
Abstract
Post-traumatic stress disorder (PTSD) is a chronic and debilitating disorder characterized by hypervigilance and recurrent, intrusive memories of the traumatic event. Estimates for lifetime prevalence of PTSD diagnoses for United States military personnel vary widely from 10% to more than 30%. The current study aimed to investigate the attitudes and beliefs regarding PTSD and its diagnosis and treatment within U.S. military service members and their families. An online survey was administered to current and former members of the U.S. military and members of their immediate families. The results revealed low levels of mental health stigma and positive attitudes toward treatment for PTSD. However, survey respondents also communicated a belief that the current health care system does not adequately meet the mental health needs of the U.S. military. A clear understanding of the specific attitudes and thought processes surrounding PTSD and its diagnosis may aid mental health professionals in effectively communicating with those in need of their services.
Post-traumatic stress disorder (PTSD) is a chronic and debilitating disorder of the stress response that may occur following exposure to a traumatic event. Symptoms are classified into clusters and include intrusion symptoms, avoidance, negative alterations in cognition/mood, and alterations in arousal/reactivity Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association [APA], 2013). The lifetime prevalence for a diagnosis of PTSD within the general population in the United States is estimated to be approximately 8.7% (R. C. Kessler et al., 2005). The types of traumatic events that may lead to the development of PTSD include sexual assault, child abuse, witnessing or being the victim of a violent crime, exposure to a natural disaster, and/or military combat. Recent epidemiological studies have estimated the lifetime prevalence of PTSD for United States military personnel to be somewhere between 10% and 30% (Dohrenwend et al., 2006; Fulton et al., 2015). This number seems to vary depending upon the timing of military service. The estimated lifetime prevalence of PTSD in Vietnam Veterans was determined to be approximately 30.9% (Kulka et al., 1990) while prevalence for Gulf War Veterans and Veterans of Operation Iraqi Freedom were cited as 10.1% (Kang et al., 2003) and between 13.8% and 20% (Hoge et al., 2004; Tanielian & Jaycox, 2008), respectively. The discrepancies between these numbers may be related to a number of factors including time elapsed since combat, the type of combat and military tactics utilized during each action, the location of service and the stigmas associated with mental health at the time of service. PTSD is the most prevalent mental health diagnosis for military service members returning from Iraq and Afghanistan (Seal et al., 2007).
Stigmas surrounding mental illness in the military have steadily decreased over time but remain high (Acosta et al., 2014). Reducing the stigmas associated with mental health within military populations is a current priority as research has shown that these stigmas may serve as a barrier to treatment for those returning from combat (Acosta et al., 2014; Blais et al., 2014). In one study, veterans stated that they did not seek treatment for their PTSD symptoms because of a desire to avoid being labeled as having a mental illness (Mittal et al., 2013). The rate of individuals who meet diagnostic criteria for mental health disorders seeking care is estimated to be only 23% to 40% with a concern for “being seen as weak” cited as the most prevalent barrier (Hoge et al., 2004; Sharp et al., 2015). In addition to stigma, other identified barriers to treatment include mistrust or negative beliefs about mental health care, a belief that treatment is unnecessary, and difficulty obtaining care (Brown et al., 2011; Gould et al., 2010; Iverson et al., 2011; Kim et al., 2011; Mojtabai et al., 2011). Even within those who do seek care, as many as 90% of veterans do not receive a level of mental health care that meets the recommended number or intensity of sessions (Seal et al., 2010). Delay or non-completion of care is likely to lead to worsening of symptoms and a greater impact on the individual and their family.
To address issues related to mental health stigma, it is important to understand how individuals, both those serving in the military and their families, conceptualize PTSD and its diagnosis. Recent research into media coverage of the disorder has shown that nearly half of all articles in the New York Times involving PTSD were aimed specifically at military service as a cause of trauma (Houston et al., 2016). In addition, articles that discussed PTSD within the context of the military were more likely than those discussing civilians to identify violence, rage, suicide, and substance use as issues for diagnosed individuals. Biased media coverage may contribute to a misunderstanding within the general public regarding PTSD and its causes, symptoms, and treatments leading to further stigma. Many members of the general public have limited knowledge regarding mental health issues and the knowledge that they do have may be incorrect. In a study of public school teachers, television was identified as the source of most of their knowledge regarding mental health issues (Soares et al., 2014) suggesting a need for accurate portrayals of disorders within the media. Increasing mental health literacy would likely lead to greater acceptance of mental health treatment and increases in recognition, management, and prevention.
The current study sought to investigate the relationship between military service and perceptions of PTSD by distributing open-ended surveys to military personnel and their immediate family members. Identifying the specific information, attitudes, and beliefs regarding PTSD and its diagnosis may aid in the creation of campaigns to increase education and reduce stigmatization of the disorder leading to greater understanding and access to care.
Materials and Methods
Participants
Participants were adults between the ages of 18 to 79 (N = 50; 26 males and 24 females) recruited from postings to military affiliated social media groups and websites. As shown in Figure 1, 62% (n = 31) of the respondents were current or former members of the U.S. military with 36% (n = 18) having served in the U.S. army, 16% (n = 8) in the U.S. Marine Corps, 6% (n = 3) in the U.S. Air Force, and 4% (n = 2) in the U.S. Navy.
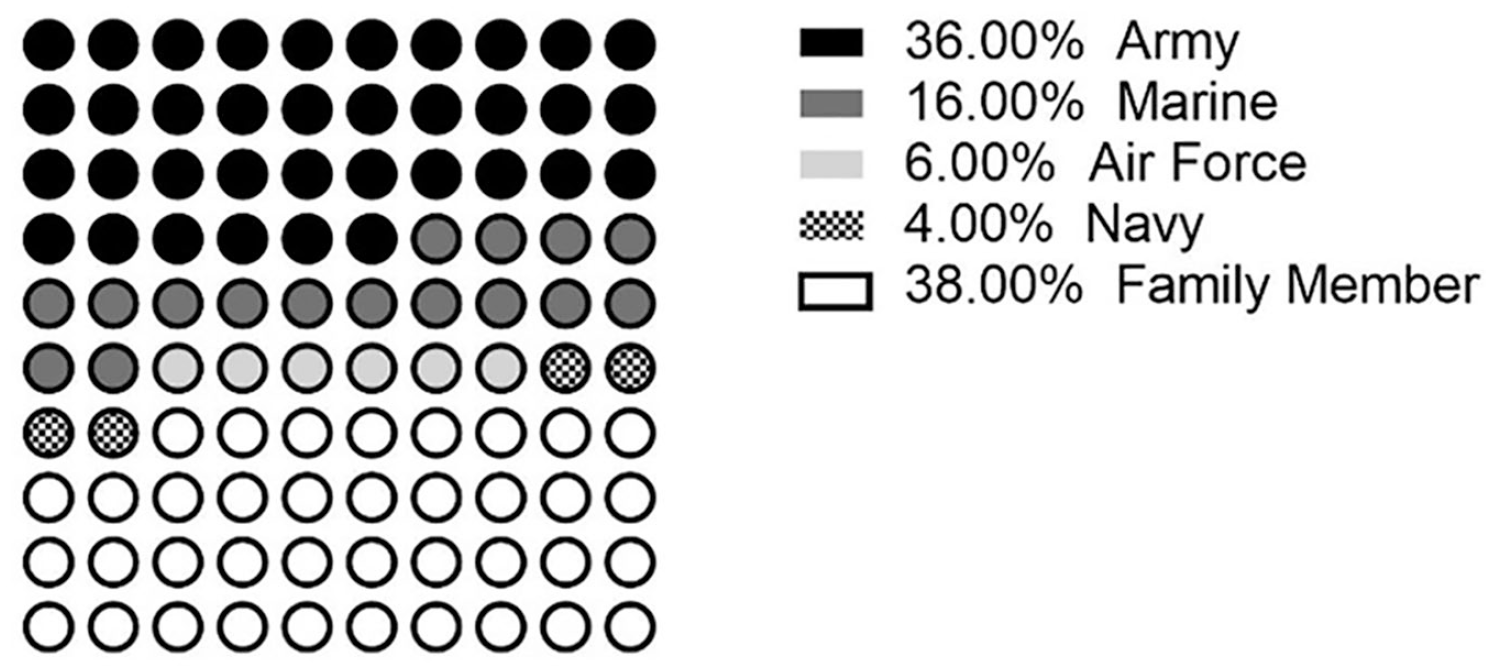
Military affiliation of survey respondents.
The remaining 38% (n = 19) of respondents had an immediate family member that was serving or had served in the U.S. military, 18% (n = 9) had a spouse who had served, 14% (n = 7) had a parent who had served, and 6% (n = 3) had a sibling who served. Of the 31 participants who had served in the U.S. military: 38.7% (n = 12) served in the Global War on Terror in Iraq, 22.5% (n = 7) served in the Global War on Terrorism in Afghanistan, 19.35% (n = 6) actively served during the Vietnam War, 16.1% (n = 5) served in Southwest Asia (Desert Storm/Shield), 6.4% (n = 2) served in Kosovo, 3.2% (n = 1) served in the Armed Forces Expeditions (Dominican Republic, Grenada, Panama), and 16.1% (n = 5) had never served in an active military campaign. Some participants served in more than one military campaign. When asked about their faith tradition, 66% (n = 33) identified as Christian, 4% (n = 2) as Jewish, and 22% (n = 11) reported no religious affiliation. Another 8% (n = 4) chose “other” as their faith tradition. Muslim, Hindu, and Buddhist were options that were not chosen by any respondents.
Measures
To collect information about personal attitudes and beliefs concerning PTSD, an online survey was administered via Qualtrics. In addition to demographic questions, the main survey included 10 open-ended questions where participants could enter as much or as little information as they chose using their own words. Questions focused on the individual’s understanding and attitudes regarding PTSD and its diagnosis. To assess knowledge regarding PTSD, participants were asked to provide a definition of PTSD and a list of symptoms and treatments. To probe for stigmas related to mental health disorders, participants were asked about their perceptions of individuals who utilized therapy and/or medications to treat PTSD. Participants were not asked to reveal any private health information or specific diagnoses though some individuals chose to share some of this information in their responses. The Institutional Review Board at Messiah University approved all survey instruments and participant recruitment procedures.
Data Analysis
Data was analyzed by a team of three reviewers using a general inductive approach. Raters independently identified themes within the data and then met to review the information and form a consensus. In addition to the identification of themes, qualitative data provided in the open-ended questions was coded based on whether the overall tone of the response was positive, negative or neutral. Questions that asked participants to provide information about PTSD, its symptoms and its treatment were coded based on whether the information was accurate based on the DSM-(5th ed.; DSM-V; APA, 2013). Questions that asked participants about their perceptions of individuals with PTSD were coded for stigma. Participant quotes were then chosen to represent identified themes or to identify uniquely worded responses.
Results
Definition of PTSD
When asked to define PTSD, 60% (n = 30) of the respondents identified the trauma as a defining feature. The idea that PTSD is a psychological/mental health disorder was communicated by 26% (n = 13) of respondents and a list of symptoms was used by 28% (n = 14) of the respondents to define the disorder. A total of 16% (n = 8) of the respondents made reference to the persistence of symptoms over time using words and phrases such as “lingering effects” (Respondent #5), “never-ending remembrance” (Respondent #34) and stating that the disorder is “with you every day of your life” (Respondent #17) and is something that the “human brain cannot forget” (Respondent #45). Some respondents stated that PTSD can develop in individuals who are witnesses to traumatic events and not only those who directly experience the trauma (10%; n = 5). These results are displayed in Table 1.
Words/Phrases Used Most Often by Respondents to Define PTSD.

Note. Some responses included reference to more than one word/phrase. Thus, percentages sum to more than 100%. PTSD = post-traumatic stress disorder.
One individual, whose sibling served in the military, defined PTSD with a single word: “shitty” (Respondent #17). Two individuals referred to the importance of medication and therapy in treating individuals with PTSD. References were also made to the idea that PTSD negatively affects all aspects of a person’s life and/or interferes with the ability function in society (28% of respondents; n = 14). Other responses included reference to the classification of PTSD as an anxiety disorder (10%; n = 5), the idea that PTSD cannot be successfully treated (12%; n = 6) and the idea that individuals who revel in past accomplishments have PTSD. In this last case, one respondent suggested that a “35-year old man consistently at high school football games to relive his moments in life” (Respondent #31) would meet a PTSD diagnosis.
Another respondent stated that he or she tried to “avoid any shows of Vietnam” (Respondent #50) and does not have “any ‘Nam caps, jackets or patches” referring to a desire to avoid associating with that time in their life but often find themselves still “in combat-ready mode.” Some respondents referred to PTSD as an atypical or maladaptive response to the trauma (6%; n = 3). Other words or phrases that were used to define PTSD include “debilitating” (4%; n = 2), “a disruption in one’s life” (Respondent #22), an “emotional roller coaster” (Respondent #26), and “a disconnect between the trauma and fitting into society” (Respondent #33). One respondent stated that if left untreated PTSD “will destroy your life” as it “has done to so many of my veteran friends” (Respondent #16).
Phrases and Images
Respondents were asked the question, “When you hear the term ‘post-traumatic stress disorder’ or PTSD, what phrases or images come to mind?.” Quotes from respondent answers are provided in Table 2. The most common answer involved war/combat/veterans (52%; n = 26) and the second most common answer involved nightmares (16%; n = 8). The only specific conflict that was mentioned was Vietnam (written in by two respondents).
Phrases/Images Respondents Associate With PTSD.

Note. PTSD = post-traumatic stress disorder.
Symptoms of PTSD
Table 3 shows the responses given when participants were asked to list the symptoms of PTSD. The most commonly identified symptoms were the intrusion symptoms of trauma-related nightmares (40%; n = 20) and dissociative reactions/flashbacks (36%; n = 18). Sleep disturbances, a criterion E symptom of increased arousal, was written in by 32% (n = 16) of respondents. Respondents included symptoms that are not part of the DSM-5 criteria for PTSD such as anxiety (40%; n = 20), panic attacks (12%; n = 6), depression (32%; n = 16), mood swings (10%; n = 5), and substance abuse (8%; n = 4).
DSM-5 Symptoms of PTSD Correctly Identified by Respondents.

Note. PTSD = post-traumatic stress disorder.
Traumatic Events
Respondents were asked to name the types of traumatic events or experiences that might cause someone to develop PTSD. These results are displayed in Table 4. The most commonly provided answer was combat experience, which was provided as an answer by 28% (n = 14) of the respondents. Of those listing combat as a type of traumatic experience that might lead to PTSD, 92.8% (n = 13) were current or former members of the U.S. military. The second most common answer was war, which was provided by 24% (n = 12) of respondents. The following traumatic experiences were each listed by 20% (n = 10) of respondents: sexual assault, abuse (with 6% mentioning sexual abuse specifically), and the death of a loved one. Other experiences mentioned included car accidents, near death experiences and taking someone else’ life.
Traumas Respondents Believe May Lead to PTSD.

Note. PTSD = post-traumatic stress disorder.
Individuals at Risk for PTSD
Respondents were asked to provide describe the type of person who may be at the greatest risk for developing PTSD. The most common answer provided was that anyone who experiences a trauma may develop PTSD. This answer was given by 82% (n = 41) of the respondents. The second most common answer was members of the military, which was an answer given by 26% (n = 13) of the respondents. The third most common answer was emergency personnel which was written in by 12% (n = 6) of the respondents.
Describing Individuals With PTSD
When asked to provide words or phrases that would describe someone with PTSD, 8% (n = 4) of the respondents used words/phrases that were coded as relating to mental health stigmas. These words included “dangerous,” “mentally weak,” and “unstable.” Positive words/phrases were used by 18% (n = 9) of the respondents; 16% (n = 8) of respondents specifically used the word “survivor.” Other positively coded words/phrases included “fighter,” “worthy,” “strong,” and “brave.” Negatively coded words/phrases were used by 58% (n = 29) of respondents; these included words/phrases such as “victim,” “tortured,” “troubled,” “lonely,” and “broken.” Neutral statements were used by 24% (n = 12) of respondents. One individual responded by saying, “I would have to meet the individual person, as the illness is not what defines them.” Other neutral responses included “human” and “in need of help.”
Treatment for PTSD
Respondents were asked to identify treatments for PTSD of which they were aware. The most common response was counseling or therapy, which was provided by 74% (n = 37) of respondents. Medication (62%; n = 31) was the second most common answer provided with cannabis, antidepressants, and anxiolytics mentioned specifically. Group therapy/support groups (28%; n = 14) was the third most common answers with specific references to “veteran’s groups,” the “Family Readiness Officer,” and “Military OneSource.” Exposure therapy was provided as an answer by 18% (n = 9) of respondents and social support, meditation, hobbies/activities, and/or exercise were each mentioned in 8% (n = 4) of the responses. Three respondents included references to the importance of including faith in the treatment process. Most respondents included more than one answer to this question, thus total percentages add up to more than 100%. These data are shown in Table 5.
Treatments for PTSD Identified by Respondents.

Note. PTSD = post-traumatic stress disorder.
Perceptions of Treatment
When asked to describe someone who engages in mental health treatment (counseling or therapy) for their PTSD diagnosis, 96% (n = 48) of respondents provided words and/or phrases with positive connotations. The most common answers provided were “strong” (28%; n = 14) and brave/courageous (28%; n = 14). Negatively worded responses included references to the individual being “worried” and that “too few” are seeking treatment. When asked to provide words/phrases to describe someone who takes prescribed medication to treat symptoms of their PTSD, 56% (n = 28) of respondents provided an answer that portrayed the individual in a positive manner. However, 28% (n = 14) of respondents provided words and/or phrases that described the individual negatively. Of these, 42.8% (n = 6) expressed concern about the use of medication with one respondent referring to it as a “bandaid” (Respondent #34) and another stating that a person on medication is a “time bomb” (Respondent #38). In addition, 28.5% n = 4) of those responding negatively to this question stated that medication is “insufficient” to treat PTSD. Finally, 16% (n = 8) of respondents provided an answer that described himself or herself as indifferent or unconcerned about someone taking medication.
Level of Care
Table 6 shows selected quotes from the respondents regarding level of care for U.S. military members diagnosed with PTSD. Responses related to insufficient levels of care were provided by 74% (n = 37) of respondents. The remaining 26% (n = 13) of the respondents stated that they did not have enough information to provide an answer to this question. No respondent provided an answer indicating that he or she felt that the current level of services was sufficient. Of those providing a response, 6% (n = 3) stated that they thought service was improving and 4% (n = 2) stated that they felt services were not being utilized due to the stigma surrounding mental health care within the military.
Beliefs About Services Available to U.S. Military Members for Treatment of PTSD.
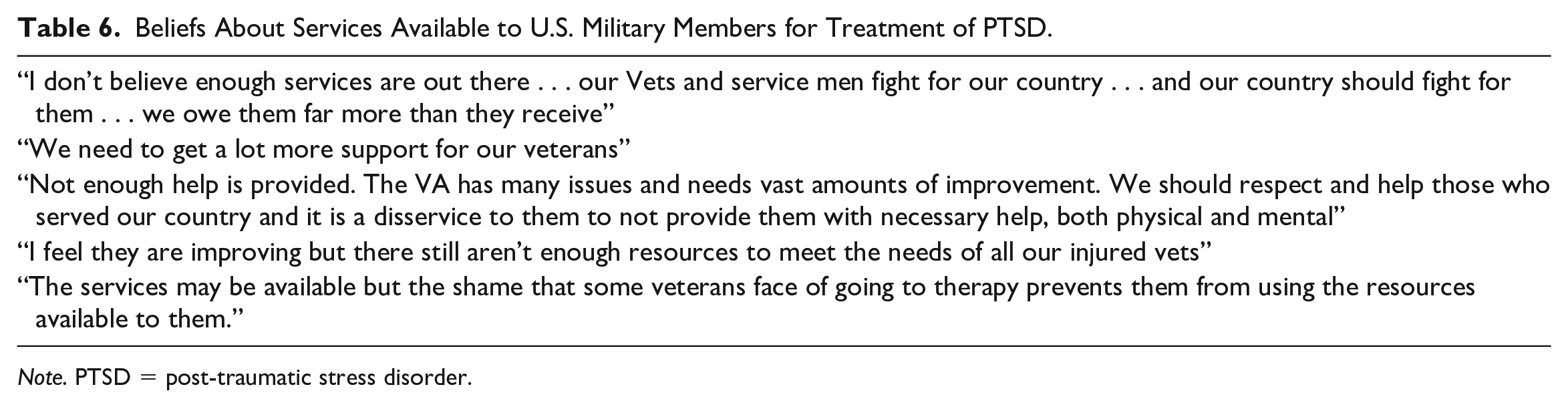
Note. PTSD = post-traumatic stress disorder.
Discussion
The current study sought to investigate the relationship between military service and perception of PTSD by distributing open-ended surveys to military personnel and their immediate family members. Between 10% and 30% of individuals having served in the United States military will develop PTSD at some point during their lifetime (Dohrenwend et al., 2006; Fulton et al., 2015). Identifying the specific information, attitudes, and beliefs regarding PTSD and its diagnosis may aid in the creation of campaigns to increase education and reduce stigmatization of the disorder leading to greater understanding and access to care. In general, health literacy is correlated with an increase in health outcomes (Berkman et al., 2011). More specifically, mental health literacy has been shown to decrease negative attitudes regarding mental illness and increase the social support offered by members of the general public to individuals with mental health diagnoses (Hadlaczky et al., 2014). In addition, Zwanziger et al. (2017) found that knowledge regarding PTSD and its symptoms was associated with an increase in resilience in individuals who have a spouse serving in the military.
When asked to provide a definition of PTSD, the majority of responses were in line with the information found within the DSM-(5th ed.; DSM-V; APA, 2013) reflecting an accurate knowledge regarding PTSD within most of the survey respondents. For example, 60% (n = 30) of the respondents identified the trauma as a defining feature. The DSM-5 states that the “essential feature of post-traumatic stress disorder (PTSD) is the development of characteristic symptoms following exposure to one or more traumatic events” (APA, 2013, p. 274). Some of the respondents (16%; n = 8) referred to the persistence of symptoms over time, which is similar to the information found in Criterion F of the DSM-5 that states that the symptoms must persist for more than one month. Some respondents also stated that PTSD could develop in individuals who witness traumatic events and not only those who directly experience the trauma. This response is also accurate as Criterion A within the DSM-5 states that witnessing the event qualifies as exposure to the trauma. Respondents did include some inaccurate information in their responses. Some respondents referred to PTSD as an anxiety disorder; however, PTSD was removed from the category of anxiety disorders with the publication of the DSM-5 in 2013 and moved to a category on “Trauma- and Stressor-Related Disorders” (APA, 2013). Other respondents stated that PTSD cannot be successfully treated; however, a number of studies have revealed a decrease in PTSD symptom severity following treatment (Beidel et al., 2017; Zalta et al., 2018). One respondent suggested that a “35-year old man consistently at high school football games to relive his moments in life” (Respondent #23) would meet a PTSD diagnosis. This description by itself does not provide any evidence of PTSD symptoms though it is unclear what the respondent may have had in mind when providing their answer. The attempt to “relive his moments in life” may be a coping mechanism for dealing with symptoms of PTSD such as the inability to experience positive emotions or an attempt to avoid distressing memories by seeking out more pleasant ones.
Survey respondents were asked what phrases or images came to mind when they heard or read the term “PTSD.” The most common answer involved war/combat/veterans and the second most common answer involved nightmares. The only specific conflict that was mentioned was Vietnam (written in by two respondents). None of the responses were coded as revealing a stigma associated with PTSD. When asked to list the symptoms of PTSD, the most commonly identified symptoms were trauma related nightmares, sleep disturbances and dissociative reactions/flashbacks. Prior research has shown that an inability to correctly identify the symptoms of mental health conditions reduces the likelihood that an individual will seek help (Wright et al., 2007). Within the current study, the most commonly listed symptoms that do not fit the diagnostic criteria for PTSD included anxiety, panic attacks, depression, mood swings, and substance abuse. However, the terms “anxiety,” ‘panic attacks “mood swings” and “depression” may hold different meanings for mental health professionals than they do for the general public. The terminology patients use to describe their symptoms is important and the use of inaccurate terms may lead to difficulty communicating with a health practitioner and a decrease in the likelihood of receiving a mental health diagnosis (Herrán et al., 1999; D. Kessler et al., 1999).
The most commonly identified experiences that respondents believed could lead to the development of PTSD were combat and war. The high rate of identification of combat and war as traumatic events may be due to the specific population that responded to the survey: all were current or former members of the U.S. military or immediate family of members of military members. In addition, the high rate of identification of war/combat as a traumatic event associated with PTSD may be due to the increase in media coverage of PTSD within the military. Media coverage of PTSD related to war and combat increased 211% between 2006 and 2008 (Armstrong & Olatunji, 2009). The third most commonly identified traumatic experience was sexual assault. Research shows that survivors of sexual assault have the highest rates of lifetime prevalence of PTSD at 50% (Creamer et al., 2001). Not all of the experiences listed by respondents would qualify as traumatic according to Criterion A of the DSM-(5th ed.; DSM-V; APA, 2013). A PTSD diagnosis is appropriate if an individual is exposed to “actual or threatened death, serious injury, or sexual violence” (APA, 2013, p. 271) by direct experience, witnessing, learning of a loved one experiencing trauma or being exposed to aversive details of trauma (such as the experience of first responders). However, some respondents listed being fired from their job, going through a divorce and giving birth to a child as traumatic experiences. None of these experiences (with the possible exception of childbirth if serious complications occurred) would qualify as a trauma that might lead to the development of PTSD according to Criterion A of the DSM-(5th ed.; DSM-V; APA, 2013).
When asked to identify individuals who might be at risk for developing PTSD, the most common answer provided was that anyone may develop PTSD. This answer is suggestive of a lack of stigma regarding the development of PTSD. Survey respondents were also asked to provide words/phrases to describe individuals with PTSD. Only a small number (8%; n = 4) of respondents used stigmatizing language to describe individuals with PTSD. Rather, the majority of responses included words/phrases that displayed “positive” attitudes toward individuals with PTSD. The rate of individuals who meet diagnostic criteria for mental health disorders seeking care is estimated to be only 23% and 40% with a concern for “being seen as weak” cited as the most prevalent barrier (Hoge et al., 2004; Sharp et al., 2015). However, the results of the current study suggest that individuals with PTSD are not seen as “weak” but as “brave,” “worthy,” and “strong.”
When asked to list treatments for PTSD, counseling and individual therapy were the most often cited by the survey respondents. Specific types of therapy listed by respondents included exposure therapy and behavioral therapy (which may be a reference to cognitive behavioral therapy or CBT). The APA and U.S. Department of Veteran’s Affairs (VA) strongly recommend CBT for patients diagnosed with PTSD and between 61% and 82.4% of individuals utilizing CBT as a treatment no longer meet the criteria for PTSD within 6 months (Jonas et al., 2013). In addition, treatment with exposure therapy has shown some of the strongest evidence for improvement of symptoms or loss of diagnosis within patients diagnosed with PTSD. Medication was the second treatment for PTSD most commonly identified by survey respondents with specific references to antidepressants, anxiolytics, and cannabis. Paroxetine and topiramate were found to be among the most effective medications for reducing the symptoms of PTSD (Jonas et al., 2013). Newer research has shown that treatment with cannabinoids has also been associated with PTSD symptom reduction (Bitencourt & Takahashi, 2018; Elms et al., 2018; Lisboa et al., 2019). Overall, the responses on this question suggest that the survey participants were well-informed regarding potential treatments for PTSD.
When asked how they would describe individuals with PTSD who sought out treatment through either therapy or medication, respondents overwhelmingly responded with positive phrases and descriptions. The most common answers provided were “strong,” “brave,” and “courageous.” One of the reasons individuals with a military background reportedly do not seek mental health care is due to stigma surrounding PTSD and other mental health diagnoses (Mittal et al., 2013). However, the results of this study suggest that this stigma may be a self-stigma rather than public stigma. When asked to provide words/phrases to describe someone who takes prescribed medication to treat symptoms of their PTSD, only 56% of respondents provided an answer that portrayed the individual in a positive manner while 28% of provided words and/or phrases that described the individual negatively. For example, one respondent describing a person on medication as a “time bomb.” These results reveal a greater stigma surrounding the use of pharmaceutical interventions than the use of psychotherapy.
In addition to stigma, other identified barriers to treatment included difficulty obtaining care, specifically within the VA health care system (Hundt et al., 2018). The final question on the survey asked respondents about their beliefs regarding the level of mental health care available to service members. Overall, the respondents had negative views regarding care describing it as “insufficient.” Previous research has shown that while the VA offers an adequate level of access to care (Shiner et al., 2012), utilization of that care remains low (Hoge et al., 2014; Lang et al., 2016). Hoge et al. (2014) found that of those individuals meeting the diagnostic criteria for PTSD and seeking treatment, 24% dropped out of treatment, 22% underwent a single visit, and 52% received minimally adequate care. Hundt et al. (2018) found that the most often cited explanations for low utilization of the VA were related to the VA system itself including previous negative experiences seeking medical care through the VA, negative experiences with VA staff, and difficulty accessing the care provided by the VA.
The results from the current study provide important information regarding the commonly held beliefs and perceptions regarding PTSD within individuals with military affiliations. It is important for mental health professionals working with military populations to be aware of these beliefs and perceptions as they may affect the decision to seek and participate in mental health care. Limitations within this study include the small sample size and a population that was mostly affiliated with military service within the U.S. army. A wider range of input from service members affiliated with the U.S. Navy, Marines, Coast Guard, and Air Force would be helpful to understand differences in beliefs about PTSD between the various branches of the U.S. military. Future research may be aimed at designing campaigns to improve the perception of the VA and reducing the stigma associated with treatments for mental health conditions within military populations.
Footnotes
Approval
This research was approved by the Messiah University IRB (Approval Code #2015-15).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research was provided through an internal scholarship grant received from Messiah University.