
Abstract
Each country is expected to take care of its growing population. In Nigeria, the pre-requisite for adequate health care delivery are still unmet. Nigerians especially the elderly fall victim to the danger of death. The study seeks to explore psycho-social experiences and healthcare delivery for older adults in Nigeria. Quantitative and qualitative methods were used for data collection from 1,180 respondents, from seven villages in the community. Data were analyzed using content analysis, simple percentages, and chi-square. The study found that there is no healthcare delivery for the elderly, they underwent problems such as loneliness, isolation, and abandonment in healthcare delivery. The study recommends the intervention of the government which will enhance the conditions of the elderly.
Introduction
Psychosocial experiences of older adults and their healthcare have been one of the lingering problems facing Africa and Nigeria in particular. The provision and improvement of quality of care rendered to the elderly remain a key priority in realizing desired active aging. According to data from World Population Prospects: the 2019 Revision, by 2050, one in six people in the world will be over age 65 (16%), up from one in 11 in 2019 (9%). By 2050, one in four persons living in Europe and Northern America could be aged 65 or over. In 2018, for the first time in history, persons aged 65 or above outnumbered children under 5 years of age globally. The number of persons aged 80 years or over is projected to triple, from 143 million in 2019 to 426 million in 2050 (United Nations, 2019). According to World Health Organization (2013) “the aging population is due to increased life expectancy resulting from declining fertility and improved standard of life through medical technological advancement.” It has been estimated that “globally the number of elderly will increase to 1.2 billion in 2025 and subsequently to 2 billion in 2050 (World Health Organization, 2013; Ndabemi et al., 2014).” In developing countries in Africa, there is a rapid increase in the elderly population. The African Research on Ageing Network (2020) posits that “Sub-Saharan African countries have a more rapid increase than in any other world region and for any other age group projecting the absolute number of older persons to rise sharply from 37.1 million in 2005 to 155.4 million in 2050. Particularly in Nigeria, the elderly population is projected to be 11.5 million in 2025 and 25. 5 million in 2050 (United Nations, 2012a, 2012b).” The elderly encounter a lot of psychosocial problems when their needs are not met (loneliness, lack of security, poor feeding habits, health issues, and lack of finance) and these problems affect their healthcare delivery services and the healthcare system has not taken adequate care of these issues. The system needs specialists that can take care of older people. To Binumoyo and Ogansola (2016) “throughout history, humanity has been at crossroads on the issue of healthcare delivery, especially for the elderly.” Animasahun and Chapman (2017) also indicated that “changes in family dynamics, increased demand for healthcare services, increased economic stress, and decreased functional independence affect the psychosocial health status of elderly Nigerians.” Psychosocial health encompasses the multiple dynamic interactions between social and behavioral variables, the influence of these biological, psychological, and social factors on the aging process influences an individual’s well-being, quality of life, and health outcomes. These psychosocial experiences which translate to a perceived threat (especially those threats over which we have no control) to social status, social esteem, respect, and acceptance within a group may result in anxiety, depression, delirium, dementia, personality disorders, and substance abuse. Common social and emotional issues may also involve loss of autonomy, grief, fear, lowliness, financial constraints, and lack of social networks. These elderly persons need to be engaged and focused to be able to independently perform activities of daily living.
World Health Organization (2015), advocated long term care which includes: “the series of activities undertaken by others to ensure that individuals at risk of significant loss or with ongoing loss of intrinsic capacity can maintain a level of functionality that is consistent with their basic rights, fundamental freedom, and human dignity,” for active aging. Also as Kontis et al. (2013), in their review on the psychosocial experiences of older adults, indicated, “that the elderly are very sensitive to many psychosocial problems such as loneliness, isolation, and abandonment in healthcare delivery system.” Loneliness and social isolation are often overlooked, despite being vital public health concerns. Older adults experience severe feelings of loneliness, an independent risk factor for depression, anxiety disorders, and suicide (Gerst-Emerson & Jayawardhana, 2015; Li et al., 2020,). “The family members have the obligation of caring for their older adults; assist the elderly with performing activities of daily living and preventing falls (Blake, 2017).”
In developed countries, for instance, the U.S. government signed the first major health care reform (Affordable Care Act) into law nearly half a century (Madan, 2016), but in developing countries like Nigeria, as was noted by (Adebanjoko & Ugwuoke, 2014), Aging in Nigeria is occurring against the background of socioeconomic hardship, widespread poverty, the HIV/AIDS epidemic, and the rapid transformation of the traditional extended family structure. The current primary health system is unresponsive to the needs of the elderly, whose major disease characteristic is their chronicity. “The need to offer medical support to a situation that will not go away but whose neglect can lead to other damages, compromising the quality of time left or leading to untimely death. The situation is not much better at the secondary or tertiary levels of health care (Togonu-Bickersteth & Akinyemi, 2014).”
Irrespective of the efforts of the United Nations Principles for Older Persons Resolution 46/91 by the General Assembly in 1991 and the Madrid Plan of Action on Aging in 2002 to which Nigeria is a signatory (Edirin & Mudarie, 2013; Mudiare, 2013), also the Nigeria healthcare policy which was placed under the care of the three tiers of government, there is a low level of awareness on the psychosocial experience of the older adults and healthcare delivery. All these efforts were not meeting up with the challenges of the elderly. Their focus is on curative measures. Ayodeji (2015) asserts that most African governments have paid little or no attention to the socioeconomic security of their older adults. Human service administrators and policymakers still hope that families always care for their elderly and that they have not shown any serious interest in aging issues like the healthcare delivery system (Okoye, 2013). The study carried out by Eniola (2020), it reveals that long-term care provisions for older persons in both rural and urban communities must preferably facilitate their ability to “Age in Place” within their homes or communities. Pension is the only welfare package for the elderly but it was meant only for those who have worked and retired as civil servants and because it is not generalized, very few are getting the benefit. Also in the area of housing, in most developing countries, including Nigeria, the government does not provide housing for the elderly; they mostly live with their children in the villages and sometimes in the cities. The government’s attitude is that families should provide care for the aged and this is reflected in the non-provision in the budget for the elderly. Although caring for a loved older adult can be very rewarding, the problems of urbanization and the search for white-collar jobs have deprived older adults of these privileges. The elderly as a matter of urgency needs the expertise of healthcare professionals to be accessing adequate healthcare. Thus, the need arises to direct the attention of individuals, families, society, NGOs, and the government to the psychosocial experiences of the elderly and their healthcare delivery, to create and sustain preventive and intervention strategies or programs that will assist and benefit all in the society. Implementing a draft aging policy to address the psychosocial experiences of older adults and their health concerns is very important. This will enhance and contribute to relieving the psychosocial conditions of the elderly Hence, a study of this nature on the psycho-social experiences and healthcare delivery for older adults in Nigeria becomes important at this time to identify and proffer possible ways of handling the psychosocial experiences of the elderly and their healthcare services.
Theoretical Framework
The theoretical frameworks adopted for the study are the Theory of Planned Behavior by Montano and Kasprzy (2008) and the Forced Compliance Theory by Festinger and Carlsmith (1959). According to the first theory, “attitudes toward behavior are shaped by beliefs about what is entailed in performing the behavior and the outcomes of the behavior. Beliefs about social standards and motivation to comply with those norms affect subjective norms. The presence or lack of things that will make it easier or harder to perform the behaviors affects perceived behavioral control.”
This theory is applicable in this study in that the health workers’ intentions and beliefs are what influence their behavior and attitudes. The demographic factors and the resources available have a role to play in the outcome which is the result of the health workers’ care for the elderly. A health worker’s perception of norms and beliefs, that is knowledge of the health worker on the care of the elderly, build-up his intention and this is what influences the health worker’s attitude and practice of care toward the elderly.
The second theory used in this study (Forced Compliance Theory), posits that people in higher authority or rank can force the lower-ranked ones to make statements or actions that violate their judgment. This implies that the attitude of those in lower-ranked positions can be altered or changed through persuasion and authority by the higher-ranked officers. Since the attitudes of public healthcare delivery personnel are not always cordial, using this theory, they can be called to order by imposing change on them for better and adequate care of the elderly.
Cooper and Faizo (1984) outlined four steps that can lead to change, namely:
The attitude must produce negative consequences, for example, from the literature reviewed above; the attitude of public health workers to the elderly is most of the time negative.
If you choose to behave negatively, then you will feel responsible and have dissonance. Negative behavior results in a lack of agreement, if someone forces you to behave negatively then you will not have dissonance, there will be agreement.
According to Festinger, a negative attitude leads to discomfort for the person and also affects him or her psychologically.
The people (for instance health personnel) are aware that their behavior is normally accompanied by dissonance. This implies a lack of agreement between the nurses and their super-ordinates.
In looking at the experiences of the elderly in health care delivery, when the negative attitude of health personnel is changed to a positive attitude it shows that the elderly compliance rate utilizing health care is dependent on the attitude toward compliance of health workers care in the hospital. These two approaches are indeed appropriate for the study because they stress the need for all possible solutions to be adopted in taking adequate care of the elderly.
Statement of the Problem
In developed countries, “health care is often provided by well-equipped public health facilities and nursing homes designated for elderly individuals, (Chukwudi et al., 2015). For instance, in the United States, older adults have a higher frequency of primary care visits of 50% hospital consultation, 80% home care services, and occupy 90% of all nursing home beds.”
Presently, “the idea that old-age security and well-being in Nigeria should remain the primary responsibility of the family is untenable” (Wahab, 2013). The health systems lack policies that can enhance adequate provision and utilization of healthcare services by the elderly population who are the poorest group in society, especially those who are not on pension. “With the gradual collapse or breakdown of the extended family system in Nigeria, the elderly persons no longer enjoy the care and support of the family members and relatives as was the case in traditional Nigerian society (Clarke & Bennett, 2013; Edeh, 2014).” This is evident among the women who had the primary responsibilities of caring for the elderly, who reported that the care of the elderly has become more difficult as more and more women are becoming educated and taking up different employments exposing the elderly to challenges of various dimensions.
Urbanization and modernization have disrupted the nuclear family system and have increased the psychosocial experience of older adults and healthcare delivery as most families move to the cities in search of white-collar jobs. In these rural communities, the aged resides alone in one room unable to go out because of a certain ailment, and are always lonely. This can complicate their health conditions and often results in death which could have been averted. In the area of study, the children resort to allowing some of their grandchildren, especially those who are out of school to stay behind in the village to be looking after the older adults, but when those children gain admission or enroll in apprenticeship, the older adults will face many challenges. In this situation, the married daughters will be visiting their old parents for assistance, these adults are not used to external caregivers (nannies) who can live with them and keep them company.
The pervasive misconceptions, attitudes, and assumptions about older people by healthcare providers have been an important barrier to developing good public-health policy on aging (Eklund & Wilhelmson, 2015). The attitude of health care providers towards older adults stereotypes them as chronically ill, unable to work, instability, incontinence, slow thinking, and financially useless burden in the society and this seems to make them lose their potential and validity. These negative attitudes of healthcare providers can become an obstacle to training skilled elderly healthcare workers. Efforts have been made to improve the healthcare delivery system for the elderly, but their psychosocial experiences have been virtually ignored. For instance, in America, government programs provide money at best that substitutes for caring and loving elderly families (American Attitudes Towards the Elderly, 2014). The cultural individualism of the western attitude toward the psycho-social experiences of the elderly is relatively positive. Nigeria did not take cognizant of understanding the psychosocial conditions of the elderly and their healthcare. The older adults in Enugu’s north senatorial zone lack the organization of health services that address active aging and utilization of health services. The inability of the health system to address these issues while health-related problems are inevitable in old age has remained a threat to the idea of healthy aging. With a collapsing extended family in Nigeria, these elderly persons no longer enjoy the care and support of family members and relatives as was the case in traditional African society, thereby exposing them to challenges of various dimensions (Omorogiuwa, 2016). These situations aggravate the psychosocial conditions of the elderly. These relatives resort to insulting, name-calling, intimidating jokes made to ridicule the older person, indifference affecting the person’s mental well-being and threatening the individual with isolation and neglect, and deliberately not talking to the older person, which is called the “silent treatment” or “keeping malice” The study explores the psychosocial experiences of older adults and their healthcare that has not been adequately addressed in the literature on such issues as it relates to the availability of public healthcare, the level of public awareness of the existence of healthcare delivery, the level of accessibility, the state of public healthcare delivery, the attitude of caregivers and other psychosocial factors on older adults in the area of study to create and sustain a preventive policy that will address the older adults health concerns as it obtains in a developed country.
Method
Validation and Reliability of Instrument
The instrument was reviewed and validated by three professionals. These professionals were selected from the field of Sociology and Social work. These specialists were selected based on their knowledge and understanding of the research area. Similarly, to determine the reliability of the instrument, the questionnaire was tried in a pilot study of 1,180 respondents. The data for the reliability test was collected by the researcher and the internal consistency of the instrument was determined by Cronbach’s alpha reliability coefficient. The choice of Cronbach alpha reliability coefficient was informed by the fact that the questionnaire items were mostly of multiple response types and it provides for a more stable measure of homogeneity as was stated elsewhere in Nwokocha and Madu (2020) Consequently, the analysis of this study showed a Cronbach alpha reliability coefficient of 0.82. The score obtained revealed that the questions in the questionnaire are consistent with the subject.
Results
Socio-Demographic Characteristics of the Respondents
We explore the psycho-social experiences and healthcare delivery for older adults in Nigeria. Table 1 below reveals the age, sex, and level of education, occupation, income, number of children, and who cares for them. The socio-demographic characteristics were tabulated as can be seen below.
Distribution of Respondents by Socio-Demographic Variables and Place of Residence.

Author’s Computation, 2019
In Table 1 above, the distribution of respondents by sex and place of residence shows that among rural residents, 53.5% are males while 46.5% are females. Among urban dwellers, Table 1 also shows that 47.2% are males while 52.8% are females. Meanwhile, among residents of semi-urban areas, 47.2% are males while 52.8% are females.
On the level of education, among the rural dwellers 14.0% have no formal education, followed by 20.0% who attend primary education, then 42.2% who attend secondary education, and lastly also the rural dwellers 23.8% attend tertiary education. Among the urban dwellers, 54.8% do not have formal education while 30.6% attend only primary education, 10.2% attend secondary school, and lastly, only 4.3% went to a tertiary institution. Looking at the table also, of the respondents in the semi-urban, 10.6% have no formal education, 50.5% attend primary school, 31.7% attend secondary school, and lastly, only 7.2% went to higher institutions.
The occupational category and place of residence show that in the rural residents, 14.0% are unemployed, 33.8% are Business people, 25.8% are farmers, 8.5% are artisan, and lastly, 18.0% are the retirees. Of the respondents in urban residents, 27.6% are unemployed, 30.4% are business people, 32.1% are farmers, 4.3% are artisans and 5.6% are retirees. Of those respondents in semi-urban residents, 1.8% are unemployed, 79.4% engage in business, 2.3% are farmers, 13.9% are artisans and 2.6% are retirees. Those who engage in business have the highest number of respondents, 47.6%.
From the above table, distribution by several children and place of residents, among the rural dwellers, 3.2% do not have children, 54.2% have 1 to 4 children, 42.0% have 5 to 8 children and only 0.5% have up to 9- above several children. Among the urban dwellers, 3.8% do not have children, 36.2% have 1 to 4 children, 42.6% have 5 to 8 children and 17.3% have a 9-above number of children, For the semi-urban dwellers, 6.2% do not have children, 53.9% have 1 to 4 children, 38.7% have 5 to 8 children and lastly only 1.3% have 9- above several children.
The monthly income shows that of those who live in rural communities, 42.5% earn less than 18,000 in a month, 35.2% earn between 18,000 and 44,000 per month, 7.8% earn 45,000 and 75,000 per month and 14.5% earn up to 76,000- above in a month. For the urban dwellers, 80.9% earn less than 18,000 in a month, 5.4% earn between 18,000 and 44,000 per month, followed by 12.0% who earn between 45,000 and 75,000 per month, and 1.8% earn between 76,000 and above. Lastly, for the semi-urban dwellers, 38.9% earn less than 18,000 per month 49.2% earn between 18,000 and 44,000 per month, 9.0% earn 45,000 and 75,000 in a month and 2.8% earn 76,000 and above per month.
It can be observed in Figure 1 that 52% of the respondents in rural areas are within the age group of 60 to 69 while 48% are within the age group of 70 and above. On the other hand, respondents in urban areas have more respondents within the age category of 70-above (54.8%) than the age category of 60 to 69 (45.2%).

Distribution of respondents by age and place of residence.
Availability, State, and Accessibility of Public Healthcare Delivery
Here the adequacy of public healthcare delivery was examined to determine if the respondents make use of the healthcare facilities in the community or if they go after other facilities for their treatments.
Author’s Computation, 2019
The table above on the distribution by places they go for treatment and sex, among those who go to the traditional healers, 45.5% are males while 54.5% are females, those who go to Pharmacy /chemist shop, 47.4% are males while52.6% are females, those who go to private hospital/clinics, 45.3% The above table shows the distribution of respondents by places they go for treatment and level of education. Of the respondents who said that they go to traditional healers, 22.1% have no formal education, 40.4% attend primary school, 32.8% attend secondary school and 4.7% went to a tertiary institution. Of those who go to pharmacist/chemist shops 38.1% have no formal education, 37.9% attend primary school, 20.4% attend secondary school and 3.6% went to a tertiary institution. Of those who go to private hospitals/clinics, 31.3% have no formal education,28.0% attend primary school, 26.7% attend secondary school and 14.0% went to tertiary institutions, those who receive their treatment from government hospitals/clinics 14.7% have no formal education, 26.2% attended primary school, 34.6% attend secondary school and 24.4% went to tertiary institution, and finally those who go to prayer houses, 34.6% have no formal education, 46.2% went to primary school,15.4% went to secondary school and 3.8% went to a tertiary institution. The distribution by places they go for treatment and the number of children. Of the respondents who said they go to traditional healers, 5.5% have no child, 51.9% have 1 to 4 children, 37.0% have 5 to 8 children and 5.5% have children from 9-above. Of those who said they go to pharmacy/chemist shops, 4.1\% have no child, 44.8% have 1 to 4 children, 42.5% have 5 to 8 children and 8.0% have children from 9- above. Of those who said they go to a private hospital/clinic, 4.7% have no child,44.7% have 1 to 4 children 42.97 have 5 to 8 children and 8.0% have children from 9- above, those who receive their treatment from government hospital/clinic, 3.7% have no child, 51.4% have 1 to 4 children, 40.7% and 3.9% have 9- above several children and finally, those who said that they go to prayer houses to receive treatment, 7.7% have no children, 34.2% have 1 to 4 children,50.0% have 5 to 8 children and 7.7% have children from 9- and above.
In the distribution by places they go for treatment and monthly income, among the respondents who said they receive treatment from traditional healers, 54.0% earn less than 18,000 in a month,36.6% earn 18,000 to 44.000 in a month, 7.7% earn 45.000 to 75.000 in a month and 1.7% earn 76.000-above. Of the respondents who said they receive treatment from a pharmacist/chemist shop,64.7% earn less than 18,000 in a month, 23.2% earn 18,000 to 44.000 in a month, 10.1% earn 45.000 to 75.000 in a month and 2.1% earn 76.000-above. Of those who said they receive treatment from private hospitals/clinics, 48.7% earn less than 18,000 in a month,28.0% earn 18,000 to 44.000 in a month, 17.3% earn 45.000 to 75.000 in a month and 14.2% earn 76.000-above, those who receive their treatment from government hospital/health centers, 44.9% earn less than 18,000 in a month,33.6% earn 18,000 to 44.000, 7.3% earn 45.000 to 75.000 in a month and 26.9% earn 76.000-above, and lastly those respondents who said they receive treatment from the prayer houses, 61.5% earn less than 18,000 in a month, 33.5% earn 18,000 to 44.000, 7.7% earn 45.000 to 75.000 in a month and 3.8% earn 76.000-above.
Figure 2 captures different reasons why respondents choose different health centers. The most mentioned reason (40%) is closeness to one’s house and it is followed by being taken to the place (32%). Furthermore, the availability of specialists is another reason as indicated by 14% of the respondents as well as cheapness and being on health insurance with 9% and 6% respectively.
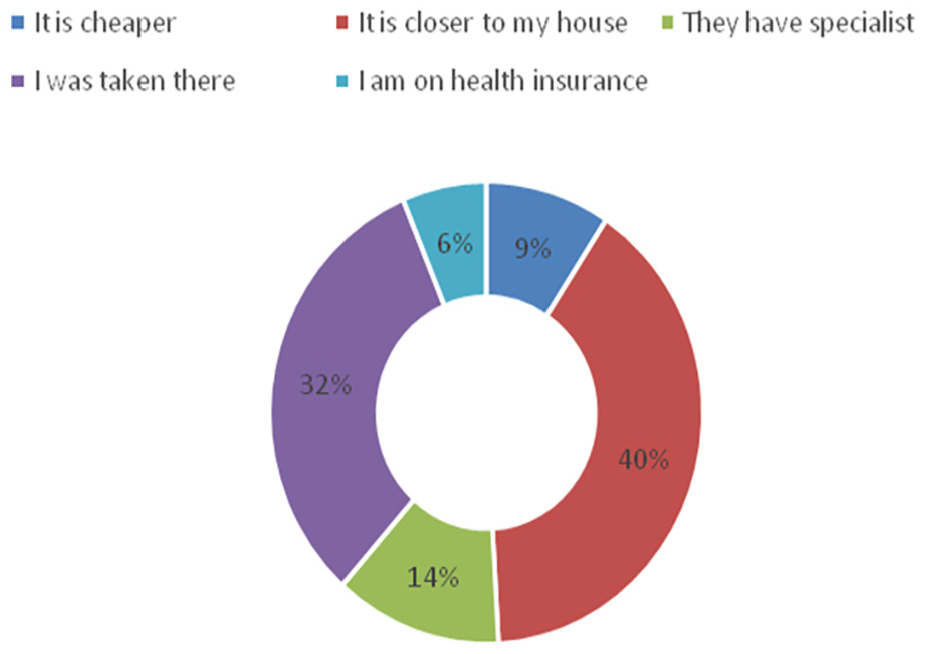
Distribution of respondents to ascertain the reason for choosing the health center.
Test of Hypothesis
Null Hypothesis (H0)
There is no relationship between the place of access to medical care and the extent of psychosocial problems
Alternative Hypothesis (H1)
Elderly persons who access medical care at private hospitals are less likely to encounter psychosocial problems than elderly persons who access medical care at public hospitals: Questions 14, 15, 16, and 17 were used to ascertain places of access to medical services and level of attitude of doctors and nurses in both private and public hospitals while questions 29, 30 and 31 were used to determine the experiences of the elderly when they are sick when they are in the hospital and among members of the family.
From Table 3, it can be observed that the place the elderly go for treatment, accessibility of healthcare, and extent of psychosocial problems was cross-tabulated. From the table, it could be seen that out of all the respondents who go to treatment at private hospitals/clinics, 74.0% have fewer psychosocial problems while 26.0% have a more psychosocial problems. On the other hand, out of all the respondents that receive treatment from a government hospital/health center, 61.7% have fewer psychosocial problems, and 38.3% have more psychosocial problems.
The chi-square test showed χ2 = 6.664 with a degree of freedom of 1 and a p-value of .010. This is lower than the significant level of .05. It indicates that the alternative hypothesis was accepted while the null hypothesis was rejected, that is there is a difference in place of healthcare services and the extent of psychosocial problems. In other words, an association does exist between where the respondents receive treatment and their psychosocial problems.
Discussion of Finding
Availability, State, and Accessibility of Public Healthcare Services
In the availability, state, and accessibility of public healthcare services for the elderly in the area of study, here all of the respondents indicated that there are no public healthcare delivery services meant for the elderly. This finding is in agreement with the statement by Togonu-Bickersteth and Akinyemi (2014) which states that the Primary Health Care system (PHC) is unresponsive to the needs of the elderly, whose major disease characteristics are their chronicity, this situation is also applicable to the secondary and tertiary level of healthcare. Table 2 on the distribution of respondents by places the elderly go for treatment and sex, the majority of the respondents receive treatment from prayer houses,65.4% and they are females, on the distribution of respondents by places they go for treatment and level of education, majority of the respondents who go to prayer houses to receive treatment (46.2%) attended primary school, on the distribution of respondent by places they go for treatment and number of children shows that majority of the respondents who receive treatment from traditional healers 51.9% have 1 to 4 children and lastly, on the distribution of respondents by places they go for treatment and monthly income, a greater percentage of the respondents go to treatment at traditional healers, 64.7% and they earn less than 18,000 per month. We can deduce that many of the elderly who access healthcare with traditional healers and prayer houses are within a low socioeconomic status. The government attitude is that the families should provide care for the aged and this is reflected in the non-provision in the budget for the elderly. The stress of modern life has led to the neglect of some older persons in society (Ayenibiowo et al., 2014). Binumoyo and Ogansola (2016) indicated that throughout history, humanity has been at crossroads on the issue of healthcare delivery especially for the elderly. The health ministry should provide policies and regulations meant to guide the implementation of healthcare. As was also indicated by Animasahun and Chapman (2017) changes in family dynamics, increased demand for healthcare services, increased economic stress, and decreased functional independence affect the psychosocial health status of elderly Nigerians. Although family members in the area of study engage in routine visits to provide for their older parents’ well-being, their material needs as well as their social support for maintaining kinship ties in the village, some also relocate their older parents to where they reside in the city to give them adequate care, all these depend on how they perceive the need to care for their older parents. The orientation regarding the family size and the accepted members involved passed unto most children nowadays is a strictly nuclear family system: consisting of the father, mother, and children, as obtained in most western countries. If their grandparents, older uncles, or aunties come around, they are not always well regarded as being part of the family, let alone their need to care for them. Omorogiuwa (2016), noted that with a collapsing extended family in Nigeria, these elderly persons no longer enjoy the care and support of family members and relatives as was the case in traditional African society, thereby exposing them to challenges of various dimensions.
Distribution of Respondents on Availability, State, and Accessibility of Public Healthcare Delivery and Socio-Demographic Variables.

These efforts by family members have not reduced the psychosocial experiences of older adults mainly because they are not used to life outside their home environments. Also, the way younger generations feel and act toward them may be attributed to a lack of understanding of the aging process and the characteristic of the elderly coupled with cultural beliefs whereby some manifestations of dementia are interpreted as witchcraft (Ayenibiowo et al., 2014). Gerst-Emerson and Jayawardhana (2015) and Li et al (2020) asserted that loneliness and social isolation are often overlooked, despite being vital public health concerns. Thus, there is a need for assistance in the state of public healthcare delivery in the area of study to create and sustain preventive and intervention strategies that will assist and benefit all the elderly in society. The provision of health facilities and trained health workers (Geriatricians) will be of utmost importance in surmounting the psychosocial experiences of the elderly and their healthcare delivery services.
Contributions of the Study to Knowledge
Many studies have been done on the psychosocial needs of the elderly and healthcare delivery but they did not focus on the low level of awareness of the experiences of older adults due to a lack of comprehensive research and government policy to address them. In the area of study, care of the elderly are left in the hand of family members and this aggravates their psychosocial experiences and healthcare services. There are inadequate health facilities in hospitals and no specialist doctors or hospitals for the elderly. The study found that the elderly resort to either alternative medicine for their healthcare and most of them confessed that it has not taken care of their age-related problems of the elderly. Some of the older adults also take care of themselves from the teaching they receive from village meetings, media, and churches but these places have not reduced the psychosocial experiences of older adults and healthcare delivery. The study has helped sensitization of researchers on the situation of public healthcare delivery for the elderly to remedy the situation by carrying out further research that will focus on the psychosocial experiences of older adults and their healthcare delivery.
The study also found that primary healthcare providers with teeming clinic attendance are unable to provide adequate healthcare, education, and support services to older persons due to limited or no institutionalized care for the elderly, as can be seen in the study there are no guitarists that can provide such services as they are trained for such purposes. The lack of up-to-date equipment in public hospitals and little or no action by the government on improving the state of the health sector enhances the psychosocial experiences of older adults. There are no budgets meant particularly for older adults that should have been used to enhance the healthcare system. In the study, the respondents complained that the absence of these facilities demoralizes them from seeking healthcare services in public hospitals. The study, therefore, set a pace for other researchers on the conditions of the elderly in the areas that need more responses.
Finally, the study also identified that successful planning and execution of plans for successful aging need some level of force from authority figures such as human rights activists and senior health workers whose interventions in the provision of facilities, drugs, and services can be respected and their instructions obeyed and the psychosocial experiences of the elderly will be given instant attention. In this study, the elderly demanded cordial relationships with nurses in public hospitals which will make them feel at home in expressing their conditions, therefore driving interventions from authority figures that are intended to enhance essential services in public hospitals is paramount.
Limitations of the Study
The limitation of the study was the unwillingness of some. of the respondents to disclose some information or otherwise respond to some questions because it reminds them of their fearful past. Secondly, they are unwilling to answer “any” questions because the researcher does not have an immediate solution to their health challenges like distributing drugs to them or any other benefit. The researcher made them understand that though she was not with an immediate solution to the problem that was her main aim of the study was to proffer possible solutions to policymakers that when implemented will get rid of the problems. Those that eventually allowed us to interview them or administer the questionnaire did it with much reluctance.
Another major limitation was that the researcher depended solely on self-help (no grant to support the research work for financial assistance), and was only able to cover less number of respondents. Also as the study location is in Nsukka, the results from the respondents may not be used for generalization on what is obtainable in other areas, this work was unable to cover different places.
Implications of Practice, Research, Policy Prevention, and Public Health
There are important findings from this study that have significant implications for practice, research, policy prevention, and public health. The research will add to the existing body of knowledge on the psychosocial experiences of older adults and their healthcare delivery in Nigeria, thereby contributing to the growing field of public healthcare delivery for older adults. In practice, if the recommendations made by the researcher based on the findings of the research are carried out it will create a robust policy on health for policymakers.
Therefore the study will serve to establish a legal approach to implement and utilize policies by policy makers, non-governmental organizations, donor agencies and government at all tiers of the federation. Hence, they will see the need for deliberate government efforts toward establishing more elderly people’s homes, visiting both private and public old people’s homes to ensure that groups get the necessary healthcare services they require.
Social scientists use every available opportunity as a baseline to intensify efforts of the government, NGOs, individuals, and the general public on the need to encourage adequate provision for public healthcare delivery for older adults.
Medical Sociologists and Social work professionals should play the crucial roles of creating public awareness and sensitization through media, seminars and workshop programs, policy advocacy, and research works. They then act as facilitators and advocate between policymakers (government and communities) and older adults for the provision of adequate facilities, and specialist health workers (Geriatricians) in healthcare institutions to encourage good access to and adequate utilization of healthcare services.
Conclusion
The study centered on the psychosocial experiences of older adults and healthcare delivery services bordering on, the availability, state, and accessibility of public healthcare delivery services for the elderly in the Enugu North senatorial zone. The study found that there are no healthcare delivery services for the elderly, there are no specialist doctors (Geriatricians) and poor or inadequate facilities in public hospitals Care of the elderly is in the hands of the family members. In Table 3 the study revealed that most of the respondents (79.6%) are not aware of health care services for the elderly as a result, 57.5% of the older adults do not have access to health care services. Also out of all the respondents who go to treatment at private hospitals/clinics, 74.0% have fewer psychosocial problems while 26.0% have more psychosocial problems. On the other hand, out of all the respondents those who receive treatment from a government hospital/health center, 61.7% have fewer psychosocial problems, and 38.3% have more psychosocial problems.
Distribution of Respondents by Places They go for Treatment and Elderly Psychosocial Problem.

Note. χ2 = 6.664; df = 1; p = .010.
Having evaluated the efforts of a non-governmental organization that has institutions for older adults like homes for the elderly in which none is located in the area of study and the services of care providers both public and private, it was noted that the psychosocial experiences and poor healthcare of the elderly are still at increase. Therefore, the government is enjoined to better equip the hospitals and clinics with drugs of equipment at a subsidized cost, especially for poor older adults, and bring trained personnel to are a force of the elderly at homes and hospitals.
Recommendations
Following the results from the research, the researcher proposed that to address the psychosocial experiences of older adults and their healthcare delivery, global support and promotion of health policies for older adults should be sort for at all levels of government. Execution of such policies through opportunities such as the creation of local or regional healthcare centers for them and increase/regular government assistance in the provision of types of equipment and drugs in the government hospitals and clinics especially for the aged at a reduced cost.
The elderly in communities should through government intervention, access resources or have technical assistance related to water and sanitation, housing, transportation, health promotion, and disease prevention strategies which will reduce the psychosocial experiences of older adults and enhance healthcare delivery services. There should be an improvement in the state of public health services in the area of study for easy accessibility.
Suggestions for Further Study
Arising from the recommendations of this study, further research is needed on the issue concerning psychosocial experiences of the elderly and healthcare delivery as there is limited or no healthcare delivery for the elderly in the area of study. It will be interesting to conduct further research in various communities in other senatorial zones to:
Identify the similar psychosocial experiences of older adults in healthcare delivery.
Researchers should use the findings of research to improve the psychosocial experiences of older adults.
Studies embarking on fieldwork to find out the negative experiences of the elderly that endanger successful aging in this modern period of the computer age that is foreign to the older adults that have in turn made them redundant in the community.
Studies on how to improve the situation of older adults through the establishment of institutionalized homes.
Research on how to improve the attitude of health workers toward the elderly for effective cordial relationships.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.