
Abstract
Studying the role of social change, I investigated trends in approval for euthanasia between cohorts in the United States and how those trends are influenced by cohort replacement and religious attitudes. Using 16 waves from the General Social Survey (1985 to 2014; n = 6,638), I estimated differences in approval ratings between cohorts using logistic regression models. Models accounted for religious preference, religiosity, age, sex, race/ethnicity, socioeconomic status, marital status, and political ideology. Members of the baby boomer cohort are significantly more likely to approve of euthanasia than either their predecessors or successors, suggesting a cohort effect. Individuals who belong to more conservative religious groups and display higher levels of religiosity are less likely to approve. Cohort has a meaningful effect on approval of euthanasia, successors to the baby boomer cohort might increase their approval as their religiosity decreases and their parents and grandparents increasingly face end-of-life decisions.
Introduction
Attitudes toward end-of-life care are social issues with potential implications for how we handle our aging population as more people reach the later stages of life. Social issues and social changes ebb and flow over time. Specifically, the topic of euthanasia—ending a patient’s life using medical methods (Emanuel, Onwuteaka-Philipsen, Urwin, & Cohen, 2016)—seems to highlight conflicting norms in society: It is not appropriate to end a person’s life; it is also not appropriate to allow people to suffer if it can be avoided. These conflicting norms can be seen in the increased approval of euthanasia and increased used of hospice care in the United States (Livne, 2014), which conflict with the increasingly common opinion that life-saving attempts should be made in all circumstances (Pew Research Center, 2013). Understanding what drives these opinions grows increasingly important with increasing costs of health care at the end of life, with approximately 77% of Medicare costs for decedents occurring during the final year of life and 40% being spent in the final month (Luce & Rubenfeld, 2002). The rising cost of health care at the end of life is becoming increasingly important within our aging population as the oldest baby boomers are now in their early 70s. The baby boomer cohort could potentially pose an increasing cost burden on end-of-life care as they age. This study seeks to understand if the increasing trend in approval for euthanasia in the United States is driven by attitudinal changes in individuals or by cohort replacement.
Research has shown that social change is driven mostly by cohort replacement rather than by changes in individuals’ attitudes over time (Elder & George, 2016; Riley, 1987). This occurs because younger cohorts will not only adopt attitudes and behaviors from their parents but they will also form their own attitudes based on the attitudes prevalent in society and of other members of their cohort. One such example is the gradual decline in religiosity and increase in secularization over time in the United States. These changes in religious attitudes are largely driven by cohort differences rather than individuals changing as they age (Schwadel, 2010, 2011). Religious variation by cohort directly relates to attitudes regarding euthanasia. Such religious variations over time are seen in both declines in religiosity—individual practices such as prayer or church attendance—and in institutional religious identity—such as belonging to a specific denomination (e.g., Ammerman, 2007; Chaves, 2011; Schwadel, 2010, 2011). Opinions regarding euthanasia also tend to vary by religion, sect, and denomination, with some liberal groups favoring euthanasia and others opposing it (Burdette, Hill, & Moulton, 2005).
This article seeks to add to the literature by investigating American approval toward euthanasia by considering whether the current attitudes are a result of cohort effects, including secularization. In this study, American approval of euthanasia is compared across cohorts using nearly 20 years of data from the General Social Survey (GSS). Furthermore, religious variation in attitudes toward euthanasia is investigated by comparing various religious groups and levels of religiosity.
Recent Trends
Advancements in medical technology over the past several decades have enabled medical professionals to diagnose more accurately, prescribe, and treat patients. This progress has also increased life expectancy as well as the ability to sustain life for those who are terminally ill (Burger, Baudisch, & Vaupel, 2012; Caddell & Newton, 1995). Euthanasia gives patients, families, and physicians an option to relieve pain and suffering either by ending life-sustaining care or hastening the end of life through medical methods.
Several studies have considered the changing opinion of the American public regarding euthanasia (e.g., Aghababaei, 2013; Burdette et al., 2005; Caddell & Newton, 1995; DeCesare, 2000; Horsfall, Alcocer, Temple Duncan, & Polk, 2001; Marini, Neuenschwander, & Stieffel, 2006; Montero, 2011). DeCesare (2000) investigated the public’s attitudes regarding euthanasia and suicide when one is terminally ill using data from 1977 through 1996 and found that approval increased from just above 62% in 1977 to just above 70% in 1996. It is important to note that the data used in this study encompassed a period in which there were national news stories in the United States regarding end of life and the right to terminate, and Oregon voters had passed their initial Death With Dignity Act in 1994, suggesting a period effect. DeCesare (2000) suggests that this may reflect two broader social trends: a decline in the public’s confidence in medicine and an increase in the belief of autonomy, especially concerning end-of-life decisions. In a recent and comprehensive study of American attitudes toward euthanasia, Montero (2011) used multiple data sets to view trends dating back to 1947. This study found that since 1947, public approval of euthanasia has steadily increased from about 50% of Americans supporting a patient’s right to end his or her life when suffering from a terminal illness up to 60% in 1977, peaking at approximately 75% in 2005 before leveling off to around 70% in 2007.
Although there is a general positive trend in the approval of euthanasia over time, there have been no studies to date—that this author is aware of—that specifically investigate this trend between cohorts. This upward trend could either be a result of changes in attitudes by individuals as they get older, or it could be due to cohort replacement.
Social Change Between Cohorts
The idea that cohorts can affect social change or attitudes is not a new one. Ryder (1965) suggested that cohorts spark social change because of a cohort’s characteristics and place in history. Ryder further suggested that large cohorts bring about more social change than small cohorts and that movements driven by younger members of a cohort generate more change. This is applicable to a cohort like the baby boomers. Born between 1946 and 1964 and numbering 76 million people, American-born baby boomers were born and grew up as members of a large cohort wrought with changing ideologies and social movements (Hogan, Perez, & Bell, 2008). Social issues such as abortion, same-sex marriage, women’s rights, and end-of-life care have been debated for many years. Changes in the public’s attitudes toward these and other social issues over time are a result of changes in cohorts and not in individuals changing their attitudes (Riley, 1987). For example, baby boomers’ attitudes toward these social issues tend to be more liberal than their parents’ or grandparents’ attitudes before them (Pew Research Center, 2015). The Women’s Movement—one of several different social movements that generated attention and change in the 1960s and 1970s when the baby boomers were in their youth and early adult years—is a prime example of social change due to cohort replacement. Age, period, and cohort analyses have demonstrated that the overall increase in gender egalitarian attitudes since the 1970s is a result of older cohorts being replaced by younger cohorts (Cotter, Hermsen, & Vanneman, 2011; Pampel, 2011a, 2011b). This understanding of change via cohort is important in understanding how social issues, policies, and laws evolve over time. It could be argued that people’s attitudes change over time, which would suggest that there are some social factors that influence people as they age. However, much research suggests that these changes are a result of cohort replacement.
Cohort replacement is also associated with declining levels of religious participation and an increase in secularization (Elder & George, 2016; Schwadel, 2011). Secularization consists of declines in religious attendance as well as declines in confidence in religious authority or institutionalized religion (Schwadel, 2010, 2011; Sommerville, 1998). This is an important consideration as religion has long been of interest to researchers when studying the trends of American attitudes of euthanasia (e.g., Aghababaei, 2013; Burdette et al., 2005; Caddell & Newton, 1995). These studies, and other studies (e.g., Hamil-Luker & Smith, 1998), have shown that there is a correlation between religious belief, religiosity, and attitudes regarding euthanasia and physician-assisted suicide; individuals with a higher level of belief or religious practice and more conservative religious views are more opposed to euthanasia, due to the social and religious norm of “Thou shalt not kill,” while those who are less religious or have less religious authority or control of their lives are more approving. It is important to note the context of religion in the United States. Compared with other nations, and especially Westernized nations, the United States is very religious (Chaves, 2011). Americans are considered highly religious in both their individual expressions of religiosity (e.g., frequency of prayer, belief in God, attending religious meetings, etc.) and in their identification with institutionalized religious groups (e.g., Catholic, Protestant, etc.) (Ammerman, 2007; Chaves, 2011). This study will investigate the correlation between measures of religiosity and religious identification and approval of euthanasia.
Another correlation between religion and attitudes about euthanasia could be the increase in the number of people who claim no religious affiliation, or religious nones. There has been an increase in the religious nones over the past several decades with a steep rise beginning in 1990 (Lim, MacGregor, & Putnam, 2010). During this era, favorable attitudes toward euthanasia have also increased (DeCesare, 2000; Montero, 2011). However, favorable attitudes of euthanasia have leveled off at around 70% since 1990, while the religious nones have continued to increase. If social change and secularization are linked to cohort replacement, then it is plausible that increased approval for euthanasia is a result of younger cohorts being more liberal and less religious than older cohorts. Baby boomers are less likely to be religious than generations before them and would therefore be less likely to have their attitudes on euthanasia influenced by religious beliefs or authority.
Hypotheses
A summary of the literature suggests that approval for euthanasia saw a steady rise from the 1940s to the 1990s when it leveled off around 70%. This leveling off suggests that even though we have an aging population, these attitudes might be driven by cohorts or cohort replacement. Consistent with social change via cohort, secularization is increasing over time and this is not due to people becoming less religious as they age, but by younger cohorts being less likely to identify as religious. The literature leads to two research questions:
Data and Method
For this study, I use the GSS to assess changes in attitudes toward euthanasia over time. The GSS is a nationally representative survey that began in 1972. From 1972 to 1994, data were collected annually before switching to a biennial collection process beginning in 1994. For this analysis, I will be using 16 waves of data from 1985 to 2014, as not all the measures used in this present analysis are available in each collection year.
Approval for euthanasia is measured by respondents’ answer to a question in the GSS: “When a person has a disease that cannot be cured, do you think doctors should be allowed by law to end the patient’s life by some painless means if the patient and his family request it?” I then create a dummy variable for their responses with “no” (0) and “yes” (1) and I remove those who either did not answer or answered “don’t know” from my analysis.
The main independent variable is cohorts, and I create this variable in two ways: First, I create three different generational cohorts based on the respondents’ reported birth year. My emphasis in this study is the baby boomers, who were born between 1946 and 1965. For consistency in my cohorts, I code pre–baby boomers as those who were born between 1936 and 1945, and post–baby boomers as those who were born between 1966 and 1985. Second, I restrict the data by age to reduce collinearity and to ensure that changes seen in cohorts were a result of cohort membership and not age. Only respondents aged 27 to 49 years are included in this analysis. This age range was selected because there are no respondents in the data who were born before the baby boom that were younger than 27 years and no respondents born after the baby boom that were older than 49 years. Other coding mechanisms for cohorts were attempted and analyzed, ranging from three birth cohorts to five birth cohorts. However, cohort sizes were so small that statistical power was lost. Other analyses using more cohorts demonstrated the same general patterns but with less power.
The GSS offers a wide array of religious groups that respondents can identify with. For simplicity, these groups have been clustered down to seven broader groups based on a modified version of Steensland and colleagues’ (2000) religious coding. In this analysis, the groups are nones, Catholics, Jewish, Conservative Protestants, Mainline Protestants, Black Protestants, and others. Other includes more eastern traditions such as Islam, Buddhism, and Hinduism.
To assess religiosity, I include three different variables available in the GSS. First is attendance at religious services, a commonly used measure of religiosity in the literature (Burdette et al., 2005; Montero, 2011; Schwadel, 2010); consistent with other studies I truncate this to a dummy variable with attending religious services less than twice a month (0) and attending religious services twice a month or more (1). In addition to attendance at religious services, I include two other measures of religiosity that aim to capture more intrinsic levels of religiosity, which is often underexamined (Aghababaei, 2013). The GSS asks respondents how often they pray, which I also truncate to a dummy variable with less than once a week (0) and once a week or more (1). My third measure of religiosity is Biblical literalism. Participants are asked their feelings about the Bible with the following response options; the literal word of God (1), an inspired word of God but not everything is literal (2), an ancient book of fables (3), and other (4). As with my other measures of religiosity, I create a dummy variable with those who do not feel the Bible is the literal word of God (0) and those who do feel that the Bible is the literal word of God (1).
Controls include age, ranging from 27 to 49 years; sex, coded 0 for male and 1 for female; race, the GSS only distinguishes White (0), Black (1), and other (2). Other controls include years of education, family income, marital status dichotomized as not married (0) and married (1), and political ideology coded as liberal (0), moderate (1), or conservative (2). My total n for this study is 6,638.
Analytic Approach
To estimate differences in approval for euthanasia between these three cohorts, I employ logistic regression. I estimate several models using logistic regression, progressively adding more variables. In all my models, the baby boomer cohort is the reference group. Model 1 estimates the bivariate relationship between cohort and approval for euthanasia. Model 2 builds upon Model 1 by controlling for age. Model 3 includes the rest of my control variables: sex, race—with White as the reference group—marital status, years of education, and political ideology—with conservative as the reference category. In Model 4, I introduce the seven religious groups with the nones as my reference category. Model 5 adds my three measures of religiosity to this analysis. Models 6 and 7 include interactions in addition to the full list of variables: Model 6 includes an interaction of praying at least once a week with cohort, and Model 7 interacts cohort with religious group. Additional interactions were estimated and were not significant and are therefore not included in this article, but they are available upon request. The Bayesian information criterion found that the best model that fit these data are Model 5.
Results
Descriptive statistics of my sample are presented in Table 1. I will briefly highlight some of the key descriptive statistics from this table and then discuss the results. First, roughly 55% of my sample belong to the baby boomer cohort with approximately 39% belonging to the post–baby boomer cohort and only about 6% being in the pre–baby boomer cohort. Second, nearly 78% of the sample report as being White, with approximately 14% of the sample reporting as Black and only 8% reporting as other. The pre–baby boomers have the highest percentage of White participants with the post–baby boomers having the lowest percentage of White respondents. Third, approximately 55% of the sample is female and this is relatively consistent among the three cohorts, with pre–baby boomers being the only group that is nearly 50% female and 50% male. Fourth, political ideology is relatively evenly distributed among the sample and among the cohorts. Those who identify as moderate make up about 37% of the sample, and within cohorts no group has a strong majority. The strongest majority observed is among moderate post–baby boomers who only claim approximately 39% of their cohort’s political ideology.
Descriptive Statistics (GSS 1985 to 2014).
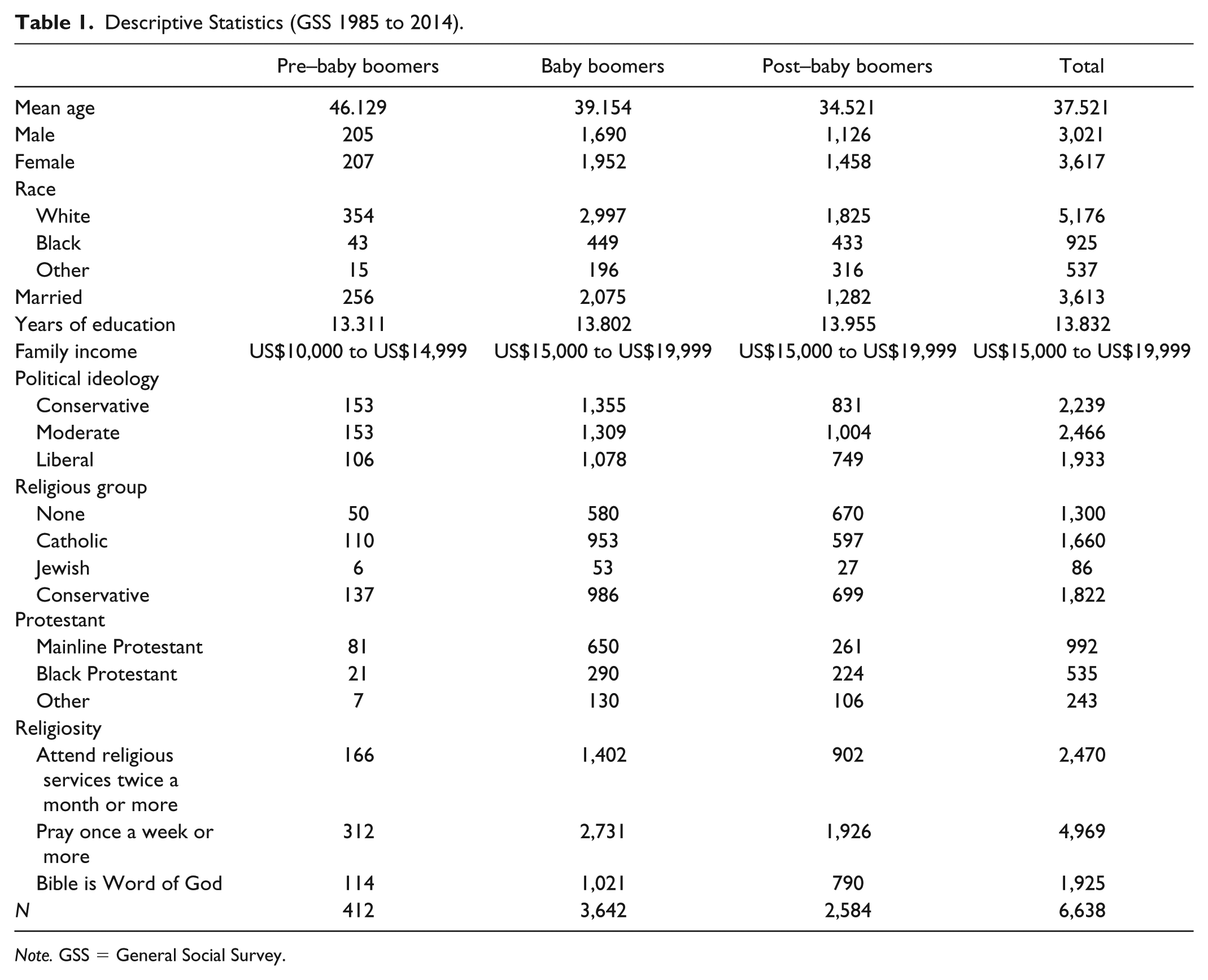
Note. GSS = General Social Survey.
Fifth are the different religious groups. The faith groups with the largest representation in the overall sample are Conservative Protestants (~27%), Catholics (~25%), and nones (~20%). Although 80% of the sample identify with some religious group, when broken down, the nones are the third largest group in the sample. Some of the more notable differences between cohorts are seen with the nones only being about 12% of pre–baby boomers, just below 16% of baby boomers, and then reaching nearly 26% of post–baby boomers. This is consistent with the idea that secularization is growing and is more common among younger cohorts. Another notable change among the religious groups is the decline in Mainline Protestants, who represent nearly 20% of pre–baby boomers, almost 18% of baby boomers, and just 10% of post–baby boomers. Finally, the measures of religiosity. Roughly, 37% of respondents in the sample attend religious services at least twice a month. Those most likely to do so are pre–baby boomers at about 40%, and the least likely are post–baby boomers at about 35%. One of the more notable descriptive statistics is for those who report praying at least once a week or more. In the overall sample, 75% of people report weekly prayer, and this figure remains constant between all three cohorts. Even though more people report being nones in younger cohorts, the amount of prayer has not decreased between cohorts. Crosstabs indicate that among the religious nones, nearly 43% of the overall sample report praying at least once a week and this figure was 42% among pre–baby boomer nones and up to just over 43% of post–baby boomer nones. This finding supports the idea that religious nones still might practice some level of spirituality or intrinsic religiosity.
Table 2 shows the results for all seven of the estimated logistic regression models. Model 1 shows the bivariate relationship between cohorts and approval for euthanasia. Results show that both pre–baby boomers and post–baby boomers are significantly less likely to approve of euthanasia in comparison to baby boomers. Pre–baby boomers have an odds ratio of 0.764 while post–baby boomers have an odds ratio of 0.872. This suggests that baby boomers are significantly more likely to approve of euthanasia than either their predecessors or successors. This relationship is consistent in all the models estimated. This provides only partial support for Hypothesis 1, while baby boomers were more likely than their predecessors to approve of euthanasia, levels of support do not increase from baby boomers to post–baby boomers. For simplicity in interpretation, I convert odds ratios into predicted probabilities. Figure 1 shows the predicted probability for each of the three cohorts approval of euthanasia based on estimates from Model 5. Displaying predicted probabilities for each model was considered, but as the pattern is consistent and similar in magnitude, only those from Model 5 are presented in the figures. Note that in Figure 1, the predicted probability of approval for euthanasia is highest among the baby boomers at 0.739, lowest among the pre–baby boomers at 0.704, and only at 0.709 for post–baby boomers.
Logistic Estimates for “Approval of Euthanasia” (N = 6,638).

p < .05. **p < .01. ***p < .001.

Predictive probability for approval of euthanasia.
When age is added in Model 2, the significance for pre–baby boomers is explained away; but there is still a negative effect for pre–baby boomers compared with baby boomers. In Model 2, the odds ratio for age is 0.985, which demonstrates that odds of approval for euthanasia declines with age. This relationship shows (see Figure 2) that each cohort is less likely to approve of euthanasia as they age. It is important to know that I did estimate an interaction between cohort and age and found no significant effect. Because of this finding, it could be suggested that the oldest cohort would be the least likely to approve of euthanasia and the youngest cohort would be the most likely to approve. However, at every age, baby boomers are still more likely to approve of euthanasia, which supports the idea that cohort does matter for attitudes and that baby boomers are unique as a cohort.

Predicted probability for approval of euthanasia across cohorts by age.
The results from Model 3, shown in Table 1, are worth noting even if there were no unexpected findings. Again, the pattern for pre– and post–baby boomers being less likely to approve of euthanasia than baby boomers holds when controlling for all the demographic and control variables. The effect is slightly smaller for postboomers in this model but is still significant. Females are significantly less likely than men to approve of euthanasia with an odds ratio of 0.698, and this finding is consistent with previous research (Burdette et al., 2005; Montero, 2011). Non-Whites, or Blacks and others in this sample, are both significantly less likely than Whites to approve of euthanasia, which is also consistent with previous literature (Burdette et al., 2005; Montero, 2011) that suggest that some of the results could be explained by mistrust in the medical profession, especially among Blacks. Also, consistent with previous research (Burdette et al., 2005; Montero, 2011), higher education is significantly associated with higher odds for approval of euthanasia, as is higher income, although this is not significant. As expected, both moderates and liberals have significantly higher odds for approval of euthanasia than conservatives.
Model 4 in Table 2 shows the results when including religious groups in the regression. Unsurprisingly, belonging to a religious group is associated with lower odds for approval of euthanasia than being a part of the nones and all these groups, except for those who identify as Jewish, are statistically significant. The religious groups’ odds ratios of approval are consistent with traditional levels of conservatism within each group. Those with the lowest odds ratio (0.296) are the Conservative Protestants, who are generally the most conservative religious group in the United States. Catholics (0.382) and Black Protestants (0.399) have similar odds ratio and are both seen as religiously conservative groups. Among the religious groups that are statistically significantly different than the nones, the largest odds ratio is for Mainline Protestants (0.691). Again, this is expected since belonging to a religious group is usually correlated with higher levels of conservatism on social issues compared with those who do not belong to a religious group. Furthermore, among major religious groups in the United States, Mainline Protestants are typically more progressive than their Christian peers.
To assess the extent to which attitudes are driven by belonging to one of these religions within a cohort, I also estimate an interaction between cohorts and religious groups (see Figure 3 and Model 7 in Table 2). Although not every one of these interactions is significant, there are some patterns and results worth noting. In general, these interactions show that being a pre–baby boomer and belonging to these religious groups leads to lower odds of approval for euthanasia. The pattern is the opposite for post–baby boomers who belong to these religious groups. Although only three of these interactions are significant at the p < .05 level, the trends do suggest that post–baby boomers who identify with these religious groups have higher odds for approving of euthanasia. This could suggest that secularization is having some effect among the religious post–baby boomers, meaning that even though these post–baby boomers do identify as religious, they might be less likely to adhere to religious leaders or religious authority.
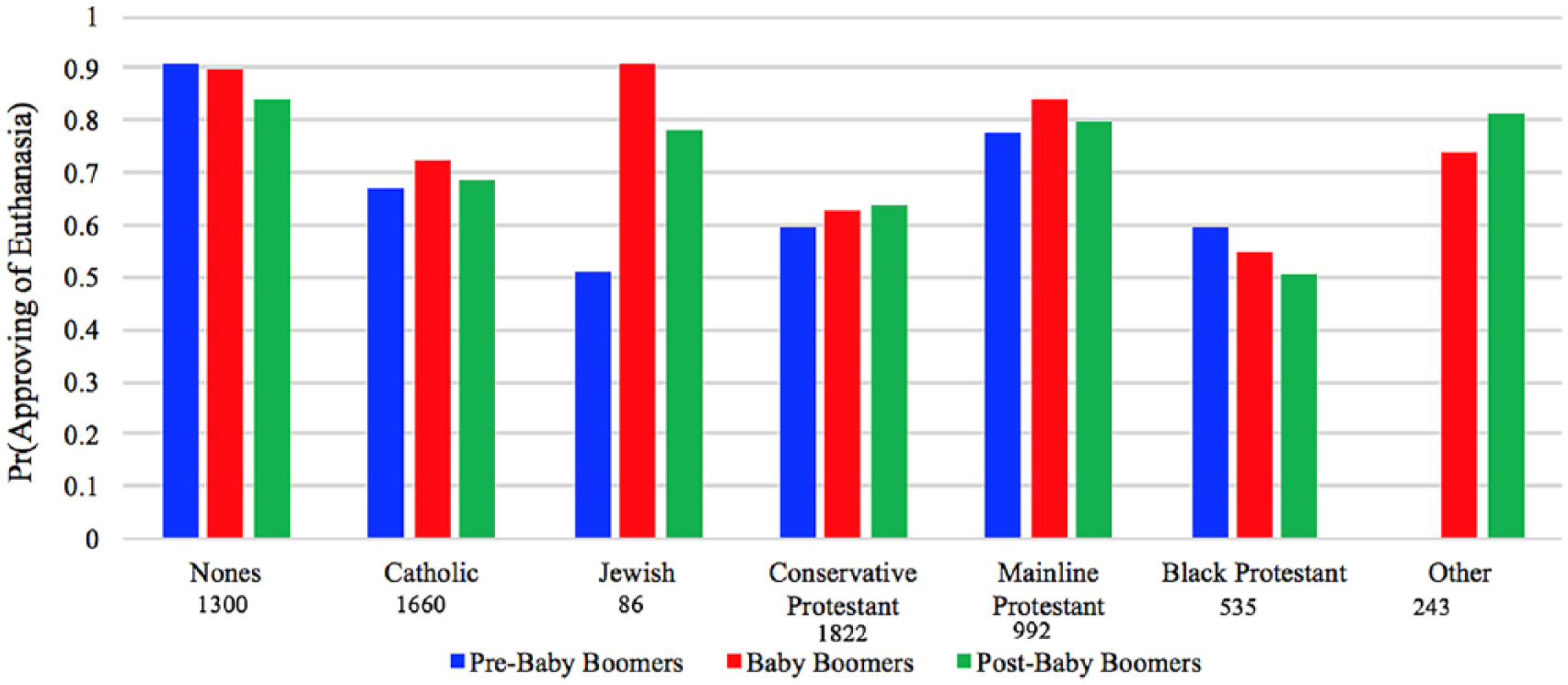
Cohort interactions with religious groups.
In Figure 3, I report predicted probabilities from postestimation techniques to highlight differences between groups and cohorts. Jewish baby boomers have a much higher probability of approval (0.913) than Jewish pre–baby boomers (0.513) and a noticeably higher probability than Jewish post–baby boomers (0.784). However, it should be noted that this could also be due to the small number of survey participants who identify as Jewish, with only 86 in the sample. This pattern is similar for Mainline Protestants, with baby boomers having the highest probability of approval (0.838), pre–baby boomer Mainline Protestants having the lowest probability (0.777), and post–baby boomers also having a lower probability (0.797) than baby boomers. Although these two groups do standout, this is not entirely surprising as these groups are generally considered to be more progressive than their religious counterparts. However, another religious group worth noting in this interaction is the Catholic group. Although this interaction is not significant, it is noteworthy because it follows the same pattern as Jewish and Mainline Protestant respondents even though Catholics are typically one of the more conservative religious groups, with Catholic leadership being publicly opposed to euthanasia. These could be respondents who identify as Catholic but might not have high levels of religiosity, suggesting support for secularization. They could also be practicing Catholics that do not adhere completely to Catholic leadership on this issue, again, supporting secularization.
The final results are those from Models 5 and 6 found in Table 2. All three measures of religiosity have odds ratios below one, indicating a negative effect or that the odds for approval of euthanasia are less, and all three are significant at the p < .001 level. Those who attend religious services at least twice a month have the lowest odds ratio (0.484) while those who pray at least once a week have the highest odds ratio (0.567), which still suggests that regular prayer diminishes approval for euthanasia. Finally, those who believe the Bible to be the literal word of God have an odds ratio of 0.539. When adding my three measures of religiosity in Model 5, the pattern and odds ratios for cohorts’ approval of euthanasia do not appear to have any meaningful change. Furthermore, except for marital status, which loses statistical significance, none of the standard controls and demographic measures see any noteworthy changes with the addition of religiosity. However, there are some important changes that occur within religious groups when accounting for religiosity.
While five out of six religious groups for which coefficients are reported in Model 4 were statistically significant, when adding religiosity there are only two out of six that remain significant, Catholics and Conservative Protestants. Every single religious group sees an increased odds ratio when measures of religiosity are included in the model, with the statistical significance explained away by accounting for religiosity among Mainline Protestants, Black Protestants, and others. Perhaps the most interesting change from Model 4 to Model 5 is among Mainline Protestants. Not only do Mainline Protestants lose statistical significance by accounting for religiosity but they also go from an odds ratio below 1.000, a negative effect, to an odds ratio above 1.000, which suggests a positive effect. Even though this odds ratio is not significant in Model 5, it suggests that those who identify as Mainline Protestants and exhibit higher levels of religiosity are more likely to approve of euthanasia than those who do not. A possible explanation for this is that Mainline Protestants, who are generally considered more progressive, might be more likely to hear more progressive social views from religious leaders and from fellow worshipers in their communities when they are participating.
Finally, interactions with cohort and all three measures of religiosity were estimated, and only praying at least once a week has a significant effect only among post–baby boomers (see Model 6 in Table 2). For those post–baby boomers who do report praying at least once a week their odds ratio for approval of euthanasia is 1.442, which is a positive effect. Prayer is a more intrinsic measure of religiosity and therefore captures those who might be less inclined to attend services, take the Bible as the literal word of God, or even identify with an organized religion, but still seek some level of spirituality or prayer within themselves. In general, these findings support Hypothesis 2, that secularization partially explains cohort differences. If secularization did not play a role between the cohorts, differences would be explained by other factors such as political ideology or educational differences between cohorts, but there is no evidence of this in these results.
Discussion
Attitudes regarding euthanasia have been of interest among researchers for decades. Most studies in this line of research have focused on the social characteristics of those who do or do not approve of euthanasia or on general trends of approval over time. This study focused on differences between cohorts in an effort to further understand social change and how these attitudes might change going forward. Findings from this study provide evidence that there are cohort differences for approval of euthanasia and that younger cohorts are not necessarily more likely to approve.
Although past research has shown a steady increase for approval of euthanasia from the 1940s until the 1990s when approving attitudes seemingly leveled off at around 70% (DeCesare, 2000; Montero, 2011), it is unclear whether or not this number will remain constant in the coming years. Findings from this study show two possible reasons why approval for euthanasia might dip down in the future. First, approval of euthanasia does decline as people get older. As pre–baby boomers die and become replaced by aging baby boomers, the baby boomers also might be less favorable in their approval of euthanasia. Second, this study found that the post–baby boomers, those born between 1966 and 1985 are less likely to approve of euthanasia than their predecessors. Even though post–baby boomers currently approve of euthanasia at a level similar to the overall trends we observe in the population, their support might diminish with age. Furthermore, if even younger cohorts—those born after 1985—follow this trend, overall approval could decline in the future. However, this is highly dependent on several factors.
First, depending on how baby boomers deal with end-of-life care for their aging parents, the pre–baby boomers, their attitudes about euthanasia might shift. Second, and in conjunction with making decisions for their parents, baby boomers are currently between the ages of 52 and 71 years, meaning that they are not only in the process of making end-of-life care decisions for their parents but are also in the position or very soon will be required to make decisions on their own behalf or on behalf of their significant others. A third factor that could influence future attitudes on euthanasia is how post–baby boomers and other younger generations react to helping the baby boomers make end-of-life care decisions. Post–baby boomers might see either an increase in the need for euthanasia to alleviate suffering, or they might want to prolong life to spend more time with loved ones.
This study found that nearly three quarters of baby boomers approve of euthanasia, which is significantly more than pre– or post–baby boomers’ approval of euthanasia. Baby boomers represent roughly 25% of the entire United States population, meaning that at their current age and size they likely have the most influence on current opinions and policies. Overall approval for euthanasia reached 70% in 1991, when baby boomers were between ages 25 and 44 years (DeCesare, 2000; Montero, 2011). As has been argued in the literature and in this article, much social change is driven by cohorts and not by aging individuals. If baby boomers developed these attitudes in early adulthood and early middle age, findings from this study would suggest that their large size in the United States population could explain why approval reached 70% in the early 1990s and has leveled off since then.
In addition to identifying differences between cohorts, this study found that, consistent with prior research (Burdette et al., 2005; Caddell & Newton, 1995; Hamil-Luker & Smith, 1998; Montero, 2011), approval for euthanasia is associated with religious belief and secularization. This study adds to previous research by investigating multiple measures of religiosity. Most previous studies have not considered intrinsic measures of religiosity and have focused more on external measures, such as frequency of attendance at religious services (e.g., Aghababaei, 2013; Burdette et al., 2005). By including these additional measures of religiosity, I am able to account for more of the possible effects of secularization between cohorts. As noted in the literature, evidence of secularization is not only found through an increase in the religious nones, but there is also evidence that there is a decline in religious authority and privatization of religion and spiritualism (Schwadel, 2010, 2011, 2013; Sommerville, 1998). This current study finds that many people who do not identify as religious, or as belonging to an organized religion, still seek some level of spirituality and practice some form of prayer as a part of their lives. Post–baby boomers who pray at least once a week are more likely to approve of euthanasia than baby boomers who pray regularly, even though post–baby boomers are significantly less likely to approve of euthanasia. This suggest that for post–baby boomers, who are less likely to be religious, those who pray regularly could still be seeking some form of intrinsic spirituality while not seeing a need for extrinsic religiosity that is displayed by frequent attendance at religious services.
There are qualitative differences between people who simply identify as a part of a religious group and those who display higher levels of religiosity. The most conservative religious groups, Catholics and Conservative Protestants, seem to be the most resilient to these changes and maintain higher levels of religiosity (e.g., Aghababaei, 2013; Burdette et al., 2005; Caddell & Newton, 1995; Hamil-Luker & Smith, 1998). It is possible that these more conservative groups might be less affected by secularization and still might be more likely than their counterparts to adhere to religious authority, or that their religious leaders are less likely to approve of euthanasia. It is possible that for the more progressive groups who lose their significance when accounting for religiosity, that when participating in their religious communities, they are more likely to encounter more progressive leaders and fellow members. Thus, it is possible that by participating in their religious communities and through intrinsic expressions of their faith, they become more likely to approve of euthanasia.
Conclusion
This study and these findings are not without limitations. First, while the religious groups were created based on Steensland et al. (2000), there are still some important qualitative differences between certain religious groups that are grouped together. For example, the other group is comprised of mostly eastern traditions that are less common in the United States. Another limitation with the religious measures is that the measures for religiosity, while well established in the literature, cannot fully capture the level of conviction or belief among those who identify as religious. Finally, the outcome measure is commonly used in this literature and does capture attitudes on euthanasia. However, this particular measure does not distinguish between voluntary active euthanasia—physician-assisted suicide—and voluntary passive euthanasia—ending or withholding treatment. These two types of euthanasia are qualitatively different and when asked directly about the two, people are less likely to approve of voluntary active euthanasia (Burdette et al., 2005; Emanuel et al., 2016).
Despite these limitations, this study has important implications for understanding attitudes toward euthanasia as well as potential policy. Although there are cohort differences for attitudes of euthanasia, it is not clear whether these attitudes will continue to change as a result of cohort replacement. There is some evidence for this because baby boomers were more likely to approve than their predecessors; however, post–baby boomers were less likely to approve than baby boomers. Therefore, cohort replacement might not be able to completely explain the trending approval for euthanasia since the 1940s.
Policy makers should consider the differences in approving attitudes for euthanasia between cohorts as they continue to address health care reform and end-of-life treatment options. At the time of this study, six states and Washington, D.C., allow some form of voluntary active euthanasia; Oregon was alone in this practice from 1994 until 2008. Although the increase in legalization of this practice as an end-of-life care option has been on the rise during the past decade, if post–baby boomers remain less likely to approve of these practices, legislators may have a more difficult time passing these types of laws in the future. However, there is still a sizable number of baby boomers who are in favor of these laws.
Future research should consider qualitative research methods to better understand differences between religious groups and types of religiosity. If researchers can determine if and why some types of religiosity have a greater effect on attitudes of euthanasia, we might be able to better understand the impact of secularization on these attitudes and how this might affect social change. Future research should also investigate the impact of period effects on these attitudes. For example, even though approving attitudes have remained relatively level at 70% since 1990, there was a slight spike to approximately 75% in 2005, which was when Terri Schiavo died after a widely publicized 15-year legal battle between her husband and her parents to end and withhold her treatment after she was left in a vegetative state. This particular study was not concerned with period effects as the study window was from 1985 to 2014, during which overall approval remained fairly constant except for the aforementioned spike in 2005. However, this does not mean that other increases in the past are not partially a result of periods when medical technology and health care advanced.
In conclusion, the overall high approval for euthanasia in the United States seems to be a product of the large baby boomer cohort. Due to its large size and unique era in which baby boomers grew up, their attitudes are more favorable than their predecessors. Baby boomers are also more likely to approve of euthanasia than post–baby boomers, suggesting that there is something unique about the baby boomers which drives their social attitudes. While it is possible that attitudes could decline in the future, this seems unlikely. Even though post–baby boomers are less likely to approve of euthanasia than baby boomers, most of them still approve. As health care costs, especially in the final 12 months of life, continue to remain high, and as baby boomers age, it is possible that younger cohorts will seek for less expensive end-of-life care to deal with the coming needs. Finally, secularization does appear to be a contributing factor to attitudes about euthanasia. However, the effects of secularization appear to vary between cohorts and do not affect all religious groups to the same degree. Furthermore, it appears that among some religious groups, higher religiosity might increase odds for approval of euthanasia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.