
Abstract
Different scales have been validated to assess the medication regimen complexity. However, the effect of this complexity on the risk of health care center consultations in patients with drug-related problems is unknown. This study’s objective is to evaluate the association between the Medication Regimen Complexity Index (MCRI) and the number of drugs prescribed and new consultations to the health care system in patients who visit an emergency service due to drug-related problems. This is a retrospective observational study. We included patients >65 years who attended in an emergency service for drug-related problems. To identify variables associated with health care center reconsultation, a multivariate analysis was performed, including demographic and comorbidity variables, number of drugs prescribed, and MCRI value. Two hundred and one patients were included. A significant association was found between the prescription of more than five drugs (odds ratio [OR] = 2.50, 95% confidence interval [CI] = [1.08, 5.79]), an MCRI > 20 (2.98 [1.46–6.09]), and an increase in the number of drugs prescribed (2.87 [1.57–5.21]) and its MCRI (2.06 [1.13–3.77]) at discharge and a new visit to the emergency department. An association was found between the prescription of more than five drugs, an MCRI > 20, an increase in the number of drugs, and in MCRI value at discharge and a new visit to any other health care center. The number of prescribed drugs and the medication complexity of patients who visit the emergency department for drug-related problems was associated with an increase in the number of revisits to the emergency department and to other health care centers.
Introduction
Over the last 40 years, developed countries have experienced a progressive aging of their population, with an increase in the number of patients with multiple chronic conditions and, consequently, the number of patients receiving multiple medications (Colchero et al., 2016; Salive, 2013).
It is known that multiple medications are associated with an increase in hospital admissions and visits to emergency departments, as well as an increase in costs for the health system (Burnier, 2017; Gellad et al., 2011; Peterson et al., 2003; Simpson et al., 2006). Several studies have associated a high therapeutic complexity with a lack of adherence to the treatment, as well as an increase in adverse effects (Mansur et al., 2012; Salvi et al., 2017), especially in elderly patients (Onder et al., 2002). The lack of adherence to the long-term treatment by the patient has been estimated between 10% and 50%, with it being higher in those patients who suffer any adverse event associated with their treatment, as well as in those with more complex treatment regimens (Marcum & Gellad, 2012).
Different scales have been validated over the past few years to assess the pharmacotherapeutic complexity in these patients on multiple medications (Paquin et al., 2013), highlighting among them, the scale published by George et al. (2004). However, the information is limited as regards the relationship of these scales with the likelihood of suffering a drug-related problem (DRP), defined as a situation that causes the appearance of a negative effect associated with the drug (Research Group in Pharmaceutical Care [University of Granada], Research Group in Pharmacology [University of Granada], 2007), including problems associated with the indication (the patient does not use the medicines that s/he needs or uses medicines that s/he does not need), the effectiveness (the patient uses an erroneously chosen medicine or uses a lower dosage and/or a different dosage schedule than required and/or does not continue therapy for the full duration of the treatment indicated), or its safety (the patient uses a higher dosage or a different dosage schedule than required and/or exceeds the full duration of treatment indicated or uses a medicine that causes an adverse drug reaction). Furthermore, the effect of polypharmacy, defined as five or more medications daily (Masnoon et al., 2017), as well as its complexity on the patients who are seen in hospital emergency departments due to a DRP, has still not been established.
For all these reasons, this research study was conducted with the aim of evaluating the association of the complexity of the treatment on repeat visits to the health care system in those patients who visit emergency departments due to a DRP.
Material and Method
A retrospective, observational study was designed. It included patients over 65 years old who visited an emergency department of a tertiary hospital in Spain for any DRP, in accordance with diagnosis made by the physician during the period from June 2017 to June 2018. Those patients who went to emergency department with a DRP secondary to treatment with chemotherapy or hospital dispensed medication were excluded. The hospital has 644 beds, dealing with around 140,000 emergencies annually. The Spanish health care system during this period was based on a co-payments system of both pensioners and working-population, depending on income intervals and with a maximum contribution per month. The identification of patients was made prospectively as a usual activity by a pharmacist attached to the emergency department, based on the information included in the emergency admission and discharge reports obtained at 8 a.m. in the morning from Monday to Friday. The DRPs were classified as necessity, safety, or efficacy by the emergency department pharmacist, based on the criteria established in the Third Consensus of Granada (Research Group in Pharmaceutical Care [University of Granada], Research Group in Pharmacology [University of Granada], 2007).
From the patients included, the reasons for consulting in emergency department were recorded, as well as the number of chronic diseases based on the information obtained from electronic primary care records at the moment of admission, the length of the stay, and the destination on discharge from the emergency department. The number of drugs on admission and at discharge were recorded, as well as the Medication Regimen Complexity Index (MCRI) obtained from the electronic primary care prescription system, which includes regular medications and those used only if necessary, in accordance with the criteria established by George et al. (2004). This index calculates the complexity of the treatment based on the number of drugs prescribed and other factors, such as dosage form, route of administration, dose frequency, or additional instructions given for their use.
To analyze the impact of the complexity of the treatments on the repeat visits of the patients with DRP, a number of steps were followed; these included the effect of the number of drugs, the MCRI at discharge from the emergency department on hospital readmissions, and the number of unscheduled visits to public health care centers in Catalonia (including hospitals, long-term healthcare facilities and primary care centers) at 30 days from hospital discharge, based on the data obtained from the clinical notes computer system shared with the Catalan Health Institute.
Statistical Analysis
The data analysis was performed using the Stata 13.0 statistics program (StataCorp LLC, College Station, TX, USA). The quantitative variables were obtained as mean values and standard deviation (SD) or median and interquartile range (IQR), whereas the qualitative variables were expressed as percentages. The variables between the different groups were compared using parametric (Fisher’s exact test, Student’s t-test) or nonparametric (χ2 test, Mann–Whitney U test) tests depending on the normality analysis of the sample.
To assess the impact of the number of drugs prescribed at discharge and the MCRI on the repeat visits to the emergency department, as well as to the health system, a multivariate logistic regression analysis was performed, with those variables with a value of p < .2 in the previous univariate analysis being included. The following factors were evaluated: age > 80 years, prescribed multiple drugs (defined as more than five drugs, Masnoon et al., 2017), diabetes, heart failure, chronic kidney failure, chronic obstructive pulmonary disease (COPD), cirrhosis, destination of the patient at discharge (residence or home), and a DRP caused by the most common anatomical therapeutic chemical classification system (ATC) therapeutic groups (A: digestive tract and metabolism; B: blood and hematopoietic derivatives; C: cardiovascular system and N: central nervous system) (World Health Organization Collaborating Centre for Drug Statistics Methodology, n.d.). Given the strong association between the number of drugs and the treatment complexity, both variables were introduced separately into the model. For this propose, patients included were divided into two groups based on the following variables: polypharmacy, >5 drugs (Masnoon et al., 2017), greater treatment complexity (MCRI value higher than the median value of all included patients), and an increase in the number of drugs and the MCRI value at discharge. The study had the approval of the Research Ethics Committee of the Hospital (reference no. IIBSP-COD-2018-25).
Results
A total of 201 patients were included (112 females [56.1%]; mean age [SD] = 77.6 [15.3]), identified by the emergency department specialist or the pharmacist in emergency department with a DRP as primary (79.0%) or secondary (21.0%) diagnosis. Their characteristics are shown in Table 1. Twenty-five patients consulted the emergency department due to an effectiveness DRP, 55 (12.4%) due to a necessity DRP, and 131 (65.2%) due to a safety DRP. The main DRP of the patients included were thromboembolic events (15.4%), changes in blood glucose (14.4%), hemorrhagic events (13.9%), sedation confusion (10.9%), and cardiovascular changes (10.9%). The principal therapeutic groups involved in the DRPs included Group A (digestive tract metabolism; 37; 18.4%), Group B (blood and hematopoietic derivatives; 72; 35.8%), Group C (cardiovascular system; 30; 14.9%), and Group N (nervous system; 50; 24.9%) (Table 2).
Characteristics of Patients Included in the Study (n = 201).

Note. IQR = interquartile range; MCRI = Medication Complexity Regimen Index; COPD = chronic obstructive pulmonary disease.
Drugs Involved in Drug-Related Problems of the Patients Included in the Study.

Note. ATC = anatomical therapeutic chemical classification system.
An increase in the number of drugs prescribed at discharge was observed in 82 (38.6%) patients (median = 1 drug [IQR = 1–2]), as well as an increase in their MCRI in 106 (52.8%) patients (mean percentage increase = 27.0% [SD = 21.4%]), with a significant overall increase being observed in the group of patients included, 21.5 (13.1) versus 24.3 (14.3), p = .043.
A total of 70 (34.8%) patients made a repeat visit to the emergency department, and 106 (55.6%) patients required unscheduled visit to health care centers in the 30 days after hospital discharge. Treatment with five or more drugs at discharge, as well as an MCRI greater than 20 points, is associated with a greater number of visits to emergency department and health clinics (Figures 1 and 2). The increase in the number of prescribed drugs, as well as their complexity, is also associated with a higher number of repeat visits to emergency department (drugs = 48.3% vs. 24.6%, p < .001; MCRI = 42.2% vs. 26.1%, p = .017) and health clinics (drugs = 69.0% vs. 40.4%, p < .001; MCRI = 62.4% vs. 41.3%, p < .001) at 30 days from discharge.

Percentage of patients who visit the emergency department 30 days after discharge according to the MCRI value and the number of prescribed drugs.

Percentage of patients who visit health care centers 30 days after discharge according to the MCRI value and the number of prescribed drugs.
The results of the univariate analysis are shown in Table 3. In the multivariate analysis, a significant relationship is observed between the prescription of more than five drugs at discharge (odds ratio [OR] = 2.50, 95% confidence interval [CI] = [1.08, 5.79]), an MCRI > 20 (2.98 [1.46, 6.09]), and the increase in the number of drugs (2.87 [1.57, 5.21]) and in the MCRI (2.06 [1.13, 3.77]) and repeat admission in emergency department (Table 4). As regards the number of consultations in any health center, the multivariate analysis found a relationship between these and the prescription of more than five drugs at discharge (2.74 [2.95, 12.23]), an MCRI > 20 (4.56 [1.36, 15.24]), and the increase in the number of drugs (3.78 [1.58, 9.00]) and in the MCRI value (3.01 [1.72, 5.92]).
Results of the Univariate Analysis.
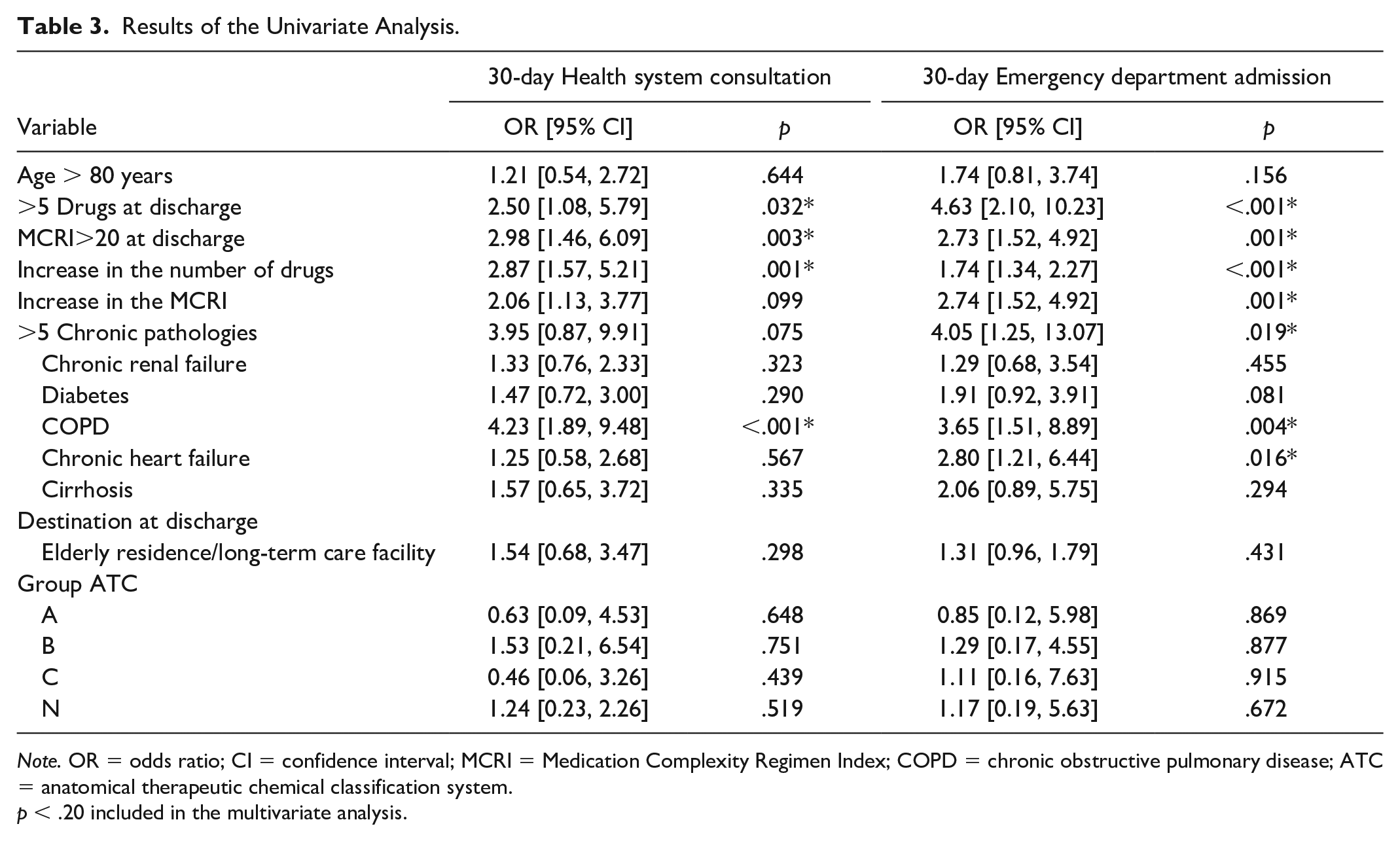
Note. OR = odds ratio; CI = confidence interval; MCRI = Medication Complexity Regimen Index; COPD = chronic obstructive pulmonary disease; ATC = anatomical therapeutic chemical classification system.
p < .20 included in the multivariate analysis.
Results of the Multivariate Analysis.

Note. OR = odds ratio; CI = confidence interval; MCRI = Medication Complexity Regimen Index; COPD = chronic obstructive pulmonary disease.
p < .05 is statistically significant.
Discussion
According to the results of this study, the increase in the number of drugs, as well as in the therapeutic complexity of those patients who go to emergency departments due to a DRP, is associated with an increase in the number of repeat visits to the health system.
DRPs are a very prevalent health issue. Different studies have shown that they are implicated in between 20% and 40% of the visits to emergency departments, and that around 70% of the cases are considered avoidable (Baena et al., 2006; Castro et al., 2013).
In our study, the majority of patients who consulted due to a DRP were elderly, with a mean of nine drugs, an MCRI of 21, and 91% had more than five chronic conditions, being a patient population with significant comorbidity and multiple medication and, therefore, highly vulnerable to have a DRP.
Polypharmacy has been widely associated with an increased risk in suffering a DRP, and the MCRI has been associated with an increased number of admissions in patients receiving multiple medications (Oscanoa et al., 2017; Tesfaye et al., 2019; Wimmer et al., 2014). However, it should be noted that our results show, for the first time, the impact of pharmacotherapeutic complexity on those patients who consult emergency department due to a DRP.
It should also be noted that a high percentage of patients of our study, after consulting due to a DRP, paradoxically experienced an increase in the number of prescribed drugs and in the complexity of their treatment at discharge, despite that the inappropriate use of a drug was a direct or indirect factor that caused their emergency department visit.
Patients who had already suffered a DRP leading to a visit to the emergency department may be considered as high risk for new DRPs. Given that the increased risk of suffering adverse events occurs in the first days or months after a new prescription, a rapid medication review is needed for the long-term treatments in patients who visit emergency departments due to a DRP, as well as education on the new treatments prescribed, to minimize the appearance of new complications.
According to the results obtained in this study, an increase in the number of drugs prescribed is associated with an increased risk of readmission. Treatment simplification may be an option to prevent new consultation to health care centers. Several studies have found a relationship between treatment simplification and the increased adherence to it, despite that the results in terms of clinical variables and quality of life are still controversial (Iskedjian et al., 2002; Reeve et al., 2017; Ulley et al., 2019). Identification of sequential drug prescribing that could represent a prescribing cascade (Rochon & Gurwitz, 2017) and adjust the treatment to the new clinical situation of the patient after the consultation must form part of the strategies to improve the quality of life of patients with multiple conditions (Brath et al., 2018). In this sense, the guidelines published to help in the de-prescription are a useful tool, and in addition, they advocate taking into account the opinions of the patients in this process (National Institute for Clinical Excellence, 2015; Scottish Government Model of Care Polypharmacy Working Group, 2015).
It should be pointed out that the patients included in our study were of advanced age, with a high percentage with cognitive impairment, although an appropriate evaluation of the degree of disability could not be obtained from medical records. In this patient group, the establishing of an effective communication with the doctors responsible for the patients outside the hospital environment would ensure a rapid optimization of treatment on an essential factor to avoid repeat consultations. It has been demonstrated that a significant percentage of patients receive insufficient information on their new treatment at hospital discharge (Glintborg et al., 2007; Hesselink et al., 2013). Good communication with the different care levels has a positive impact on the control of chronic diseases (Coll-Vinent et al., 2007; Polnaszek et al., 2015), thus being a key element to prevent new decompensations in patients with chronic conditions after hospital discharge.
Among the limitations of our study, is its single-center retrospective character. We have not evaluated other parameters that have been associated with adherence to the treatment, such as the educational and socioeconomic factors of the patients included (Kardas et al., 2013). However, the characteristic of the Spanish health care system makes the accessibility to drugs different from other countries. Thus, the number of drugs prescribed in patients included may be different from patients in others health care systems. However, polypharmacy is a frequent phenomenon described in all developed countries (Colchero et al., 2016; Salive, 2013). Our study has mainly included patients with DRPs of ATC Groups A, B, C, and N. This fact could mask the effect of other therapeutic groups in patient’s consultation to health care centers. In fact, more the 20% of patients included suffered from COPD. Respiratory inhaled therapy adds to the complexity of the treatment, and poor adherence has been associated with an important number of visits to emergency departments (Van Boven et al., 2014). However, poor adherence to inhaled therapy is included as cause of decompensation rarely in emergency department discharge forms. However, A, B, C, and N therapeutic groups are main ones responsible for emergency department admissions according to different published studies (Baena et al., 2006; Castro et al., 2013; Oscanoa et al., 2017; Shehab et al., 2016; World Health Organization Collaborating Centre for Drug Statistics Methodology, n.d.). Therefore, our results could be applicable to the majority of the population.
To sum up, the complexity of the treatment and multiple medications are associated with repeat health care center visits in patients who attend emergency departments due to a DRP, and must be taken into account when considering treatment at discharge in this patient group.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study had the approval of the Research Ethics Committee of Hospital de la Santa Creu i Sant Pau (reference no. IIBSP-COD-2018-25).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Spanish Ministry of Health (Carlos III Health Institute, ISCIII) FONDOS FEDER through the Fondo de Investigación para la Salud (FIS) (PI18/00889).