
Abstract
Bereavement and spousal loss lead to emotional and practical problems, especially for those in failing health. The aim of this study was to explore the meaning of bereavement in older adults after the death of their spouse. The participants took part in in-depth interviews. The themes and sub-themes were identified using a hermeneutic approach. One overall theme, Struggling to maintain pride and dignity; three themes; and six sub-themes emerged. The first theme, Understanding health decline, included one sub-theme: Difficulty asking for help. The second theme, A lonely painful struggle, had three sub-themes: Striving to avoid feeling sorry for oneself, Searching for meaning when life becomes meaningless, and Sensing that one’s spouse is present. In the third theme, Feeling misunderstood in the dialogue with others, two sub-themes emerged: Longing for support to achieve inclusion and Togetherness is the best medicine. It is vital to prevent older adults from carrying a permanent state of grief with them for the rest of their life.
Introduction
Bereavement is considered particularly challenging for older persons because of concurrent losses outside a bereavement context (Moss et al., 2001; Naef et al., 2013). Bereavement and spousal loss lead to many emotional and practical problems, especially for those in failing health, who struggle with their own limitations when performing everyday activities (Naef et al., 2013). Research on the experience of bereavement has been applied in fields such as psychology, philosophy, and art, where grief and loss are examined in ways that enable bereaved persons to search for meaning after the loss of loved ones (Gillies & Neimeyer, 2006). These experiences can split the internal world by shattering one’s most fundamental assumptions (Janoff-Bulman, 2010). According to Janoff-Bulman (2010, p. 133), one must build a non-threatening assumption that contributes to a resolution of the survivor’s existential dilemma. Bereavement should be seen in a positive light where the person can face the situation with dignity (Janoff-Bulman, 2010, p. 277). The necessity of meaning making on the part of bereaved older adults is supported by a review study by Holm and Severinsson (2012), which suggests that older widows struggle to perceive meaning and numb their emotional pain in an attempt to control their feelings. They tried to maintain close emotional relationships and meaningful activities in a process of self-management dominated by resilience (Holm and Severinsson, 2012).
Bereavement has been linked to social, mental, behavioral, and physical issues, consistent with a stress-induced weathering process (Das, 2013). Thus, bereavement is seen as a major stressor that triggers problems such as depression and complicated grief (Shear et al., 2011).
Holm et al. (2019) examined factors that influence the health of older widows and widowers. One of the themes that emerged was emotional challenges related to experiences of bereavement, depression, and anxiety, which was based on the sub-theme social support as the main strategy for coping with emotional pain and suffering. The second theme was struggling with poor physical health (Holm et al., 2019). In their longitudinal survey, Van den Berg et al. (2011) found that bereavement affected health, because healthy years were replaced by years with chronic diseases. The strong effects of bereavement suggested that monitoring and/or interventions shortly after spousal loss were important for the length and quality of life of older individuals. Bereavement has also been associated with health, age, and gender where being a widower, being older, less well educated, and functionally healthy were associated with better health (Krochalk, 2008). Sasson and Umberson (2014) found no gender differences in bereavement effects on depressive symptoms in either the short or long term. The sample included widows/widowers aged from 51 to 61 years. When regard to gender and bereavement, Martin and Doka (1996) suggested a masculine and feminine pattern of grieving. In the masculine pattern, individuals exhibit more cognitive and active responses to grief, while the experience and expression of grief in the feminine pattern is more emotive. When describing the masculine and feminine patterns, Martin and Doka (2000) moved away from the notion that grief responses are distinctly gender-related. Their perspective places less emphasis on gender as a critical determinant of how individuals grieve and instead proposes that there is a continuum of grieving styles from intuitive to instrumental (Martin and Doka, 2000). The critical point is that while gender is influential, it does not determine grieving styles. Martin and Doka (2000) found a more nuanced understanding of the individuals’ pathways of grief. Doka and Martin (2011) based their understanding on two patterns of grieving. One is an intuitive pattern where individuals experience grief in an emotional way. Intuitive grieving is oriented toward the expression of emotions or affects. The other pattern is termed instrumental, in which grief is experienced physically, such as in restlessness or cognition. These two patterns can be seen as end points on a continuum. The instrumental pattern is typical of the way many men grieve, due to contemporary patterns of male socialization. Doka and Martin (2011) emphasized that there is no clear relationship between gender and grieving patterns, as women can exhibit an instrumental style, while both widows and widower can demonstrate intuitive patterns. As highlighted by Doka and Martin (2011), these patterns are influenced by gender, but not determined by it.
High rates of institutionalization and an increased mortality risk are found in widowed older adults compared to their non-bereaved peers (Elwert & Christakis, 2008; Onrust & Cuijpers, 2006). Mortality and risk of death have been associated with the stress caused by the bereavement on persons who have lost their spouse (Alter et al., 2007; Stimpson et al., 2007). The highest risk of death has been reported among widowed adults aged 65 years and older in the 24 months after the death of their spouse (King et al., 2017). The likelihood of a widowed person dying has been called the “widowhood effect” and is an example of the influence of social relationships on health (Elwert & Christakis, 2008). In addition, gender and age differences have been found in descriptions of bereavement and risk of death. A meta-analysis by (Shor et al., 2012) revealed that as age increased, hazard ratios decreased more rapidly for widowers than for widows. (Fang et al., 2012) found that for widowers, the bereavement and spousal loss-related mortality increased with lower baseline probability of death, particularly from cancer and circulatory diseases. For widows, the widowhood-associated risks seem fairly homogeneous. Another study by (Shah et al., 2013) found that unexpected bereavement has a greater impact on the risk of death preceded by chronic disease. Thus, a decrease in physical and mental health related to bereavement is evident. The findings highlighted the value of preparing older adults for the death of a spouse with known morbidity and providing extra support for those who experience a sudden and unexpected bereavement (Shah et al., 2013).
Two studies revealed that the use of a support group reduced grief severity (Bergman & Haly, 2009; Ghesquiere et al., 2013). Stroebe et al. (2001) described lack of social support, life routines, and financial status as the most stressful experience related to bereavement. Naef et al. (2013) demonstrated that the need for social support appears to be related to a sense of loneliness, as well as difficult times of the day and year. Changes in relationships with significant others are described as both a challenge and a resource for older widows and widowers. It was also found that older persons maintain connections with their deceased spouse (Naef et al., 2013). Collins (2017) explored the personal communities of a group of older widowers. The findings illustrate that some older widowers have very restricted personal communities, which puts them at greater risk of loneliness and social isolation (Collins, 2017).
Some qualitative studies have explored how bereavement influences the everyday life of older widows and widowers. Collins (2014) revealed that the themes that emerged were related to Christmas celebrations, family friction, dependence, additional losses, over-commitment, passivity, and feeling different. Li (2007) focused on recovering from bereavement in later life by investigating how widowhood influences subsequent voluntary subsequent willingness to participate as a volunteer and the possible moderating effect of voluntary participation in coping with the death of a spouse. The results revealed a greater likelihood of pursuing voluntary roles a few years after the death of the spouse. Working as a volunteer after spousal loss protected against depressive symptoms and an increased/a greater number of volunteer hours enhanced self-efficacy (Li, 2007).
In the research mentioned in this section, bereavement and spousal loss in older adults has been described as emotional pain, stress, depression, anxiety, grief, loneliness, lack of social support, mortality, and risk of death as well as physical illnesses and problems. Few studies seem to focus on the meaning of bereavement in older adults after the death of their spouse. The intention behind this study is thus to increase understanding of spousal loss and bereavement in older adults.
Aim
The aim of this study was to explore the meaning of bereavement in older adults after the death of their spouse.
Methodology Section
Design
An exploratory design with a hermeneutic approach was used. This design is both a philosophy and a mode of interpretative reading of the text. The authors explored older persons’ experiences of bereavement, focusing on spousal loss. Such an approach requires that the authors are aware of their own pre-understanding (Gadamer, 2004). In this study, the authors’ pre-understanding is based on their theoretical and practical knowledge gained from their professional experience as mental health nurses (A.L.H. and E.S.), an anesthesia nurse (A.B.), clinical supervisors (A.L.H., E.S., and A.B.), and researchers (A.L.H., E.S., and A.B.).
Participants
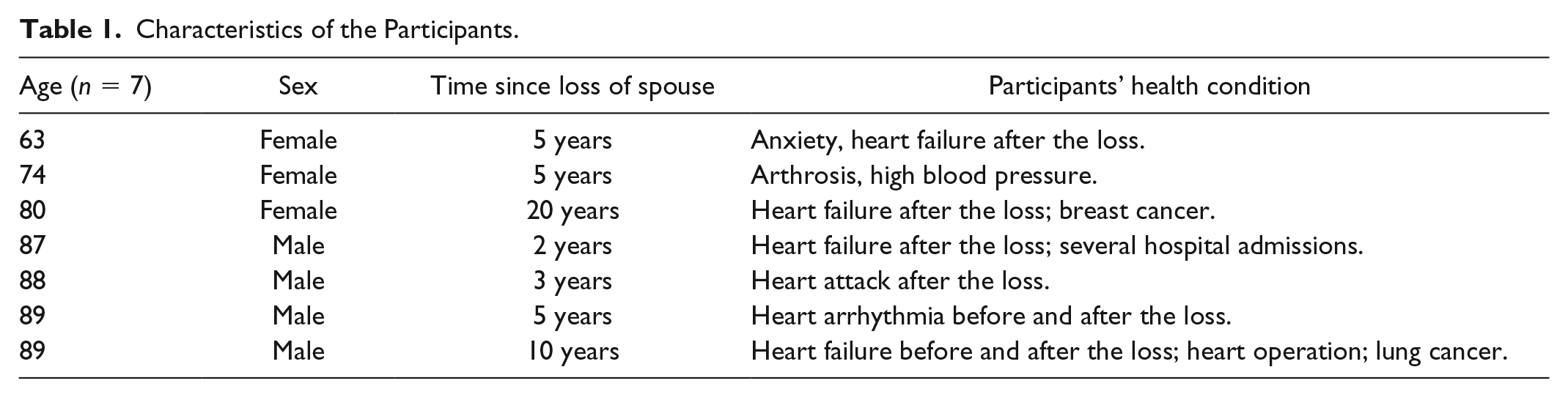
Four men and three women were recruited by the leaders of a senior center in a county on the West Coast of Norway. One inclusion criterion was having lost their spouse during the last 5 years. On several occasions, the first and third author (A.L.H. and A.B.) provided information about the project in a senior center. However, after several months, they were still unable to find a sufficient number of participants who had lost their husband/wife during the last 5 years. A second inclusion criterion was that that the participants should be aged over 65 years. As a result of the difficulty finding a sufficient number of participants both of the above-mentioned criteria were excluded (see Table 1). Therefore, the inclusion criteria were as follows: able to speak and understand the Norwegian language, no cognitive deficit, living in a community in Norway, and over 60 years of age.
Characteristics of the Participants.
Interviews
This study used in-depth interviews (Polit & Beck, 2017). Each interview lasted for 1 to 2 hr and took the form of a dialogue with the participant (Gadamer, 2004). The first and the third author (A.L.H. and A.B.) encouraged the participants to contribute to the dialogue about their experiences of bereavement and asked them the following question: “Can you please tell me how you manage your everyday life since the death of your spouse?” Sometimes the participants found it difficult to describe their experiences and stated that they had few words to express their feelings related to the mourning process, especially the men. It was important to make the participants feel safe and some of the time was used to discuss other things, such as their previous work. The interviews were audio-taped and transcribed verbatim.
Hermeneutic Interpretive Analysis
The interpretation of the text can be seen as a process within the hermeneutic approach. In the first step, the text was structured into an analysis that can increase understanding of the impact of spousal loss on older adults. The hermeneutic research method developed by Fleming et al. (2003) was used. The text was read by the first and second authors to obtain an overall understanding. In addition, a summary of each interview was performed in which meanings and possible themes were explored. In this first reading, the participants’ statements guided the understanding of spousal loss.
The second step included an investigation of the sentences to deepen the initial understanding of the text (Fleming et al., 2003). The first and second authors read the text for a second time, writing codes that described the text in other words in an attempt to expand the understanding of what the participants had said. Several themes emerged that could be representative of the underlying meaning of the sentences in the summaries.
According to Fleming et al. (2003), the third step is important because the researcher returns to the whole text and tries to deepen the understanding of the inherent meaning. The authors thus read the interview text a third time to capture the underlying meaning of the emerging themes. This step of the analysis has also been described as finding the “hidden meaning” of the text (Porter & Robinson, 2011, p. 121).
The fourth step concerned identifying and interpreting the theme and sub-themes, followed by reaching consensus on the essential meaning and understanding. This was a time consuming phase but important for a common understanding of the whole text. The themes and sub-themes were then searched for an abstraction that captured a common understanding.
Trustworthiness
The first and the second authors performed the interpretation of the text, while the other authors critically reviewed the interpretation, thereby increasing the credibility and confirmability of the emerging themes and sub-themes. Trustworthiness is related to confidence in the interpretation and analysis (Polit & Beck, 2017). Discussion of the themes and sub-themes was a process aimed at finding the most suitable interpretation. The authors attempted to identify meaning units that best represented the participants (Denzin & Lincoln, 2008). Using the participants’ own words enables the reader to decide whether or not the interpretation is credible (Holm et al., 2013).
A limitation of this study might be the fact that the participants ranged in age from 63 to 89 years. In addition, their ability to remember events could be a cause of concern especially as many of the participants were in their eighties. Another limitation could be related to the time that had passed since the death of the spouse (see Table 1).
Ethical Considerations
The study was approved by the Norwegian Social Science Data Services (NSD) (No. 5553) and carried out in accordance with the ethical guidelines for nursing research in the Nordic countries (Northern Nurses Federation, 2003). The first and third authors conducted the interviews in a sensitive manner to decrease the older persons’ feelings of grief related to the lived experiences of bereavement (Liamputtong, 2011). The older persons were provided with detailed written information and signed a consent form. They were assured that their name and identity would not be disclosed and that they had the right to withdraw at any time. All data were stored in a locked and fireproof filing cabinet.
Results
Struggling to maintain pride and dignity, three themes and six sub-themes emerged. The first theme, Understanding health decline, included one sub-theme: Difficulty asking for help. The second theme, A lonely painful struggle, had three sub-themes: Striving to avoid feeling sorry for oneself, Searching for meaning when life becomes meaningless, and Sensing that one’s spouse is present. In the third theme, Feeling misunderstood in the dialogue with others, two sub-themes emerged: Longing for support to achieve inclusion and Togetherness is the best medicine (Table 2).
Overview of Overall Theme, Themes and Sub-Themes.

Struggling to Maintain Pride and Dignity
Becoming a widow or a widower in old age (aged over 65 years), seems to involve maintaining one’s pride and dignity to understand a chaotic world. According to our findings, the meaning of bereavement can be understood as the participants’ attempt to maintain both intrapsychic and social aspects. An older person often lacks certain skills and has difficulty understanding the value of help in their everyday life. Loneliness and anxiety seem to be a part of the bereavement process and one can experience that life is no longer worth living. One attempts to maintain one’s pride and dignity by not asking for help from children, friends or professionals. The widowed person struggles to avoid feeling sorry for herself/himself and being perceived as a victim.
Understanding Health Decline
Most of the participants stated that they had to force themselves to understand their health decline. Many of them revealed that they suffer from physical health problems such as high blood pressure, heart disease, and arthritis (Table 1). All of the widowers and two of widows had undergone surgery for heart disease after the death of their spouse. One of the widows stated, I have had several heart attacks after the death of my spouse. I have also had problems with my knees and shoulders, but I really want to manage myself and do not want to bother anybody with my health problems.
Others mentioned the difficulty of having a big house when one is in poor health and two had decided to move to a smaller apartment, making it easier to manage household tasks.
One of the widowers stated, After my wife died I got a heart attack. Both of these two separate experiences have influenced my health condition. I have had two heart operations. In addition, I had lung cancer and had surgery for that too.
A widow expressed, I struggle with arthritis and ankylosing spondylitis. In addition, I also had cancer and this is something that will never leave me. I try not to think about it, but it seems to be stuck in my head. So my physical health is not always good, but I do not give up, because I think of people who suffer more than me. It has nothing to do with being tough, but rather something you accept and have to deal with.
The participants did not complain much about their mental health decline. However, some explained that mental health was related to darkness that often comes in the evening or at night.
A widower stated, I struggle with my mental health, especially in the evening when I am alone, many thoughts go through my head. I try not to think too much, but sometimes I cannot sleep when I think too much.
Another widower commented, Mental health, what is that? I know nothing about that. It has something to do with the mental and not the physical. I have no problem with it.
Difficulty asking for help
Being too proud to ask for help was described as a problem when one’s health was poor. Most of the participants revealed how difficult it is to admit that one needs help from significant others, friends, or health care professionals. One participant expressed, Many people asked if I needed help. But I never said yes, I answered that I could manage myself. It is so stupid.
Most of the participants did not want help from the health care services. Health care professionals were described as working in accordance with the law and procedures, but not always using their head. One participant had experienced health care professionals who refused to assist older patients in their home. This participant was denied help because the homecare professionals did not approve a decision about her or his need for help and stated, The healthcare professionals told me why they cannot help me with this or that based on law and procedures. This refusal does not help me to makes me wonder what view the healthcare services have of human beings.
The participants experienced themselves as independent persons. However, they had problems with the routines, when for example, a different health care professional came each day or a new health care professional offered to help them with showering or other intimate needs. One stated, I have a problem with the healthcare professionals when they promise to come early in the morning, but do not turn up until eleven o’clock. Am I expected to sit around waiting for hours? No, it would be horrible! I often go to the elderly centre to eat or buy a meal to take home. Then I have dinner for two days. I do not work anymore so I do not need so much food. And my daughters bring me some food occasionally. However, I do the shopping myself. Sometimes I manage to cook a dinner when I want to eat something else.
The same participant reported that he would like a technical device where the health care professional could check on a monitor to see if he was asleep or not. He explained, It would be much worse if someone wakes me up after I fall asleep. I would experience that as an assault. And after such an experience I would never get any sleep.
A Lonely Painful Struggle
Several of the older adults described the initial period of widowhood as a lonely struggle where they felt sad and isolated. One of the widows stated, It was like being inside a bubble where everything outside was foggy. It was a tough time. I ask myself why he died before me. Why him and not me?
This widow was prescribed medication by her general practitioner. She felt agitated and nervous. The agitation was physical. Another widow stated, I do not mean you don’t have to grieve. However, I need to go through the grieving process alone. And it is how you go through it alone that is important for the future. Who can I complain to? Many people experience grieving the same way as I do. If I complain to someone who has not had the same experience, she/he will not understand what I am complaining about. Only by having the same experience can a person discover the truth about grieving. My struggle to manage everyday life involved becoming aware of my responsibility for the new situation of being alone in the world. A struggle to survive and try to manage my everyday life.
This struggle was described as a long process where one gradually achieves a sort of self-awareness.
Striving to avoid feeling sorry for oneself
Most of the older adults reported that they did not want to be seen as someone who complains and feels sorry for themselves. They had to pull themselves together. When feeling sad they explained that they forced themselves to stay at home. One of the participants stated, I have to stay at home when I suffer too much. Sometimes I feel that I do not want to live anymore. I want to give up, I admit that.
Some mentioned that they do not expect nor want significant others to take care of them, but wish to manage their life themselves. One of the participants explained, I want to be responsible for myself. I do not want others to take over. I tell myself that living life like this is my destiny. I do not want to be “poor dad.” And my daughters understood me.
Searching for meaning when life becomes meaningless
The participants related that when one is alone there is nothing that can be done about it. One has to be thankful for previous experiences and memories. Voluntary work was described as something that gives meaning to life and allows one to help other people. One participant stated, I can help and as it is voluntary work I get no money, but it gives me a feeling that my life is meaningful.
Others revealed all the positive things that happened in their voluntary work and explained how meaningful such work is. One participant commented, Since my husband died suddenly several years ago I have been involved in a children’s home in eastern Europe.
The participants revealed how they searched for hope and continued with daily life. One of the women used the following words to describe what she meant: You have to find the light yourself, find moments that light up your everyday life and do something you find positive.
Many of the participants stated that they sometimes feel that life is meaninglessness and not worth living. One of the widowers expressed, “Why should I go on living?” but most of the participants believed in God or that fate had decided that this is their life. One of the widowers stated:, You are tired of living. Such thoughts come when I am tired. It is not too serious. It has something to do with being tired of life. I do not think I could have shot myself.
This statement revealed that the widower felt that life is meaningless sometimes.
Sensing that one’s spouse is present
Two of the participants related that they often have a feeling that their spouse is still with them. One of them found this comforting: Sometimes when I am watching TV I fall asleep for a while and then I hear her calling my name and I wake up. So I feel as if she is with me all the time.
The other participant explained, I keep having the same dream that he is back. He is coming and suddenly I wake up thinking “oh dear now you are going crazy.” I see him clearly on the road where we lived, but the children are small. At other times I feel as if he is sitting in the chair looking at me, but the worst thing is when I feel him at my back when I am in bed.
This participant did not feel that this was positive. She was not scared, but explained that such feelings could be related to the fact that her late husband was very demanding and extremely ill before he died.
Feeling Misunderstood in the Dialogue With Others
Most of the participants stated that they sometimes felt misunderstood in the communication and dialogue with other people. They felt stigmatized and experienced discrimination after the loss of their spouse. One of the widows related that she was invited to join a so-called grief group. She had no interest in joining such a group and found the advice given by the professional moderator inappropriate: He told me that I was lucky to have a grave to go to. He told me to think about others who do not have a grave such as divorced people. I lost my temper and answered him like this: Do you really compare the death of my spouse with a divorce? I then added that he must never say things like that to anyone.
Others stated that people avoid talking to them when, for example, they meet on the street. They do not experience empathy from others. One of the participants said, People behaved very strangely as if I had done something wrong. Some even asked me: “Are you here?” I remember answering: “Do I not have the right to be here?” Others said things such as: “Oh, it looks as if you are coping well” as if that was surprising.
Longing for support to achieve inclusion
Most of the participants described how they were longing for support to achieve inclusion. Some mentioned membership in various organizations as playing an important role in their self-management in the initial period after their bereavement. One of the older men stated, The care I perceived was extremely important. People supported me in many ways.
They described the value of meeting people and attending lectures, stating that they have a responsibility to do something themselves to regain meaning in life. Although most of the participants reported positive experiences, it was not the case for all of them. One of the men related: I wish that the people in the organization of which I am a member would make a greater effort to include me. I feel like a stranger and do not perceive any contact. I experienced sitting alone at a table all the time.
Some told about friends who did not remain in contact after the bereavement. This mainly concerned couples with whom they and their late spouse had spent time occasionally. One of the participants explained, There were some couples who we did things together with now and then, but they disappeared after my husband died and I no longer have any contact with them.
Others mentioned that meeting people is more difficult when you grow old. In the past, they knew many people in the city. Nowadays they could walk through the city and nobody knew them and they knew nobody. One of the men stated, Most of the people you knew are gone when you are old.
Togetherness is the best medicine
In contrast to the quotations presented above, some of the participants told themselves to think positively and tried to socialize. Most of them commented that the best thing is meeting other people with the same attitude or values and finding a way of giving something to others. One stated, I really do not want to be a burden to anyone.
They wanted to be a resource. Some of the participants went to church on Sundays. They explained that the care they receive in the church is helpful because they no longer function as well as when they were younger. Some use a rollator and have joined a physical training group. One of the widowers stated, Afterwards we go to a café where some eat dinner and others have a cup of coffee. The socializing and chatting after the training is good and can last for two or three hours. This is helpful.
Another widower expressed, I decided to sell my house because I do not want to be a burden for my children. This house in the middle of the town has a lift and everything is on the same floor, so I have no stairs to climb. The future seems brighter because of this. I do not want to be a burden to my family if I get problems with my legs and cannot walk for instance. My daughter phones me every day to hear how I am managing.
The participants spoke about how they missed their spouse, especially in relation to the events of daily life and having someone to talk to. Someone who meets you at/when you open the door who is interested in you and asks how you feel and how your day has been. One of the widowers stated: I told my wife things that went on in the meeting for instance. What the people talked about. But also small things such as what my day was like. The worst thing about being alone is that you have no one to talk to.
One of the widows commented, I can tell about one episode three months after my husband died. I went to a meeting where there were a lot of people I knew. They looked at me as I had done something wrong. One came up to me and asked: “Are you here? It seems as if you are coping well” ‘Yes I am here I replied. Do I not have the right to be here?’ I have met such attitudes several times. People behave in strange ways. There are twenty four hours in a day and at other times where I do not go outside the door, so no one knows how I struggle.
The results revealed that spousal loss is an on-going struggle even several years after the bereavement. The emotional problems as well as the longing for inclusion highlighted the social aspects of bereavement. The participants did not report that no bereavement groups were available.
Discussion
The attempt to gain an understanding of the meaning of bereavement for older adults by means of interviews revealed one overall theme: Struggling to maintain pride and dignity. It seems to be a lonely struggle as the participants appeared to lack adequate words to describe their environment and emotions. Their world is shattered and the future appears uncertain and difficult to understand. They appear to lack the necessary skills to handle both emotional and health problems. The older adults seem to perceive themselves as stigmatized and discriminated against because they are no longer productive and active agents of society. Not being considered an active and productive member of the community can be understood as ageism, where the where older people are seen as unproductive and useless (Officer & de la Fuente-Núñez, 2018). Ageism tends to be socially accepted and unchallenged because of its implicit and unconscious nature (Cuddy et al., 2005; Levy & Banaji, 2002). Ageism can thus be understood as the need to maintain pride in an environment where one feels excluded by other people. Pride has been described as an emotion and a way of being more conscious of oneself with intrapersonal characteristics (Tracy & Robins, 2004, 2007; van Osch et al., 2018). But it has also been characterized as a social emotion that revolves around about one’s relationship with others (van Osch et al., 2018, p. 404). The emotional meaning of pride seems to vary across cultures and has been associated with positive valence and potency (van Osch et al., 2013, 2018). Most studies ignore the social context in which emotional experiences take place (Fischer & Van Kleef, 2010). Maintaining pride cannot be seen as something that only happens once, as every day seems to be a battle to maintain one’s status (Tracy & Robins, 2007). In this struggle, pride and dignity can be of the utmost importance. Dignity can be related to pride, as it is understood as feeling valuable in relation to others (Haddock, 1996). Thus, the social aspects of dignity seem obvious. However, the findings in our study revealed that dignity is a feeling of being valuable in relation to oneself. This meaning of dignity can be related to self-respect, which is dependent on a sense of importance both in relation to self and others (Nordenfelt, 2004). As in our study, the older adults in Nordenfelt’s (2004) study perceived themselves as dignified persons who appear to do their best to act according to their own moral law to increase their self-respect. In our study, the findings revealed that dignity can be understood and interpreted as an inner feeling of self-respect. Older adults can exhibit a behavior they consider right for being deemed valuable in the eyes of self and others (Nordenfelt, 2004).
Understanding health decline, may be exacerbated by the fact that older adults find it difficult to ask for help. Although their health decline was obvious they were unwilling to admit to themselves and others that they needed help. They seemed to be exhausted and stated that it was best to remain alone. Health decline as described in the present study has often been associated with bereavement and loss (Aniruddha, 2013). Loneliness and lack of energy increase the need for help and the individuals involved struggle to understand what to do. Stress can increase health problems due to negative behaviors such as smoking (Klungsøyr et al., 2006), alcohol use (Davis et al., 2008), poor sleep and physical inactivity (Berger et al., 2009). Stressors may trigger a broad process involving social relationships, poor health and biological problems (Geronimus et al., 2006). Research has demonstrated that experiencing loneliness after a loss decreases opportunities for self-management, although not all social relationships seem to satisfy emotional needs (Holm & Severinsson, 2012; Janke et al., 2008).
A lonely and painful struggle seems to be a state in which the participants were isolated, strove to avoid feeling sorry for themselves, searched for meaning and sensed the presence of their spouse by which they hoped to prevent the development of mental health problems. Pretending that the pain does not exist may be dysfunctional in certain situations, but can also be a way to survive bereavement. Estrangement can be described as an existential lack of self-management and understood as emotional pain and suffering, where the realization of one’s existential aloneness becomes visible and alienates the older person from herself/himself (Holm et al., 2013). In this estrangement, there seems to be a sort of invisible blanket between the world and the individual and loneliness can be a step up from a sense of estrangement. Such persons strive to avoid feeling like a “fifth wheel” in social situations, a phenomenon that is not related to age. Research has revealed that the pain of despair and bereavement can be a state where one attempts to control one’s emotions. Grief and social withdrawal can increase the stress caused by bereavement that can be seen as representing social deficits (Thoits, 2010). The findings of this study revealed that the participants were striving to avoid feeling sorry for themselves. Feeling sorry for oneself can be a part of self-pity that is often perceived negatively by other people. Self-pity is frequently understood as being controlled by powerful others (Stöber, 2003). In this study, the participants tried to avoid being seen as a victim. Self-pity has been described as a response to stressful events such as personal failure, loss, or illness (Stöber, 2003). To avoid feeling sorry for oneself can be a protection against the sense that one’s world is shattered and there is different forms of emotional pain (Holm & Severinsson, 2012). Searching for meaning when life become meaningless can be an effort to find, create, or reconstruct meaning, which is an important aspect of understanding bereavement. This study revealed that the older adults searched for meaning, despite the fact that life became meaningless after the death of their spouse. Research supports this finding, suggesting that people engage in three major activities by which they reconstruct meaning in response to bereavement: sense making, benefit finding, and identity change (Gillies & Neimeyer, 2006). A reconstruction of meaning can be seen as an adaptation to bereavement where people construct a new identity that changes them forever (Holm & Severinsson, 2012; O’Connor, 2002). Constructivist theories suggest that the process by which bereaved persons question and make sense of their bereavement is central to the experience of grief (Neimeyer, 2001). By reconstructing meaning in life in response to a loss, one reconstructs oneself. Changes that occur can be termed “posttraumatic growth,” in which persons respond to the loss in adaptive ways (Tedeschi & Calhoun, 2004). This was also highlighted in our study. People who experience such growth have reported a changed sense of self, stating that they became more resilient, independent, and confident. They took on a new role, developed an awareness of life, and became more sensitive to other peoples’ losses. In this way, their social relationships seem to change in terms of their increased capacity for empathy and becoming emotionally closers to others (Gillies & Neimeyer, 2006; Holm & Severinsson, 2012). As the findings in this study and also in Neimeyer (2001) revealed, continuing bonds as resources for enriched functioning can increase the understanding of bereavement. Thus, bereavement can be seen as a process of reconstructing a world of meaning that has been shattered by the spouse’s death. In contrast, bereavement can represent a decrease in self-management when there is no hope or optimism for the future (Holm & Severinsson, 2012; Valdimarsdóttir et al., 2003). An alternative approach to the idea that successful grieving requires “letting go” is presented by Hall (2014), who suggests that after a death the bonds with the deceased do not necessarily have to be severed and that it can be positive to maintain such bonds. This idea represents recognition of the fact that death ends a life, not a relationship, while the participants in the present study revealed that the deceased can be both present and absent. Such bonds can be understood as conscious, dynamic, and changing (Hall, 2014). One can experience the deceased in dreams, by visiting her or his grave and feeling her or his presence. A sense of the deceased being present may be much higher than revealed by the literature, as people may be unwilling to disclose this phenomenon due to fear of being considered ridiculous or as in the present study, thoughts of going “crazy.”
Despite the fact that being with others was described as the best medicine, one can feel misunderstood in the dialogue with others. The participants described themselves as angry and confused, which can be interpreted as a feeling of stigma that increases the experiences of loneliness and being misunderstood. This can weaken the feeling of support, implying that some older persons are at risk of developing trauma symptoms (Holm & Severinsson, 2012). Social support has been described as one way to alleviate the painful influence of bereavement (Bisconti et al., 2006). Many studies have investigated resilience in widowhood and found that older adults can be resilient to survive bereavement (Holm & Severinsson, 2012). Social support can be a way of describing the size of the social network, while functional support includes various types of emotional support as well as the perceptions of and judgments about support (Powers & Bisconti, 2014). The first 2 years of widowhood have been described as characterized by an increased need for emotional and instrumental support, which decreased after 2.5 years (Bisconti et al., 2006). Longing for inclusion was understood as an experience of loneliness as the participants longed to be included in social dialogue. Research has revealed that social inclusion can be one way to survive bereavement (Holm & Severinsson, 2012). Togetherness is described as the best medicine, as it provides a sense of well-being in times of stress and constitutes a form of support that endows life with meaning, even if it does not solve their problem(s) (Holm et al., 2013). The experience seems to be “beyond words” and metaphors helped them to express the inexpressible (Buchanan-Barker & Barker, 2005). In real life, there is an “absolute inseparability of the living body and life itself” (Gadamer, 2004, p. 71). Mutual respect arises from the reality that one is fundamentally related to the other. Mutual respect is respect for difference (e.g., power, knowledge, beliefs and values, experience, attitudes) and not easy to achieve. Through a resilience process, one may construct a new identity by including a new narrative of oneself (Holm & Severinsson, 2012).
Implications can be related to ageism and how the loss and bereavement are understood by widows and widowers in the community. Some can exhibit resilient reactions after spousal loss, while others are dependent on help from other people. Most people are able to adjust to spousal loss without long-term difficulties (Van Der Houwen et al., 2010). However, a minority can be prone to long-term grief reactions (Bonanno & Mancini, 2008). Early identification of those at risk of suffering health consequences makes it possible to intervene and prevent negative outcomes (Van Der Houwen et al., 2010). Sometimes professional help is needed. Stroebe et al. (2007) found several factors that can reduce risks, while Powers and Bisconti (2014) demonstrated that social support can be the most important factor after the loss of a spouse. However, widows and widowers should receive social support that is not associated with the health care system such as a local bereavement support group.
Conclusion
In this painful struggle, the participants strived to avoid feeling sorry for themselves, searched for meaning when life became meaningless, and sensed that their spouse was present. They often felt misunderstood in the dialogue with others and longed for support to achieve inclusion as well as togetherness. Thus, this study provides a valuable insight into the meaning of bereavement following spousal loss. We recommend that the implications be developed and evaluated.
Footnotes
Acknowledgements
The authors wish to thank Monique Federsel for reviewing the English language.
Author Contributions
A.L.H. contributed to the study design; A.L.H. and A.B. contributed towards data collection; and data analysis, discussion, and preparation were done by A.L.H., E.S., and A.B.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.