
Abstract
The 2011 Australian federal budget included a large investment in youth mental health and early intervention services. In this article, we focus on the critical role of agenda setting in the preceding 4 years to examine how and why these services were given such a high priority at this time. We undertook a systematic review of relevant literature, including parliamentary Hansard transcripts from the House of Representatives and Senate, the final reports of all available parliamentary committees, government policy documents, other pertinent documents held by the Commonwealth Department of Health and Aging, and media reports from five widely circulated Australian publications/news outlets. We used Kingdon’s multiple streams framework to structure analysis. We highlight three factors that were influential in getting youth mental health issues onto the policy agenda: (a) the strategic use of quantitative evidence to create a publicly visible “problem,” (b) the marshalling of the “public” to create pressure on government, and (c) the role of serendipity. Overall, we found the decision to prioritize youth mental health resulted from a combination of advocacy for a well-articulated policy solution by high-profile, influential policy entrepreneurs, and political pressure caused by an up swell of national support for mental health reform. Our findings highlight the socio-political factors that influence agenda setting and health policy formulation. They raise important ethical and strategic issues in utilizing research evidence to change policy.
Keywords
Background
On May 10, 2011, the Australian government announced new funding commitments of A$419.7 million for two major youth mental health programs: Early Psychosis Prevention and Intervention Centres (EPPIC) and Headspace. EPPIC is an integrated mental health service aimed at youth aged 15 to 24 years with a first episode of psychosis. Headspace comprises one-stop early treatment centers aimed at improving youth mental health and providing drug and alcohol, employment, and other integrated social services (Commonwealth of Australia, 2011; Headspace, 2011; Muir et al., 2009; Russell, 2011). These reforms were promoted as “the centerpiece” of the federal Labor government’s mental health commitments by the then Prime Minister Julia Gillard (Australian Associated Press, 2011b). In this article, we examine the events leading up to the 2011 budget to identify the reasons why early intervention services for youth were adopted. Our aim is to increase the awareness of both mental health policy makers and researchers of the socio-political dynamics that affect the uptake of research findings by governments.
Conceptual Framework
John Kingdon’s (2003) multiple streams framework provides one way of understanding how and why early intervention mental health services for youth rose to the top of a crowded health policy agenda. This approach to understanding the agenda-setting phase of the policy process has been used extensively in the analysis of health and social policy (Battams & Baum, 2010; Craig, Felix, Walker, & Phillips, 2010; Guldbrandsson & Fossum, 2009; Kruger, 2001; Lancaster, Ritter, & Colebatch, 2014; Laraway & Jennings, 2002; Lenton, 2008; Sharma, 2008).
Kingdon (2003) conceptualized the agenda-setting phase of the policy process as comprising three streams: problems, policies, and politics (see Figure 1). Each stream contains its own processes and actors and operates independently of the others according to its own set of rules and dynamics. Kingdon argued that, at certain times, the actions of advocates, or policy entrepreneurs, can lead to the coupling of these three streams to open a “policy window” that leads to action in the form of policy change (Craig et al., 2010; Felix, 2007; Kingdon, 2003). More recent iterations of the multiple streams approach have relaxed the condition that the streams are independent and argued that this approach is best viewed as a conceptual device to help the analyst identify the elements that contribute to policy “rationality” (Zahariadis, 1999). A summary of key concepts that underpin a multiple streams analysis is outlined below.

The Kingdon multiple streams model.
Problems
The problem stream encapsulates any problems that could come to hold decision makers’ attention. At any one time, there are many potential problems that decision makers could address but, for a small subset of these, there will be a growing belief that something can and should be done. Possible reasons for the ascendency of such a belief include a focusing event such as a crisis or disaster, publication of numeric or other indicators that suggest a worsening of the problem, or feedback that an existing policy or program is not working (Kingdon, 2003).
Policy Solutions
Kingdon conceptualizes potential policy proposals or “solutions” as undergoing development, recombination, discussion, and debate within a policy community comprising a usually small group of influential people inside and outside of government. This process yields a limited number of technically feasible, and/or affordable policy contenders. These need to be frequently advocated and discussed within the policy community if they are to gain traction. Kingdon argues that consensus on a policy contender can facilitate its diffusion. Furthermore, he suggests that a “problem” is more likely to rise to the top of the policy agenda if a well-defined, widely accepted policy solution is known to exist (Kingdon, 2003, p. 117).
Political Context
The political stream is an entity that comprises elements such as: public mood, pressure group campaigns, election results/changes of government, and ideological divides within and between the major political parties. For a policy solution to be seriously considered, it must be politically palatable for the government of the day.
Policy Entrepreneurs
Policy entrepreneurs are individuals who invest time and resources in seizing opportunities where change is more likely and push for their particular policy solution to a perceived problem in the political sphere. Policy entrepreneurs are important actors in coupling a problem with a policy solution so as to facilitate its political adoption that results in policy change.
Policy Windows
Policy windows are the final major element of Kingdon’s framework. They are defined as opportunities that make decisions and action more likely. Policy windows can open expectedly (with a change in government and federal budgets) or unexpectedly (as a result of a pressing problem or disaster, or by a shift in national mood that makes government action seem imperative; Kingdon, 2003). Windows are often open for a short period of time, so policy entrepreneurs must be ready with their problem well-defined and framed, an acceptable policy solution to that problem and have political support for the solution. An opportunity may quickly pass if it is not seized.
Method
Data Collection
Our analysis is based on a two-stage literature review of key texts in the public domain. First, relevant documents were collected from the following sources: (a) transcripts of parliamentary proceedings (recorded in Hansard) from the Australian House of Representatives and Senate, (b) the final reports of all available Australian government parliamentary committees, (c) Australian government policy documents, and (d) other pertinent documents held by the Commonwealth Department of Health. We also reviewed media reports from five widely circulated Australian publications/news outlets: The Australian, the Sydney Morning Herald, The Age, The Canberra Times, and Australia’s ABC network.
Parliamentary records were searched for the period May 10, 2010, to June 10, 2011. This included 1-year prior and 1 month post 2011 budget. This date range was set both for pragmatic reasons, because of the large amount of data that were collected and to isolate the political debate relating specifically to the 2011 budget. Other sources (media articles, government documents, and the final reports of parliamentary committees) were examined across a wider period (January 1, 2008-June 10, 2011) to capture longer term trends.
Texts were included in our study if they explicitly mentioned “youth mental health services,” Headspace or EPPIC, or “early intervention services.” While early intervention for mental health is applicable across the lifespan, in this particular context, “early intervention” was often used in conjunction with youth mental health. Prominent or repeated mentions of media coverage and constituent concerns by politicians in Hansard were also identified and the articles retrieved.
The second stage of review involved a search of academic literature to refine findings drawn from primary sources and provide context. Electronic databases searched included MEDLINE, PsycINFO and Embase (searched via Ovid), Australian Public Affairs Full Text (APAFT), Humanities and Social Sciences Collection, TV News Archive, Rural and Remote Health Database, Australasian Medical Index (AMI), Australian Public Affairs Information Service-Health (APAIS-Health), Health Issues in Criminal Justice (CINCH-Health), Health and Society Database, Health Collection, and Media Scan (via Informit).
Using this search strategy, we identified 143 Hansard transcripts, 110 media articles, 11 non–peer-reviewed publications (grey literature), and 20 peer-reviewed journal articles relevant to Australian youth mental health policy over the period of interest.
Data Analysis
For the first step of analysis, we carried out a content analysis of Hansard to provide a rough proxy measure of changes in the importance of youth mental health on the political agenda from 2007 to 2012. Mentions of the following key words, mental health, youth mental health, headspace, and EPPIC, were counted over the 4-year period and for the year prior and afterward.
For the second stage of analysis, a deductive approach was employed, using Kingdon’s multiple streams framework (Kingdon, 2003) as a means to operationalize/code data. This approach was partly guided by the pragmatic need to sort large volumes of data, which rendered an inductive, grounded-theory approach (Strauss & Corbin, 1990) infeasible (J. Smith, Bekker, & Cheater, 2011).
All documents identified in the first and second stages of the review process were reviewed and their contents categorized in an Excel® spreadsheet template according to whether they related to (a) policy problems, (b) policy solutions, and/or (c) political issues, based on Kingdon’s framework, as defined above. “Problem” representations were further categorized as indicators, feedback, or focusing events (Kingdon, 2003).
Using this method, the major problems, policy solutions, and political events between January 2008 and the end of May 2011, relating to youth mental health, were identified and described. Finally, we drew conclusions about cause and effect relationships between different spheres of influence (i.e., different “streams”).
Results
Change Over Time in Mention of (Youth) Mental Health in Hansard
Mentions of mental health rose sharply in Hansard documents in 2010 and 2011. Youth-specific terms such as “youth mental health,” “EPPIC,” and “Headspace” also increased over the time in the lead up to the funding announcement in 2010-2011 (Figure 2).

Mental health key words in Senate and House of Presentatives Hansard titles and content 2007-2012.
Problems, Policy Solutions and Political Context in Youth Mental Health
Key themes were found in all data sources relating to problems, policy solutions and political issues relevant to youth mental health, the role of policy entrepreneurs and the character of the policy window. These are described below and summarized in Table 1.
Summary of the Elements in the Case Study Conforming to Kingdon’s Multiple Streams Framework.
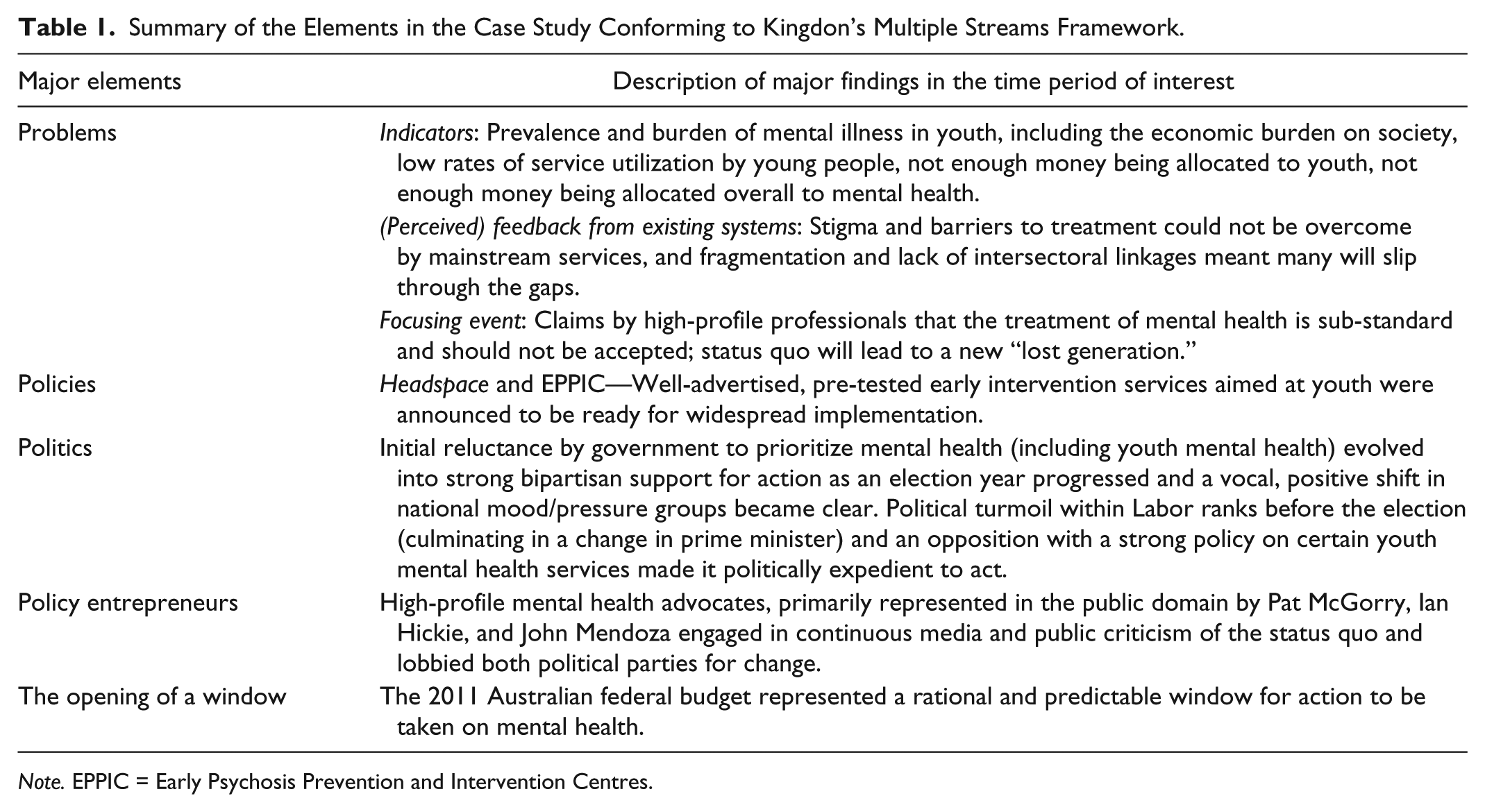
Note. EPPIC = Early Psychosis Prevention and Intervention Centres.
The Problem Stream
There were two ways in which the problem of youth mental health was constructed in public and policy spheres: Indicators that quantified the extent and burden of youth mental health were used to highlight the seriousness of the issue while evidence to suggest that youth were underserved by existing mental health services promoted the need for specialized youth mental health services. Although there was no single focusing event to spur action, advocates and the media used statistical data to quantify the burden of youth mental health and suicide and highlight the crisis of youth mental health. However, there were constraints on how government could act: natural disasters in 2010-2011 left a substantial “clean-up” bill, and at the same time, the Labor government was under sustained pressure from the Liberal dominated coalition, in opposition, over its financial management.
Use of indicators
Hansard transcripts of speeches often included data on the population prevalence of mental disorders in youth (Commonwealth of Australia: House of Representatives, 2010). For example, Hansard excerpts that framed mental health and suicide as a problem of youth included phrases like: “half of the Australians aged between 12 and 25 will experience a diagnosable episode of mental illness” (Commonwealth of Australia: House of Representatives, 2011, p. 2009), and “[suicide is] a leading cause of deaths under 44” (Commonwealth of Australia: House of Representatives, 2010, p. 6346).
Media stories also focused on the burden of youth mental illness reporting statistics that “75 percent of mental health problems will appear by age 25” (“A Man on a Timely Mission,” 2010) and “one in three young Australians will experience mental illness by their 25th birthday” (Australian Associated Press, 2008). In addition, the media emphasized the high level of youth need for mental health services (Jones, 2010; Marcus, 2008; McGorry, 2011a; Stark, 2008).
Indicators of persistently low levels of mental health service utilization among young people were reported in the 2009 release of findings from the 2007 National Mental Health and Wellbeing Survey (Slade, Johnston, Browne, Andrews, & Whiteford, 2009). This issue was identified as a major concern in Senate enquiries in 2008 (The Senate Standing Committee on Community Affairs, 2008) and 2010 (The Senate Finance and Public Administration References Committee, 2010). It also featured in parliamentary debate (Commonwealth of Australia: House of Representatives, 2011) and numerous academic articles (Boyd, Hayes, Wilson, & Bearsley-Smith, 2008; Burgess et al., 2009; “Youth Initiatives: Headspace—National Youth Mental Health Foundation,” 2008).
Economic losses from untreated mental illness, in general, were also highlighted in parliamentary debate, the academic literature, and the media. The cost to the economy of untreated mental illness was estimated at A$30 billion in lost productivity and lost lives. Mental illness was identified as a major contributor to unemployment and to long-term receipt of welfare (Australian Associated Press, 2008; Butterworth, Burgess, & Whiteford, 2011; Commonwealth of Australia: House of Representatives, 2010; Commonwealth of Australia: Senate, 2010; Leach & Butterworth, 2012; McGorry, 2010a; Waghorn, Chant, Lloyd, & Harris, 2011). At the same time, the federal Labor government was under pressure to return the budget to surplus following the 2008 global financial crisis (Commonwealth of Australia: House of Representatives, 2010) so parliamentary debate focused on increasing youth participation in employment or training and education by investing in mental health services (Commonwealth of Australia: House of Representatives, 2010).
Feedback from existing programs
In parliamentary debates (Commonwealth of Australia: House of Representatives, 2010) and the media (Australian Associated Press, 2008), mainstream mental health services were described as inappropriate for youth with emerging mental health problems. Among the explanations offered for this situation were that parents and mainstream mental health professionals often mistook youth mental illness for a normal part of adolescence (Commonwealth of Australia: House of Representatives, 2010; Stark, 2008), that overworked mainstream health care professionals were not equipped to deal with youth problems (Commonwealth of Australia: House of Representatives, 2011) and that negative first experiences of seeking help discouraged further efforts to obtain assistance (Cohen, Medlow, Kelk, & Hickie, 2009). Parliamentarians identified the following major barriers to adequate services for young mental health consumers: fragmentation of the mental health sector, lack of collaboration and co-ordination, and poor intersectoral linkages (Commonwealth of Australia: House of Representatives, 2011).
The research literature identified multiple reasons why young people did not seek help for their mental health. These included poor mental health literacy among young people, stigma, lack of awareness of the services available, lack of youth-focused information on mental health and drug education programs, and consumers not believing they needed help or not believing that they would benefit from professional help (Cohen et al., 2009; Collin et al., 2011; Hampshire & Di Nicola, 2011; Harris, Burgess, Pirkis, Slade, & Whiteford, 2011; Henderson, Andrews, & Hall, 2009; McCann & Lubman, 2012; Whiteford & Groves, 2009).
By contrast, parliamentarians identified the barriers to youth help seeking as primarily geographical (e.g., lack of access in rural and regional areas), financial (e.g., ability to pay for services), and social (e.g., stigma of being labeled mentally ill; Commonwealth of Australia: House of Representatives, 2011). Parliamentarians agreed that these barriers to youth access could not be overcome using existing mainstream health services (Commonwealth of Australia: Senate, 2010). A 2008 Senate enquiry on mental health services found that much of the 2006 Council of Australian Governnments (COAG) National Action Plan funding had been provided to generic services. It recommended a greater focus on meeting the mental health care needs of specific groups, especially youth (The Senate Standing Committee on Community Affairs, 2008).
Focusing events and crises
There was no one crisis or event, such as a mass shooting or high-profile suicide, which focused attention on mental health during this time period, as had stimulated earlier mental health reform initiatives (Whiteford, 2014; Meurk, Whiteford, Head, Hall, & Carah, 2015); although there was a suicide “spike” in a major regional center (Mackay, Queensland) reported in national television media on Four Corners (McDermott, 2010) and mentioned repeatedly in parliament as an example of the problem (Commonwealth of Australia: House of Representatives, 2010, p. 1864; Commonwealth of Australia: House of Representatives, 2011, p. 119, p. 1316, p. 3008). Rather, the main issues highlighted by mental health advocates to construct a visible “crisis” in the public domain were statistics on the burden of mental illness, poor service utilization by young people and overall suicide rates. They argued through the media that there was a moral imperative for government to urgently act on youth mental health to prevent a generation being lost to chronic illness or premature death.
Advocates argued that mental health suffered from a social neglect that would be unacceptable in treatment of physical conditions (Australian Associated Press, 2010a; Hickie, 2010; McGorry, 2010c). For example, Professor Pat McGorry was quoted as saying,
Failure to invest in early psychosis reform will result in another lost generation of young Australians consigned to unnecessary disability as well as premature death from suicide and cardiovascular disease (Medew, 2010).
Media claims were repeated in parliamentary debates and focused political and public attention on the tragedy of youth mental illness and suicide (Commonwealth of Australia: House of Representatives, 2010; Commonwealth of Australia: House of Representatives, 2011).
Competing “problems”
Governments often find it difficult to prioritize spending on programs, such as early intervention and preventative programs, where the benefits are arguably long-term while the costs are immediate (Head & Redmond, 2011). The Labor government faced a number of political and financial constraints on their capacity to invest in youth mental health. These included large clean-up bills after unprecedented natural disasters along much of Australia’s east coast in late 2010 and early 2011. In addition, they were subject to persistent criticism from the Opposition over wasteful spending and demands that they honor their election commitment to return the budget to surplus by 2012-2013 (Commonwealth of Australia: Senate, 2011).
The Policy Solutions Stream
Headspace and EPPIC were the primary policy solutions advanced to address the youth mental health “problem.” Advocates argued that these programs were effective, had evidence of prior success, and were ready to be scaled up to meet needs. The option of taking no action (by either investing in other mental health services or not investing in mental health at all) and proposals to mainstream youth care were not advocated. The proposed “one-stop” policy solutions (Headspace and EPPIC) were clearly defined and conceptually simple. They also had the advantage of having been pre-tested in a small-scale pilot study domestically and on a larger scale, internationally. Headspace had received some funding in 2006 and by 2008 had 30 centers operating. EPPIC had been operating in Australia since 1992 but on a geographically limited scale. Similar models of care had, however, been adopted in other countries, most notably in the United Kingdom, where there had been significant investment in early intervention services for psychoses (Joseph & Birchwood, 2005).
Headspace and EPPIC also had high-profile policy advocates lobbying politicians and policy makers. These included: Ian Hickie, a founder and later director of Headspace; Pat McGorry, Executive Director of Orygen Youth Health, the mental health organization that developed and ran EPPIC, and a director of Headspace; and John Mendoza, CEO of what was then the Mental Health Council of Australia, the peak mental health advisory body to the federal government. Their proposed policy options received endorsement in the media and parliament as a “solution” to youth mental illness (Australian Associated Press, 2010b; Medew, 2010; Robotham, 2009; Schmidt, 2009). They were promoted as part of a “collaborative continuum of care” (Commonwealth of Australia: House of Representatives, 2010, p. 980) that was better able to meet the needs of young people than existing overburdened mainstream services that prioritized care for people with severe and chronic mental illnesses (McGorry, 2011b; Muir, Powell, & McDermott, 2012).
The Political Stream
The political context in the 4 years preceding the 2011 budget was characterized by the political upheaval of replacing a first-term Labor Prime Minister in June 2010 followed by a closely fought election that produced a minority Labor government in August 2010. The 2007 federal Labor election victory had raised expectations that youth mental health would be part of the new government’s “revolutionary” national health reforms (Commonwealth of Australia: Senate, 2010, p. 4210; Crosbie, 2009; Office of the Prime Minister & Minister for Health and Ageing, 2010). These hopes were dashed when the 2009 and 2010 budgets provided little new funding commitments to mental health (Metherell, 2010).
Transcripts of parliamentary debate around this time reveal that politicians were conscious of the growing public criticism about the lack of funding for mental health in the national health reforms (Commonwealth of Australia: House of Representatives, 2010; Commonwealth of Australia: Senate, 2010). The media initially reported that government action was pending, for example, “[that Headspace would] be well positioned to make the most of our health reform decisions” (Jenkins, 2009). However, later media comments by the then health minister after the 2010 federal budget suggested that mental health reform would occur as part of national health reform at an unspecified future date (B. Smith, 2010).
Politicians acknowledged increasing criticism that the overall level of funding to mental health was low compared with physical health, with mental health labeled a “poor relation” (Commonwealth of Australia: House of Representatives, 2010, p. 1495).
The resignation of Prime Minister Kevin Rudd and his replacement by Deputy Prime Minister Julia Gillard on the June 24, 2010, overshadowed the delivery on the same day of a letter signed by over 60 of the nation’s peak mental health organizations, demanding that greater attention be paid to mental health in the wider health care reforms. However, the sustained high media profile achieved by mental health advocates, combined with the unflattering media comparisons of the Labor and previous Liberal Government’s records on mental health, positioned mental health as an issue to which the new Gillard-led government needed to respond.
The Labor government was being criticized by the opposition who strongly advocated for mental health investment, including in youth services, both before the August 2010 election, and after their narrow election loss. Coalition advocacy often focused on their collaboration with leading mental health experts and the previous Coalition Government’s decision to start funding early intervention services in 2006 (Commonwealth of Australia: House of Representatives, 2010; 2011). Both sides of politics used their alleged support for mental health to promote their own records and attack that of their opponents, increasing mental health’s position on the national policy agenda (see, for example, Commonwealth of Australia: House of Representatives, 2010).
Policy entrepreneurs worked with the opposition to develop an alternative, mental health election “Action Plan” of A$1.5 billion, which placed a special emphasis on early intervention (Liberal Party of Australia, 2010). This commitment far exceeded the Government’s July 2010 election promise of A$277 million and placed pressure upon the Government to match the opposition promise. The result was a significant election promise from Labor to make mental health a second-term priority (Commonwealth of Australia: House of Representatives, 2010; Grattan, 2010). One of Prime Minister Gillard’s early decisions after the resignation of Mr. Rudd was to appoint an inaugural federal minister for mental health in September 2010 to give greater policy attention to the area than her predecessor had done. In the wake of the federal election, increased resources for mental health was seen as a “political imperative” (Drape, 2010), and the new minority Labor government was under significant pressure to fund new services (Commonwealth of Australia: House of Representatives, 2010, p. 1614, p. 1499).
Policy Entrepreneurs and the Opening of the Policy Window
There was a growing recognition that the mental health sector needed high-profile champions to gain political support, especially after the low allocations to mental health in the 2009 and 2010 budgets (Australian Associated Press, 2010c; Commonwealth of Australia: House of Representatives, 2010; Hocking, 2010; O’Conner & Storm, 2010). This may have prompted the application of consistent, high-impact pressure by policy entrepreneurs on the political stream through the media in 2010 and early 2011. These policy entrepreneurs comprised a group of mental health advocates who worked closely together. They included the highly visible public presence of 2010 Australian of the Year, Pat McGorry (Commonwealth of Australia: House of Representatives, 2010), John Mendoza, and Ian Hickie.
The naming of Professor McGorry as Australian of the Year in 2010 provided important exposure for mental health issues and enabled other mental health advocates to argue for better youth mental health and mental health services more generally (Australian Associated Press, 2011a; Commonwealth of Australia: Senate, 2010). Professor McGorry used his status to highlight the low commitments to mental health in 2010 and was quoted as saying: “[the] Government . . . is pumping all its precious fuel into acute health while mental health is left to run on fumes” (McGorry, 2010b). McGorry was also quoted in parliament as describing the funding for EPPIC in the 2010 budget as “[only enough to build] a heavily diluted cardboard cut-out service lacking many of the core features of EPPIC” (Commonwealth of Australia: House of Representatives, 2010, p. 2216). Hansard reveals that politicians on both sides of the house responded to media appearances and comments by this core group of policy entrepreneurs and also attempted to obtain experts’ approval for their policies (Commonwealth of Australia: House of Representatives, 2010).
Policy entrepreneurs were engaged in creating a further focusing event to publicize their criticism of Labor’s commitment to mental health: John Mendoza’s public resignation on the June 18, 2010, as the CEO of National Advisory Commission on Mental Health, a Commission that the Labor government itself had established. In his resignation letter, Mendoza (2010) argued that “it is now abundantly clear that there is no vision or commitment from the Rudd Government to mental health” and that the government was “publicly claiming credit for the increased investment in mental health when almost all of this is a consequence of the work of the Howard Government.” The contents of his letter were reported nationally (Fyfe & Star, 2010). Mendoza’s resignation ensured that mental health received media coverage in the lead up to the August 2010 election and Hansard records an extensive, often vituperative debate after Mendoza’s resignation. His comments were seized on by the opposition as an indication of wider problems within the Rudd’s Labor Government (Commonwealth of Australia: House of Representatives, 2010; Commonwealth of Australia: Senate, 2010).
Mental health was further promoted as an issue by the highly visible public advocacy organization GetUp! It cooperated with Mendoza after his resignation to highlight mental health issues, generally, and youth mental health, specifically. In the months before the August 2010 election, GetUp! ran a campaign that included candlelight vigils across the country, National TV ads, three full-page newspaper ads funded by donations, a mass emailing campaign to politicians, and the delivery to the Government of a petition signed by 103,000 Australians (Hagan, 2010).
Cohesiveness and unity among professionals in the mental health sector was publically acknowledged as important by these entrepreneurs (McGorry, 2011a). In March 2011, a group of advocates, the Independent Mental Health Reform Group (comprising Monsignor David Cappo, Professors Patrick McGorry and Ian Hickie, Sebastian Rosenberg, John Moran, and Matthew Hamilton), released a report “Including, Connecting, Contributing: A Blueprint to Transform Mental Health and Social Participation in Australia.” This report strongly encouraged the Government to invest in services that were ready for immediate implementation (Independent Mental Health Reform Group, 2011). The coalition’s August 2010 plan and final budget announcement broadly accorded with the Blueprint’s recommendations (Boxall, 2011).
These policy entrepreneurs successfully constructed and maintained youth mental health as a problem demanding political attention. The policy solution—two early intervention programs for youth—was attached to a problem in ways that resonated nationally. These solutions were just as well publicized as the problems they addressed and advertised as ready to be rolled out. Professor Hickie argued in a radio interview hours before the 2011 budget announcement on May 10th, that these programs were “shovel-ready” and so should be funded immediately (Australian Associated Press, 2011a). Widespread lobbying by policy entrepreneurs, including their partnership with GetUp!, was critical to opening the policy window. So was bipartisan support for mental health reform.
Discussion
All five main elements of Kingdon’s framework—problems, policies, politics, policy actors, and policy windows—could be identified at work in this analysis. A social condition, youth mental illness, was identified as a problem requiring action, using data from suicide rates, burden of illness, inequity in access to services, economic costs of not treating mental illness, and through the argument that existing programs were not fit for purpose in dealing with the problem. This effort was aided by focusing events such as the public resignation of a key advocacy figure. Early intervention was the policy solution claimed by these high-profile policy entrepreneurs as effective, having demonstrated success and being readily scalable to meet the recognized need.
The Role of Evidence in Achieving Reform
Evidence was used for policy advocacy, but it was not the sole reason why youth mental health reform reached the threshold where a policy solution was adopted. The way the problem was framed, in terms of the high prevalence and low treatment rates of mental illness, was not new; the data had been available for many years. However, this research evidence was marshaled to construct the problem, and references to the effectiveness of the proposed programs were used to justify their adoption. Evidence was presented in the media by highly effective advocates and supported by media advocacy campaigns by GetUp! These effectively generated a perceived change in national mood that convinced politicians that something should be done. Widespread dissemination of early intervention as a policy persuaded them that something could be done.
The debate, including dissent, within academic and professional communities about the evidence base for the long-term effectiveness and cost-effectiveness of early intervention in reducing the overall burden of mental health is well documented (see, for example, Bosanac, Patton, & Castle, 2010; Pelosi, 2008; The Royal Australian and New Zealand College of Psychiatrists, 2009; The Senate Finance and Public Administration References Committee, 2010), but beyond the scope of this article to address. Interestingly, however, this debate did not appear to significantly affect the political trajectory of the publicised problem or its solution and was in fact primarily publicized in the media after the federal government had announced its decision to implement their policies.
The Role of the (Media-Savvy) “Public” in Creating Political Pressure
An important factor in this case study was the increasing political will for change. The political stream was dominated by Government reactions to a perceived overwhelming public pressure for change, as evidenced by public support for the GetUp! campaign, and the endorsements of Opposition policies by highly influential mental health advocates. Public pressure, however, did not necessarily reflect the views of a representative section of the voting public. Rather, it was a group that could be termed “the conspicuous public,” those who most effectively utilized social media to make their views known, and thus became important influencers of agenda setting on this issue. A recent study has suggested that the “youth vote” (below 35) may have decided the outcome of the 2001, 2004, 2007, and 2010 federal elections (Brooker, 2011). If this is so, then support for youth issues may have increased a political party’s chances of success.
Serendipity
The role of serendipity in policy processes should not be under-estimated. The unexpected change in leader of the Labor party in 2010 and the election of a new government in the same year provided an opportunity for a new leader to move away from the previous leader’s non-committal stance on investing in mental health. This support’s Kingdon’s argument that political timing and context, not all of which can be predicted, are essential for policy change (Hall, 2004; Kingdon, 2003).
Limitations
The findings of the study should be viewed in light of its limitations. First, the short time period used to analyze this case study does not take account of policy developments over the span of decades. A short time period may fail to capture some of these explanatory elements, particularly in the policy stream. The benefit of examining a short policy time frame is that it can examine the role of short-term political pressures and focusing events. Second, the conclusions drawn from an analysis of information in the public domain is almost certainly incomplete. Under recent amendments made to the Archives act of 1983, Cabinet records are now publically available after 20 years rather than the previous interval of 30 years (Commonwealth of Australia, 2013). A future analysis with benefit of access to cabinet documents and the recollections of key policy actors will enable a better assessment of the accuracy of the conclusions we have drawn. Third, the Kingdon framework describes agenda setting rather than the implementation of policy. It was beyond our scope to examine the extent to which the new services actually created the outcomes intended by policy. This is an important area for future study.
Conclusion
We analyzed the case study of youth mental health reform using Kingdon’s multiple streams approach to investigate when and how evidence may have informed agenda setting. Our findings suggest that the policy solutions most likely to succeed are those that are pre-packaged and publicized, are seen to address an identifiable and quantifiable problem, and are supported by high-profile and credible public figures. However, the fact that some research evidence (e.g., the evidence base for the cost-effectiveness of early intervention) did not enter the public debate, or did not feature prominently, raises a number of issues that require careful consideration in terms of the effective use of research evidence to achieve long-term mental health reforms. Our analysis also identified an increasing “double-role” of scientific researcher and policy advocate. The politicized use of evidence by policy entrepreneurs for the advancement of funding to one part of the mental health system has been shown in this study to be a successful approach; however, the scientific community should be conscious that selective reportage of research evidence runs the risk of reinforcing a piecemeal and ad-hoc approach to reform (Whiteford, Harris, & Diminic, 2013). We suggest that the path toward strategic, long-term, evidence-informed mental health governance is perhaps better served by developing and building upon an open political culture, fluid knowledge flow across research and policy realms, and the development of a skilled bureaucratic workforce enabled to make the best use of evidence to inform policy questions (Head, 2014).
The success of policy advocates increased the visibility of youth mental health in the political sphere but only future research will establish whether this policy change has produced lasting changes for the better or perpetuated a cycle of ad-hoc reform prompted by the need to address a perceived crisis created by policy advocates.
Footnotes
Acknowledgements
The authors would like to acknowledge the assistance of Gemma McKeon, Sandra Diminic and Meredith Harris in this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded by the National Health and Medical Research Council (NHMRC) Centre for Research Excellence in Mental Health Systems Improvement (GNT1041131).