area. Interviews were recorded, transcribed verbatim, and then checked for accuracy by reading individual transcripts while listening to the audio recording.
Observations were conducted during visits to the facility (~twice a week) over a 17-month period by the first author (S). During this time, resident interactions – with each other, with staff and within the common areas of the facility – were observed by ‘S’. The first author had two roles at the research site: (1) principal investigator and ethnographer, and (2) exercise physiologist, running group-based exercise classes. It was not unusual for ‘S’ to visit the communal lounge areas, and interact with residents, staff, and visitors. ‘S’ also had capacity to visit residents in their private rooms, reminding them about the group exercise classes, checking up on participants if they were unwell, or simply to just say ‘Hello’ and have a chat. Informal observations and conversations were recorded in a ‘field note’ journal-that is, about the nature of interactions, apparent mood, and any noteworthy comments residents made about their daily experiences. Due to the different roles performed by ‘S’, a conscious effort was made to bracket the way in which she interacted with residents and analysed the data. As per Cruz and Higginbottom (2013), reflexive notes were added to the journal so that ‘S’ could interrogate and negotiate her roles as researcher and exercise physiologist. ‘S’ also recorded observations about the participants’ daily activities – for example, if a resident usually ate all meals in their room or if they ate in the communal dining area. While these observations and interactions were recorded generally (ethnographically), they naturally included residents who engaged with participants (but were not participants themselves). Ethics was granted for this on the basis that those ‘other’ residents would not be identified or quoted verbatim.
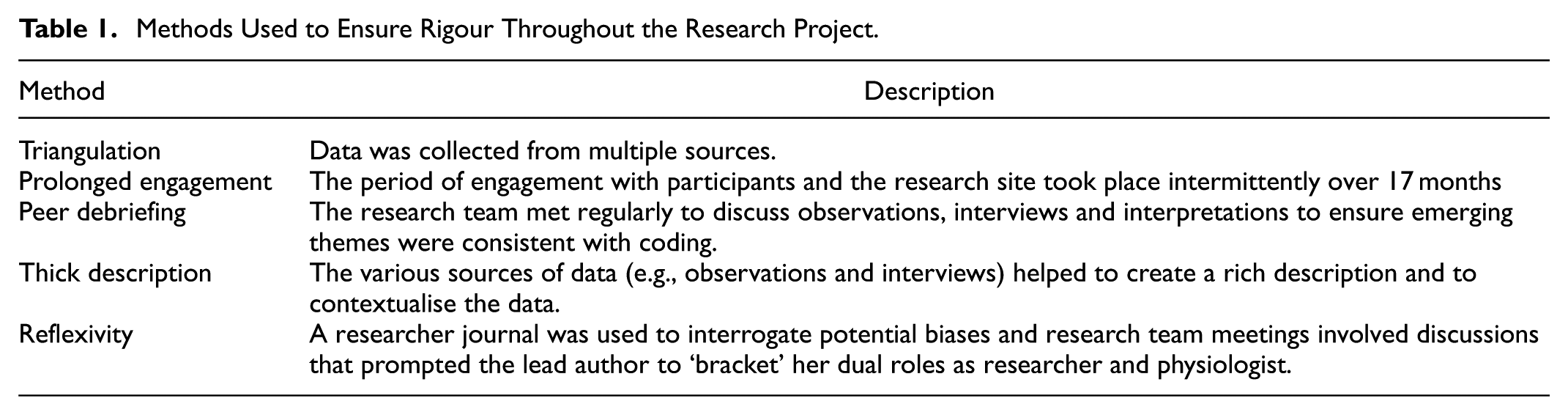
Data analysis was guided by Braun and Clarke’s (2006, 2022) ‘six steps’ of thematic analysis (see Appendix 2 for further details) and NVivo 12 was used to support data organisation and coding. Codes were derived inductively and refined to ensure they captured the intrinsic meaning of the experiences constructed by the participants during interviews (Fossey et al., 2002) and reviewed in light of other observational field notes. Data saturation was not the focus of this research, as the study provides a ‘snapshot’ of the transition experience post the Royal Commission investigation and was therefore not evaluated; however, it is unlikely that data saturation was reached. General methods used to ensure rigour in ethnography (Rashid et al., 2015) were followed; however, the duration of engagement was modified, as engagement in focused ethnography is typically performed episodically, rather than over a continuously long period of time (Higginbottom et al., 2015; for further details, see Table 1).
Methods Used to Ensure Rigour Throughout the Research Project.
Findings
The journey of transition is presented in this section through the three themes developed during data analysis. The first theme, ‘The Transition Journey – how it begins’, describes the various reasons and ways in which new residents embark on their journey from one relatively stable phase to another (i.e., accepting and adapting to their new life in a residential care-facility), along with their attitudes regarding their move. The views held by new residents concerning the losses they have experienced, as described in Theme 2, combined with their ability to implement effective coping strategies, which are explored in Theme 3, are intrinsically connected, as one often impacts the other. The manner in which residents perceive their losses not only shapes their emotional and psychological responses to transition, but also influences their readiness to embrace coping mechanisms that can facilitate their adaptation to and acceptance of their new circumstances. Ultimately, the participants’ journey towards stability offers a profound perspective on the ways in which new residents navigate the complexities of transition. Table 2 provides a summary of the themes and sub-themes discussed below. The participants’ names provided below are pseudonyms.
Summary of Themes.

The Transition Journey – How It Begins
The transition journey can be fairly simple and straightforward for some; conversely, others may feel disorientated and struggle to accept and adapt to their new way of life. The data collected highlighted that moving into RAC can be a complex and emotional journey, which can begin in a variety of ways. The stories shared by participants showcased their perspectives on transitioning into RAC, along with some of their reflections on acceptance of their new living environment. The start of the journey appears to significantly influence these views, as well as the rest of their journey.
It appeared as if some participants were simply ready to make the move into RAC. Deidre and Sue reported engaging in discussions with their respective families prior to moving, and neither reported experiencing any major health issues that precipitated the move. Within the first month of moving, both Deidre and Sue’s views of their new residence were fairly positive: I really have that feeling that I live here. (Deidre) There really isn’t very much to complain about … [this is] my home now. (Sue)
Other participants shared similar sentiments, such as Joan, who had planned a brief stay to ‘test the waters’; however, just 2 days after moving into the care-facility, she decided to make her stay permanent. Reflecting on her decision 5 months later, Joan appeared to be delighted that she had settled in so well and noted that ‘‘maybe the secret is making the decision while you still can’’!
In contrast, Mary, who moved into RAC due to health issues, appeared to have some initial difficulties adjusting, with her journey resembling a roller coaster at times. When interviewed 5 months post-admission, she explained: When I had a bad day … [let’s say] something happens at lunch time, I go back [to my room] and get a bit emotional, and think, “Oh God, I wish I hadn’t come”, … I have my ups and downs. More ups than downs, put it that way. (Mary)
Jennifer’s move was also precipitated by an unexpected health crisis that left her with little time to prepare. Having lived very independently before the move, Jennifer struggled with how drastically her life had changed, and how she had suddenly become ‘‘an old woman’’. During her interview 5 months post-admission, Jennifer noted that while she ‘‘just accepted it’’ and was ‘‘resigned’’ to the fact that RAC was ‘‘home for the moment’’, she still found it ‘‘hard to adjust’’. Jennifer’s view that she was ‘‘just passing through’’ the facility may explain why she did not seem to feel it necessary to create a homely space (noted as an important coping strategy in the discussion). During the 7 months that Jennifer had been living at the facility, she brought only one painting and some crafting supplies from her home; the rest of her furniture and personal belongings remained in the home she still owned. Jennifer’s struggle to accept and adjust may have been influenced by her decision to keep her home, presumably leaving open the possibility to return to her former life.
Other participants inferred similar challenges to accepting life in their new environment. Jane’s views on accepting her new life seemed to fluctuate during the 5 months we interacted. In her first interview, 1-month post-admission, she explained: I mean you realise that this is it and whether you like it or not, you’ve got to face up to it, so you do…. I ask myself is there an alternative? And if there’s not, and I don’t think there is, then I suppose one has to accept these things. (Jane)
Despite knowing that she had to accept the situation, Jane explicitly redacted her use of the word ‘accept’: I mean I put up with it. Accept is a sort of stronger word. No, I would say put, I put up with it, but I don’t like it and I don’t feel happier about it or anything. I don’t think I can even say that I’m getting to accept it more. Accept, I’m not really sure I’d like to use that word. (Jane)
Five months post-admission, Jane expressed a type of resigned acceptance, saying: ‘‘I suppose I don’t really want to be here, but I have no choice in the matter, … I’m here whether I like it or not. I’m not happy about it’’.
While for many participants the move to RAC was triggered by personal health issues, Margaret reportedly moved because her husband needed a higher level of care. It was a move that Margaret appeared adamantly opposed to: ‘‘I just really hate being here … I just feel like crying … Terrible … [I] just don’t want to be here … I just feel [I’ve] got claustrophobia … nothing nice here, I don’t like it’’. By the 5th month, Margaret’s opinion towards RAC had not changed: ‘‘I still don’t want to be here … I want to be home … I didn’t want to come in the first place … I just can't settle … I think I'm homesick’’. There were several occasions during our interactions when Margaret seemed agitated and tearful, and appeared to be experiencing significant emotional distress. In these situations, ethical protocols were followed whereby various support services were offered and the nursing staff were notified of her distress.
These accounts suggest that some residents had started to accept and embrace their new living environment as home, while others completely rejected any sense of home or belonging from the outset. The circumstances which led to the participants’ admissions, along with their perspectives regarding the move and the RAC itself, played a significant role in their capacity to accept their new place of residence, thus affecting their transition journey. The participants’ sense of loss, which will be discussed in the next theme, can also impact their transition.
Loss
Participants expressed a profound sense of loss associated with the absence of their home, which is widely recognised as being linked to personal freedom, control over their daily lives, and a place to express their individuality. The loss of their home and moving to a care-facility appeared to reduce the participants’ sense of autonomy, freedom and independence, limit their choices, and create a restrictive and rigid environment as they transitioned from a self-determined life into an institutional one.
Autonomy
The loss of autonomy was a salient issue expressed by numerous participants in this study, as many of them struggled to cope with the loss of their autonomy. This loss was intensified for Jane when other people made decisions on her behalf. Jane, who had always been an independent person, recounted feeling as if she were now ‘‘in somebody else’s hands’’, when other people suddenly began making decisions for her. As Jane described, ‘‘being told to do this, that and the other’’ was ‘‘bloody hard and unpleasant’’.
Some of the participants described how the rigid rules and regulations of RAC had negatively impacted their sense of autonomy, which seemed to exacerbate their feelings of loss. For example, Ron had an issue regarding the fixed mealtimes: ‘‘It was still a problem in accepting that I’ve got to go to meals when I’ve got to go. And not necessarily that I wanted to eat anyway’’. Ron found the routines ‘‘a bit of a shock to the system’’, and described life in RAC as ‘‘a regimented, almost prison-like existence’’. It was not simply the strict routines that frustrated Ron – he conceded that he had ‘‘no real power’’, which contrasted sharply with how he described himself before moving to the facility.
Furthermore, losing agency to make simple choices about everyday life appeared to result in unpleasant and uncomfortable situations for some participants. An example of this was being assigned a particular seat at the dining table, rather than choosing one of their own. For Betty, being seated next to residents with cognitive impairments was particularly challenging and reduced her enjoyment of mealtimes. In Betty’s words, her dining companions were often ‘‘away with the fairies’’, and she struggled to cope with other residents poking at her food, or having regurgitated food smeared on the table beside her plate. Similarly, Lauren, a wheelchair user, explained how her original dining companion was not ideal. Mealtimes were one of the few occasions Lauren left her room to talk with others – unfortunately her dining companion was ‘‘terribly deaf’’: I was sitting at a table with him and nobody else, and it was pretty stultifying because we couldn’t have a conversation. He would say things, occasionally, or even quote a few poems and things … it would have been awful had I been left with him. (Lauren)
While both ladies were eventually moved to a new table and their dining experience improved, disgruntlements about not being able to make simple choices were widely expressed by participants in relation to their loss of autonomy.
Independence
Similar to Jane, Elaine also described herself as being independent pre-RAC by recalling her former freedoms, describing how she ‘‘drove all over the place’’ visiting friends – essentially doing whatever she wanted to do. Following her move to RAC, Elaine explained that her independence had been lost, along with her ability to ‘‘go and do what you [she] want[ed]’’. Elaine no longer described herself as independent – the fact that she was no longer able to do what she wanted to do suggests that she was now an individual who was being controlled by others. This was a common sentiment expressed by participants in this study, primarily for those who declared that they did not accept or want to adapt to life in a care-facility.
Identity
Considering that many residents described themselves as independent before moving into the care-facility, their perceived absence of independence and control as residents in a care-facility appeared to negatively impact their identity. Jane’s sense of self seems to have been similarly impacted by the loss of her home and the institutional routines associated with living in a care-facility: What sort of person am I? I mean really, I think to myself, “Who do you think you are?”… I have nothing, I’m in somebody else’s hands, which you know I’ve always been an independent person … This is not really me. I’m not really quite…all of me [is not] here. Part of me is somewhere else. (Jane)
Not only did Jane comment that part of her was missing, she also expressed a complete loss of her identity: ‘‘To me it’s rather as if I lost myself, I’m standing back as if I’m looking at these things [pointing to her room] but I’m not really here. I don’t know, where am I?’’
Against this backdrop, the following theme outlines the various mechanisms that participants used to help them cope with life in RAC.
Coping Practices
In order to foster a sense of stability amidst the upheaval of their new circumstances, several participants identified a range of practices and strategies they adopted. These approaches appeared to facilitate their adaption to their new lives, and manage the considerable changes they encountered.
Making New Connections
Meeting others and forming new connections helped new residents develop friendships, and created opportunities for residents to support and help one another, thus providing some residents with a critical sense of purpose in RAC.
A short while after Ron and his wife moved into RAC, another couple, David and Yvonne, moved into the room next door and the couples struck up a friendship. Ron used humour to connect with Yvonne and reported that he had ‘‘someone to talk to, who [could] understand’’ him, and with whom he could ‘‘have a laugh, and a joke’’. Ron reflected that Yvonne was ‘‘good therapy’’ for him. Ron appeared to value Yvonne’s jovial nature, and his story highlights the importance of making new connections in the process of transition.
While some participants described the enjoyment they derived from these social connections, there was also evidence that new connections fulfilled a need for purpose and meaning. For example, making new connections with other residents was often described in relation to providing emotional support. Margaret recounted how she helped her neighbour: A couple of weeks back, you know when Yvonne’s husband died, well she was coming in every night, into my bedroom, or I'd go to hers to cheer her up. I'd take her some chocolate or something. (Margaret)
It was rare to see Margaret interacting with others as she was quite deaf and had difficulty conversing with others. Despite Margaret’s hearing impairment, she was still able to support and comfort her neighbour during a particularly sad time.
Other examples of providing support and helping others took place in the dining area. Jennifer described how the residents at her table, ‘‘our little group of eight’’, helped each other by moving walkers closer to the table ‘‘because they [other residents] are a bit shaky from the chair to the walker’’. Jennifer also stated that ‘‘if the staff are too busy, and somebody needs to be wheeled down to their room, there’s a couple of us that’ll actually do that’’. I often witnessed Elizabeth pushing Lauren’s wheelchair to meals or assisting her in her room. While Lauren appeared to value Elizabeth’s assistance, it is likely that Elizabeth derived as much benefit through an enhanced sense of purpose.
Jennifer was also able to find meaning by caring for and helping others, as was apparent in the story she recounted about her interaction with a new staff member: Sarah was in the dining room, we’re having breakfast and she just walks in and stands there … and she was crying. She was holding it in but you could see that she was really upset and I asked her, her name. I made a point of watching her, always speaking with her. And when the week was up she came to me and she said, “I’ve got a gift for you” and she gave me that plant. And she said, “Thank you very much”… and just gave me a little hug. (Jennifer)
As noted in Theme 1, Jennifer described herself as ‘‘an old woman’’ and no longer the person she was pre-RAC; however, the realisation that she could continue to help others in RAC was particularly meaningful for her.
Approaches to Regaining Self-Determination
The coping practices that participants adopted during their transition in relation to the losses discussed in Theme 2, are presented in this sub-theme. Participants attempted to improve their sense of self-determination by preserving their identity, regaining a sense of control, and creating a homely space.
Jennifer remarked that residents were ‘‘getting to the age where [they are] becoming invisible’’ - to counter this, she actively sought out ways to preserve her individuality by ensuring she was acknowledged by name and was ‘seen’. This was one of the reasons that Jennifer joined in with so many activities, ‘‘I’ve got people that’ll say, ‘Hello Jennifer’ or ‘Sit here Jennifer’’. It appeared as if Jennifer was comforted by the fact that the staff knew her and remembered her, but was the only participant who explicitly discussed the importance of ‘revering someone’s name’ as a sign of their individuality.
Despite stating that they had lost a sense of autonomy in RAC, some participants described how they had regained some level of control. One strategy participants used was creating their own routines. Three months post-admission, Mary had formed her own personal night and daytime rituals. In addition, both Mary and Deidre discovered they did not ‘‘have to’’ participate in activities if they did not want to. When Deidre was interviewed, she said she could do what she liked, and she did not do anything that she did not like! Mary also knew how she wanted to spend her time and did not ‘‘feel guilty in saying ‘no thanks’’’. Both ladies appeared confident in their decisions and seemed to have regained some sense of control in RAC.
Creating a homely space was another way in which participants were able to preserve their individuality and regain a sense of control. Moreover, having personal possessions in their rooms helped several participants to maintain a connection to their past. For example, Sue’s personal items created links to her youth and her family: It just brings me back to my younger days, and my happy memories, and then later on, particularly with my husband, and of course my children and grandchildren. I mean, everything here has a memory for me. (Sue)
Similarly, many of the items Betty brought to RAC reminded her of family and friends. The various objects were ‘‘just things that mean[t] a lot’’ to her. Some of the items were ‘‘from friends that might not be here anymore’’, and from Betty’s husband, that reflected things they enjoyed together. Personal treasures reminded participants of happy occasions, creating a link to their past and seemed to serve as a continuation of their identity.
While Mary was in hospital, her family decorated her room so that she would be surrounded by items that were familiar and reminded her of home. These actions helped Mary to be more confident in her decision to enter RAC, and helped her to adjust to her new home: The kids all brought things from home, like the bookcase with all my photos … And June (daughter) [had] even gone to the point of somehow or other cutting down my bedspread that I had in there, so I walked into familiar things. And that was very pleasing that you’ve got things that were in the house. (Mary)
Jane tearfully described leaving her home as ‘‘painful’’; however, having her personal possessions made ‘‘things a lot easier’’, and although many of the objects were not worth much money, their value (for Jane) lay in the memories attached to them. Jane described the objects as being part of her home and part of her. These special items not only created a connection to Jane’s past, they were also closely linked to her individuality. It was important to Jane to be able to bring these items into RAC, as it meant that she had part of her home with her and she was eager to share what they ‘said about her’ and her former life.
During transition, several participants successfully implemented a range of strategies to navigate the various challenges they encountered. These approaches appeared to facilitate a smoother transition for some of the new residents. However, the journey to stability for new residents who struggled to develop meaningful friendships, maintain their sense of identity, regain a sense of control, and create a homely space is likely to remain a distressing and unhappy experience.
Discussion
This study aimed to gain an in-depth, rich understanding of the experiences of new residents when they moved into a care-facility in Western Australia, soon after the Royal Commission into Aged Care Quality and Safety released its final report in 2021. The challenges experienced by new residents as they transitioned into RAC, as previously identified by Nay (1995); Polacsek and Woolford (2022); and Zizzo et al. (2020), appear to still persist. Indeed, the experiences of the participants in the current study are a familiar story, and although some residents were able to develop their own coping strategies, few participants appeared to have experienced a completely healthy transition. The findings of the current study serve to emphasise that aged care providers need to intensify their efforts and be more vigilant in identifying those residents who are struggling to adjust and accept their new way of life in a care-facility.
Three themes were identified from the data analysis, with the first, ‘The Transition Journey - how it begins’, highlighting the variations in acceptance among participants, as well as the influence of the circumstances preceding the transition on this process. The findings echo previous research that identified that the circumstances precipitating transition and the residents’ involvement in the decision can shape their transition journey (Brandburg, 2007; Brownie et al., 2014). Residents who choose to move into RAC and feel in control are more likely to have a positive experience (Davison et al., 2022; Yong et al., 2021; Zizzo et al., 2020). Conversely, those who do not fully accept that their care needs have changed may feel pressured to move (Zizzo et al., 2020), leading to feelings of regret, loss, and anger (Scheibl et al., 2019). However, accepting their new living situation generally cultivates a ‘‘positive outlook’’ (Bradshaw et al., 2012, p. 431), which can facilitate independence, promote resilience and ameliorate feelings of loss (Bradshaw et al., 2012).
The theme of ‘Loss’ highlights the numerous losses experienced by new residents when moving into RAC, of which a perceived loss of autonomy, independence, and identity were most salient. Feelings of grief, mourning, imprisonment, sadness, anger, and fear were common among participants (Paque et al., 2018) as they reflected on their former freedoms that had been lost upon leaving their homes. This aligns with Hatcher et al. (2019), who reported that home is strongly associated with notions of autonomy, independence and freedom of choice. Furthermore, transition appeared to impact the participants’ sense of identity, corresponding with Riedl et al. (2013), who reported that moving into RAC affects an individual’s social status, connections, and habits, which, together with autonomy, can collectively ‘‘destabilize’’ the resident’s identity (p. 8).
The final theme, ‘Coping Practices’, described how some participants managed the challenges of transition by regaining a sense of autonomy and control, developing meaningful connections, and creating a homely space. Notably, these coping strategies appear to be driven by their innate needs, which is most clearly understood with reference to Self-Determination Theory (SDT; Deci & Ryan, 2000). The premise of SDT is that when individuals have their basic psychological needs of autonomy, relatedness, and competence fulfilled, it leads to ‘‘psychological growth, integrity, and well-being’’ (Deci & Ryan, 2000, p.229). In this study, participants regained autonomy and control by actively preserving their daily rituals, declining requests to attend activities that did not appeal to them, and personalising their room with familiar and sentimental objects to create a sense of home. Creating a homely space using personal possessions can make it easier for residents to maintain (or strengthen) their personal identity (Blackler et al., 2023; Cooney, 2012; Falk et al., 2013) and can foster feelings of belonging (Blackler et al., 2023).
Participants in this study also found ways to meet their need for relatedness and competence (elements of SDT). In this study, the benefit of relatedness was two-fold: it offered residents a sense of enjoyment and a feeling of being connected to others, as well as the opportunity to help others. Participants’ discussions on helping others reflect their need for purpose and meaning and allow them to demonstrate competency. Here, the benefit is not just to the resident being helped; it also enables the ‘helper’ to demonstrate they are still a capable member of society and not just an older person receiving care.
This paper showcases the voices of residents as captured through the lens of focused ethnography. Whilst some residents demonstrated resilience and utilised effective coping strategies that preserved their identity and helped them to regain a sense of control, this study also presents the thoughts and reflections of those residents who were unable to utilise the necessary individual or environmental resources to create a new stable lifestyle for themselves. Despite recommendations from the Royal Commission into Aged Care Quality and Safety (RCAC) for care-facilities to promote autonomy and meaningful living for their residents (RCAC, 2021), the perception of some participants in this study suggested that they had to discover their own way to cope, create meaning in their lives, and regain a sense of autonomy.
Transition is a personal journey, and the needs and preferences of new residents are unique. Social connections may prove beneficial for some residents, while others may find them insufficient to ease their transition. Some residents may have been able to create a charming, homely space and express their individuality through decorating their rooms; however, they may have felt as if they lacked autonomy in areas that were meaningful to them. The voices of those who struggled to accept their new lifestyle offers the aged care sector some insights that can be employed by organisations to identify these residents pre- or on admission and provide them with appropriate and additional support, which may differ for each resident. While some residents had the confidence to exercise agency and to make their own decision, others chose to ‘go with the flow’, assuming a position of no choice. The findings presented here serve as a type of report card for the aged care-facility in which the study took place, and not only provide insights into the varied experiences of residents during their transition into RAC, but they also offer the sector some awareness of what must change at the present time to avoid further investigations into the quality of care in Australian aged care-facilities and to make transition and the subsequent time spent in RAC more enjoyable.
Strengths and Limitations
The expertise and aged care experience of the first author, an Exercise Physiologist who has worked with older adults in various settings, and possessed communication and relation-centred care competencies, allowed for a richness of authentic and reliable data collection. Furthermore, timely and supported access to the care-facility, its staff and residents was facilitated by the partner organisation. As with all research a number of limitations were experienced. Research into RAC has been challenging, particularly in a post-COVID-19 world, given mandatory face masks needed to be worn, facial expressions were often hidden and verbal communication was affected, particularly with participants who were hard of hearing. Infection control is especially important in RAC; however, it often obstructed access to residents during COVID-19 and other outbreaks. Repeat interviews over the first 5 to 6 months in RAC could not be conducted with all participants, as some were unwell or in hospital at the time of the follow up interviews. Two participants passed away during the research period. The current study was limited to those residents who had either no or mild cognitive impairment which accounted for only 45% of the new residents entering the care-facility during the research period. An understanding of the transition experience for people with moderate or advanced cognitive impairment using a similar focused ethnographic methodology is needed to gain further insights. Further studies are clearly warranted that will continue to increase the body of knowledge that is aged care and will be of value for all older Australians.
Conclusion
This focused ethnographic study aimed to provide fresh insights into the transition experience from the perspectives of new residents. This study reported on some good news stories regarding the coping practices voiced by our participants; however, there were also participants who were unable to draw on some of the strategies mentioned and who were adamant that they would never settle and be happy in the care-facility. Residential care-facilities and their staff must be cognisant and possess the necessary competence to enable residents from diverse backgrounds to assimilate into the care-facility and experience a healthy transition. All organisations must have processes and practices in place to meet the individual needs of each person entering their care-facility, thus providing a place that they can call home and where they can live an active, self-determined, and meaningful life.
Practical Implications
RAC organisations need to provide a supportive environment that potentiates autonomy, choice and decision making to the maximum extent feasible. This is achieved by collaborating with residents and their families to ensure quality of life, wellness and well-being are fully realised on each person’s terms.
New residents who have entered RAC due to a sudden and/or unexpected event/illness must be identified using a pre-admission process. This will enable the care-facility to offer early engagement in a specialist, targeted transition program to promote wellness through a sense of enhanced autonomy and control.
Residential care-facilities must consider a variety of opportunities for new residents to engage in meaningful and relational activities that enhance their sense of confidence and competence, and thus their self-worth.
Footnotes
Appendix 1: Interview Guide
Appendix 2: Data Analysis Process Following Braun and Clarke’s Thematic Analysis
I started by familiarising myself with the data – the transcripts were read through in full three times. Firstly, transcripts were read while listening to the interview audio to ensure the transcription was accurate, secondly, transcripts were re-read in full without the audio. The last full read through was more active – notes were made as the transcripts were read though, which included additional context from field notes and any initial thoughts on what participants were reporting. The transcripts were then downloaded into NVIVO and the process of generating initial codes (step 2) began. Transcripts were analysed one at a time. As transcripts were read through, content relating to the research topic was given a label/code. Once the transcripts had been organised into smaller segments of codes, the data assigned to each the initial code was examined. Some of the initial codes were re-labelled and some were merged together. The initial coding resulted in a large number of codes. The process of building initial themes (step 3) started with grouping similar codes together into rudimentary categories. Within each of these broad categories, further similarities and connections between the codes were reviewed – these codes were then grouped together to form a number of initial themes. The research team met periodically to discuss the initial themes during Step 3 (see Table 1– Peer debriefing). These themes were then reviewed and refined (step 4), firstly, within each theme and then as a whole data set. The following questions were considered for each theme: was there a logical connection between the codes; were themes clear, did the themes convey the essence of the data within them; did the themes relate to the research question; did each theme centre around one concept; and did the codes grouped under each theme support the theme as a whole. For the revision of the data set as a whole, the following questions were considered: how did the themes relate to each other; did each theme provide a deeper meaning of the central idea; were the themes distinct enough; and were the themes comprehensive. Answers to the above questions resulted in some themes being split, and other themes were merged together. Furthermore, some of the codes were grouped together to form sub-themes, particularly, if there were a large number of codes linked to a particular theme. Once the themes had been reviewed and organised, each theme’s name was defined (step 5) to ensure that it conveyed the essence of the central concept of the theme, and a description of each theme was written. Once the themes were defined and re-named, I circled back to step 4 to once again ensure that the codes in each theme fitted the name and description of the theme. Once this was done, I went back to step 5 to ensure the theme names and definitions conveyed the essence of the data in each theme description. Each theme was also inspected to ensure that they were coherent and understandable and that there was no ambiguity.
The themes were then written up (step 6) to convey what each theme illustrated separately and together in the broader context of the study. Extracts were selected that clearly and fully supported the themes and sub-themes. The themes were presented in a manner to ensure that the broader implications of the findings were clearly conveyed and understandable. As per Table 1, reflexivity was an inextricable component of the data analysis process, and was practiced throughout the steps described above. The values and motivation of the principal investigator, both as a researcher and exercise physiologist, align, as they aim to support older adults in leading fulfilling lives and maintaining ties with their families and communities. Specifically, the desire to help older adults remain connected to others brings immense fulfilment to the principal investigator.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.