
Abstract
There is a need to better understand contemporary issues of nomenclature and group construction around people with intersex variations shaping health research and practices—including their framing within concepts like disorders of sex development (DSD), intersex, or the lesbian, gay, bisexual, transgender, and intersex (LGBTI) umbrella. This article reviews health literature in the broad field of Intersex Studies since 2015. It outlines the contexts, theoretical lenses, methods and participant numbers, framing of participants, and health findings around interventions evident in 61 sources. Sources came from the African region, American Canadian region, Asia-Pacific region, European region, and the Middle East. While health-related work was largely found in medical journals, it was also located in publications focused on a range of other fields including, for example, bioethics, education, and legal studies. The piece discusses the tensions between institutional expert-centered work with a traditional clinical/medical lens and the arguments found in a range of other patient-centered, community group–centered, and theory-centered sources applying innovative perspectives onto key issues. Liberal Constructivist, Bioethical Narrative Inquiry, Critical Intersex Studies, and Critical LGBTI Liberationist lenses have introduced a range of methods (from autobiographical analyses through to large-scale online surveys) to questions of the need for and processes of certain health care interventions and norms in the treatment of patients with intersex variations. Problematic practices in clinical health care and research are identified and discussed: particularly the lack of adequate information dissemination and consent-gleaning in areas ranging from anatomical photography through to application of “corrective” genital surgeries.
Introduction
The potential to have somatic intersex variations exists (however, briefly) in all humans’ prenatal development in the first few weeks—for a portion of humans, a level of ambiguity in their sex traits continues on after this point (Ainsworth, 2015). Intersex variations are atypical sex characteristics (Organisation Intersex International [OII] Australia, 2012b); these sex characteristics potentially include our chromosomes, genes, external genitalia, internal reproductive organs, hormones, or secondary characteristics (like body hair). In the last decade, people with intersex variations have been increasingly studied or referred to as part of an umbrella group, rather than seen only as those with a specific variation such as congenital adrenal hyperplasia (CAH) or androgen insensitivity syndromes (AIS). This group has been termed (however, incorrectly or inappropriately) hermaphroditic, intersex, as having disorders or differentiation of sex development, or otherwise.
Problems in research beyond variable terminology include variable population estimates. Research has generally estimated that 1.7% to 4% of people go on to actually have intersex variations (Carroll, 2005; Fausto-Sterling, 1993; OII Australia, 2012b). Given that many elements of sex (chromosomes, genes, hormones) are not apparent without testing, current estimates of the incidence and types of intersex variations seen in humans may be conservative. Some common intersex variations are diagnosed prenatally, some at birth; others may only become apparent at puberty, when trying to conceive, or through random chance; and it is important to emphasize that many people will never know they have intersex variations. Many individuals with intersex variations have two or more variations (Jones et al., 2016). Numbers can also be impacted by the inclusion of congenital variations stemming from hormone-related conditions; some researchers have included extreme polycystic ovary syndrome (PCOS)–related hyperandrogenism within the umbrella of intersex variations (Huang, Brennan, & Azziz, 2010; Jones et al., 2016). Furthermore, researchers may intentionally or unintentionally include individuals who identify as intersex as a gender or political identity choice—without having somatic intersex variations. There is, however, a need in health research to limit the group to only those with somatic intersex variations (regardless of gender/political identity), due to their distinct medical experiences (Jones et al., 2016).
Another complicating issue is that the health of people with intersex variations is sometimes studied in relation to their sex traits, disabilities, rights, or a range of issues that seem to lend themselves to divergent theoretical lenses understanding this group and their needs in very different ways. There is a need to understand how issues of group construction and nomenclature shape health research around people with intersex variations. This article reviews the range of ways in which the health and well-being of people with somatic intersex variations have been recently studied in international research literature. It uses a critical sociology of health frame, responding to and foregrounding recent intersex activist movements casting intersex variations as a biological variation rather than a medical pathology (Holmes, 2009; OII Australia, 2012b; Pagonis, 2016), and accepting intersex individuals’ own research on their own health and well-being experience as part of the key literature to be explored (rather than limiting the parameters of health literature purely to that produced by traditionally conceived medical experts). The method for the review is explained, followed by key trends in the literature sources—their contexts, theoretical lenses, methods and participant numbers, and framing of participants and interventions. This article then discusses issues that arise from these trends and draws conclusions on key tensions in the field.
Method
The review aimed to explore how people with somatic intersex variations have been studied “as a holistic group” to better understand how the health of “the group as a whole” has been constructed in recent research. A formal systematic review was completed through the ProQuest Central database (selected for its broad coverage of health-related literature from a multi-disciplinary range of approaches and lenses). An Advanced Search was completed for the key terms “intersex” or “disorder of sex development (DSD).” This was applied across the Source Type categories “Scholarly Journals.” The search was initially limited to peer-reviewed full text pieces published from 2006 to 2016, in English for (the researcher’s) ease of review. As a search from the last decade yielded 2,101 results, only the texts from 2015-2016 were selected to provide a more recent focal point and ensure the review was contained. Each title and abstract were read to ensure relevance, and then the full article was read for further clarity. Only 61 of these texts were deemed relevant, based on their focus on humans with somatic intersex variations/disorders of sex development/differences in sex development (DSDs) and health care (in its broadest sense ranging from clinical conceptualizations to holistic well-being). Those focused on intersex expression in animals, human sex development more broadly without any consideration of variations, unrelated disorders or themes (such as works solely on autism), or nonhealth related topics were manually eliminated from the search results.
The texts were then read again in full and analyzed with reference to a previous discourse analysis of key theoretical indicators in the field (detailed in Jones et al., 2016). Specific information was gleaned on their context from the publication and author location information recorded in the database and on the documents themselves. The sources’ theoretical lenses were deduced from a combination of both their stated theory applications (if available) and/or other indicators including language and concept usage, data type, and methodological and analytical stances (whether positivist, constructivist, relativist, deconstructive, subversive, or otherwise, for example) in relation to their data collected. The sources were allocated a roman numeral for ease of reference. The sources’ specific methods, participant numbers, and ages were directly gleaned from the sources’ own descriptive text in the abstract and the full text source, or noted as absent. The sources’ construction of people with intersex variations (including nomenclature and variations recognized) were directly gleaned from the sources’ abstract and full text. Finally, the health-related findings were gleaned from direct statements (or their absence) on health-related issues (especially interventions, including diagnosis, analysis, treatment, and evaluation of any kind) experienced by any people with intersex variations featured in the sources (variably including the authors themselves, study participants of any kind, or any generally conceptualized version of the group as constructed in a given source). These data were systematically tabulated and are reported in this article in a combination of qualitative and quantitative summaries, with some basic figures to enhance accessibility.
Results
Source Contexts
Overall, the 61 textual sources in this literature review came from studies based in several global regions—see the appendix (Achermann, Domenice, Bachega, Nishi, & Mendonca, 2015; Ahmed & Fadl-Elmula, 2016; Amanda, 2015; Amarillo et al., 2016; Anderson, 2015; Anonymous, 2016; Baratz & Karkazis, 2015; Bonanni, Pasetti, Ghiggeri, & Gandolfo, 2015; Brasileiro et al., 2016; Camats et al., 2015; Ceci, Calleja, Said, & Gatt, 2015; Cynthia, 2015; Davis, 2015b; Dong et al., 2016; Dreger, 2015; Dwyer, Ball, & Barker, 2015; Ediati et al., 2015; Ekenze et al., 2015; Frader, 2015; Garcia, 2015; Grimbly, Caluseriu, Metcalfe, Jetha, & Rosolowsky, 2016; Grimes, 2016; Grover, French, & Yazdani, 2015; Gül, Sayar, Özten, & Eryilmaz, 2015; Howard, 2015; Inter, 2015; Jones, 2016; Kalra, Baruah, & Kalra, 2016; Kelsey et al., 2016; Khadilkar et al., 2015; Kim et al., 2015; Kraus, 2015; Lalor, 2015; Latrech, Skikar, Mohammed El Hassan, Chraïbi, & Gaouzi, 2015; Lin-Su, Lekarev, Poppas, & Vogiatzi, 2015; Long, 2015; Lucas-Herald et al., 2015; Mannaerts, Muys, Blaumeiser, & Jacquemyn, 2015; Miller, 2015; Mohamed & Noor, 2015; Mutlu et al., 2015; Oliveira, de Paiva-e-Silva, Guerra-Junior, & Maciel-Guerra, 2015; Pagonis, 2015; Palanisamy et al., 2015; Paula et al., 2015; Petersen, 2015; Quinn, 2015; Rios et al., 2015; Rubin, 2015; Saraswat, Weinand, & Safer, 2015; Simon, 2015; Tinney et al., 2015; Topcu et al., 2015; Truffer, 2015; Vasundhera, Jyotsna, Kandasamy, & Gupta, 2016; Viloria, 2015; von Klan, 2015; Wall, 2015; Walsh, 2015; Wang & Tian, 2015; Zieselman, 2015). These included 38 sources from the American Canadian region (Amarillo et al., 2016; Amanda, 2015; Anderson, 2015; Baratz & Karkazis, 2015; Brasileiro et al., 2016; Camats et al., 2015; Ceci et al., 2015; Cynthia, 2015; Davis, 2015b; Dreger, 2015; Frader, 2015; Garcia, 2015; Grimbly et al., 2016; Grimes, 2016; Grover et al., 2015; Howard, 2015; Inter, 2015; Kelsey et al., 2016; Kraus, 2015; Lin-Su et al., 2015; Long, 2015; Miller, 2015; Oliveira et al., 2015; Pagonis, 2015; Paula et al., 2015; Petersen, 2015; Quinn, 2015; Rios et al., 2015; Rubin, 2015; Saraswat et al., 2015; Simon, 2015; Topcu et al., 2015; Truffer, 2015; Viloria, 2015; von Klan, 2015; Wall, 2015; Walsh, 2015; Zieselman, 2015). There were 12 from the Asia-Pacific region (Anonymous, 2016; Dong et al., 2016; Dwyer et al., 2015; Ediati et al., 2015; Jones, 2016; Kalra et al., 2016; Khadilkar et al., 2015; Mohamed & Noor, 2015; Palanisamy et al., 2015; Tinney et al., 2015; Vasundhera et al., 2016; Wang & Tian, 2015), six from Europe (Achermann et al., 2015; Bonanni et al., 2015; Kim et al., 2015; Lalor, 2015; Lucas-Herald et al., 2015; Mannaerts et al., 2015), three from Africa (Ahmed & Fadl-Elmula, 2016; Ekenze et al., 2015; Latrech et al., 2015), and two from the Middle East (Gül et al., 2015; Mutlu et al., 2015)—see Figure 1. The sources specifically featured studies from a total of 21 countries. Over half (31) of the studies were based in the United States (Amanda, 2015; Amarillo et al., 2016; Anderson, 2015; Baratz & Karkazis, 2015; Cynthia, 2015; Davis, 2015b; Dreger, 2015; Frader, 2015; Garcia, 2015; Grimes, 2016; Grover et al., 2015; Howard, 2015; Inter, 2015; Kelsey et al., 2016; Kraus, 2015; Lin-Su et al., 2015; Long, 2015; Miller, 2015; Pagonis, 2015; Petersen, 2015; Quinn, 2015; Rubin, 2015; Saraswat et al., 2015; Simon, 2015; Topcu et al., 2015; Truffer, 2015; Viloria, 2015; von Klan, 2015; Wall, 2015; Walsh, 2015; Zieselman, 2015). Four studies were based in India (Kalra et al., 2016; Khadilkar et al., 2015; Palanisamy et al., 2015; Vasundhera et al., 2016), three in Australia (Dwyer et al., 2015; Jones, 2016; Tinney et al., 2015), and three in Brazil (Brasileiro et al., 2016; Oliveira et al., 2015; Paula et al., 2015). Two studies were based in China (Dong et al., 2016; Wang & Tian, 2015), Turkey (Gül et al., 2015; Mutlu et al., 2015), and the United Kingdom (Achermann et al., 2015; Lalor, 2015). Individual studies were based in Belgium (Mannaerts et al., 2015), Canada (Grimbly et al., 2016), Indonesia (Ediati et al., 2015), Italy (Bonanni et al., 2015), Malaysia (Mohamed & Noor, 2015), Malta (Ceci et al., 2015), Mexico (Rios et al., 2015), Morocco (Latrech et al., 2015), New Zealand (Anonymous, 2016), Nigeria (Ekenze et al., 2015), Scotland (Lucas-Herald et al., 2015), Spain (Camats et al., 2015), and Sudan (Ahmed & Fadl-Elmula, 2016). One study largely based in Germany included collaborative multi-national input (Kim et al., 2015).1

Number of sources by global region.
The overwhelming majority of the sources came from peer-reviewed journals (Achermann et al., 2015; Ahmed & Fadl-Elmula, 2016; Amanda, 2015; Amarillo et al., 2016; Anderson, 2015; Anonymous, 2016; Baratz & Karkazis, 2015; Bonanni et al., 2015; Brasileiro et al., 2016; Camats et al., 2015; Ceci et al., 2015; Cynthia, 2015; Davis, 2015b; Dong et al., 2016; Dwyer et al., 2015; Ediati et al., 2015; Ekenze et al., 2015; Frader, 2015; Garcia, 2015; Grimbly et al., 2016; Grimes, 2016; Grover et al., 2015; Gül et al., 2015; Howard, 2015; Inter, 2015; Jones, 2016; Kalra et al., 2016; Kelsey et al., 2016; Khadilkar et al., 2015; Kim et al., 2015; Kraus, 2015; Lalor, 2015; Latrech et al., 2015; Lin-Su et al., 2015; Long, 2015; Lucas-Herald et al., 2015; Mannaerts et al., 2015; Miller, 2015; Mohamed & Noor, 2015; Mutlu et al., 2015; Oliveira et al., 2015; Pagonis, 2015; Palanisamy et al., 2015; Paula et al., 2015; Petersen, 2015; Quinn, 2015; Rios et al., 2015; Rubin, 2015; Saraswat et al., 2015; Simon, 2015; Tinney et al., 2015; Topcu et al., 2015; Truffer, 2015; Vasundhera et al., 2016; Viloria, 2015; von Klan, 2015; Wall, 2015; Walsh, 2015; Wang & Tian, 2015; Zieselman, 2015). One was from a peer-reviewed book series (Dreger, 2015). Most of the journals represented were either medical journals or at least broadly covering a thematic remit inclusive of medical science issues. The largest number of articles (18) from a repeatedly represented journal came from Narrative Inquiry in Bioethics due to its release of a special issue (Volume 5, Issue 2) focused solely on intersex themes not otherwise typical for that journal (Amanda, 2015; Baratz & Karkazis, 2015; Cynthia, 2015; Davis, 2015b; Frader, 2015; Garcia, 2015; Inter, 2015; Long, 2015; Pagonis, 2015; Petersen, 2015; Quinn, 2015; Simon, 2015; Truffer, 2015; Viloria, 2015; von Klan, 2015; Wall, 2015; Walsh, 2015; Zieselman, 2015). Multiple articles also came from Journal of Pediatric Endocrinology and Metabolism (Brasileiro et al., 2016; Grover et al., 2015; Mutlu et al., 2015; Oliveira et al., 2015; Paula et al., 2015; Topcu et al., 2015), and three articles from International Journal of Pediatric Endocrinology (Grimbly et al., 2016; Lin-Su et al., 2015; Lucas-Herald et al., 2015). Two articles came from Archives of Sexual Behavior (Ediati et al., 2015; Kraus, 2015), BMJ Case Reports (Bonanni et al., 2015; Mannaerts et al., 2015), Endocrine Practice (Khadilkar et al., 2015; Saraswat et al., 2015), Indian Journal of Endocrinology and Metabolism (Kalra et al., 2016; Vasundhera et al., 2016) and PLoS ONE (Camats et al., 2015; Kelsey et al., 2016). These journals historically appeared to have evidenced regular past attention to intersex themes over time outside of the pieces represented in this literature review. Of the remaining sources, most (15) came from individual journals/publishing series in areas of the medical or broader health sciences that have had some association with intersex themes in the past—in genetics (Amarillo et al., 2016; Dong et al., 2016; Kim et al., 2015), endocrinology (Achermann et al., 2015; Khadilkar et al., 2015; Latrech et al., 2015), biology (Ahmed & Fadl-Elmula, 2016; Rios et al., 2015), nursing (Anderson, 2016; Anonymous, 2016), pediatric or other surgery (Ekenze et al., 2015; Palanisamy et al., 2015), psychogeriatrics (Tinney et al., 2015), neuropsychiatry (Gül et al., 2015), and urology (Ceci et al., 2015). Only nine sources came from nonmedical journals—in education (Jones, 2016; Miller, 2015), science ethics (Dreger, 2015; Mohamed & Noor, 2015), religion (Grimes, 2016), rural society (Dwyer et al., 2015; Howard, 2015), and feminist legal studies (Lalor, 2015; Rubin, 2015). These latter journals did not otherwise evidence regular past coverage of intersex themes.
Theoretical Lenses
Direct explanations of the theoretical lenses applied in the studies behind the sources were rare. However, the conceptual framings used in the studies were nevertheless apparent in the way the sources framed people with intersex variations (whether in pathologizing through to deconstructive views), positioned the researcher (whether as the subject, object, or context of inquiry) reported on data (whether using positivist through to poststructuralist approaches), and so on. The theoretical lenses applied in the studies were alternately expert-centered, patient-centered, group-centered, or theory-centered (see Table 1).
Theoretical Lenses Applied in Literature by Number of Sources.

Note. LGBTIQ = lesbian, gay, bisexual, transgender, intersex, and questioning.
Institutional expert-centered
Over a third (23) of the sources featured studies with a Traditional Clinical/Medical lens or conceptual framing (Ahmed & Fadl-Elmula, 2016; Amarillo et al., 2016; Bonanni et al., 2015; Brasileiro et al., 2016; Camats et al., 2015; Ceci et al., 2015; Dong et al., 2016; Ediati et al., 2015; Ekenze et al., 2015; Grimbly et al., 2016; Grover et al., 2015; Kelsey et al., 2016; Khadilkar et al., 2015; Kim et al., 2015; Latrech et al., 2015; Lucas-Herald et al., 2015; Mannaerts et al., 2015; Mutlu et al., 2015; Palanisamy et al., 2015; Paula et al., 2015; Rios et al., 2015; Topcu et al., 2015; Vasundhera et al., 2016). This lens privileged a view of people with intersex variations as patients with DSD and consideration of pathology in (usually some combination of any of) their anatomy (Dong et al., 2016), biology (Rios et al., 2015), endocrinology (Mutlu et al., 2015), genealogy (Kim et al., 2015), and/or urology (Ceci et al., 2015). The group was thus cast in these sources as in need of expert-centered clinically/institutionally based analysis, diagnosis, and often corrective treatment, for example, hormone therapy (Grover et al., 2015) or genital surgeries (Brasileiro et al., 2016). The researchers creating the sources were generally medical doctors, surgeons, or scientists, and applied their interrogative work to their patients or the patients’ perceived disorders (rather than to their own medical practices, biases, or philosophies, for example). Their reports were pitched at, for example, improving DSD diagnosis methods (Grimbly et al., 2016), refining analysis techniques and/or intervention techniques or practices (Khadilkar et al., 2015), and/or drawing attention to rare cases (Palanisamy et al., 2015). Data and standards for data were treated in a positivist manner (as being self-evident and not conceptually in dispute). A more unique theoretical lens which otherwise supported traditional views of patients as having DSDs in a largely pathologizing manner and which relied on expert-centered (religious and clinical) analysis was seen in one additional source which used a Maqasid al-Shari’ah lens: requiring the mechanistic interpretation of Qur’an and Hadith toward Islamic views on health care for patients with DSD (Mohamed & Noor, 2015).
Patient-centered
A small portion of the sources (five sources) featured Liberal Constructivist views on clinical practice privileging patient-centered care and some element of patient choice (Achermann et al., 2015; Kalra et al., 2016; Lin-Su et al., 2015; Oliveira et al., 2015; Saraswat et al., 2015; Wang & Tian, 2015). The researchers creating the sources were a combination of people with medical and other academic backgrounds, who applied their interrogative work to patients’ or represented parties’ perceptions of their own needs, experiences, and identities, sometimes including in literature (Kalra et al., 2016) or diagnostic manuals. Their reports were pitched at improving patient quality of life and holistic experience (Lin-Su et al., 2015), and/or some elements of clinical practices to enable a greater range of options to patients (Achermann et al., 2015). Data and standards for data were treated in a progressive manner (as being subjective and individually specific). More unique theoretical lenses which otherwise supported liberal views on patients as having DSDs (sometimes called “differences” in sex development in a destigmatizing manner) were seen in two additional sources (Gül et al., 2015; Kalra et al., 2016). One used a Phenomenology lens: requiring the interpretation of an individual patient’s experiences—in this case, of gendered psychotic delusions in relation to their social experience of intersex diagnosis (Gül et al., 2015). Another used a Liberal Literary Forensic Analysis lens: requiring consideration of ancient textual characters’ reported experiences as potentially aligned with modern experiences of DSDs (Kalra et al., 2016).
Community group-centered
There was strong representation (in 18 sources) of the Bioethical Narrative Inquiry lens specifically from Narrative Inquiry in Bioethics Volume 5, Issue 2 (Amanda, 2015; Baratz & Karkazis, 2015; Cynthia, 2015; Davis, 2015b; Frader, 2015; Garcia, 2015; Inter, 2015; Long, 2015; Pagonis, 2015; Petersen, 2015; Quinn, 2015; Simon, 2015; Truffer, 2015; Viloria, 2015; von Klan, 2015; Wall, 2015; Walsh, 2015; Zieselman, 2015). The introducing editor Georgiann Davis had actively described the issue as intentionally pitched at disrupting the dominance of Medical/Clinical lenses for work on people with intersex variations (Davis, 2015b). The lens privileged a critical view of people with intersex variations as members of a marginalized community group overall who had collectively been at risk of poor access to medical information about their conditions or structures privileging bodily autonomy in medical settings. The use in this frame of autobiography or personal recall of conversations with individuals from the group also cast intersex people as individuals with underrepresented experiences of specific variations, stories, personalities, desires, and health care phenomena (such as interactions and dynamics with family members and medical staff) impacting their different health care needs. Standards for data were de-institutionalized; the sources valued visibility or other rights-based goals for the collective social group rather than traditional notions of rigor or precision. Other group-centered lenses represented included Critical Intersex Studies lenses (in three sources) focused on human rights and bodily autonomy for intersex people as a specific group, via philosophical or textual analysis (Anderson, 2015; Anonymous, 2016; Kraus, 2015). Also, Critical LGBTI Liberationism (in three sources) focused on nondiscrimination rights for LGBTI people more broadly (Dwyer et al., 2015; Howard, 2015; Tinney et al., 2015). The latter lens did not include a clear conceptualization of intersex people as separate from lesbian, gay, bisexual, and transgender (LGBT) people, and therefore examples did not feature clear active intersex participation.
Theory-centered
The remaining sources (six sources) featured variously conceived deconstructive lenses which generally required conceptual critique of other theoretical approaches to people with intersex variations seen in health-related research, polity, or literature (Dreger, 2015; Grimes, 2016; Jones, 2016; Lalor, 2015; Miller, 2015; Rubin, 2015). These lenses included application of Queer historiography of health science (Dreger, 2015): a Critical-Queer feminist theology (Grimes, 2016), a Transnational feminist frame (Rubin, 2015), a Postmodern and critical sociology of health (Jones, 2016), Poststructural feminist legal studies (Lalor, 2015), and Queer theory (Miller, 2015). In these lenses, theory or philosophy itself (including nomenclature and theoretical constructions of people with intersex variations and their health care needs) are interrogated whether in law or polity (Lalor, 2015), in literature or theological texts, and/or in fields of language and conceptualization impacting health care (Grimes, 2016; Miller, 2015). Research itself, and researchers, came into question (Dreger, 2015; Rubin, 2015) and were cast as limited by their sociohistoric and location-based contexts, field-based biases and constraints, and exposures to diverse visions of health care (Dreger, 2015; Rubin, 2015).
Methods and Participant Numbers
Overall, the sources represented studies using a range of methods, including clinical, textual, and socially oriented approaches. The sources included a broad array of participant numbers, ranging from sources with unclear numbers of people with intersex variations (Dwyer et al., 2015; Howard, 2015; Kim et al., 2015; Rios et al., 2015) through to a source with 272 participants specifically from the group (Jones, 2016). Higher numbers were rare, however, as over a third of the sources focused on only one participant (Amanda, 2015; Bonanni et al., 2015; Brasileiro et al., 2016; Ceci et al., 2015; Cynthia, 2015; Davis, 2015b; Garcia, 2015; Grimbly et al., 2016; Grover et al., 2015; Gül et al., 2015; Inter, 2015; Kalra et al., 2016; Long, 2015; Mannaerts et al., 2015; Mutlu et al., 2015; Pagonis, 2015; Palanisamy et al., 2015; Paula et al., 2015; Petersen, 2015; Quinn, 2015; Simon, 2015; Truffer, 2015; Viloria, 2015; von Klan, 2015; Walsh, 2015; Zieselman, 2015). Almost as many had no direct participants with intersex variations and, instead, used the general existence of the group, other participants, or secondary sources to make key arguments about intersex variations (Achermann et al., 2015; Anderson, 2015; Anonymous, 2016; Baratz & Karkazis, 2015; Dreger, 2015; Frader, 2015; Grimes, 2016; Kelsey et al., 2016; Kraus, 2015; Lalor, 2015; Miller, 2015; Mohamed & Noor, 2015; Oliveira et al., 2015; Rubin, 2015; Saraswat et al., 2015; Tinney et al., 2015). The sources also included a wide span of ages ranging from 1 day (Lucas-Herald et al., 2015) to 87 years of age (Jones, 2016). Over a third of the sources did not specify the precise ages of participants or the group being referred to (Achermann et al., 2015; Amarillo et al., 2016; Anderson, 2015; Baratz & Karkazis, 2015; Camats et al., 2015; Dong et al., 2016; Dreger, 2015; Dwyer et al., 2015; Ediati et al., 2015; Frader, 2015; Grimes, 2016; Howard, 2015; Kalra et al., 2016; Kim et al., 2015; Kraus, 2015; Lalor, 2015; Lin-Su et al., 2015; Miller, 2015; Mohamed & Noor, 2015; Rios et al., 2015; Saraswat et al., 2015). Around a third focused on (or could be assumed to have focused on, given the span of time covered in the piece) adults 18 years and above (Amanda, 2015; Anonymous, 2016; Ceci et al., 2015; Cynthia, 2015; Davis, 2015b; Garcia, 2015; Gül et al., 2015; Inter, 2015; Jones, 2016; Long, 2015; Mannaerts et al., 2015; Oliveira et al., 2015; Pagonis, 2015; Palanisamy et al., 2015; Petersen, 2015; Quinn, 2015; Rubin, 2015; Simon, 2015; Tinney et al., 2015; Truffer, 2015; Viloria, 2015; von Klan, 2015; Wall, 2015; Walsh, 2015; Zieselman, 2015). Ten sources focused purely on infants and/or young people below 18 years (Bonanni et al., 2015; Brasileiro et al., 2016; Ekenze et al., 2015; Grimbly et al., 2016; Grover et al., 2015; Latrech et al., 2015; Lucas-Herald et al., 2015; Mutlu et al., 2015; Paula et al., 2015; Topcu et al., 2015). Five explicitly focused on a precise participant group, age-range crossing over younger and adult age groups (Ahmed & Fadl-Elmula, 2016; Kelsey et al., 2016; Khadilkar et al., 2015; Vasundhera et al., 2016; Wang & Tian, 2015).
Figure 2 shows the seven types of methods described in the sources. The most common methods in 18 sources constituted autobiographical critical analyses/narratives of author’s intervention impacts, observations, and/or views (Amanda, 2015; Baratz & Karkazis, 2015; Cynthia, 2015; Davis, 2015b; Frader, 2015; Garcia, 2015; Inter, 2015; Long, 2015; Pagonis, 2015; Petersen, 2015; Quinn, 2015; Simon, 2015; Truffer, 2015; Viloria, 2015; von Klan, 2015; Wall, 2015; Walsh, 2015; Zieselman, 2015). These studies were mainly on one adult individual (usually a community member rather than an MD or academic) considering his or her own experiences across his or her lifetime, especially the negative well-being impacts of receiving a lack of information and/or negative well-being and health impacts of early intervention without express consent (including feelings of disconnection from health care processes, trauma and depression, infertility, decreased sexual function/pleasure, undesired sex-based presentations, and/or surgical complications). Two of these pieces focused on secondary data (observations) about the lack of dissemination of information or consultation with people with intersex variations about their health needs and experiences, seen as an abuse of the group leading to unwanted outcomes (Baratz & Karkazis, 2015; Frader, 2015). In one example, a pediatrician expressed concern about his and others’ own endorsements of past gonad removals (e.g., removing testes from females) on the basis of potentially imagined cancer and “corrective” clinical concerns, given retained gonads can provide patients with a “natural” form of hormone production (Frader, 2015).
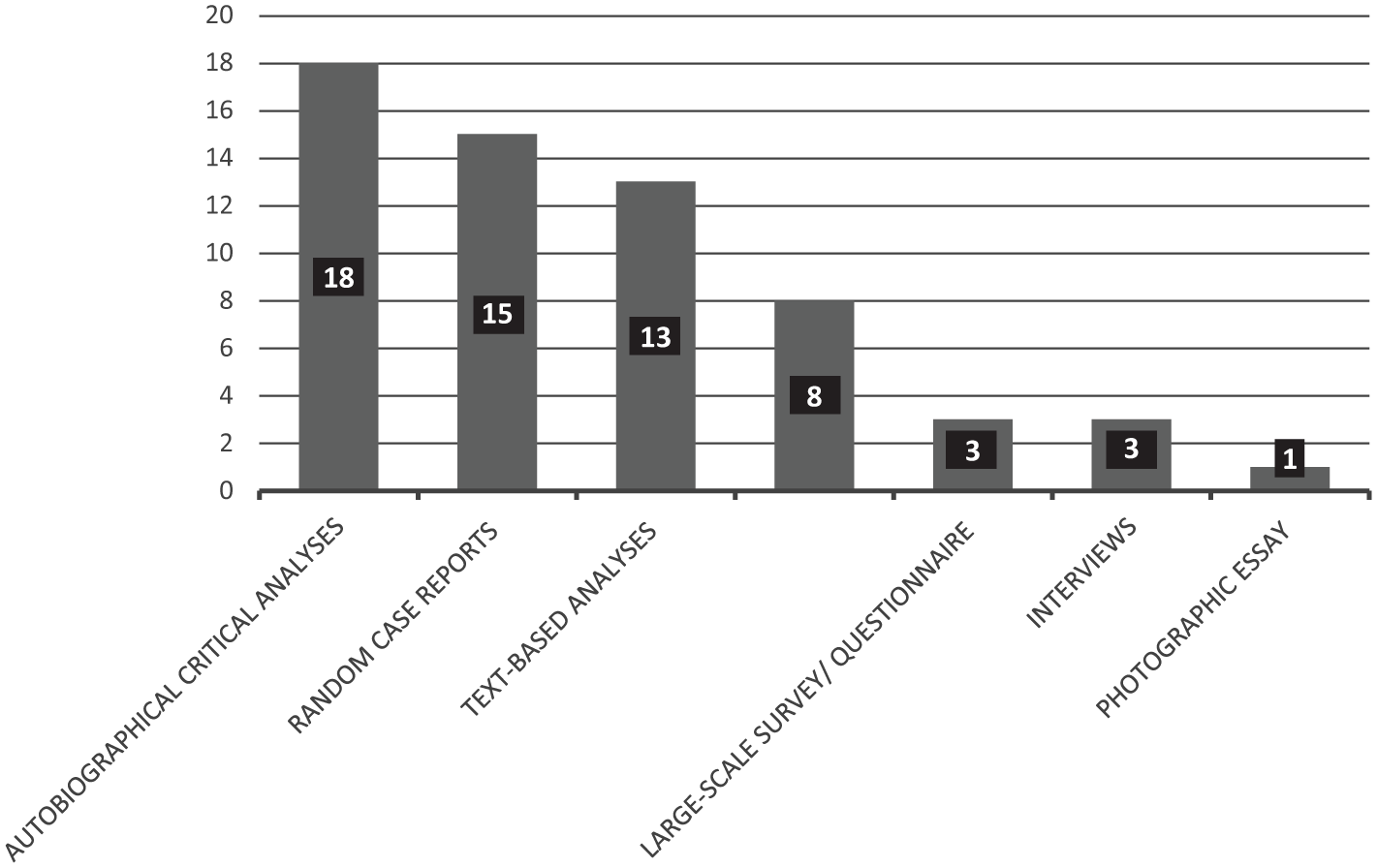
Number of textual sources reporting on particular study method types (n = 61).
The second most common methods were random case reports (15 sources) on analyses of patients toward diagnosis and/or interventions (Ahmed & Fadl-Elmula, 2016; Bonanni et al., 2015; Brasileiro et al., 2016; Ceci et al., 2015; Ekenze et al., 2015; Grimbly et al., 2016; Grover et al., 2015; Gül et al., 2015; Khadilkar et al., 2015; Latrech et al., 2015; Mannaerts et al., 2015; Mutlu et al., 2015; Palanisamy et al., 2015; Paula et al., 2015; Vasundhera et al., 2016). These were pieces written by MDs/academics on variably one to 108 participants with intersex variations whom they had analyzed and treated clinically—mainly just one infant or young person who had been subjected to tests (anatomical, cytogenetic, hormonal, and/or radiological evaluations) and often hormonal and/or surgical interventions (e.g., genital surgeries such as gonad removals or cosmetic constructive work, for example, or mastectomies and so on). Evaluations of the cases strongly privileged the MDs/academics assessment of analytical or intervention “success,” and the pieces gave a strong overall message that in the authors’ own views, the interventions they had applied were successful overall. In fairness, the purpose of such papers is usually to present a novel approach to medical management, and as such would be expected to treat the “case” as a medical condition needing treatment. However, this meant the sources largely did not report on the participants’ own assessment of the need for or success of the treatments, which could be relevant measures. Several contained direct photographs of patients’ internal and external genitalia (Ahmed & Fadl-Elmula, 2016; Brasileiro et al., 2016; Ekenze et al., 2015; Palanisamy et al., 2015); in some of the photos, children’s external genitalia were arranged for display by another party’s bare (not gloved) hands (Ahmed & Fadl-Elmula, 2016; Brasileiro et al., 2016; Ekenze et al., 2015). Those sources offered no clarity about what permissions were obtained or what ethical consideration was given to the photography process or the individual’s international online exposure, constructing the bodies of this group as quite freely intimately accessible without obvious ethical or hygiene considerations to medical experts, and to any interested viewers globally.
The third most common methods were largely text-based analyses (13 sources) including literature reviews and socio-historical analyses of secondary records of people with intersex variations/diagnoses/intersex groups/relevant events (Achermann et al., 2015; Anderson, 2015; Dreger, 2015; Dwyer et al., 2015; Grimes, 2016; Kalra et al., 2016; Kraus, 2015; Lalor, 2015; Miller, 2015; Mohamed & Noor, 2015; Rubin, 2015; Saraswat et al., 2015; Tinney et al., 2015). These analyses were conducted mainly by academics with a range of training (health sciences, law, sociology, education, etc.) on no (Grimes, 2016), through to unclear (Dwyer et al., 2015), numbers of participants with intersex variations. The studies mainly used the general existence of, or cited textual or historical incidences of, people with intersex variations—or else their fictional existence or classification/construction (Kalra et al., 2016; Mohamed & Noor, 2015; Rubin, 2015). These studies mostly problematized the way people with intersex variations have been presented in classifications, historical incidences, or socially. The fourth most common methods could be considered systematic experimental group testing/modeling (eight sources) of a novel medical approach or hypothesis like, for example, Magnetic Resonance Imaging, Copy Number Variation and cell transgenic experiments, gene network modeling, and so on (Amarillo et al., 2016; Camats et al., 2015; Dong et al., 2016; Kelsey et al., 2016; Kim et al., 2015; Lucas-Herald et al., 2015; Rios et al., 2015; Topcu et al., 2015). These studies were variably on zero (Kelsey et al., 2016) to 93 (Lucas-Herald et al., 2015) participants with intersex variations. The study with no participants with intersex variations modeled measures for the intersex females’ internal genitalia based on another group—only what it termed “healthy females” aged 0 to 40 years (Kelsey et al., 2016). The pieces gave a strong overall message that in the authors’ own views, the medical approaches or hypotheses they had applied had been largely successful overall.
A less common method (three sources) included the use of a large-scale survey/questionnaire (Jones, 2016; Lin-Su et al., 2015; Wang & Tian, 2015). These studies had the most participants with intersex variations: variably 87 (Wang & Tian, 2015) to 272 (Jones, 2016). These studies considered teenagers through to significantly older adults’ perspectives on their own experiences of quality of life, nomenclature, and/or a combination of medical and social experiences and services. These studies problematized a range of health care–related issues including casting use of DSD as a disordering term and conceptualization (Jones, 2016; Lin-Su et al., 2015), noting problems with interventions and/or sexual experiences postinterventions (Jones, 2016; Wang & Tian, 2015), and decrying the lack of direct consultation around the groups’ needs generally in relation to a range of general health care (Wang & Tian, 2015), mental health (Lin-Su et al., 2015), and school-based health education services (Jones, 2016). Another less common method (three sources) was interviews (Anonymous, 2016; Ediati et al., 2015; Oliveira et al., 2015). These studies had variably zero (Anonymous, 2016) to 118 (Ediati et al., 2015) participants with intersex variations. One article discussed interviews of parents on how health workers disclosed their child’s “DSD” diagnoses (Oliveira et al., 2015), one discussed an interview with an expert on interventions (Anonymous, 2016), and one a set of clinical psychological interviews (Ediati et al., 2015). Ages of specific interviewees were not consistently clearly specified in these studies, although participants could mostly be inferred to be adults. These articles problematized the lack of health care information dissemination and psychological follow-up for people with intersex variations from their different stakeholders’ perspectives (parents, experts, and patients). While the Indonesian interviewers argued for intervention based on its infrequency in their context and their perception was that their context was therefore lacking (Ediati et al., 2015), the interviewed expert—a nursing clinician from New Zealand—argued that intervention on intersex infants was traumatizing and unnecessary (Anonymous, 2016). One unique study constituted a photographic essay documentation and analysis of public change and continuity in Rankin County’s LGBTI citizens (Howard, 2015). It was unclear which or how many participants were specifically intersex in the original photographic data, or whether the term LGBTI was simply applied as an umbrella term in an inclusive spirit or in evaluation of perceived likely participation. The essay argued that LGBTI people were generally marginalized in a range of local health and care services.
Framing of Participants and Health-Related Messages About Interventions
The sources provided a mixture of messages about health care intervention for people with intersex variations: 27 sources cast medical interventions as potentially problematic for the group’s health or well-being (Amanda, 2015; Anderson, 2015; Anonymous, 2016; Baratz & Karkazis, 2015; Cynthia, 2015; Davis, 2015b; Dreger, 2015; Frader, 2015; Garcia, 2015; Grimes, 2016; Inter, 2015; Jones, 2016; Kraus, 2015; Lalor, 2015; Long, 2015; Miller, 2015; Pagonis, 2015; Petersen, 2015; Quinn, 2015; Saraswat et al., 2015; Simon, 2015; Truffer, 2015; Viloria, 2015; von Klan, 2015; Wall, 2015; Walsh, 2015; Zieselman, 2015). Nineteen cast interventions as unproblematic (Achermann et al., 2015; Ahmed & Fadl-Elmula, 2016; Amarillo et al., 2016; Bonanni et al., 2015; Brasileiro et al., 2016; Ceci et al., 2015; Dong et al., 2016; Ediati et al., 2015; Ekenze et al., 2015; Grimbly et al., 2016; Kelsey et al., 2016; Khadilkar et al., 2015; Latrech et al., 2015; Lucas-Herald et al., 2015; Mannaerts et al., 2015; Mutlu et al., 2015; Palanisamy et al., 2015; Paula et al., 2015; Wang & Tian, 2015), and 15 presented unclarified/mixed views (Camats et al., 2015; Dwyer et al., 2015; Grover et al., 2015; Gül et al., 2015; Howard, 2015; Kalra et al., 2016; Kim et al., 2015; Lin-Su et al., 2015; Mohamed & Noor, 2015; Oliveira et al., 2015; Rios et al., 2015; Rubin, 2015; Tinney et al., 2015; Topcu et al., 2015; Vasundhera et al., 2016). These messages roughly aligned with the use of nomenclature and sometimes certain theoretical lenses. Noticeably, the strongest divide was between the use of community-related terms and medically related terms (Figure 3). Over a third of sources (26 of 61, including all 18 sources using the Bioethical Narrative Inquiry theoretical lens) applied the term “intersex” to the group, largely framing the group as a marginalized group with specific service needs, sex traits not considered standard socially/theologically, and a need for protection from unwanted discrimination (Amanda, 2015; Anonymous, 2016; Baratz & Karkazis, 2015; Cynthia, 2015; Davis, 2015b; Dreger, 2015; Frader, 2015; Garcia, 2015; Grimes, 2016; Inter, 2015; Jones, 2016; Kalra et al., 2016; Kraus, 2015; Long, 2015; Pagonis, 2015; Petersen, 2015; Quinn, 2015; Rubin, 2015; Simon, 2015; Tinney et al., 2015; Truffer, 2015; Viloria, 2015; von Klan, 2015; Wall, 2015; Walsh, 2015; Zieselman, 2015). Some studies using this nomenclature included people with specific variations, including, for example, 47XXY, AIS, CAH, Kallman’s, Klinefelter’s, PCOS-related hyperandrogenism, and over 40 others (Jones, 2016); while other studies were more generalized in discussing individuals born with sexual anatomies that various societies deem to be nonstandard (Rubin, 2015), or “endocrinology-related features” that can be read as intersex (Kalra et al., 2016). A few studies applying Queer conceptualizations of the word intersex described the group as disrupting the sex binary (male/female) or dominant sex and gender discourse (Grimes, 2016). Most sources using the “intersex” nomenclature cast the group as unfairly subjected to cosmetic surgery in problematic ways as infants and young people with negative outcomes for their health and well-being (Anonymous, 2016), and having largely unheard perspectives on their choices and negative experiences that needed to be privileged (Davis, 2015b). These studies called for greater consultation in health care, health care policy production, and the development of mental health services.

Number of textual sources using particular group nomenclature for people with intersex variations (n = 61).
A similar portion of sources (24 of 61, including 20 of the 23 sources featuring the Traditional Clinical/Medical theoretical lens) applied the phrase “patients with disorders of sex development/DSD” to the group, largely framing the group as containing smaller groups of patients with specific sets of disorders to be analyzed, with a range of medical needs sometimes confronting to family or medical staff (Achermann et al., 2015; Ahmed & Fadl-Elmula, 2016; Amarillo et al., 2016; Brasileiro et al., 2016; Camats et al., 2015; Dong et al., 2016; Ediati et al., 2015; Ekenze et al., 2015; Grimbly et al., 2016; Gül et al., 2015; Kelsey et al., 2016; Khadilkar et al., 2015; Kim et al., 2015; Latrech et al., 2015; Mannaerts et al., 2015; Mohamed & Noor, 2015; Mutlu et al., 2015; Oliveira et al., 2015; Paula et al., 2015; Rios et al., 2015; Saraswat et al., 2015; Topcu et al., 2015; Vasundhera et al., 2016; Wang & Tian, 2015). Sometimes, concepts considered offensive or inaccurate to community members were applied as types of subclassifications where this DSD language was used, such as pieces casting the group as presenting in “pseudohermaphroditism”/“true hermaphroditism” (Gül et al., 2015) and having “abnormal” chromosomal, hormonal, or anatomical traits (Ahmed & Fadl-Elmula, 2016). Several of the studies actually contrasted the group against what they termed “normal” people in terms of anatomy or other traits (Camats et al., 2015). There was a strong focus in sources using DSD nomenclature on the cause of the group’s “abnormal” traits (Camats et al., 2015; Kim et al., 2015; Topcu et al., 2015); the need for managing parents’ experiences of shock and stigma and aiding their intervention choices for their child rather than patient choice (Achermann et al., 2015; Oliveira et al., 2015); and an assumption of the value and success of early intervention (Paula et al., 2015). A smaller group (four of 61) exclusively used the specific diagnosis or condition in focus only, framing the group in terms of particular condition-based traits and risks (Bonanni et al., 2015; Lin-Su et al., 2015; Lucas-Herald et al., 2015; Palanisamy et al., 2015). These included patients with persistent mullerian duct syndrome (PMDS; Palanisamy et al., 2015), patients with CAH (Lin-Su et al., 2015), patients with Turner syndrome (TS; Bonanni et al., 2015), and children with suspected disorders of steroid/hormone synthesis (Lucas-Herald et al., 2015). The sources using group-specific nomenclature were mostly affirming and unquestioning about the need for early analysis and intervention, although one considered the need for greater consultation with the patient group (Lin-Su et al., 2015).
There was a small portion of sources (four of 61, including all sources using the Critical LGBTI Liberationist theoretical lens) that mainly applied the phrase “lesbian, gay, bisexual, transgender and intersex/LGBTI” or similar acronyms (Dwyer et al., 2015; Howard, 2015; Lalor, 2015; Miller, 2015), whether the specific acronym LGBTI (Howard, 2015; Lalor, 2015), LGBTIQ (Dwyer et al., 2015), or LGBT*IAGCQ youth (*IAGCQ included intersex, agender/asexual, gender creative, and questioning) was used (Miller, 2015). These sources framed the group within a broader politically and socially marginalized community, usually with rights protections in law, policy, or ethical frames which need to be asserted. Even within this group, the intersex people were cast as the subgroup for which mental health information, specifically for older people, was most minimal (Tinney et al., 2015). These studies took mixed or neutral approaches to corrective intervention, however, not collectively providing critique or endorsement. Finally, the smallest portion (three of 61 sources, including two using the Traditional Clinical/Medical theoretical lens) applied the phrase “Disorders of sexual differentiation/DSD,” a term used in a similar manner to the other DSD acronym with emphasis on sex trait and genital ambiguity (Anderson, 2015; Ceci et al., 2015; Grover et al., 2015). Perhaps this was intended to be less pathologizing—although given it was used in one of the articles used in conjunction with the terms “disorder” and “hermaphroditism,” the possibility of any depathologizing rationale was in question (Ceci et al., 2015). No clear relationship between this nomenclature and approaches to health care or intervention could be determined.
Discussion
The data suggested a developing divergence in the literature from the long-established location of health-related studies on people with intersex variations within the institutional expert-based orientation, particularly Traditional Medical/Clinical framings and their remaining overall dominant concentration in medical journals. This was particularly affected by not only American and Australian work, for example, but also other contexts. Clearly, more patient-centered, community-centered, and theory-centered work is emerging in this field—particularly a range of Critical Bioethics and Intersex Studies perspectives which have emerged and are actively challenging the way this group is framed. This has included a trend toward new nomenclature and considerations. In this literature review, the large number of expert-centered sources promoting interventionalist pathologizing views on “patients with DSDs” were equaled by the large number of community group–centered and other sources promoting a critique of these dominant health care attitudes on the basis of marginalized “intersex” peoples’ perspectives, bodily autonomy, and rights. This reflected broader debates in the field discussed in other papers chronicling recent resistance to the assumption people with intersex variations need cosmetic correction from international human rights organizations, Queer theoretical work, and community-based sources (Davis, 2015a; Jones et al., 2016; OII Australia, 2012a; Turner, 1999; United Nations, 2012). This literature evidenced a shift toward a view of medical intervention as problematic.
However, older conceptualizations of clinicians as having unmitigated rights over patients remain in a significant portion of the literature—this was particularly evident in the lack of consideration some researchers gave to patients’ perspectives on their health care in the sources, and moreover the problematic use of photographs of participants’ external genitalia illustrated in several case studies. Researchers are in an extremely powerful position over these studies’ participants (especially if their participants are also their patients and at their mercy for medical care, moreover if they are children). People with intersex variations have complained about feelings of being abused in medical and research scenarios where their variations were shared without their permission, let alone access to their bodies (especially their genitalia) whether put on display or touched and photographed (Jones et al., 2016). Anonymized diagrams would have sufficed in outlining specific anatomical indicators of intersex variations without compromising an individual patient’s respectful treatment (recalling the lack of glove use) or right to control over their genitalia and its depiction (recalling that permissions were either unobtainable for infants or not reported from adults). A limitation of this review is that it is unclear from examining the literature itself with whom the responsibility would legally lie to ensure permissions for procedures or photographs were obtained, or if any such responsibility is allocated in various global contexts. In future, clinicians will need to start listening to the growing push from people with intersex variations for greater consultancy around interventions impacting sex traits (especially hormones and genitalia) by ideally holding off on such intervention and only pursuing it in consultation with and consideration of the recipient (at an age where this is possible). Another limit of this review is that constructions of ages by which informed consent might be possible were not examined; this is an area for researchers and policy makers to start considering. To a smaller extent, another concern in the literature was that publications claiming to be on “LGBTI” people appeared not to have been reviewed for whether they actually contain people with intersex variations; this issue could be better addressed in advice given to researchers from both ethics committees in research institutions and research publishers and peer-reviewers, as relevant. Intersex activists have mixed views on inclusion in LGBTI studies—some argue heteronormativity marks intersex bodies as “queer bodies” making LGBTI and anti-homophobia perspectives applicable (Holmes, 1994). Others argue that LGBTI work exposes intersex people to added homophobia and “pinkwashing”—having their goals deprioritized against gay groups’ goals (Koyama & Weasel, 2001; Pagonis, 2016).
Conclusion
Clinicians’ analyses of clinical processes around people with intersex variations may indeed provide some valuable information and cast intervention work in affirming ways. However, external analyses from lenses that really privilege people with intersex variations themselves as agentic subjects in a more empowering dynamic, than simply a patient-object, show a strong disconnection between how clinicians and people with intersex variations consider health care provision. Notably, there has been an increasing level of consultancy with patient advocate groups in some contexts in recent years, and major shifts away from performing unnecessary procedures on infants (in the reported experiences of both the author, who has worked with Government Advisory Groups on intersex policy issues in Victoria Australia, and of members of this article’s peer review team). It is important for more clinicians to respond to the largely community-based and rights-based pushes for a patient-centered model of intersex health care. Patient-centered care literature broadly privileges principles of prioritizing an individual patient’s goals and well-being, building a relationship which empowers a patient, making accessible clinician communication with the patient routine, and using patient experience narratives and feedback toward service improvement (Koyama & Weasel, 2001). A patient-centered approach to patients with intersex variations would therefore foreground greater valuing of the holistic well-being of the individual in the long term, their diverse needs and identity potentials, their possible fertility and hormone balance, their sexual function (not just in a simplistic valuing of penetrative sex but in a valuing of the full range of human sexual pleasures and possibilities), and their many other autonomous considerations only discoverable through placing proper consultation and support processes in place in all clinical settings. It would acknowledge that many patients later in life have bodily autonomy goals which differ from guardians’ goals to have their childrens’ bodies become “normalised” (Jones et al., 2016). Contemporary clinicians should seek and prioritize their patient’s own language and goals around their intersex variations and bodily difference (rather than imposing DSD terminology), should acknowledge that young patient’s goals may ultimately differ from their family’s goals long term through putting off any unnecessary interventions until the patient is old enough to seek them out and give informed consent, and should source patient support information from large-scale internationally recognized intersex organizations (including those for all intersex people such as OII, and local chapters for patients’ specific variations such as TS and AIS societies).
Similarly, research institutions, researchers, and publishers could take a more active share in the responsibility of avoiding the exploitation of people with intersex variations through the health-related studies they publish. This could include standardizing indicator questions for people with congenital intersex variations (so that studies claiming intersex participants must actually include them), and standardizing requirements of evidence of informed consent for any external genitalia photography published or even key problematic intervention practices described within studies published (such as cosmetic genital surgeries). Indeed, the divide between the clinical and the nonclinical literature exposes possibilities for improving not only treatment outcomes but also opportunities for changing the relationship between biomedical expertise and patient- and theory-centered knowledge production. In particular, involving diverse groups of people with intersex variations in research development and knowledge development around biomedical and theoretical knowledge, and in the creation of success measures for treatment evaluations, would be key steps forward. Methods might include (but are not limited to) involving intersex people in study reference groups, focus groups, professional development training sessions, or paid consultants and team members. Where LGBTI work seeks to include intersex people, this should be achieved directly via consultation with intersex groups and active recruitment strategies, to overcome tendencies toward pinkwashing or assuming intersex people are included where they are not (Holmes, 1994; United Nations, 2012). LGBTI work should only include intersex people where their goals align with the work or are actively prioritized in the work, and where an understanding of the particular impacts of homophobia on intersex people can be understood and worked against. A pro-active stance toward aligning the range of perspectives on health care for people with intersex variations needs to be taken by a range of stakeholders (from policy makers to health care providers and publishers) if the tensions are to be resolved in this field—and ultimately used to improve it.
Footnotes
Appendix
All sources, categorized by type and perspective on corrective intervention.

| Source | Country | Theory/lens | Methods | No. of participants with intersex variations | Framing of participants with intersex variations | Health messages cast intervention for people with intersex variations as (unproblematic, problematic, or unclarified/mixed)? |
|---|---|---|---|---|---|---|
| Amarillo et al. (2016) | The United States | Traditional Clinical/Medical | Systematic experimental group testing/modeling—CMA | 52 (age unspecified) | Patients with atypical characteristics or DSD: hosts of atypical chromosomes in need of diagnosis for adrenal anomalies; genital anomalies; chordee; hypospadias or epispadias; micropenis or clitoromegaly; scrotal anomalies; Turner syndrome or stigmata; urethral anomalies; undescended testis; or inguinal gonads. | Unproblematic. |
| Jones (2016) | Australia | Postmodern and Critical Sociology | Sociological online health and education services survey | 272 (aged 16-87 years). | Students with intersex variations: a constructed, marginalized group with service needs and rights to autonomy (over 40 variations included PCOS-related hyperandrogenism). | Problematic. |
| Kelsey et al. (2016) | The United States | Traditional Clinical/Medical | Systematic experimental group testing/modeling—Measuring size and configuration of internal female genitalia via ultrasound (MRI) data from four studies to create norms. | None (only “healthy females” without DSDs aged 0-40). | Patients with DSD: females with uterine volume different to the “healthy females” studied. | Unproblematic. |
| Kalra, Baruah, and Kalra (2016) | India | Liberal Literary Forensic | “Forensic endocrine” textual analysis of intersex case described in episodes of the Mahabharata (ancient Indian epic). | 1 (age unspecified). | Intersex people, who have endocrinology-related features identifiable in historic texts (none were very specifically detailed), and should be treated with empathy. Sikhandini, who exchanged her womanhood with a yaksha and returned as a (not fully accepted) man, read as intersex. | Unclarified/Mixed. |
| Vasundhera, Jyotsna, Kandasamy, and Gupta (2016) | India | Traditional Clinical/Medical | Case reports. All new and old patients of 46XY DSD attending the endocrine OPD in a period of 16 months were subjected to clinical, cytogenetic, hormonal, and radiological evaluation and treatment. | 19 (aged 3 months-49 years). | 46 XY patients with DSD: a wide spectrum of phenotypes ranging from unambiguous female genitalia to ambiguous male genitalia with hypospadias or dysgenetic gonads (complete and partial gonadal dysgenesis, congenital bilateral anorchia, ovotesticular DSD, complete and partial AISs, 5α reductase deficiency, and three indefinite diagnoses). | Unclarified/Mixed. |
| Anonymous (2016) | New Zealand | Critical Intersex Studies | Interview with Craig Waterworth, Massey University. | None (interview with academic). | Intersex infants: people often unfairly subjected to cosmetic surgery in problematic ways. | Problematic. |
| Grimes (2016) | The United States | Critical-Queer Feminist Theology | Uses critical appropriation of Virgilio Elizondo’s theology of La Virgen de Guadalupe and scientific evidence to disrupt religious dogma (e.g., John Paul II’s criteria of femininity). | None (uses the general existence of). | Intersex people: seen as neither essentially male nor female, and as thus disrupting the sex binary (male/female) in traditional Judeo-Christian sex and gender discourse. | Problematic. |
| Brasileiro et al. (2016) | Brazil | Traditional Clinical/Medical | Case report. A patient was referred due to ambiguous genitalia, treatment was applied to remove cosmetic difference. | 1 (aged 3 months). | Patients with DSD: hosts of chromosomal abnormalities. The 46XX infant girl was considered “otherwise healthy.” | Unproblematic. |
| Grimbly, Caluseriu, Metcalfe, Jetha, and Rosolowsky (2016) | Canada | Traditional Clinical/Medical | Case report. Expedient genetic testing for the HSD17B3 gene. | 1 (infant). | Patient with DSD—17β-hydroxysteroid dehydrogenase type 3 (17βHSD3) deficiency, a rare impaired conversion of androstenedione to testosterone: called an otherwise phenotypically female infant presented with bilateral inguinal masses and a 46,XY karyotype. | Unproblematic. |
| Ahmed and Fadl-Elmula (2016) | Sudan | Traditional Clinical/Medical | Case reports. Medical history, physical examination, culturing of lymphocytes, chromosomal analysis, PCR analysis for SRY gene, hormonal profile, pelvic ultrasound, laparoscopic examination, histopathology, and psychological assessment. | 70 (infants under 2 years to adults). | Patients with DSD: described as presenting in several forms, e.g., male and female pseudohermaphroditism, gonadal dysgenesis, and true hermaphroditism. (The patients received the diagnoses: male pseudohermaphrodites, testicular feminization syndrome, complete gonadal dysgenesis, female pseudohermaphrodites, true hermaphrodites, Smith–Lemli–Opitz syndrome, Down syndrome, or “controversial”). | Unproblematic. |
| Dong et al. (2016) | China | Traditional Clinical/Medical | Systematic experimental group testing/modeling—Targeted NGS to diagnose genetically heterogeneous disorders (or “causative mutations” for DSDs). | 21 (ages unspecified). | Patients with DSD: seen as having “causative mutations” to be discovered by genetic analyses. They were classified in a table according to whether their external genitalia looked male or female, whether or not they had gonads and other anatomy (e.g., uterus). | Unproblematic. |
| Dwyer, Ball, and Barker (2015) | Australia | Critical LGBTI Liberationist | The article highlights examples from three research projects that explored rurality and LGBTIQ young people’s interactions with police; LGBTIQ people’s interactions with police liaison services; and LGBTIQ-identifying police officers. | Unclear how many (if any). | Amalgamated within the LGBTIQ umbrella of marginalized people with human right not to be discriminated against. | Unclarified/Mixed. |
| Camats et al. (2015) | Spain | Traditional Clinical/Medical | Systematic experimental group testing/modeling—Comparative cell tests and Western blots (tissue, protein, enzyme and cell analysis). | 108 (ages undefined). | 46,XY patients with DSD: compared in the paper to “normal individuals.” Discussed traits including, for example, small penis, hypospadias, hypogonadism, clitoromegaly, etc. | Unclarified/Mixed. |
| Dreger (2015) | The United States | Queer Historiography | Reflection on others and her own studies on the medical treatment of intersex children. | None (secondary analyses of some of her own studies and their social and medical responses). | Intersex children and people as objects of medical and research science: sometimes constructed as having a DSD in self-fulfilling treatment approaches. | Problematic. |
| Topcu et al. (2015) | The United States | Traditional Clinical/Medical | Systematic experimental group testing/modeling—Investigation of androgen receptor gene mutations, sequence analysis, etc. | 21 (aged 6 days-14 years). | Patients with 46,XY DSD: in need of genetic analysis. | Unclarified/Mixed. |
| Palanisamy et al. (2015) | India | Traditional Clinical/Medical | Case report (analysis and intervention). | 1 (aged 38 years). | Patient with PMDS: cast as a rare intersex disorder “caused by defective anti-mullerian hormone or its receptor, characterized by undescended testes with presence of underdeveloped derivatives of mullerian duct in genetically male infant or adult with normal external genitals and virilisation” (abstract). | Unproblematic. |
| Tinney et al. (2015) | Australia | Critical LGBTI Liberationist | Literature review. | None (uses the general existence of). | Intersex people are included within the LGBTI acronym, however, they are seen as the group for which mental health information for older people is most minimal. | Unclarified/Mixed. |
| Rubin (2015) | The United States | Transnational Feminist | Examines the Intersex Society of North America’s (a 1993-2008 group), attempt to cast normalizing surgery within the United States 1997 ban on “female genital mutilation”; and Colombian court limits of surgeries. | None (uses the history of a specific intersex advocacy group). | “Intersex” is an umbrella term for individuals born with sexual anatomies that various societies deem to be nonstandard. | Unclarified/Mixed. |
| Achermann, Domenice, Bachega, Nishi, and Mendonca (2015) | The United Kingdom | Liberal Constructivist | Review of advances in molecular biological techniques for diagnosing DSDs. | None (secondary analyses). | DSDs: as a diverse group of conditions that can be challenging to diagnose accurately using standard phenotypic and biochemical approaches. Organized into “Sex chromosome DSDs,” “46,XY DSDs,” and “46,XX DSDs.” | Unproblematic. |
| Howard (2015) | The United States | Critical LGBTI Liberationist | Photographic essay documentation of public change and continuity in Rankin County’s LGBTI citizens. | Unclear how many (if any). | Part of the LGBTI group umbrella with a marginalized and tenuous political standing. | Unclarified/Mixed. |
| Anderson (2015) | The United States | Critical Intersex Studies | Historic overview and critical analysis of treatment recommendations for individuals with DSD since the 1950s. | None (secondary sources). | Disorders of “sexual differentiation”: a number of genetically influenced congenital anomalies of the genitalia for which the previous standard of care has included emergent sex assignment and early genitoplasty and gonadectomy. | Problematic. |
| von Klan (2015) | The United States | Bioethical Narrative Inquiry | Autobiographical critical analysis of author’s intervention impacts. | 1 (autobiographical). | Intersex as a marginalized group, Swyer Syndrome focus. | Problematic. |
| Simon (2015) | The United States | Bioethical Narrative Inquiry | Autobiographical critical analysis of author’s intervention impacts. | 1 (autobiographical). | Intersex as a marginalized group, mixed gonadal dysgenesis focus. | Problematic. |
| Cynthia (2015) | The United States | Bioethical Narrative Inquiry | Autobiographical critical analysis of author’s intervention impacts. | 1 (autobiographical). | Intersex as a marginalized group, ambiguous genitalia focus. | Problematic. |
| Frader (2015) | The United States | Bioethical Narrative Inquiry | Autobiographical critical analysis of author’s observation and view. | None (uses general experience). | Individuals with intersex conditions: a group who have experienced considerable abuse at the hands of medical personal. | Problematic. |
| Baratz and Karkazis (2015) | The United States | Bioethical Narrative Inquiry | Autobiographical critical analysis of author’s observation and view. | None (secondary sources and some experience). | Intersex people as telling stories of painful health care since the 1990s: constituting negative long-term evaluative feedback to clinicians. | Problematic. |
| Zieselman (2015) | The United States | Bioethical Narrative Inquiry | Autobiographical critical analysis of author’s observation and view. | 1 (48 years, autobiographical). | Intersex as a marginalized group, AIS focus, also uses the term “Difference” of Sex Development. | Problematic. |
| Walsh (2015) | The United States | Bioethical Narrative Inquiry | Autobiographical critical analysis of author’s observation and view. | 1 (57 years, autobiographical). | Intersex as a marginalized group, CAIS focus. | Problematic. |
| Wall (2015) | The United States | Bioethical Narrative Inquiry | Autobiographical critical analysis of author’s observation and view. | 1 (38 years, autobiographical). | Intersex and Black people as each a marginalized group with nonnormative and thus punished bodies through incarceration/execution vs. corrective intervention, AIS focus. | Problematic. |
| Viloria (2015) | The United States | Bioethical Narrative Inquiry | Autobiographical critical analysis of author’s intervention impacts. | 1 (autobiographical). | Intersex as a marginalized group, ambiguous genitalia/clitoromegaly focus: sees group as at risk of unwanted IGM and hormonal therapies. | Problematic. |
| Truffer (2015) | The United States | Bioethical Narrative Inquiry | Autobiographical critical analysis of author’s intervention impacts. | 1 (50 years, autobiographical). | Intersex as a marginalized group, multiple diagnoses (alternately ambiguous genitalia/CAH/hypospadias, and differing sex allocations over time) focus. | Problematic. |
| Quinn (2015) | The United States | Bioethical Narrative Inquiry | Autobiographical critical analysis of author’s intervention impacts. | 1 (25 years, autobiographical). | Intersex as a marginalized group subject to assumed need for correction, CAIS focus. | Problematic. |
| Petersen (2015) | The United States | Bioethical Narrative Inquiry | Autobiographical critical analysis of author’s intervention impacts. | 1 (63 years, autobiographical) | Intersex as a marginalized group subject to assumed need for correction, androgen “excess” focus. | Problematic. |
| Pagonis (2015) | The United States | Bioethical Narrative Inquiry | Autobiographical critical analysis of author’s intervention impacts. | 1 (autobiographical). | Intersex as a marginalized group, clitoromegaly focus. | Problematic. |
| Long (2015) | The United States | Bioethical Narrative Inquiry | Autobiographical critical analysis of author’s intervention impacts. | 1 (52 years, autobiographical). | Intersex as a marginalized group, multiple diagnoses (growth hormone deficiency, hypothyroidism, panhypopituitarism, hypoadrenalism, hypogonadism, gynecomastia) focus. | Problematic. |
| Amanda (2015) | The United States | Bioethical Narrative Inquiry | Autobiographical critical analysis of author’s intervention impacts. | 1 (autobiographical). | Intersex as a marginalized group, AIS/clitoromegaly focus. | Problematic. |
| Inter (2015) | The United States | Bioethical Narrative Inquiry | Autobiographical critical analysis of author’s intervention impacts. | 1 (aged approximately 30s+, autobiographical). | Intersex as a marginalized group, CAH focus. | Problematic. |
| Garcia (2015) | The United States | Bioethical Narrative Inquiry | Autobiographical critical analysis of author’s intervention impacts. | 1 (aged approximately 50s+, autobiographical). | Intersex as a marginalized group, internal genitalia focus. | Problematic. |
| Davis (2015) | The United States | Bioethical Narrative Inquiry | Autobiographical critical analysis of author’s observation and view. | 1 (aged approximately 50s+, autobiographical). | Intersex as a marginalized group, with largely unheard stories. | Problematic. |
| Grover, French, and Yazdani (2015) | The United States | Traditional Clinical/Medical | Case report (anatomical analysis and intervention). | 1 (aged 5 years). | Disorder of sexual “differentiation” (DSD): compared 45Xmale experiences to Turner’s Syndrome. | Unclarified/Mixed. |
| Oliveira, de Paiva-e-Silva, Guerra-Junior, and Maciel-Guerra (2015) | Brazil | Liberal/Constructivist | Interviews with 30 parents on how health workers disclosed their child’s DSD diagnoses. | None (parents only). | Children with ambiguous genitalia/DSD as a source of “shock and societal stigma” for parents. | Unclarified/Mixed. |
| Khadilkar et al. (2015) | India | Traditional Clinical/Medical | Case reports. Records on the clinical, biochemical, imaging, cytogenetic, surgical, and histopathologic findings and outcomes. | 7 (aged 2 months-25 years). | Patients with OT DSD: as needing interventions from early years according to parents’ choice in sex assignment. | Unproblematic. |
| Ediati et al. (2015) | Indonesia | Traditional Clinical/Medical | Clinical and psychological assessments and interviews. | 118 (age unspecified). | DSD, including ambiguous genitalia, begins at diagnosis soon after birth. | Unproblematic. |
| Kraus (2015) | The United States | Critical Intersex Studies | Textual analysis of how different terms provided for intersex/DSD in the DSM historically and conceptually. | None (textual classifications only). | Challenges use of “Disorders of Sex Development” (DSD), as a specifier of GD. | Problematic. |
| Gül, Sayar, Özten, and Eryilmaz (2015) | Turkey | Phenomenology | Case report of patient’s DSD, psychotic symptoms, and bipolar affective disorder delusions. | 1 (aged 35 years). | Patient with DSD: described as “abnormal development of the external and internal genital organs and male pseudohermaphrodite-type” (17-hydroxylase deficiency) that “creates problem in determination of gender” (abstract). | Unclarified/Mixed. |
| Paula et al. (2015) | Brazil | Traditional Clinical/Medical | Case report (anatomical analysis and intervention). | 1 (aged 2 months) | Patient with OT DSD with “unusual karyotype” (46,XX/47,XXY/48,XXYY). | Unproblematic. |
| Miller (2015) | The United States | Queer | Argues the need for a Queer literacy framework to be taught in schools. | None (uses the general existence of). | Part of the LGBT*IAGCQ group umbrella with a marginalized and tenuous political standing. | Problematic. |
| Mohamed and Noor (2015) | Malaysia | Maqasid al-Shari’ah: Islamic views on health care | Mechanistic interpretation of Qur’an and Hadith toward Islamic bioethical deliberation on the issue of SAS. | None (uses the general existence of). | Patients with DSD or intersexed infants: cast as being a primarily Islamic subject/object before being a medical one. | Unclarified/Mixed. |
| Kim et al. (2015) | Germany (and the United Kingdom, the United States, Ireland, Italy). | Traditional Clinical/Medical | Systematic experimental group testing/modeling—CNV analysis and genetic tests (cell transfection and transgenic experiments). | Unclear how many (3 cases, four families). | Patients with DSD as having familial genetic links/determinations. | UnclarifiedMixed. |
| Lalor (2015) | The United Kingdom | Poststructural Feminist Legal Studies | Analysis of iterations of LGBTI rights are limited by the binary of homosexual/heterosexual. | None (uses the general existence of). | Part of the LGBTI group umbrella with a marginalized and tenuous political standing. | Problematic. |
| Saraswat, Weinand, and Safer (2015) | The United States | Liberal Constructivist | Literature review. | None (secondary sources). | Patients with DSDs, also “differences” of sex development. | Problematic. |
| Rios et al. (2015) | Mexico | Traditional Clinical/Medical | Systematic experimental group testing/modeling—Examined and modeled gene networks directly associated with the process of sex differentiation (toward sertoli and granulosa cells). | Unclear how many. | Patients with DSD; as subject to gene expressions. | Unclarified/Mixed. |
| Ekenze et al. (2015) | Nigeria | Traditional Clinical/Medical | Case reports (anatomical analysis and intervention). | 39 (aged 2 months-14 years). | Patients with DSD (including 46, XX DSD, 46, XY DSD 16, Ovotesticular DSD); as requiring interventions. | Unproblematic. |
| Mutlu et al. (2015) | Turkey | Traditional Clinical/Medical | Case report (anatomical analysis and intervention). | 1 (aged 15). | Patients with DSD (Swyer syndrome); as requiring interventions and being at risk of cancer. | Unproblematic. |
| Lin-Su, Lekarev, Poppas, and Vogiatzi (2015) | The United States | Liberal Constructivist | Survey on patient views regarding DSD nomenclature, sent via email to eligible subjects with a short introduction explaining DSD. | 128 (of 589 CAH patients or family members). | Patients with CAH only. | Unclarified/Mixed. |
| Lucas-Herald et al. (2015) | Scotland | Traditional Clinical/Medical | Systematic experimental group testing/modeling—Urinary steroid metabolite ratios, with comparisons to control group samples. | 93 (aged 1 day-18 years, compared to 252 children without endocrine concerns). | Children with suspected disorders of steroid/hormone synthesis (including 11β-hydroxylase deficiency, steroid hormone disorder, 21-hydroxylase deficiency, and 5α-reductase deficiency), cast as genetic abnormality. | Unproblematic. |
| Ceci, Calleja, Said, and Gatt (2015) | Malta | Traditional Clinical/Medical | Case report (anatomical/genetic analysis). | 1 (aged 22 years). | Patient with disorders of sexual “differentiation” (DSD), including “true hermaphroditism”/genital ambiguity. | Unproblematic. |
| Latrech, Skikar, Mohammed El Hassan Chraïbi, and Gaouzi (2015) | Morocco | Traditional Clinical/Medical | Case reports (anatomical/genetic analysis). | 2 (aged 1 month-3 years). | Patients with DSD (47XYY); as potentially experiencing co-morbid “disorder” or impacts. | Unproblematic. |
| Mannaerts, Muys, Blaumeiser, and Jacquemyn (2015) | Belgium | Traditional Clinical/Medical | Case report (anatomical/genetic analysis and intervention). | 1 (aged 18 years). | Patients with DSD, as (only) conditions where sexual phenotype and genotype are discordant (hypergonadotropic hypogonadism case focus). | Unproblematic. |
| Bonanni, Pasetti, Ghiggeri, and Gandolfo (2015) | Italy | Traditional Clinical/Medical | Case report (analysis and intervention). | 1 (aged 6 years). | Patients with Turner Syndrome, as having medical comorbidities that may be treated. | Unproblematic. |
| Wang and Tian (2015) | China | Liberal Constructivist | Questionnaire with four domain quality of life measures scored: physical, psychological, social, and environmental. | 87 (aged 13-38 years). | Patients With DSD (including Turner’s syndrome, Noonan syndrome, AIS, testicular regression syndrome, CAH, and pure gonadal dysgenesis) deserve quality of life. | Unproblematic. |
Note. AIS = Androgen Insensitivity Syndrome; CAIS = Complete Androgen Insensitivity Syndrome; CMA = chromosome microarray analysis; CNV = Copy Number Variation; DSD = disorders of sex development; DSM = Diagnostic and Statistical Manual of Mental Disorders; GD = Gender Dysphoria; IGM = Intersex Genital Mutilation; LGBTI = lesbian, gay, bisexual, transgender, and intersex; LGBTIQ = lesbian, gay, bisexual, transgender, intersex, and questioning; MRI = magnetic resonance imaging; NGS = next-generation sequencing; OPD = outpatient department; OT DSD = ovotesticular disorder of sex development; PCOS = polycystic ovarian syndrome; PCR = polymerase chain reaction; PMDS = persistent mullerian duct syndrome; SAS = sex assignment surgery.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author is currently funded by an Australian Research Council Discovery Early Career Researcher Award.