
Abstract
By the year 2050, over 6 million of Ghana’s population will be people aged 60 years and above. Because of increased health challenges that accompany aging, older Ghanaians have health needs to address communicable and chronic non-communicable diseases. This suggests that now into the future, older adults in Ghana will have increased contact with health care professionals. The aim of this qualitative study was to explore older adults’ expectations and experiences with health care professionals to generate information that will shape health care policy and service delivery. Interviews were conducted with a purposive sample of 23 persons aged 60 years and above from the North and South of Ghana. The transcribed data were imported to NVivo software to aid with analysis of the data. An inductive approach ta data analysis was used, drawing from thematic analyses procedures. Three key findings emerged from the study. These include (a) noncompassionate care—health professionals were neglectful, inattentive, discriminatory, and stigmatizing toward participants; (b) disrespectful attitude—professionals showed disrespect by shouting or yelling, making participants feel invisible, or not distinguishing participants from younger patients; and (c) a better way to treat us—participants called for compassion, patience, respect, honesty, and priority attention from health care professionals. The study contributes to literature on older adults’ experiences with health care professionals and suggests to health policy makers and health care professionals to consider older adults’ care expectations to make health care services elder-friendly.
Keywords
Many Ghanaians now reach post-reproductive age and attain the status of older adults. As a reflection of the global trend in aging, older people (aged 60 years and above) constituted 6.5% of the 25 million Ghanaians in the year 2010 (Ghana Statistical Service [GSS], 2012), and their number will increase by 4.7 million by 2050 (GSS, 2013). Population aging in Ghana is occurring at a time of increased migration and urbanization, increased importance of formal education, and a weakening of the traditional safety net (Aboderin, 2004a, 2004b; Apt, 1996; Assimeng, 1999; Coe, 2017; Darkwa, 2000; GSS, 2012; Nukunya, 2003). The demographic transition has also occurred in the context of a shift from an agrarian and traditionalist society to a more industrialized one, where modern services spearheaded by young professionals with formal educational credentials, predominate (GSS, 2012). This trend has a high potential to increase older adults’ contact with formal service providers. One such group of professionals with whom older adults in Ghana have increased contact is health care providers. Because of increased health challenges that accompany aging (World Health Organization, 2018), older Ghanaians have health needs to address communicable and chronic non-communicable diseases (Ayernor, 2012; Debpuur et al., 2010; Duda et al., 2011; Kpessa-Whyte, 2018; Kuuire et al., 2017; Kwankye, 2013; Mba, 2006; Minicuci et al., 2014; Tawiah, 2011). Poverty among older Ghanaians (GSS, 2014) is a key reason for their precarious health needs, as it is for their lack of care and decent housing (Coe, 2017; GSS, 2012). Nearly 28% of Ghanaians, predominantly the elderly, live in poverty (GSS, 2014). Poverty is a health risk factor in any age group, but exacerbates the health situation of older adults (Walker & Druss, 2017; Woo et al., 2020; Zimmer, 2008). Clearly, we know that the health needs of older adults in Ghana necessitate their regular encounters with health care professionals. What we do not know yet is older adults’ experience with health care professionals; that is, the attitude these health care professionals, a younger generation, put up toward older adults. To our knowledge, no previous Ghanaian study has looked at this question. The current study therefore explores older adults’ experiences with health care professionals; how these professionals receive and treat them, and how older adults wish professionals would treat them when they seek health care services.
Theoretical Perspective—Ageism
Ageism offers a perspective with which we understand people’s unpleasant, paternalistic, or patronizing attitudes toward older adults (Butler, 1980; Palmore, 2001). Although Duncan and Loretto (2004) have argued that young people may also be targets of ageism, there is a high likelihood that every older adult will experience ageism at some point during the life course (Ayalon & Tesch-Romer, 2018). Ageism includes stereotypical, prejudicial, and/or discriminatory attitudes mounted toward the elderly by younger-middle-aged adults. Ageist behaviors manifest in communication—verbal and nonverbal—as well as actions and inactions in encounters with older adults (Ben-Harush et al., 2017; Greenberg et al., 2004; Martens et al., 2005). One underlying factor for ageist attitudes, according to Greenberg et al. (2004), is the tendency to ward off any reminder of mortality. As Ben-Harush et al. (2017, p. 40) have put it, because older age is characterized by frailty, debility, and an impending death, “being physically close to older adults or even thinking about them tends to evoke death anxiety.” Therefore, the ageist attitude is a defense or protective shield against death anxiety and against anything that will remind us of our own impending decrepitude (Martens et al., 2005). Ageism also derives from the intergenerational organization of modern society (Ayalon & Tesch-Romer, 2018; Hagestad & Uhlenberg, 2005; Riley & Riley, 1994). Ageist attitudes and mind-set fester in an environment where the younger and older generations are segregated due to retirement policies and institutional care practices, as well as the moving away of young people to live on their own or to pursue full-time education (Hagestad & Uhlenberg, 2005). We can further understand ageism as flowing from age-based power relations ushered in by modernization and social advancement (Ayalon & Tesch-Romer, 2018). Modernization describes the context of advanced technology, increased urbanization, and increased secularization, an environment where the accumulated knowledge of older adults, who are relatively less educated, is deemed obsolete by the younger, more highly educated generations. This perception of obsolescence, perhaps reinforced by retirement policies, is a trigger for condescending, discriminatory, and dismissive attitudes toward older adults.
Itzin and Phillipson (1995) and Krekula et al. (2018) have pointed to a gender dimension of ageism, which Itzin and Phillipson (1995, p. 91) termed “gendered ageism.” Gendered ageism refers to the situation where, for no other than their gender, women are more likely to face age-based discriminatory treatment compared to men. Gendered ageism is posited as a double jeopardy whereby, women, more than men, are judged for their appeal—appearance and looks—to determine how much closeness one can establish with them (Granleese & Sayer, 2006; Handy & Davy, 2007; Jyrkinen & McKie, 2012). In characteristic and consequence, therefore, ageism is comparable to and complicated by racism and sexism (Ayalon & Tesch-Romer, 2018; Butler, 1980); it marginalizes and makes older adults vulnerable, while purporting to save them. Ageism is thus a useful perspective for understanding older adults’ experiences with health care professionals when they seek health care services.
Ageism in Health Care: Overview of Literature
Extant research has investigated ageism among health care professionals and reported findings of negative attitudes (Burroughs et al., 2006; Chang et al., 2020; Gomez-Moreno et al., 2019; Lambrinou et al., 2009; Lee et al., 2020; McLafferty & Morrison, 2004; Peake et al., 2003; Rush et al., 2017; Schroyen et al., 2016). Although Rush et al. (2017) found mixed attitudes overall, they report that nurses’ negative attitudes permeated their approaches to care for the elderly. In another study (Ben-Harush et al., 2017), health care professionals—physicians, nurses, and social workers—held that older patients were offensive in behavior and unpleasant and unaesthetic to work with. As a result, the professionals described how they would often rush older patients through service or use discriminatory communication to exclude these patients from care decisions. In addition, Schroyen et al.’s (2016) study which shows a lower level of support for various types of treatment for older adults among nurses extends the literature and builds on previous studies (Burroughs et al., 2006; Peake et al., 2003). In another study, Higashi et al. (2012) reported that physicians expressed empathy toward younger “end-of-life” patients but were neutral in countenance toward similarly diagnosed older patients. It is not surprising then, that, in their systematic review, Chang et al. (2020) have concluded that ageism worsens the health conditions of older adults across the globe. Research investigating older adults’ experiences with health care professionals confirms Chang et al.’s (2020) conclusion. In a study by Clarke et al. (2014), older adults reported experiencing anxiety and confusion due the disparaging or dismissive attitudes of health care providers. According to Clarke et al. (2014), participants wished their providers would listen to and hear them out. Other studies have reported similar findings. For example, in a study on older adults’ experience with primary care services (Naidoo & van Wyk, 2019), participants complained of “lack of caring” from professionals. Participants explained lack of caring to include the fact that professionals approached them as diseases to be treated, rather than as people with health needs, and burdened them with pills; that is, professionals prescribed multiple medications without education on their interactions, some of which gave serious side effects. This finding builds on Williams-Roberts et al.’s (2018) work where a participant complained that her doctor is always pushing medications on her without considering her need to explore other options. Added to this is Protiere et al.’s (2010) work, which found, among others, that some physicians failed to prescribe beneficial treatments for older adults.
The overview shows there is a growing literature on ageism in the health care system in both the Global North and South, with consequences for older adults who are frequent guests of health professionals. The current study adds to the existing literature by exploring older adults’ experiences with health care professionals in Ghana, a geographic context where literature on this subject is currently nonexistent.
Methods
Participants
Twenty-three participants were purposively selected from the Northern and Greater Accra Regions for the study. Personal outreach and purposive sampling (Singleton & Straits, 2005) ensured that the sample included participants who were typical of the elderly population; older men and women, people from rural and urban areas, individuals of varied levels of formal education, people who had pursued varied careers during their active years, and people belonging to different ethnic groups. Table 1 presents characteristics of the participants.
Demographic Characteristics of Participants.

Data Collection
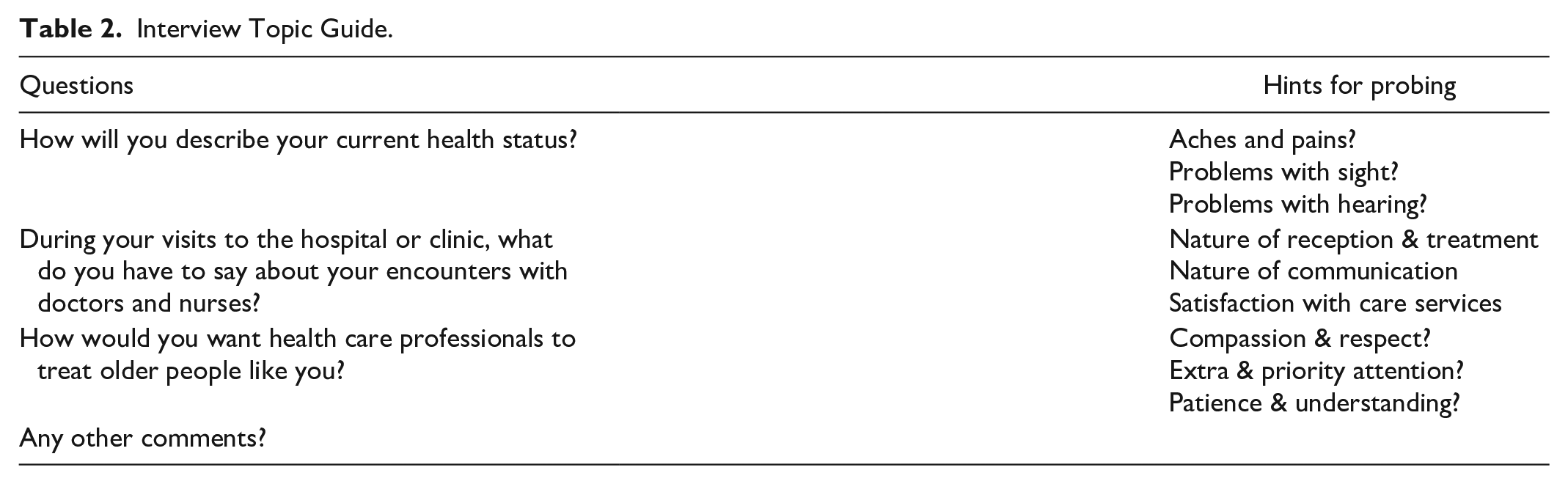
The strategy for data collection were semi-structured interviews, conducted in person by the first author at mutually agreed locations. The interview guide consisted of three main questions, with hints for probing, as shown in Table 2. However, the focus of this paper is the two questions on experiences during visits to the hospital or clinic and how they would want health care professionals to treat them. Nineteen interviews were conducted in English and the remaining four were in Dagbanli, where the questions were interpreted for participants. The interviews ranged from 25 min to 45 min in duration. All interviews were digitally recorded and transcribed. The second author, who is fluent and competent in both Dagbanli and English, ensured a faithful translation of the Dagbanli interviews into English.
Interview Topic Guide.
Data Analysis
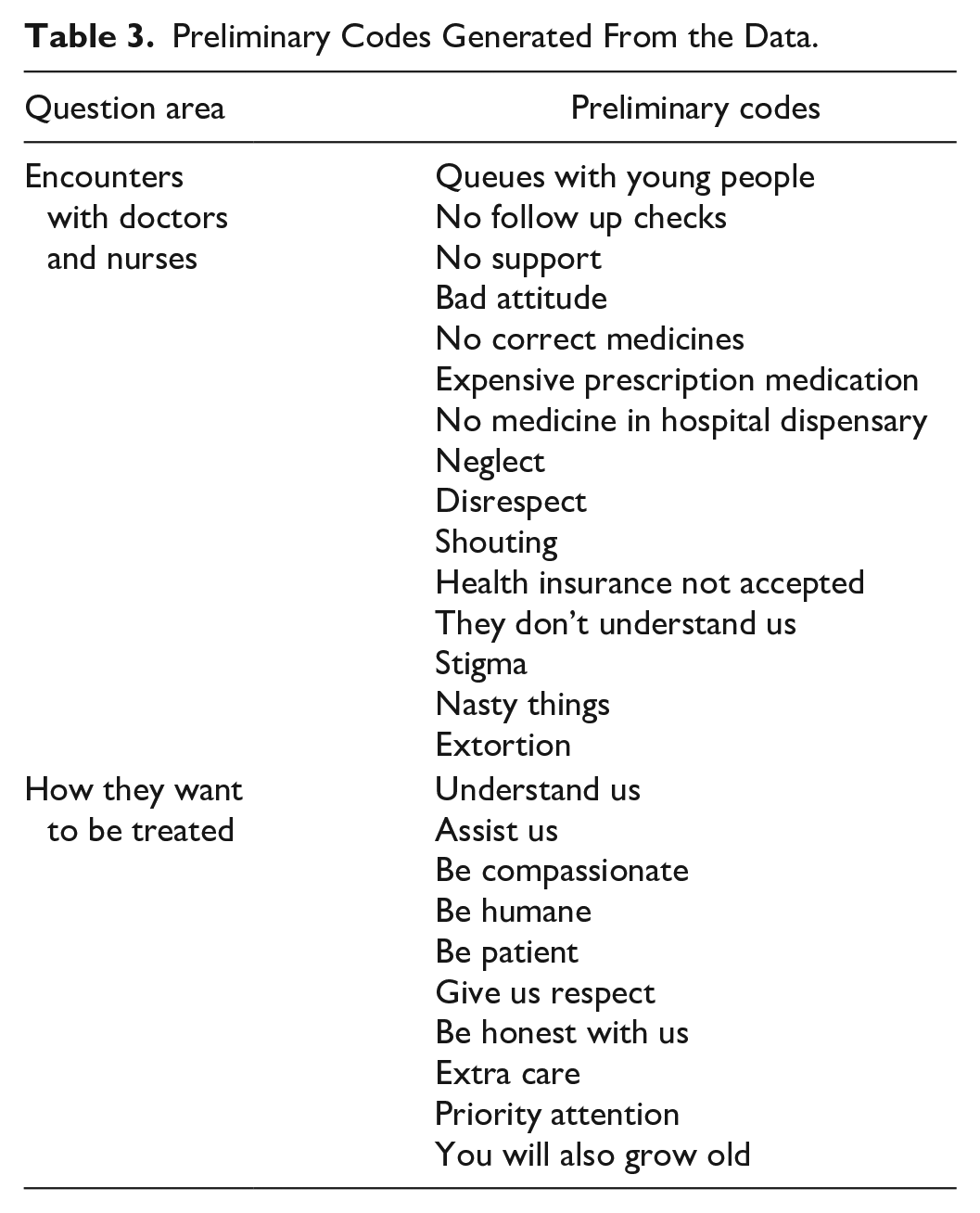
The first author analyzed the data, drawing from thematic analysis procedures as elaborated by Braun and Clarke (2006). All the interview transcripts were imported into NVivo 12 software to aid the organizing and sorting of the data. The researcher read and re-read each of the transcripts, while referring to his field notes. With a focus on the research questions and using thematic analysis procedures (Braun & Clarke, 2006; Holloway & Todres, 2003; Miles et al., 2014; Tuckett, 2005), the data were deductively and inductively coded to identify thematic categories and subthemes. Table 3 shows codes (not exhaustive) generated from data on the two questions that are the focus of this paper. Subsequently, codes were merged to establish meaning patterns or themes that were formulated into statements of findings of the study. This was in consonance with Braun and Clarke’s (2006) explanation that thematic coding helps to identify, analyze, and report patterns or themes in the data. As Braun and Clarke (2006, p. 82) point out, themes capture “something important about the data in relation to the research question, and represent some level of patterned response or meaning within the data set.” For example, from the data on experiences or encounters with health care professionals, the themes of “non-compassionate care” and “disrespectful attitude” emerged. These themes captured participants’ dissatisfaction or disappointment with health professionals’ attitudes and approach to service provision. Then the theme of “a better way to treat us” emerged from the data on participants’ expectations. This theme captured participants’ advice and suggestions on how they should be treated by health professionals.
Preliminary Codes Generated From the Data.
Trustworthiness
The audio recordings and transcripts provided an audit trail for the study. Three colleagues, one being a research mentor, vetted and approved the themes derived from the data, after independently auditing the transcripts with the tape recordings. For ethical considerations, participation in the study was voluntary, all participants provided verbal informed consents, and no identifying information was included in the analyzed data. Memorial University of Newfoundland provided ethics clearance for the study.
Findings
Three main themes emerged from the data; non-compassionate care, disrespectful attitude, and a better way to treat us. These themes are presented below as findings of the study.
Non-Compassionate Care
Non-compassionate care was a major concern for participants. Some of them needed support with hypertension, chronic pain or emergency health care, and, therefore, needed to visit the hospital or clinic regularly. However, contrary to expectations, participants reported experiences of neglect, inattention, discrimination, and stigmatizing treatment from doctors and nurses during some of these visits. According to one participant, I have hypertension, which is my problem. If my BP goes high, I know that I am hypertensive, so am going to collect treatment. But you go and it is like the aged we are always worrying people. They will even see you and do as if they don’t know you. Should I stop the medication so that I don’t go to the hospital? So you find out that some people will sit down with their sicknesses, so a sickness that is not supposed to kill you, it will kill you because you are afraid to go because, number 1, you don’t have money, number 2, nobody will mind you, then number 3, they say finally that it is aging. (65-year old female participant)
It appeared that female participants were more the targets of “bad attitudes” from health professionals, perhaps giving it a gender dimension. A further illustration of this complaint by participants is captured in the following: Their (professionals) attitudes toward us the older people in Ghana here is not good. If you are old and they see that you have something, they will pretend to be nice to you, like “madam has come.” They will pretend to be nice. But if they see that you, when they prescribe medicine for you to buy, you can’t get money to buy it, even the correct medicine the doctor will not give it to you. Because they will tell you that the medicine is expensive. Maybe that medicine will help you to live for some time. You see. So, me, if I had my own way, I would prefer not to deal with these professionals. (74-year old female participant). Health professionals, we really have problems with them. So sometimes, they should make somethings flexible for older persons but they don’t. For example, you get to the hospital, I’m a retired nurse, but that doesn’t mean that when you go they take care of you. You still go through all the dirty, all the nasty, all those things, you still go through them. (68-year old female participant).
It really came across as a big disappointment for older adults who feel they have contributed their quota to society to be treated with inattention in spaces where they really need compassionate care. Building on this sentiment of inappropriate treatment, a 61-year-old retired male nurse had the following: I can have patience to listen to, to ignore something that somebody is doing at the hospital because I was a nurse, and I know they [doctors and nurses] can be like that. Some other people haven’t got this background. So, you get there and the way the providers behave, somebody’s behavior changes, it triggers the person’s condition.
There was also the sense among participants that health care professionals, young and relatively well to do, do not appreciate the difficult circumstances of older people to understand that they need subsidized health care. Therefore, another dimension of the complaint of non-compassionate care revolved around the fact that their health insurance coverage was not accepted for treatment. For this reason, they had either to pay out of pocket for lab tests and prescription medications or forfeit treatment. There seemed to be a disagreement over what exactly the health insurance scheme covers for older people in Ghana, and how much control frontline health care workers have over this. One participant provided a background to their disgruntlement. “You go with your insurance card to seek health care, they give you a prescription and ask you to go and buy the medicine. But it was said that we older persons should be given free health care.” (67-year old female participant). Another participant captured it very bluntly, that “They (health professionals) deny us support. This is a huge problem for older people, but that is not the way things should be” (77-year old male participant). A participant was emotional about the nonacceptance of their health insurance coverage for prescription medication when she posed the question, “What if you die before you can raise money for the drug?” According to this 78-year old female participant: We complain about this all the time. Because hypertension does not want too much thinking and it doesn’t want you to skip taking the medication. We were told that older persons will get free health care on the national health insurance scheme. But today you go to the hospital and they expect you to pay for treatment. If you don’t have the money you sit there and watch while they attend to those who have money to pay.
Several other participants related to this disgruntlement about non-compassionate care. The following are further illustrations: If there are any professionals who should be compassionate toward older persons, it should be doctors. But if you go there, they will not see you as an older person. A few days ago, I fell ill and went. For the blood tests, I paid 350 Ghana Cedis. And they create the impression that older persons are not charged, but for all the tests, I paid. On that occasion, I cried a lot. One of my children just sent me the money for a funeral and I had to spend it on the lab tests. They are liars. The health services here are not helpful to older persons. (66-year old female participant). It would be proper for the professionals to assist us, so we can receive health care. The health insurance they talk about, you have the card and go to the hospital and they ask you to go to a drug store for the drug. But if you go you will have to pay out of your pocket. You don’t have money, so you cannot get the prescribed medicine and that means there is no health care. (80-year old male participant) Health care is very important for us older people and they say we have health insurance coverage. But if you go to the hospital with your insurance card, you will have to spend money before you get care, what the professionals are required to do they won’t do it. They may only give you common over-the-counter drugs, like paracetamol, and ask you to go and buy the important medications. But it is obvious, as an older person, you don’t have the money to pay for these drugs. (75-year old male participant).
Disrespectful Attitude
Participants reported disrespectful attitude and/or treatment from health providers during some of their encounters. Disrespect was a source of anger and frustration or confusion for participants, because they believed that they deserved better. One area of disrespect lay in how providers communicated with the older adults, such as shouting or yelling and showing no regard. According to one participant, “Sometimes some of us go to the hospital and they treat us as if we are nobody. For this reason, some older people don’t want to visit the hospital” (64-year old male participant). Because of such frustration, a participant indicated, “If God permits that you have a child who can communicate with the professionals when you are going to the hospital, then he can lead you there. Because they will understand each other.” (80-year old male participant). Other quotes supporting this dimension of disrespectful treatment include the following: They [health professionals] feel they will never perhaps become old and they feel old age is a hindrance, is a taboo; something that you should not get nearer to. It is stigmatized. Something like that, stigmatized. That is how most of the young professionals behave, not to say a few of them are okay. But majority of them are too, they show a very bad attitude towards old age. (72-year old male participant) Actually, if you are old, some of them [professionals], the young ones, they don’t know how to talk. You can even approach the person and the person will shout on you. And some of them, there are some, they know you and you know them very well, but when they see you, they will pretend. Because, maybe, if he greets you it means he should come and help you. (62-year old female participant) One thing is that some of the professionals don’t understand older people. So, they are not humane to us. They don’t have any regard. Like some of us, they see us having our own private businesses and they feel you are so wealthy that this is the time they have to extort from you. “You are taking pension and you have established a business.” (70-year old female participant)
Asking older adults to wait in queues with young people to receive care was also seen as disrespectful treatment. Participants believed that they are not as strong as young people are, and it is inappropriate to mix them up with young people their children’s age. The following quotes illustrate this perception of disrespect: Imagine you go to the clinic and see that old men and young men are standing in the same queue, while they could have separated us and given me priority attention. You see. That is the thing. That is my problem with the health professionals. (73-year old male participant) They know what to do but they won’t do it. If you see an elderly person, the person is in the queue, you should call me and attend to me. But they won’t mind you. So, me, when I go to the hospital, those nurses I know, if I see you, I turn my face away. (62-year old female participant) I usually go with a child so I can sit aside while he joins the queue to get the necessary papers for me to see the doctor. What if you don’t have a child or if the children are all in school? (80-year old male participant)
A Better Way to Treat Us
Participants provided advice, suggestions, and warning, all of which indicated clearly that there is a better way in which health professionals can provide care to older adults. Male participants were overrepresented in the voices that called for a better way to treat older adults, especially the need to give them priority attention. Their suggestions seemed to be grounded in three core foundations; received custom and tradition, which requires that older people be treated with compassion, medical ethics, which suggests that the most vulnerable patients—children and the elderly—be given extra and priority attention, and exceptions in human rights codes, which make protection of the weak a top priority. Compassionate treatment of older adults, captured in the concepts of respect, patience, and honesty, is illustrated in the following: The professionals have to relate to us nicely. You don’t have to shout on us, driving us. You have to exercise patience with us. Because when you are 60 and above, some of them, they don’t have patience with you. If you shout on me like this, if you don’t take care, I will fight you. I will tell you that I have a son like you in the house; I have a lady like you in the house. So you have to give me the due respect. (61-year old female participant) I think the first thing is for professionals to be patient with older persons. Because as one is aging, the capacity of the mind reduces. So, these professionals need to follow older persons with patience. They also have to be honest and truthful with older persons during provision of services. Remember that you will also grow older tomorrow. (60-year old male participant) The young professionals should give more respect. If you talk to us with sense, talk with respect and advise us and say, “this is what you are supposed to do, this what you are supposed to do.” Then the elder person will also give you more respect and give you advice. (71-year old female participant)
One participant hinted at the fact that compassionate treatment required the professional to be honest and truthful about the prognosis of their conditions: We just say, if you are not well and go to the hospital; we just say the professionals should be compassionate toward you. You are old and you are sick. As I am sick and they bring me to the hospital, they give me to you the health professionals. Be compassionate toward us older people and give us treatment. And if we cannot be treated, you allow us to return home until our life ends. (68-year old male participant)
Included in participants’ admonition was what we may term “professionals beware”, because there are consequences for not treating older adults with compassion. Such a warning to professionals against bad behavior toward older people is exemplified in the following quote: Look, if you are in a service, you are young and energetic, and those elderly people come into your office for assistance, and you don’t handle them well, I bet you, it will pay back to you. There are no two ways about it. So the doctors, the nurses, they should do well before God and man to take good care of the elderly people. Because one day, one day, you will get to where they are. (67-year old male participant)
Participants also wanted priority attention so they can have a shorter turn-around time. They indicated that older people need priority care because they are not strong and need more time to rest at home. One participant suggested that, “Professionals should not allow older people to struggle to get service. They should quickly pick older persons out of the crowd and attend to them.” (62-year old male participant). It was clear that participants do not want to wait in queues to receive health care services. The following quotes further illustrate this point: For the doctors and nurses, it is appropriate that when an elderly person visits the hospital, the nurses reckon that this is an older person; they cannot put you among young people. They should give you extra attention, treat you well and give you good medical care so you can return home and rest. (68-year old male participant) The professionals should give us that respect. Yes, let the young people know that this man, you don’t expect him to struggle with you. The energy you have to stand and wait he doesn’t have. (62-year old male participant)
Some participants referenced ethics and human rights provisions to support their call for priority treatment at the health centers. One illustration went like this: Ethically, we have to give reverence to our aged, wherever you are. You have to keep at the back of your mind that you are meeting people who are not very strong, who are not able to understand many things. You need to have patience and give priority to the aged. If you want to give care to patients: one, children are those that we look at first, children; secondly, the aged. Children and then the aged. (61-year old male participant)
Another, on exceptions to fundamental human rights dictates, went as follows: We are all equal when it comes to human rights. But there are exceptions. So, any elderly person who seeks help or services, the service provider should keep that in mind. You don’t have to listen to what people will say. If you have that at the back of your mind, then you will be doing something. But if you want to say “first come, first served,” that is where the problem is. Because a lot of the aged feel frustrated and discouraged from coming the next time. (70-year old male participant)
Discussion
This study explored older adults’ experiences with health care professionals in Ghana. Our conceptual lens for the study was ageism and intergenerational power relations between the young and the old in modern society. We drew from thematic analyses for data analysis and identified three themes from the data. The themes were (a) noncompassionate care, (b) disrespectful attitude, and (c) a better way to treat us. Participants were disgruntled about professionals’ attitudes, which suggested that geriatric patients were a worry or that the conditions they presented were just normal part of aging, thus, calibrated their care behaviors accordingly. As such, participants experienced discriminatory, inhumane, and neglectful treatment, which they regarded as disrespectful and non-compassionate care on the part of health professionals.
One aspect of noncompassionate care that shows it is a serious concern is participants’ explanation that it is the reason why some older adults will not visit the hospital with their ailments. As they pointed out, doctors and nurses make you go through nasty things, and their behavior triggers some people’s health conditions. Reports of stigmatizing, discriminatory, and extortionary practices were another area of professionals’ noncompassioante behavior. Participants believed that this was the reason why they did not get the medications they needed at the hospital; they were rather asked to go to town to pay for medications out of pocket, which they could not afford. Again, participants had to pay exorbitant fees for lab tests. For many participants, these were enough to deny them health care. Because many participants live in poverty and cannot afford the costs of health care, a major disappointment with health providers was the refusal to treat them free of charge even when they presented a health insurance card. Their frustration derived from the fact that, although there is the impression that older adults receive free health care under the National Health Insurance Scheme (NHIS), health professionals asked them to pay for service or stand aside. Looking at their accounts, one gets the sense that health professionals acted to deny them the benefits provided for older adults by the NHIS, which suggests the professionals are not compassionate.
In addition to noncompassion was what participants described as disrespectful attitude from health professionals. Disrespect was a source of anger and dejection among participants, because they believed that moral codes deriving from custom and tradition require that the young treat the elderly with respect and extra attention. Contrary to this, participants described how they were belittled or made to feel invisible; such as being shouted on or rushed, or being treated as if they were nobody. An area of disrespectful treatment that appeared very concerning for participants was the fact that doctors and nurses did not give them priority attention. Thus, having to wait in queues with young patients, instead of being “separated and given priority attention,” was a source of distress for participants. The feeling was like, “what is wrong with this generation? Have we lost our timeless values regarding care for the elderly? How do you expect us to stand in queues with young people our grandchildren’s age?” Participants therefore gave advice and suggestions on how health professionals should relate to and treat them; professionals should try to understand them and treat them with patience, respect, and priority attention.
The finding of disrespect and noncompassionate care in this study is parallel to findings of other studies in Sub-Saharan Africa (SSA) and elsewhere. For example, in one study, geriatric patients complained of disrespect and lack of care from primary health care professionals, and expressed a dissatisfaction with long waits in queues (Naidoo & van Wyk, 2019). Also, similar to our participants for whom professionals’ behavior communicated stigma and the impression that they were a burden, or that their conditions were part of normal aging, participants in the Naidoo and van Wyk’s (2019) study felt providers treated them as diseases rather than human beings. One study captured disrespect or noncompassion for older adults as “insufficient respect” or not being approached “in a professional manner” (Jangland et al., 2009, p. 201). Our findings further build on a study by Ben-Harush et al. (2017), where health providers reported that they have difficulty working with older adults because they are demanding and unpleasant.
Again, our participants’ report that professionals treated them with no regard, or as if they were nobody, is similar to what is reported in other studies (Ben-Harush et al., 2017; Clarke et al., 2014; Jangland et al., 2009; Sagner, 2002). In Clarke et al.’s (2014) study, disrespect or noncompassionate care by health providers took the form of disparaging and dismissive attitudes, where professionals assumed they knew what was wrong with older adults without engaging in a conversation with them. Professionals in Ben-Harush et al.’s (2017) study confirmed this when they indicated that they usually make treatment decisions without a meaningful discussion with older adults. Our finding that health providers were shouting on participants or driving them through the treatment process resonates with Ben-Harush et al.’s (2017) work, which found that, for nurses, treatment of older adults is routine and should not consume much of their time.
A big issue for our participants was that providers required them to wait their turn in queues with young people. Perhaps long wait times is an unpleasant issue for all patients across the health care system (Herring et al., 2009; Horwitz et al., 2010; Willoughby et al., 2010). For our participants, however, it is culturally insensitive and disrespectful to treat them this way; by custom and tradition, older adults have earned a special right to priority attention. Another finding that deserves attention is participants’ belief that health professionals deny them free health care services guaranteed them by the NHIS, including costs of laboratory examinations and prescription medications. Perhaps this is a misperception on the part of participants about their entitlements under the scheme, rather than a deliberate act of refusal by health professionals. The NHIS is a basic scheme that requires beneficiaries to contribute a basic premium for primary health care services. The scheme exempts older adults of a predetermined age range from paying the premium, or subsidizes the premium for them. As a basic health insurance scheme, perhaps the NHIS does not cover costs of lab tests and/or prescribed medicines for the health cases presented by participants. In this regard, Kuuire et al. (2017) have pointed out that, with the premium exemption policy alone, the NHIS does not do enough to make health care accessible and affordable for older adults. If this is the case, however, professionals have a responsibility in making time to educate older adults on what is covered and what is not covered for them by the NHIS. Failure to do this because of some of the reasons identified above goes to buttress the perception that the health professionals are noncompassionate.
A significant finding of our study is the advice participants gave on how health professionals should relate to and care for older adults: “a better way to treat us.” Participants wanted professionals to understand them, to know what their worries are. What this suggests is that participants expected professionals to make time to listen to them explain their conditions. As a 70-year old female participant put it, “if you understand somebody, whatever the person does you can interpret it correctly.” Participants also wanted compassionate treatment, which they explained to mean health professionals should be honest, patient, and respectful toward them. As part of compassionate care, honesty or truthfulness would mean that, as a 68-year old male participant put it, “if we cannot be treated, you allow us to return home until our life ends.” In addition, participants wanted health care workers to give them priority care, instead of applying what looked like “first come, first served” rules that made them wait in queues with younger patients. Participant were saying that at their age they are a weaker and vulnerable group who should not be made to wait long for service and who should not be mixed up in queues with young people. Our participants’ call for a better treatment approach from health care professionals builds on age-friendly (Araujo de Carvalho et al., 2017) and patient-centered care expectations of older adults (Harrefors et al., 2009; Naidoo & van Wyk, 2019; Williams-Roberts et al., 2018) and resonates with the research by Pawlikowska et al. (2012) on patient enablement. For example, similar to our participants’ call on health professionals to take time to understand them, Williams-Roberts et al. (2018) found that older adults wanted their providers to listen to and spend time discussing treatment options with them. Again, the need for priority care, which was a key concern for our participants, was a major expectation by older adults in the study by Naidoo and van Wyk (2019).
Theoretically, ageism helps us to make sense of the findings. The three dimensions of ageism—cognitive (e.g., stereotypes), affective (e.g., prejudice), and behavioral (e.g., discrimination) (Ayalon & Tesch-Romer, 2018; Greenberg et al., 2004; Levy, 2003; Marques et al., 2020) are all captured in the findings. More importantly, the findings corroborate the theoretical position that ageism exists in two forms; “other-directed ageism” and “self-directed ageism” (Ayalon & Tesch-Romer, 2017; Iversen et al., 2009; Marques et al., 2020). Other-directed ageism is where we think negatively of older people and treat them based on such negative perceptions (Ayalon & Tesch-Romer, 2017; Iversen et al., 2009; Marques et al., 2014). Drawing on this, one sees the ageism in health care professionals’ discriminatory and disrespectful attitudes as recounted by participants. Other-directed ageism among health professionals is perhaps part of a widespread phenomenon in the general population (Inglehart et al., 2014; Marques et al., 2020; North & Fiske, 2015; Officer & de la Fuente-Nunez, 2018). For example, in a 57-country World Values Survey, Inglehart et al. (2014) reported that 60% of respondents showed negative attitudes—disrespect—toward older adults. In addition to other-directed ageism is self-directed ageism. According to the theory, self-directed ageism happens where a person has negative feelings or beliefs about her or him-self, and about the conditions of their aging (Ayalon & Tesch-Romer, 2017; Marques et al., 2020). In light of the theory, one can see self-directed ageism at work among participants. For example, participants’ belief and argument that they are not strong enough to wait in queues for their turn to receive service is self-directed ageism (a suggestion that being older means being weak) that may serve to reinforce other-directed ageist attitudes. An important theoretical point to make is that no matter the form or direction it takes, ageism is harmful and should be addressed (Officer & de la Fuente-Nunez, 2018).
Limitations
A purposive sample of 23 older adults provided data within a 2-month period for this study. The sample is predominantly male, urban, and Northern Ghana. This is not representative of all persons aged 60 years and above in Ghana, and, therefore, the findings cannot be generalized to the whole country. More research with much larger and diverse samples is needed to further explore older adults’ experiences with health care professionals in the country.
Conclusion and Implications
This study adds to the literature on older adults’ experiences with health care professionals in various health care settings. It adds to the literature on ageism in the health care system where older adults complain of disrespectful and impatient treatment while yearning for priority care and shorter wait times. Older adults belong to an age group whose presence induces death anxiety, whose conditions are stereotyped as normal part of aging, and who are seen as unpleasant to deal with. Furthermore, because of the prejudicial view that older adults’ knowledge is obsolete, health professionals do not think that these patients know anything about the science of disease and its treatment. As a result, older adults’ opinions about their conditions and how they should be treated are dismissed. Gender did not appear to make a marked difference in older adults’ experience of ageism in this study. Although male participants were in the majority, similar proportions of men and women reported noncompassionate care and disrespectful attitudes. However, female participants were more likely to report being shouted at or discriminated against. Consequently, one female participant wondered whether she should not go to the hospital for treatment, while another wished she could avoid dealing with the health professionals. Similarly, although participants were unanimous in their call for respectful treatment, priority care, and cost-free health care, male participants were more likely to call for respect and honesty from health professionals.
Results of this study have implications for further research and for practice. As noted above, further research involving larger samples is needed to investigate issues of ageism in the health care system in Ghana to provide a much stronger basis for elder-friendly health care policies. The findings suggest that at the most basic level, health care managers, and service directors need to inculcate in frontline personnel a culture of respect and compassion for older patients. An elder-friendly health care service will require a sensitization on ageism and training in gerontology and geriatrics for doctors and nurses, a policy of priority care for older adults, including a separate priority queue for geriatric patients, and a health insurance scheme that covers costs of lab tests and prescription medications for older adults. Furthermore, there is need for a number of measures: first, more education to bring clarity on what is covered and what is paid out-of-pocket by older patients under the National Health Insurance Scheme (NHIS); second, diligence in ensuring that hospital dispensaries are stocked with essential medications, which are either covered by the NHIS or sold at subsidized rates for older patients; and, third, priority attention to older patients during their visits to the outpatient departments (OPDs) of the hospitals.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a Social Science and Humanities Research Council-Vice President Research (SSHRC/VC-Research) Grant (RGCS: 20170865).
Ethical Statement
Ethical approval for this study was obtained from the Interdisciplinary Committee on Ethics in Human Research (ICEHR) of Memorial University of Newfoundland (ICEHR Number 20171397-SW).