
Abstract
We used a participatory action research (PAR) strategy for optimizing health literacy and access (Ophelia) to improve hypertension (HTN) management in a peri-urban village of Chandigarh (India). We used an embedded mixed method design for development, implementation, and evaluation. Through community consultations and vignettes created from interviews with population sub-groups and input from healthcare providers, we co-designed the intervention. Volunteers facilitated community-based awareness activities like door-to-door interaction, mobile messages, posters, collaboration with healthcare providers, and free blood pressure monitoring services. At the health facility, we improved communication by re-orienting healthcare providers and introducing medication adherence charts after identifying gaps through patients’ journeys. We measured changes in health literacy, HTN knowledge, risk factors, medication adherence, and HTN control in a sample of 510 randomly selected adults in pre and post-intervention design using chi-square and t-test. A checklist assessed community capacity and multivariable regression adjusted the effect of confounders. Health literacy significantly improved across most scales (beta range 0.17 to 0.76, p < 0.01). Hypertension knowledge scores increased from 2.9 to 3.4 (p < 0.05). Physical activity (≥1,500 MET min/week) (aOR 0.19, 95% CI 0.11 to 0.33, p < 0.01) and daily salt consumption (<5 g/day) (aOR 0.47, 95% CI 0.36 to 0.6, p < 0.01) improved. However, body weight, tobacco and alcohol use remained unchanged. Medication adherence (aOR 0.08; 95% CI 0.02 to 0.32 p< 0.01) and HTN control (aOR 0.28; 95% CI 0.08 to 0.94; p = −0.04) increased. Community capacity in leadership, planning, management, learning and skill development received high rating.
Plain language summary
In this study, we aimed to develop an intervention to help a marginalized community in a village in Chandigarh, India, to better manage hypertension (HTN). We used the Ophelia (Optimizing Health Literacy and Access) approach to identify health literacy challenges and gaps within the population. A mix of quantitative and qualitative methods helped us design the intervention and assess its impact. Community leaders and volunteers were actively involved in planning and implementing the intervention through repeated cycles of planning, action, and observation. Need-based activities included door-to-door awareness campaigns, text messages, poster displays about blood pressure management, medication adherence charts distribution through dispensary, and providing free BP monitoring services in the village. We also trained local health workers and healthcare providers to raise awareness. Despite challenges of COVID-19 pandemic, the results showed significant improvements in health literacy and increased knowledge about hypertension. The community also showed positive changes in physical activity, reduced daily salt intake, and improved medication adherence. Overall, the community’s ability to address health challenges strengthened after the intervention. In conclusion, participatory action interventions like ours, which rely on local resources and the existing healthcare system, can effectively improve health literacy and lead to better health outcomes.
Keywords
Introduction
Public health interventions are crucial for preventing diseases, promoting health, and reducing health disparities. Some of these interventions are more effective than others. For example, health promotion efforts are more effective when adopting an ecological perspective than the traditional information, education, and communication approaches. This perspective emphasizes addressing individual behaviors and broader social, organizational, and environmental factors.(Nutbeam & Muscat, 2021). Therefore, integrated approaches are required to enhance community capacity to develop and implement culturally appropriate interventions (Kumar & Preetha, 2012). Participatory Action Research (PAR) embodies this holistic approach as it places the community at the center of research (Macdonald, 2012).
Originating from the work of Paulo Freire and Kurt Lewin, PAR has been used extensively in both low and high-income countries to empower communities, particularly among marginalized groups, for social transformation (Burgess et al., 2022; Fernández-Aballí Altamirano, 2020; Tripathy et al., 2010). It requires genuine engagement with the community to share power and control over the research process (Arnstein, 1969; Baum et al., 2006). The community engagement involves fostering a meaningful relationship with groups of people, their formal and non-formal leaders, and local government and non-government organizations by exchanging information in formal and informal meetings to enhance community capacity for decision-making that affects their well-being.
In this context, researchers have proposed optimizing health literacy and access (Ophelia) as a structured participatory process between healthcare users and providers to identify and respond to the health literacy needs, ultimately improving health outcomes. Researchers have also used it as a practical tool for co-designing health interventions (Goeman et al., 2016; Tan et al., 2023). World Health Organization has advocated using Ophelia as a collaborative process to improve access to information, services, and resources for the prevention and control of noncommunicable diseases (NCDs), as literacy needs are high in these conditions due to their chronic nature (WHO, 2022).
In our study, we used Participatory Action Research (PAR) approach, using Ophelia process to support a marginalized community in India in managing hypertension. We chose this approach because strengthening individuals’ ability to understand and use health information, along with enhancing the community’s ability to work with relevant stakeholders, can effectively address emerging health challenges.
Material and Methods
Study Area
The study was conducted in a peri-urban village of Chandigarh Union Territory (UT) as health needs were higher in villages than in urban areas. From the list of all 22 villages of Chandigarh, UT, we selected a least developed village with a population of 9,800 consisting mainly of migrant workers who had lower socioeconomic status and limited access to healthcare facilities, water, sanitation, roads, and housing.
Study Design
To develop, implement, and evaluate the participatory action intervention, an embedded mixed methods (EMM) design was followed (Creswell & Plano Clark, 2011). Qualitative data were used to develop the participatory action intervention, whereas quantitative baseline and endline surveys were conducted to evaluate it (Figure 1).
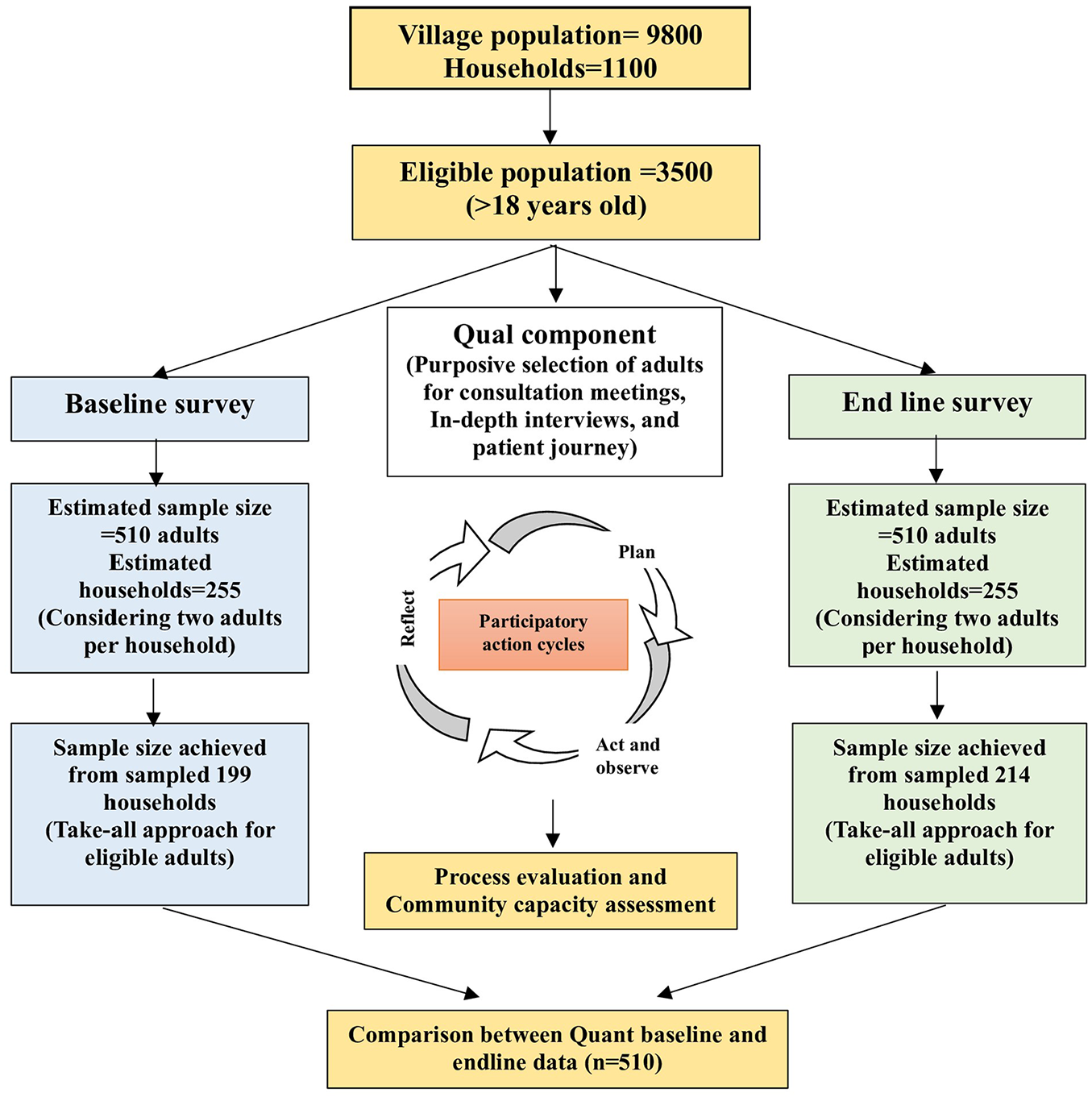
Flowchart of the study.
Study Period
The study was conducted from April 2019 to August 2021. The baseline quantitative and qualitative data took place between April 2019 and June 2019. The intervention was originally planned for the latter half of 2019, but the COVID-19 pandemic delayed its implementation until mid-November 2020 through May 2021. Process evaluations took place in January 2021 and April 2021, and endline data were collected from June 2021 to August 2021.
Study Population
Although the PAR had covered the entire community of the selected village, pre-post evaluation surveys were conducted on a sample of adults above 18 years of age (Figure 1), as hypertension is more common among adults, and early detection and management of hypertension are crucial for preventing complications. The evaluation component of the study included adults who intended to reside in the village for at least the following year and provided informed written consent. The study excluded pregnant women considering their unique requirements for managing and controlling hypertension.
Sample Size and Sampling
Quantitative Component
The research team estimated the sample size for the evaluation component using standard statistical methods for comparing two proportions with 0.8 power (β) and 0.05 alpha. Assuming a 20% medication adherence among hypertensives based on previous studies (Khwaja et al., 2017; Nagarkar et al., 2013) and to improve it to 40%, a sample size of 81 known hypertensive cases was required. Study required 162 hypertensive cases for the evaluation component, based on the assumption that 50% of hypertensive cases would be known cases. Therefore, with an estimated hypertension prevalence of 35% in the study community, 462 adults were to be surveyed to find 162 hypertensive cases. Considering a 10% non-response, we adjusted the final sample size to 510 adults.
Research team prepared a map of the village, and out of 1,072 households, 255 were randomly selected using computer-generated numbers, assuming that, on average, two adults would be available per household. All eligible adults from the sampled households were selected for the evaluation component of the study, as further sampling of one adult from the sampled households was not operationally feasible since lists of household members were unavailable.
Starting from one direction of the village, the survey was initiated from the first selected household on the left side of the street. The next household in the sample was approached consecutively until 510 adults were recruited from 199 households. If the team found a household locked on two visits, they included the nearest household from the selected households in its place.
To avoid the bias that may occur due to selective implementation of the intervention in households sampled in the baseline, for endline again we drew a random sample of 255 households, and recruited 510 adults from 214 sampled households using the same method as in the baseline. The study found only a 9% overlap in the sampled households in the baseline sample with that of the endline. All study participants had consented to inclusion in the study.
Qualitative Component
Community consultation meetings: We conducted nine community consultation meetings (participants = 76) to develop intervention activities. As most men were working, we were able to do fewer meetings (n = 3) with them, as compared to the women (n = 6). Meetings with men were conducted in the late evening hours or on Sundays. The purpose of the consultation meetings was to (a) identify the needs of the community in health literacy domains, (b) to know about the community expectations, and (c) to identify the roles and responsibilities of community members in the implementation of intervention activities.
Vignette development: The researcher (RP) conducted eight semi-structured interviews with randomly selected community members from each health literacy cluster to generate the vignettes (Passi et al., 2023). These vignettes were presented to healthcare providers to find solutions for the community’s health literacy needs.
Patient journeys: Based on input from community volunteers, researcher observed three patient journeys over 2 days at the health facility used by the community for hypertension treatment. She video recorded the interactions of patients at each level of care with the receptionist, nurse, doctor, and pharmacist, using an observation guide. Research team immediately destroyed these videos to maintain confidentiality after the multimodal transcription, that is, capturing verbal and nonverbal cues along with the context and interactions to understand the unmotivated looks (Borish et al., 2021). These data helped develop training strategies for healthcare providers.
Process Evaluation
Two process evaluations were conducted after cycles 2 and 3 to find the intervention coverage gaps and plan the next set of activities. Community leaders, volunteers, and researcher assessed the performance of intervention activities. Researcher conducted telephonic interviews of community members with high blood pressure (n = 219) during door-to-door blood pressure screening regarding the intervention uptake, perceived usefulness, and effect of the intervention activities on follow-up and treatment.
Study Outcomes
The research team measured the intervention effect primarily by assessing changes in health literacy scores in the study population, as well as self-reported HTN medication adherence scores among cases of hypertension diagnosed by a physician. Secondary outcomes included changes in the hypertension knowledge scores, body mass index (kg/m2), waist-hip ratio, daily dietary intake of salt (g/day), physical activity levels (MET min/week), alcohol consumption (%), and tobacco consumption (%), follow-up (% cases of HTN who received a check-up from a physician in the past 1 month) and control of blood pressure (below 140/90 mm of Hg among known cases of hypertension). Community capacity for planning, implementation, and evaluation was assessed after the intervention in six domains: leadership, planning and management, partnerships, learning and skill development, resource mobilization and monitoring and evaluation (Draper et al., 2010). Researchers (RP and MK) scored each domain on a scale of 1 to 5.
Study Tools
Quantitative tools used in the baseline and endline survey were: (1) Health literacy questionnaire (Osborne et al., 2013) (adapted and validated previously); (2) Hypertension knowledge questionnaire (Erkoc et al., 2012) (adapted and validated by the experts); (3) Validated 24-hour dietary recall questionnaire (Sharma et al., 1998); (4) Adaptation of WHO STEPS questionnaire for recording core behavioral measures and practices (WHO, 2020); (5) Medication adherence questionnaire (adapted and validated before use) (Fialko et al., 2008) (6) Record sheet for Body Mass Index, Waist and Hip circumference, and Blood Pressure; (7) Interview checklist for process evaluation; and (8) A community capacity building checklist (Liberato et al., 2011).
The qualitative tools were: (1) Topic guide for community consultation meetings with probe questions related to self-management of health, healthcare facilities in the village, interaction with healthcare providers, community participation in village issues and suggestions or inputs for the intervention, suggesting for volunteers and community leaders, (2) Semi-structured interview schedule for health literacy clusters’ vignette development, and (3) Observation guide for videography in the OPD of health facility to record patient journeys.
Data Collection
At the suggestion of community leaders, two volunteers (aged 18–22 years) who had completed schooling, were selected from the community for the data collection. The researcher trained them extensively to administer the study tools. The team collected 24-hr dietary recall data on two non-consecutive days (Huang et al., 2022). They followed WHO guidelines to measure anthropometric and BP readings (WHO, 2020). A digital automatic blood pressure monitor (OMRON HEM 7121J) was used to measure blood pressure. Team followed similar procedures for baseline and endline data collection. The researcher collected qualitative data and conducted community capacity assessment and telephonic interviews for process evaluation.
Development and Implementation of the Intervention
The participatory action involved cyclic progression from planning to action, observation, and reflection (Lewin, 1946). Table 1 presents cycle-wise planned, implemented, and evaluated intervention activities.
Cycle-wise Intervention Activities.

In the first cycle, after building rapport with the community leaders the researcher had meetings with the healthcare providers. Three “community leaders” (one male and two females) were identified who helped in the planning, such as organizing consultation meetings with the community members, identifying volunteers, and generating resources such as logistics for the intervention activities. The researcher acted as a “facilitator” for capacity building in the community.
Need-based, locally relevant intervention activities were co-designed using inputs from the community members and healthcare providers, and cluster analysis of health literacy data gathered in the baseline survey. Eight clusters or sub-groups of people with similar characteristics but with different health literacy needs in specific domains were identified (Passi et al., 2023), and vignettes were developed for these clusters using interviews with the community members (Tremblay et al., 2022). These vignettes were presented to medical officers of the nearest health facility to get specific solutions for addressing the health literacy gaps identified in each cluster.
As Anganwadi Centers (AWCs) - which take care of mothers and children, were an integral part of the village, team decided to integrate hypertension awareness generation activities in the weekly awareness camps held at AWCs by the Anganwadi workers (AWWs) and multipurpose health workers (MPHWs). Therefore, researcher trained AWWs and MPHWs to conduct awareness sessions. Researcher conducted two training sessions of six hours each for all six AWWs and one for two MPHWs of the village on health literacy domains, hypertension and its risk factors and treatment. The training also included measurement of blood pressure (BP).
Intervention commenced in the community during the COVID-19 pandemic in November 2020. Intervention activities planned in the first cycle were discussed with community leaders and volunteers again to ascertain their implementability while considering the pandemic situation. The plan for conducting awareness sessions for community members in groups of 10 to 12 persons, which was the favorite method suggested in community consultation meetings, had to be discontinued as AWCs did not have enough space to accommodate the groups after maintaining the required physical distancing. Exhibiting videos in the village square were also dropped to avoid gatherings. Community leaders and volunteers decided to use the methods that involved the least contact with the community members to minimize the risk of COVID-19 infection. They decided that volunteers should contact community members one-on-one and through mobile phone short messages service (SMS). Hence, researcher trained volunteers extensively in communication skills to create awareness about HTN, its risk factors, and the availability of healthcare services for routine screening and treatment follow-ups. Community collaborated with a private doctor, who was practicing in the village, and a mobile clinic of a private sector manufacturing company, to increase facilities for BP screening, follow-up and treatment within the village. The anti-hypertension drugs were initially unavailable at the HWC, so we arranged for donations to ensure their availability before starting the intervention activities. Primarily, the intervention activities in the second cycle included: (a) door-to-door BP measurement and motivation of HTN (new and known) cases and others to avail healthcare facilities, and (b) sharing SMS on reducing salt, increasing physical activity, cessation of tobacco/alcohol, regular follow-ups at the nearest HWC and medication adherence with known and newly detected cases of HTN twice a week. After performing these activities, researcher with the help of volunteers, carried out the first process evaluation among known and new cases of hypertension. It revealed that though community understood these activities, follow-up for BP measurement and treatment was low. Therefore, after discussing the process evaluation findings with community leaders, volunteers, and active community members (two female Anganwadi helpers and a male resident), door-to-door screening for BP was discontinued to avoid physical contact during the COVID-19 pandemic period. Instead of that, community decided to focus on interpersonal face to face communication, sending SMS to HTN cases again and keeping the BP apparatus in the Anganwadi center so that they could get the facility of BP check-ups near their homes. Therefore, the researcher trained the Anganwadi Helpers (AWHs) in BP measurement techniques.
In the third cycle, three trained volunteers conducted extensive interpersonal awareness activity sessions at the individual level, and sensitized 1014 adults (out of 3,500 adults in the community; 29% coverage) in 270 sessions. Researcher carried out the second process evaluation among hypertensives who had attended the awareness sessions (n = 172). It revealed that only 78 (40.6%) had a follow-up and availed physician consultation. Forty-three out of them were started on or continued the anti-HTN medications by the physician. On the other hand, only eight persons had approached AWHs for free BP measurement as AWCs were closed due to the COVID-19 pandemic.
The last intervention cycle was planned and implemented primarily on organizational health literacy. As per the suggestions of community leaders in the second process evaluation, hand-made posters on HTN awareness, prevention, and management, were displayed in the village. Researcher conducted trainings for AWWs, MPHWs and Healthcare Providers (HCPs) on behavior change communication.
Using solutions identified through review of patient journeys, the researcher trained three levels of healthcare providers: doctor, nurse, and pharmacist. The researcher trained the staff on a one-on-one basis and their practices were also observed. This training continued for 2 weeks until saturation. The researcher repeated the process after 15 days to check any remaining skill gaps.
Healthcare providers suggested the distribution of medication adherence charts to HTN patients while dispensing the medicines. Chart provided day-to-day monitoring with three types of marks to be filled in the box each day for a medicine taken on time (double tick), medication taken but not on time (single tick), and medicine not taken (cross mark). Team pilot tested the chart on five patients. This way, we implemented a six-month participatory action intervention in the community in four cycles.
Data Analysis
The data was analyzed using IBM Statistical Package for Social Sciences (SPSS) version 21. We calculated mean, standard deviation, median, and interquartile range scores for all nine scales of HLQ separately. From the risk factor questionnaire, study presented the preference for extra salt and oil in the diet, frequency of blood pressure check-ups, and weight measurement in percentages (yes or no). It also presented tobacco and alcohol users in percentages, and high physical activity at or above 1,500 METs minutes/week (WHO, 2020). BMI was categorized into four groups according to the criteria for Asians (Nishida et al., 2004). Abdominal obesity was defined as a waist-hip ratio of >90 for men and >80 for women, as per Asian cut-offs (Misra et al., 2006).
The 24-dietary recall data was entered into a spreadsheet used by the Prospective Urban Rural Epidemiological (PURE) study (Mahajan et al., 2013). Each participant’s nutrient consumption data was taken to estimate the average daily consumption in 2 days. Nutrient intakes were categorized as consuming recommended dietary allowances (RDA) or not using the Indian Council of Medical Research National Institute of Nutrition standards (Misra et al., 2006).
Participants with hypertension were categorized as “known” cases (already diagnosed by a doctor) and “newly detected” cases having high BP during the survey (systolic ≥140 mmHg and/or diastolic ≥90 mmHg). Medication adherence among known cases of hypertension was calculated as a score out of a total score of 9. The medication adherence scores were divided into two categories using quartiles: “non-adherent” with a score less than 7 (0–75th quartile) and “adherent” with a score of 7 or more (above 75th quartile).
Consultation meetings with community members, leaders, and volunteers were transcribed and analyzed using descriptive analysis. The semi-structured interviews were also analyzed using descriptive analysis to generate vignettes. Different people observed the video recordings several times to understand how the social context, power dynamics, and cultural norms influenced HTN treatment/management. The transcribed video recordings were analyzed using discourse analyses.
While testing the statistical significance of differences between the baseline and the endline groups (n = 510 in each group) for all outcome measures, the chi-square test was used for categorical variables, and an unpaired t-test was used for continuous variables. We conducted multivariable regression analysis to adjust for potential confounders since the characteristics of the sample in the baseline and endline survey were not statistically similar. The linear regression model was used to estimate the beta coefficient and its 95% confidence interval (CI) for quantitative outcome variables. The binary logistic regression model was used for categorical outcome variables where adjusted Odds Ratio (aOR) and 95% CI were presented. A p-value <.05 was considered statistically significant.
Results
We integrated the qualitative and quantitative findings to develop, implement, and evaluate the intervention. The study commenced with a community consultation meeting, and training of volunteers followed by a baseline survey and then proceeded with awareness generation activities, vignette development, recording of patient journeys and re-orientation of healthcare staff, and finally endline survey was done. In the following section major findings of the qualitative component are presented, and the details are given in Supplementary File 1.
Community Consultations
The community voiced many issues, such as garbage dumps near houses, dirty water drains running through the village, non-availability of paved roads, schools, and outreach health services. The municipal authorities were trying to provide paved roads and save them from flash floods during rains. The main health issue discussed in these meetings was frequent headaches, which led to a discussion about hypertension. While most people were aware of diabetes, they knew little about hypertension. People wanted to be healthy, but their knowledge about diseases and healthcare services was limited. Public health facilities were poor in their village. Moreover, at the health facility, the services were only available in the morning, which was also true after waiting for a long time. This arrangement led to wage loss as they worked in an unorganized sector with limited economic and social security. Most families used home remedies and consultation from local healers/quacks to save time and money. The following quotes illustrate their concerns:
“It is [quack’s clinic] closer to our home” (Echoed by most)
“Bengali [the quack] is here, ladies go to him for minor illnesses, it is easier for them. We are at work and sometimes get treatment from nearby dispensaries” (Male-1)
This place is nearby, so when we fall ill at night, we come here [quack]. (Women-2)
I feel better only with his treatment. He gives affordable medicines. The Bengali doctors provide services to all newborns and old age people, so everyone goes to them (Women-4)
The outreach health workers were unavailable in the village most of the time and would visit the village only for mother and child healthcare. Although people had limited access to government health facilities, they wanted to improve their living and health conditions.
Community members suggested having adolescents as volunteers who had completed school and would be a better fit for awareness generation activities. They suggested various methods of interacting with the community, of which, they preferred group sessions for building their capacity for disease management. They identified leaders and volunteers from the community who were interested in participating in the intervention activities.
Vignettes
Using semi-structured interviews with the community, we developed the following vignettes, which represent the eight health literacy clusters, that is, sub-groups of the population with specific sociodemographic and health literacy characteristics (Passi et al., 2023) (Table 2).
Vignettes and the Recommended Solutions.

Patient Journeys
The video recordings of patient journeys in the health facility were observed several times by different people to understand how the social context, power dynamics, and cultural norms influenced HTN management.
Social Context
The healthcare setting primarily caters to a population with a low socioeconomic status, and this context significantly influences the interactions between patients and healthcare providers. Despite familiarity with the environment, patients often lack confidence when engaging with the medical staff. The most pressing issue appeared to be overcrowding, which left many feeling overwhelmed and disconnected. Additional challenges included knowledge and socioeconomic status disparities, which likely hindered meaningful engagement with doctors, nurses, and pharmacists. For example, patients rarely initiated conversations or sought clarification about their treatment, even when they did not fully understand instructions regarding medication, diet, or lifestyle changes. This hesitation may stem from an internalized power dynamic, where patients felt disempowered to ask questions.
Power Relations
A clear power imbalance existed between the patients and the healthcare providers. Service providers’ communications, use of technical language, gestures, and body language were often intimidating. Patients, because of their poor literacy and position in the social setting, seemed unsure, avoided eye contact, and stood behind nurses if their questions were not answered or responses were not understood by them.
The interactions between the patients and the pharmacist further illustrated this hierarchy. The pharmacist, preoccupied with stock maintenance duties, provided hurried instructions, and patients had to wait longer for their medication. When patients did finally receive their medication, the pharmacist often wrote unclear instructions on paper strips, leaving the patients to navigate their medication adherence with little support.
Despite the power dynamics, patients were familiar with the health facility, which increased their comfort level while visiting for follow-up. Patients’ deference to authority and limited engagement could also be due to a lack of trust in the healthcare providers’ competence.
Cultural Practices
The doctors mostly were seated comfortably on the chair in authoritative posture and often did not respond to greetings of patients, while most patients seated on a stool with slumped shoulders and folded hands would always first greet the doctor. We observed that the patients were to follow the protocol to maintain physical distance. If forgotten, doctor strongly instructed patients to sit at a distance to ensure physical distancing without considering the communication challenges due to language, tone, or low voice.
Patients presented their OPD cards to doctors and tried to explain their symptoms. However, doctors often were busy reading the previous history and sometimes gave instructions briefly, sometimes blaming the patient for not following the prescription, like medication adherence. During the videography, we observed similar situations several times. The doctor was not trying to understand the barriers to medication adherence. Most importantly, the doctor did not explain how much, when, and for how long patient had to continue the medicines. The patients were not able to continue the medicine for two reasons. One, they were not explained that it is lifelong, and secondly, with little relief in symptoms, they would stop medicine to save money.
The doctors were most often from different states and spoke different languages. This often created an additional layer of disconnect, making it harder for patients to ask questions or express their concerns. While doctors were not spending sufficient time to satisfy patients, patients were not asking questions, even when the doctor did not communicate critical details such as medication timings, dietary instructions (e.g., salt intake), and risk factors.
Intervention Evaluation
Baseline pre-intervention and endline post-intervention surveys were conducted on a sub-sample of the village population to evaluate the effectiveness of the intervention. In contrast, we implemented intervention activities (Table 1) in the entire adult population of the village in four PAR cycles (Figure 1).
Sociodemographic Characteristics
The sociodemographic characteristics of baseline and endline groups are presented in Table 3. Of the 510 adults sampled in the baseline survey, 59.2% were women. Most participants (70.3%) were below 40 years of age. Almost half (47.2%) belonged to scheduled castes. Over one-third were illiterate (35.1%), and 3.8% had a college or university education. The endline sample was similar to the baseline in terms of gender, age, caste, and education levels, but significant differences in religion, occupation and migration was observed.
Sociodemographic Characteristics of Baseline (N = 510) and Endline Groups (N = 510).

Migrants from Rajasthan, Madhya Pradesh, Jharkhand, and Orissa.
Health Literacy
The health literacy scores of the baseline and endline groups are presented in Figure 2. The scores of most of the scales were significantly higher among participants of the endline group compared to the baseline group (beta range 0.17 to 0.76, p < .01), except for scale 6, where mean scores were high (3.7 out of 5) at baseline and remained similar in the endline group. These findings did not change even after adjusting for age, gender, education, occupation, income, religion, caste, and migration status.

Comparison of health literacy scores between baseline and endline groups.
Hypertension Knowledge, Practices, and Risk Factors
The mean score of hypertension knowledge increased significantly from 2.9 (SD 2.7) in baseline to 3.4 (SD 2.9) in the endline group (β 0.76; CI 0.41 to 1.1; p < .01). Preference for taking less salt and less oil in the diet increased significantly from 6.4% to 59.4% and 20% to 70%, respectively (p < .01), but the practice of weighing regularly (at least once a year) did not change significantly from baseline to endline (2.7% to 3.7%, p > .05).
Total energy intake reduced from 2,063 to 1,702.1 Kcal/day (p < .01) in the endline group. Carbohydrate consumption reduced from 332.7 to 240.8 g/day (p < .01). Reduction in protein consumption (60.8 to 49.7 g/day) (p < .01) was also observed. Consumption of saturated fats decreased from 20.8 to 10.1 g/day (p < .01.) Average salt consumption decreased from 6.9 g/day to 5.4 g/day (p < .01), but there was no change in potassium intake (2.1 to 2.2 g/day) (p > .05). The recommended salt intake (<5 g/day) improved from 28% to 44.7% (aOR 0.47, 95% CI 0.36 to 0.6, p < .01) (Table 4).
Hypertension Risk Factors in Baseline and Endline Groups.
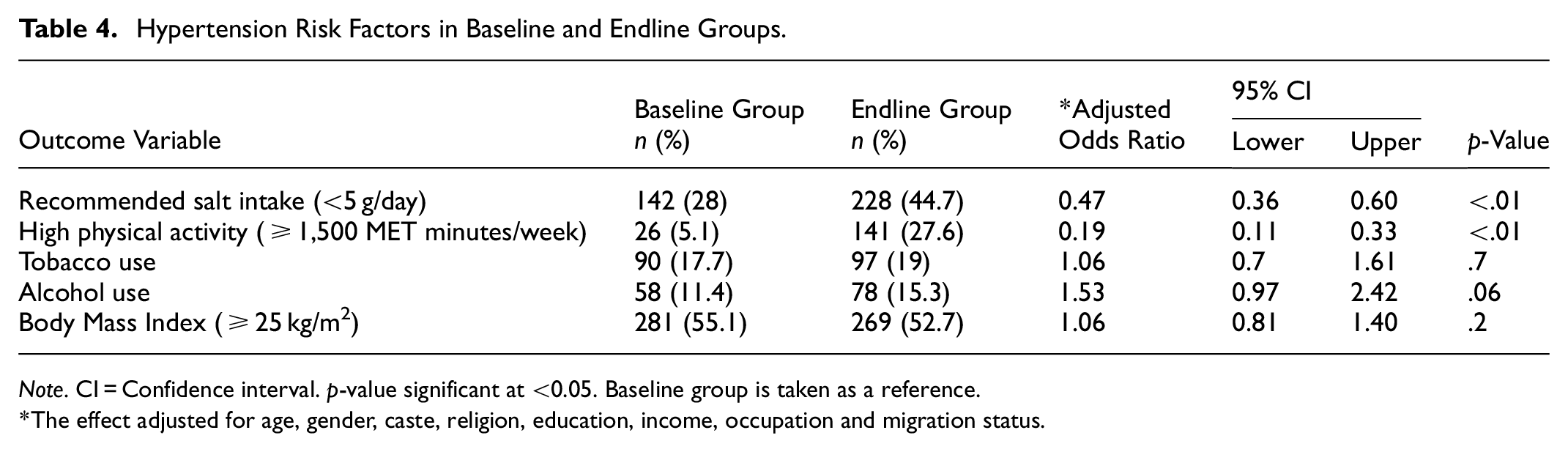
Note. CI = Confidence interval. p-value significant at <0.05. Baseline group is taken as a reference.
The effect adjusted for age, gender, caste, religion, education, income, occupation and migration status.
High physical activity (≥1,500 MET minutes/week) was reported among 27.6% of the participants in the endline group as compared to 5.1% in the baseline group (aOR 0.19, 95% CI 0.11 to 0.33, p .01). There was no difference in tobacco and alcohol consumption (Table 3). The BMI (aOR 1.06, 95% CI 0.81 to 1.40, p .2) and WHR (aOR 1.1, 95% CI 0.74 to 1.62, p .6) were similar in baseline and endline groups (Table 4).
Management of Hypertension
Among known cases of HTN (n = 79 in baseline and n = 74 in endline groups), 93.3% (95%CI 87.6% to 99%) were on treatment in the endline, which was significantly higher (p < .01) than the baseline group (72.2%; 95% CI 62.3% to 82.1%). The follow-up for HTN treatment in the past month increased from 12.6% (95%CI 5.2% to 19.9%) in baseline to 43.2% (95%CI 31.9% to 54.5%) in the endline group (p < .01). The medication adherence (score 7–9) improved from 5.1% to 33.8% (aOR 0.08; 95% CI 0.02 to 0.32 p .01), and the control of blood pressures (below 140/90 mmHg) increased significantly from 10.1% to 25.7% (aOR 0.28; 95% CI 0.08 to 0.94; p.04) (Figure 3).

Hypertension management practices.
Community Capacity
The community capacity in various domains was measured after intervention implementation (Figure 4). Each domain was scored from 1 (low) to 5 (high). Participation of the community in leadership, planning, and management of the intervention process, and learning and skill development was good. Government dispensaries and a mobile clinic were taken into the loop to provide screening and treatment for HTN. However, private doctors could not be involved fully, so the community scored low on partnership. The community actively provided volunteers, facilities, and time for intervention but could not arrange funding, so the score was low in resource mobilization. The community was involved in process evaluation and planning activities, but the community did not determine the indicators of success.

Community capacity following participatory action intervention.
Discussion
This study highlights the effectiveness of participatory action research, utilizing the Optimizing Health Literacy and Access (Ophelia) approach, in building community capacity to design and implement interventions to improve health literacy and access to hypertension management services. In most of the health literacy scales, the scores had improved, and better hypertension control was achieved in the community. The maximum increase had occurred in the scores for health literacy scale 3—“actively managing my health”; however, the scores of scale 6—“ability to actively engage with healthcare providers”—did not improve as these scores were already high (3.7 out of 5) at the baseline.
The health literacy questionnaire used in our study has not been used in India previously. Therefore, health literacy levels of this study are not directly comparable to previous Indian studies. Low health literacy levels have been reported in India (Rathnakar et al., 2013), as observed in the present study. Our study’s mean health literacy scores ranged between 1.80 and 3.12, aligning with the findings from an Egyptian study (Anwar et al., 2020). Health literacy scores were much higher in high-income countries (HICs), ranging between 2.71 to 3.98 (Bakker et al., 2021).
The increase in health literacy across multiple scales in our study aligns with a similar intervention targeting chronic disease management in Indigenous populations in Australia, where participatory approaches improved health literacy across various domains (Muscat et al., 2019). A study in Iran that focused on empowering participants to promote health literacy on heart health had positive outcomes after 1 year (Akbari et al., 2019). These studies indicate the effectiveness of health literacy in achieving better health outcomes in diverse cultural contexts.
The COVID-19 pandemic may have impacted health literacy in our study, as opportunities for interaction with healthcare providers including community health workers were restricted due to their involvement in the pandemic control activities. Improvement of only 0.2 points was observed in the scale “feeling understood and supported by healthcare providers,” and “appraisal of health information.” It is plausible that these scores would have improved more significantly under normal circumstances. Others have reported improvements in some but not all health literacy scales (Banbury et al., 2020).
The study observed significant improvement in hypertension knowledge, and dietary practices also indicated a positive shift, with a marked increase in the preference for consuming less salt and oil. However, the reduction in energy intake might have been due to decreased household purchasing power during the COVID-19 pandemic. A study from Bihar state reported reductions in the consumption of fruits, pulses, and cereals by 27%, 25%, and 21% respectively, during the pandemic (Travasso et al., 2023).
In our study, weight monitoring remained low, potentially due to the lack of weighing facilities in the village, which highlights a limitation in the intervention’s reach. In contrast, a health management project in Korea demonstrated improvements in health-promoting behaviors, including weight management, following a similar intervention (Kang et al., 2018).
Although there were improvements in treatment uptake (72.2% to 93.3%) and follow-ups (12.6% to 43.2%) in our study, fear of COVID-19 infection during the pandemic and restriction of movements may have limited the follow-ups and hindered treatment initiation among hypertensive patients. Less significant improvements in these parameters were reported in another study during the COVID-19 pandemic (Karagiannidis et al., 2023).
The proportion of hypertensives who had high medication adherence in our study increased significantly from 5.1% to 33.8% (p < .05). This improvement is in line with findings from a study in Thailand that used PAR with co-design and family involvement to enhance medication adherence among older adults with hypertension (Perngmark et al., 2022). The improvement in hypertension control from 10.1% to 25.7% (p < .05) in our study is like a community-based study in rural Kerala, which reported improvement in hypertension control from 6.5% to 21.7% after the implementation of interventions with the support of community volunteers and health workers (Balagopal et al., 2012; Thankappan et al., 2013)
Knowledge, motivation, and confidence are essential for adhering to medication. At the same time, poor healthcare services, lack of good patient-provider relationships, and training of healthcare providers are also responsible for poor adherence (Lee et al., 2017). The price and availability of drugs are other reasons for non-adherent behavior (Morgan & Lee, 2017). Studies from LMICs reported a 35% to 40% decline in anti-hypertensive medicine adherence during the COVID-19 pandemic (Abdisa et al., 2022; da Luz Pádua Guimarães et al., 2022). A study from a developed country has also observed decreased adherence post-pandemic (Gómez-Escalonilla Lorenzo et al., 2023). The negative impacts of the COVID-19 pandemic may have kept adherence at a low level (33.8%) in the present study.
The remarkable improvement in physical activity levels in our study might reflect the effect of COVID-19 pandemic. Due to economic loss during the lockdowns, people might have taken up more physically demanding jobs and the nature of their daily tasks may have changed accounting for the higher levels of physical activity.
Despite these successes, some behaviors, such as tobacco and alcohol use, did not improve because the focus of the intervention was primarily on managing hypertension rather than preventing it. Moreover, there was a lack of support systems such as de-addiction services near the community. This contrasts with findings from a Korean study where smoking rates dropped significantly post-intervention (Kim & Lee, 2020). On the other hand, several global studies have reported that pandemic-related stress and uncertainties have led to a rise in tobacco and alcohol consumption among populations (Ramalho et al., 2021; Roberts et al., 2021).
Unlike hypertension, other chronic diseases like Parkinson’s disease or Cataract may not follow similar pathways and outcomes. However, there is evidence from similar community-based participatory interventions on diabetes, cardiovascular diseases, and cancer screening where participatory research interventions have worked effectively in improving the health outcomes (Adsul et al., 2024; Campbell et al., 2020; Maharani, 2022; Thomas et al., 2022).
A community-based participatory research intervention in rural Gujarat for diabetes prevention and management reported a reduction in blood glucose levels by 14 mg/dL after 6 months, achieved through health education delivered by trained community health workers. Ekjut trials using participatory learning and action to improve MCH among Scheduled Tribe (ST) women in Jharkhand and Orrisa have demonstrated the effectiveness of group-targeted interventions over 2 years (Rath et al., 2010). However, in these trials, community involvement in decision-making was restricted, and participation was limited to intervention activities. This is a significant difference from our study that emphasized community co-design, offering a deeper level of engagement and ownership at various levels.
Many studies in the USA and Europe that adopted participatory approaches to promote health among children and adolescents have reported positive outcomes, with intervention periods ranging from 6 months to 4 years. These studies highlight the importance of robust quantitative outcome measurement, which aligns with our study’s findings, but they also suggest that extended timelines could yield even more impactful results (Benjamin Neelon et al., 2015; De Silva-Sanigorski et al., 2010; Kronish et al., 2014; Subica et al., 2016).
Unlike studies from HICs, where healthcare systems are more robust and community health initiatives are often better funded, in low-income or low-middle-income countries (LMICs), economic constraints, lower levels of infrastructure, and limited access to resources pose major challenges. We had to face many challenges viz, poor connectivity of the village to the urban area (part of village connected through an old bridge over a sewage carrying water stream), floods in the village in monsoon season, lack of paved roads, lack of space to carry out training of volunteers and awareness sessions for people, low education levels, less availability of community members as mostly men were daily wagers, inadequate financial resources for payment of honorarium to volunteers and helpers leading to dropouts and retaining of volunteers, lack of outreach healthcare, and inadequacy of anti-hypertension medicines in the health facility. To address these challenges, the researcher made multiple visits to the community and health facility to build rapport with the community. After a long time, community mobilization was enough to persuade the local councilor to get the roads paved in some village areas. Researcher approached non-governmental organizations, and they agreed to supplement the supply of medicines, sanitizers, masks, and gloves.
The COVID-19 pandemic weakened community engagement. Frontline health workers such as MPHWs and AWWs, who are vital links between the community and the health system, were more engaged in the pandemic-related duties. Additionally, we could not bring together key stakeholders—such as government and private service providers, political leaders, administrative officials, and community members—on a single platform because their priorities were redirected to pandemic control. Despite these challenges, engagement with community leaders and volunteers was maintained. However, with restrictions on large gatherings of people, we had to shift from group interactions to one-on-one engagements. In our study, these weaknesses were revealed in the domain of “partnerships” and “resource mobilization,” which were likely influenced by the challenges posed by the COVID-19 pandemic.
It is difficult to attribute observed changes in the outcome to the intervention as in this pre-post evaluation design there was no parallel control group. However, consistent improvements observed in this study along the pathway from generic health literacy to specific knowledge about hypertension, practices related to its risk factors, and adherence to treatment are likely to have led to improvements in hypertension control (Figure 5).

Health literacy intervention-outcome pathway.
We also compared our findings with data from the National Family Health Survey (NFHS)-5 for Chandigarh conducted in 2019–2021, a similar time-period to when we conducted the endline survey. We found that the percentage of men with normal BP increased more in our study (by 2.1%) compared to the NFHS-5 report (by 0.5%), suggesting a positive impact of these community-based health literacy interventions (MoHFW, 2021).
The study selected baseline and endline samples of pre-post evaluation as independent random samples from the same village before and after intervention implementation. We included all adults from the sampled households in the study, which may have affected the evaluation as behaviors tend to be similar within a household. We also found significant differences in the occupation, religion, and migration status in the baseline and endline samples. The large-scale movement of migrant workers during the COVID-19 pandemic may have led to these differences in the population characteristics of the village, primarily inhabited by migrants from other states of India who were working as laborers in the city. To draw accurate conclusions about the impact of the intervention on the study outcomes, the study employed multivariable regression analysis to account for the potential confounding effects of these variables. Due to the COVID-19 pandemic, intervention could be implemented only for six months, a relatively short period which was insufficient for addressing the deeper systemic issues related to policies. Therefore, we do not have sufficient evidence to claim empowerment, a fundamental outcome of PAR and a complex concept rooted in multiple social determinants. Additionally, due to the COVID-19 pandemic, healthcare workers were not able to do routine community awareness sessions, preventing the measurement of the impact of training imparted to Anganwadi Workers (AWWs) and Multipurpose Health Workers (MPHWs), and volunteers were selected with school educational, which restricted the inclusivity.
Overall, the unique contribution of our study lies in its application of participatory action research methods with Ophelia in a low-resource marginalized community. Designing need-based intervention activities using quantitative and qualitative data, and process evaluations helped develop a participatory framework for intervention development, implementation, and evaluation. Community members were engaged in research, starting with identifying the barriers to intervention development, implementation, evaluation, baseline, and endline surveys, and even data entry to some extent. Fran Baum used participatory approach (Baum et al., 2006) with Aboriginal Communities of Australia for behavior change and better health outcomes; Lemstra and Roger (Lemstra & Rogers, 2015) have demonstrated the importance of community consultation and social support in improving adherence to an obesity reduction program. Community consultation meetings provided the opportunity to listen to the voices of underserved populations and understand their perspectives. Through consultation, the researchers could identify key cultural practices and barriers to managing hypertension, such as trust in traditional healers, lack of BP monitoring services in the village, lack of relevant health information sources, and limited knowledge of the disease. These insights made the intervention more culturally sensitive and community-driven, significantly improving participation and health outcomes. Community consultations were essential components in shaping the intervention to improve pregnancy and newborn health among the rural poor in India (Acharya et al., 2015), and peer-support models were effective in improving health outcomes in hypertension and diabetes management (Thankappan et al., 2013).
Semi-structured interviews in developing vignettes provided deep, context-specific insights into health literacy challenges and strengths. It offered a personalized perspective on hypertension management. The vignettes, which represented distinct health literacy clusters, provided varying degrees of awareness and ability to manage hypertension, ranging from complete ignorance to partial knowledge but ineffective adherence to prescriptions and therapies. Barik & Thorat (2015), in their study, mentioned that individuals from lower socioeconomic backgrounds struggled to access consistent healthcare, where barriers such as long travel distances to health centers and unaffordable private healthcare echo similar observations (Barik & Thorat, 2015). Vignettes, therefore, enabled healthcare providers to develop targeted solutions addressing unique barriers (Batterham et al., 2016; WHO, 2022).
Instructions regarding medication and lifestyle modifications from medical officers and pharmacists reflect systemic gaps in health service delivery (Thankappan et al., 2013). Patient journeys provided a comprehensive understanding of the interface between patients and the healthcare system. Discourse analysis helped identify power relations and dynamics through verbal and non-verbal communication. It was more evident as the patients in the present study were from lower socioeconomic status and healthcare providers were from affluent families. Patients hesitated to seek clarification about their treatment, which could undermine effective hypertension management. Patient journey mapping helped identify gaps and inefficiencies. Using the journey maps for training healthcare providers, as suggested by our findings, aligns with global best practices for improving patient-provider communication in managing chronic diseases (Bulto et al., 2024).
Despite challenges, this study adds to the growing body of evidence that participatory action interventions using Ophelia can be effective in managing chronic conditions like hypertension, especially in settings with limited healthcare resources. In the future, researchers should use participatory action research (PAR) along with the Ophelia approach to create relevant solutions for marginalized groups and higher-income populations in urban areas for the comprehensive prevention and control of NCDs. Including more extensive preventive strategies and targeting younger age groups is important as most NCD risk factors take shape in children and adolescents. Therefore, health literacy should be a part of the educational curriculum of schools to inculcate healthy behaviors at early ages. Additionally, future research should allow for longer intervention periods for community engagement, build rapport, adapt intervention activities according to local beliefs and preferences, and involve more volunteers, particularly from lower socioeconomic backgrounds. Researchers should focus on prior collaborations for funding to compensate community members for spending their earning hours on intervention activities.
Since community participation is a core strategy of primary health care, governments must re-orient health services, particularly frontline healthcare staff such as community health officers, health workers, and community volunteers. They must train these personnel in participatory approaches such as Ophelia for planning and implementing need-based, culturally relevant activities to maximize the coverage of existing health interventions.
Conclusions
It is feasible to conduct participatory action research using local resources to build linkages between the community and health services. Optimizing health literacy and access (Ophelia) approach helped understand and address the specific needs of the population groups. Improving the health literacy of the village population helped reduce salt intake and improve physical activity, blood pressure treatment, and adherence to antihypertensive medication, leading to blood pressure control. Community members remained involved throughout, and the research process progressively enhanced their capacity in each participatory intervention cycle to act for their health.
At the program level, healthcare providers must receive training in the participatory action approach. Local governments should take initiatives that develop the skills of community members and leaders, enabling them to actively engage in community-wide health issues, including NCD prevention and control.
Supplemental Material
sj-doc-2-sgo-10.1177_21582440251339053 – Supplemental material for Participatory Action for Optimizing Health Literacy and Access to Manage Hypertension: Pre-post Evaluation in a Marginalized Community of India
Supplemental material, sj-doc-2-sgo-10.1177_21582440251339053 for Participatory Action for Optimizing Health Literacy and Access to Manage Hypertension: Pre-post Evaluation in a Marginalized Community of India by Reetu Passi, Manmeet Kaur, Madhu Gupta, Savita Kumari and Rajesh Kumar in SAGE Open
Supplemental Material
sj-docx-1-sgo-10.1177_21582440251339053 – Supplemental material for Participatory Action for Optimizing Health Literacy and Access to Manage Hypertension: Pre-post Evaluation in a Marginalized Community of India
Supplemental material, sj-docx-1-sgo-10.1177_21582440251339053 for Participatory Action for Optimizing Health Literacy and Access to Manage Hypertension: Pre-post Evaluation in a Marginalized Community of India by Reetu Passi, Manmeet Kaur, Madhu Gupta, Savita Kumari and Rajesh Kumar in SAGE Open
Supplemental Material
sj-xlsx-3-sgo-10.1177_21582440251339053 – Supplemental material for Participatory Action for Optimizing Health Literacy and Access to Manage Hypertension: Pre-post Evaluation in a Marginalized Community of India
Supplemental material, sj-xlsx-3-sgo-10.1177_21582440251339053 for Participatory Action for Optimizing Health Literacy and Access to Manage Hypertension: Pre-post Evaluation in a Marginalized Community of India by Reetu Passi, Manmeet Kaur, Madhu Gupta, Savita Kumari and Rajesh Kumar in SAGE Open
Footnotes
Acknowledgements
We sincerely thank the community leaders and volunteers without whom the intervention was not possible. We extend our gratitude to Prof Richard Osborne, Distinguished Professor, Centre for Global Health & Equity, La Trobe University, Australia, and his team, for their invaluable guidance in conducting Ophelia. We also acknowledge the contribution of Indian Council of Medical Research (ICMR) for financial support through a PhD fellowship to Reetu Passi.
Ethical Considerations
The study plan was approved by Institute Ethics Committee, Post-Graduate Institute of Medical Education and Research Chandigarh (INT/IEC/2019/000414; Date: 01/03/2019).
Consent to Participate
Informed written consent was obtained from all participants after briefing them about the study purpose, and confidentiality was maintained.
Trial registration
The study was registered under the Clinical Trial Registry of India (CTRI/2019/10/021827; 31/10/2019).
Author Contributions
Conceptualization: Reetu Passi, Manmeet Kaur, Madhu Gupta, and Savita Kumari. Data curation: Reetu Passi. Formal analysis: Reetu Passi, Manmeet Kaur, Madhu Gupta, and Rajesh Kumar. Funding acquisition: Reetu Passi, Manmeet Kaur, and Madhu Gupta. Investigation: Reetu Passi, Manmeet Kaur, and Madhu Gupta. Methodology: Reetu Passi, Manmeet Kaur, Madhu Gupta, and Rajesh Kumar. Project administration: Reetu Passi, Manmeet Kaur, and Madhu Gupta. Resources: Reetu Passi, Manmeet Kaur, and Madhu Gupta. Supervision: Manmeet Kaur, Madhu Gupta. Validation: Manmeet Kaur and Madhu Gupta. Writing—original draft: Reetu Passi. Writing—review & editing: Reetu Passi, Manmeet Kaur, Madhu Gupta, Savita Kumari, and Rajesh Kumar.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received financial support from the Indian Council of Medical Research (ICMR) in the form of a PhD fellowship awarded to Reetu Passi.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used in the current study are available in the Supplementary Excel File S3 data sheet.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.