
Abstract
This study explores the experiences of aging among gay men to further explain the phenomenon of gay male aging in contemporary terms, to put those experiences into a historically relevant context, and to expand upon previous findings on aging within the gay male population. Nineteen self-identifying gay men from a metropolitan area in South Florida were interviewed. The data collected were analyzed using grounded theory method. Findings from the study indicated that a great deal of optimism was revealed by the participants of the study in spite of their past adversarial experiences related to their sexuality and current challenges related to gay male sexuality and aging. Based on these findings, professionals working with an older population should consider the supportive environments that can most benefit this population in the community and even consider partnering with lesbian, gay, bisexual, and transgender (LGBT) oriented organizations to better serve the needs of their clients.
Keywords
By 2030, one in five Americans will be 65 or older, with an estimated 2 to 7 million of those individuals identifying themselves as gay or lesbian (Grant, 2010). Reports have shown that little is known about the health care needs of older gay men and lesbians (Anetzberger, Ishler, Mostade, & Blair, 2004; Simone & Appelbaum, 2011) and that gay men and lesbians are an understudied population worthy of further attention (Fredriksen-Goldsen & Muraco, 2010; Institute of Medicine, 2011). Understanding the scope of gay men’s aging is further complicated by the U.S. Census Bureau National Population Estimates (2010) not providing statistics estimating the number of gay men living in the United States.
The “Healthy People 2020” (U.S. Department of Health and Human Services, 2011) report addresses the health disparities of lesbian, gay, bisexual, and transgendered (LGBT) individuals linked to societal stigma, discrimination, and denial of many civil and basic human rights. The report also states that discrimination against LGBT persons has been associated with high rates of psychiatric disorders, substance abuse, and suicide. The minority stress model (Brooks, 1981) undergirds the premise that gay men may find aging particularly difficult (Meyer, 1995a, 1995b). Older gay men might have less social support, while experiencing stigmatization and internalized homophobia. Older gay men have also witnessed the devastating effects of the AIDS epidemic, either as long-term survivors of the disease themselves or experiencing the loss of life partners, close friends, and others within their community to the illness. While older gay men share with their heterosexual counterparts common concerns related to aging, declining health, and the need for future care, there is evidence to suggest that they have unique challenges related to self-perception, provider relationships, sociocultural support systems, and medical–legal bureaucracy (Christensen, 2005; Slevin, 2008; Smolinski & Colon, 2006). The purpose of this study was to explore the experiences of aging among gay men to further explain the phenomenon of gay male aging in contemporary terms, to put those experiences into a historically relevant context, and to expand upon previous findings on aging within the gay male population. Historical context is of particular relevance here as it may influence how study participants may perceive their experiences of being gay and aging. At the time of the collection of data for this study, Don’t Ask, Don’t Tell military policy had been repealed, employer-based same-sex benefits among private as well as governmental entities continued to expand, and same-sex marriage was legal in six states including Massachusetts, Connecticut, Iowa, Vermont, Maine, New Hampshire, as well as the District of Columbia.
Literature Review
As an area of scholarly inquiry, the phenomenon of gay aging is relatively new (Fredriksen-Goldsen & Muraco, 2010; Muraco & Fredriksen-Goldsen, 2006). With the topic of homosexuality considered taboo as recently as 50 years ago and homosexuality as a classification of a psychiatric disorder only removed from the Diagnostic and Statistical Manual of Mental Disorders (DSM) in 1973 (Spitzer, 1981), Cruikshank (1991) noted that it has only been since the late 1970s that gerontologists felt free to pursue any interest in gay subjects. Prior to the 1970s, the stigma related to homosexuality was so great, and with the origins of homosexuality still classified as a psychiatric disorder and illegal in many jurisdictions, many social scientists were reluctant to pursue research for fear of being themselves identified as homosexual or having ties to homosexuality. Needless to say, changing demographics, public policy, and societal attitudes continue to alter the current perception of the aging experiences of gay men. From a legal perspective, sodomy laws were only invalidated as recently as 2003 by the U.S. Supreme Court decision of Lawrence v. Texas (2003). Although progress has been made in social policy, legal bureaucracy, and public sentiment, particularly as it relates to changing attitudes toward marriage equality, older individuals who identify as gay continue to be a population that often is stigmatized for both their increasing age and their sexual orientation (Brotman et al., 2007; Brown, Alley, Sarosy, Quarto, & Cook, 2001; Jackson, 2008).
As previously documented in a comprehensive review (Fenkl, 2012), five domains have been identified (Fredriksen-Goldsen & Muraco, 2010) for organizing the literature on gay aging: (a) psychosocial adjustment to aging, (b) identity development, (c) social support, (d) health, and (e) aging-related community needs and services. Regarding psychosocial adjustment to aging, Price (2005) noted that the sexuality of older people, and gays and lesbians in particular, has been largely overlooked resulting in the particular experiences, needs, and concerns of older gay adults being unrecognized from policy, practice, and research perspectives. Other authors have argued that the contemporary image of gay men may favor younger adults (Acquaviva, de Vries, & Quam, 2006; Anetzberger et al., 2004; Fox, 2007). In spite of the common observation of the gay community as explicitly youth oriented, hypothetical predictions of inferior psychosocial adjustment to aging among gay men have been largely unfounded. In fact, significant findings over the course of multiple studies have revealed encouraging conclusions. While the earlier findings of both Bennett and Thompson (1980) and Berger (1984) clearly refuted the idea that older gay men were disengaged from the social aspects of the gay community and experienced especially negative mental health consequences of aging (Bennett & Thompson, 1980; Berger, 1984), other research studies have consistently demonstrated that gay men might even fare better than their heterosexual counterparts with regard to being prepared to accept the realities of aging (Brown et al., 2001; Butler, 2004; Friend, 1991; Quam & Whitford, 1992) as a result of having successfully overcome adversity in younger years. It is also equally important to acknowledge that the positive attitudes toward aging and the lessening of mental health issues among older gay men can likely be attributed to the increasing acceptance of LGBT persons and the greater self-acceptance among gay men as a result of coming out.
Identity development was the focus of studies conducted by both Peacock (2000) and Beard and Hissam (2002). Based on Erikson’s (1959) developmental stages as a theoretical framework, these authors suggested that the traditional schedules of developmental issues addressed across the life span for heterosexuals may not realistically apply to gay men. Speaking to the differences that may prevail between gay men and their heterosexual counterparts as well as between and among gay men, the authors found that recognizing that older gay men may not be at the traditional developmental stage as their heterosexual age peers was as important as recognizing that older men who have lived openly gay lives may be at a different developmental stage from their gay male counterparts who have lived most of their lives closeted. These findings were further underscored by Lee (2004), who suggested that Karp’s (1988) framework used for the examination of identity development in the aging process was heterosexist and not applicable to gay men.
The significance of a social support network for aging populations is readily familiar to professionals working across the spectrum of health care. However, it has been suggested that social support is of particular importance to populations that have been marginalized or who might otherwise perceive an isolated existence due to a lack of familial ties or support (Beeler, Rawls, Herdt, & Cohler, 1999; Christian & Keefe, 1997; Kochman, 1997). Shippy, Cantor, and Brennan (2004) suggested that previous research has shown that the needs of older gay men are no different than those of their heterosexual counterparts. Other research studies point to the AIDS epidemic as a contributing factor in the further isolation of many gay men. This isolation ultimately resulted in the provision of care and social support to friends and partners becoming a major focus of the gay community (Fredriksen, 1999; Shippy et al., 2004).
Perhaps as a result of the AIDS epidemic, matters of health appear to play a significant role among the aging gay male population. In a critical review of the medical literature related to the older HIV-positive adult, Martin, Fain, and Klotz (2008) reported that approximately 25% of new HIV infections were occurring in adults over the age of 50 years. Robinson, Petty, Patton, and Kang (2008) argued that aging with HIV can be confusing and may include times of grief, despondency, and loneliness. Advances in antiretroviral therapy are increasing survival and longevity for people living with HIV. Vance, Moneyham, Fordham, and Struzick (2008) asserted that depression and suicidal ideation represent significant problems for many older adults living with HIV who also may be particularly vulnerable to the influences of ageism and stigma, loneliness and decreased social support, neurological changes, declining health, fatigue, changes in appearance, and financial distress.
Individuals approaching retirement, both gay and heterosexual, are likely to anticipate the financial and health care challenges that lie ahead. However, the challenges facing gay men have been compounded by the institutionalized heterosexism that exists within the systems of health care, government, and society. Institutionalized heterosexism refers to an ideological system that denies, denigrates, and stigmatizes any nonheterosexual form of behavior, identity, relationship, or community (Butler, 2004; Cahill & South, 2002; Chandler et al., 2005; Fannin, 2006; Herek, 1990a, 1990b). As with institutional racism and sexism, heterosexism pervades societal customs and institutions. Operating through a dual process of invisibility and stigma, the primary consequence of heterosexism is marginalization for those not part of the mainstream heterosexual culture. This marginalization precludes the individual members of the gay community from real or perceived meaningful participation in society and perpetuates, among the marginalized, the perception that their individual needs are not being recognized or met.
Method
The method of grounded theory (Charmaz, 2006; Glaser, 1978; Glaser & Strauss, 1967) was used in this study to construct a substantive theory of the experience of aging among gay men. Grounded theory focuses on the perspectives of study participants in regard to their experiences with a phenomenon rather than applying an existing theory to those experiences. Existing theories might be applicable to specific aspects of the experience of aging among gay males but would not address the processes of aging that may be uniquely specific to this population. Grounded theory results in a substantive theory that reflects and is grounded in the experiences of the participants in the study and can expand existing theoretical approaches to the phenomenon.
This study was conducted in a metropolitan area in South Florida with a large population of men who identify as gay. Although it has been historically difficult to estimate the actual size of any gay population, recently released data from the 2012 census designates the city of Fort Lauderdale as having the highest concentration of same-sex couple households in the country with 2.8% of all households. After obtaining approval from the Institutional Review Board of the investigator’s university, the researcher distributed flyers at a variety of locations in the area that were frequented by gay men including churches, clinics, nightclubs, community centers, and local retail establishments.
The investigator conducted 19 face-to-face interviews with those who responded and who gave their informed consent to participate in the study. Eligibility criteria included male participants between the ages of 55 and 70 who self-identified as gay. Interviews of approximately 60 to 90 min in length were conducted with each participant in a private location of the participant’s choice. Following each audio-recorded interview, the recording was transcribed verbatim by a transcriptionist skilled in the confidential handling of research transcripts. The investigator checked each transcript for accuracy by comparing it with the original audio recording. NVivo 8.0 software was used for data management and the analysis proceeded from initial open, substantive coding through category construction. Using the constant comparative analysis approach described by Glaser and Strauss (1967), Glaser (1978), and Charmaz (2006), the process of analysis began with open, substantive coding. In this first stage, code words or phrases were used to capture the substantive content of each idea presented in the data. More than one code was assigned if necessary to capture as many ideas as possible without premature closure. When appropriate, codes were the actual words used by the participants. The next phase of analysis involved working with the initial codes to identify categories of similar content and ideas. Using the constant comparative analysis process that is the hallmark of grounded theory, the researcher compared content within codes and codes with other codes to identify similarities and develop a system of categories that captured the experiences of the participants. These categories next were examined to determine patterns and consistent ideas in the categories as well as to identify areas of overlap of conflict. The categories were continually reworked until a concise system of categories was developed that captured the experiences of the participants in a clear, meaningful, and parsimonious way. The final stage of analysis involved the identification of the core variable that illustrated the Basic Sociopsychological Process present in the experiences of the participants. This was accomplished by reviewing the categories, examining the content within categories, and ultimately determining the core or unifying thread that tied the categories together. While this analysis process is described here as occurring in stages, the actual work of analysis is iterative and involved the researcher continuously reexamining the raw data, exploring questions in the data and the analysis, challenging his own conceptions, and ultimately arriving at a core variable and category system that is based in the experiences of the participants and that captures those experiences in a meaningful way.
The researcher utilized a number of strategies to enhance the rigor of the research throughout all of the steps of the process. Throughout the research, the investigator maintained an audit trail (Lincoln & Guba, 1985) to document all of the aspects of the study and ensure that the findings were based in the words and experiences of the participants and not the ideas of the researcher (Glaser, 1978; Lincoln & Guba, 1985). The audit trail consisted of the actual research data along with memos regarding theoretical insights generated during analysis and field notes documenting the conditions of the interview and the researcher’s initial impressions. Using these materials as documentation of the research process, the researcher engaged in extensive peer review and debriefing with the coauthor in which analytic ideas and conclusions were challenged to ensure that results were grounded in the experiences of the participants.
Findings
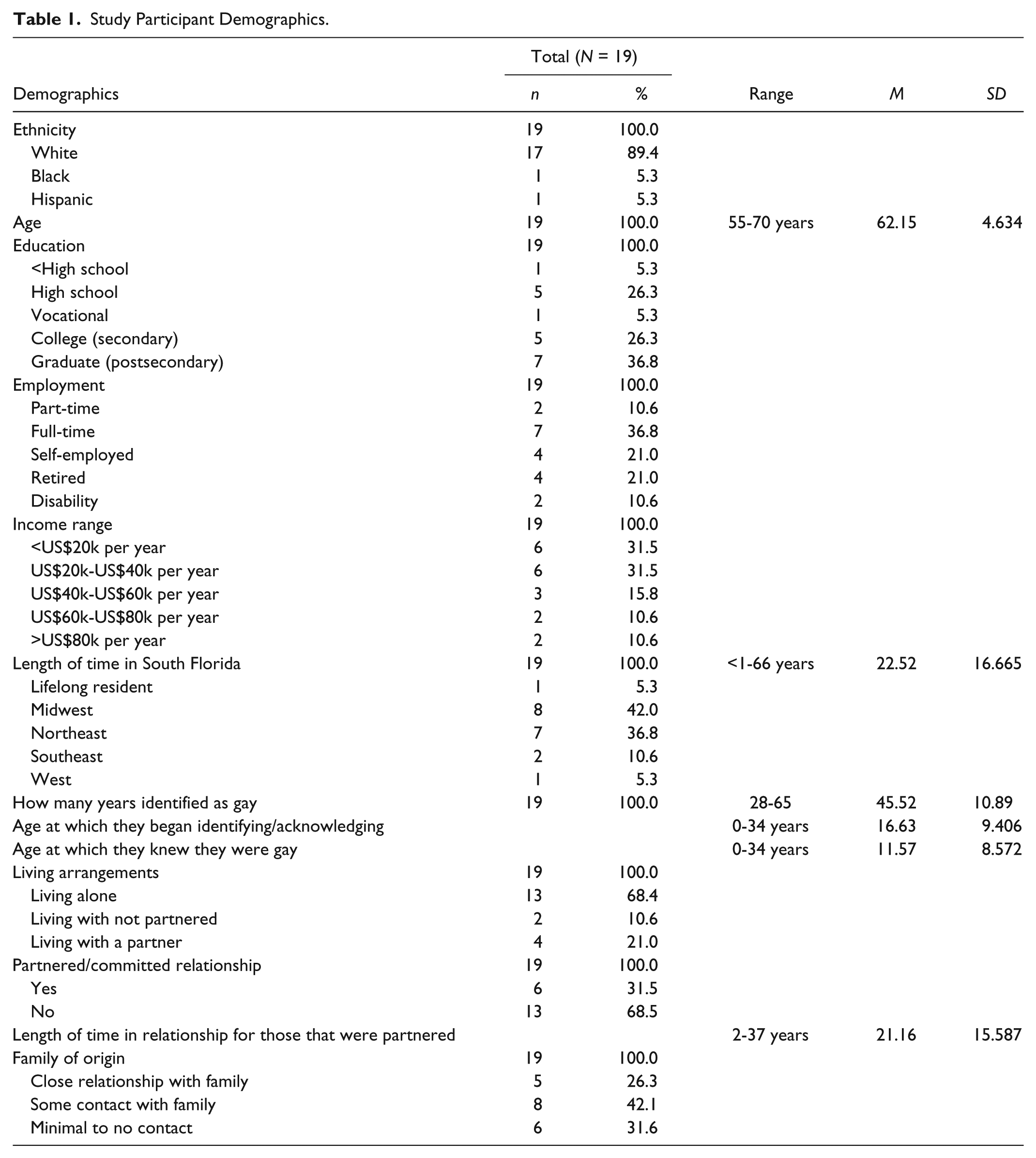
The findings of this study were developed from 490 pages of interview transcripts obtained from 19 self-identifying gay male study participants (Table 1). It is important to note that the study participants were for the most part White (89.4%) with the majority reporting having a college degree (63.1%), However, socioeconomically, the sample was not as homogeneous with study participants reporting a wide range of income levels. Overall, participants of the study perceived their experiences of aging to be overwhelmingly optimistic in spite of the adversities they have encountered in the past and the realities of aging that they currently face or anticipate encountering in the future. “Optimistically engaging in the present,” as a core category and basic social process, is the culmination of three social processes that have developed over the course of the participants’ lives, either through a learned or serendipitous process, that involve resolving adversity, negotiating the realities of aging, and developing resources (Figure 1). Resolving adversity refers to the social process of coming to terms with and/or overcoming issues in one’s life that were challenging such as the stigma related to one’s sexual orientation. Negotiating the realities of aging refers to the process of being cognizant of those elements of aging that one may encounter as one ages and cannot realistically change. Developing resources refers to the process of recognizing what can be done to improve one’s life and the experience of aging, whether as an internal process of self-perception or attitude toward aging or as an external process of seeking out resources available in the community. The process of resolving adversity has meaning and applicability for the study participants because of the unique challenges they reported encountering in their lives, not exclusively, but often related to the stigmatization and victimization of individuals identifying as or perceived as being gay. It should be further noted that the sample of men who participated in this study may be representative of a subset of the gay male population that, by virtue of their willingness to participate in such a study and self-identify as gay, may in fact be more well adjusted in terms of their perceptions of self and self worth and have a more positive outlook on life than a sample of men who are not willing to self-identify as gay outside of their own social network.
Study Participant Demographics.

Optimistically Engaging in the Present.
Resolving adversity involves the study participants resolving the past and utilizing the knowledge, strength, and wisdom that come from such resolution in the present. When asked to describe their experiences of aging, study participants would often begin by saying that they did not think about themselves as aging. Instead, they began by describing the resolution of past conflicts and coming to terms with self and self-acceptance as part of their aging experience. One participant, who reported being retired as a high school crisis counselor and being long-term partnered, described his satisfaction with life in the present, as well as the internalized homophobia he struggled with as a young man. He went on to describe how he resolved his conflict with his sexual orientation and how that may have contributed to his personal and professional development: Oh, I feel like I’ve had a very good life. Yeah. I wish that I didn’t have the issues earlier on from like 14 to 25 of not accepting myself, because really that’s what it was. I just could not accept that I was gay. I just thought I was a sick individual. And our society supported that, because it was 1950s, 1960s, you know, so that was like a lot of waste of energy also. But, I guess it made me more observant about people and it made me study more about psychology and it made me become a psychologist.
This study participant described how, in part, resolving the internal conflict he had with his sexual orientation took the form of learning to accept himself as a gay man. His acceptance of self as a gay man fostered an interest in psychology and that interest developed into a professional endeavor as a school psychologist. In turn, his chosen profession put him in a position to help other young people who struggled with their own sexual orientation, and provided him with greater career and personal satisfaction knowing he could make a difference in others’ lives.
The process of negotiating realities is the second of the three processes that emerged as foundational to the basic social process of optimistically engaging in the present. Negotiating realities involves the interplay between the challenges anticipated by all individuals as they get older—such as financial burdens, declining health and health care, loss of independence, retirement, and the need for care in older age—and the challenges the study participants may encounter that are more consistent with a gay male culture. Those challenges include an overemphasis on appearance and youth, isolation due to lack of familial or social support, and vulnerability to homophobia and victimization. Negotiating realities is characterized by study participants acknowledging changes as they related to aging, including how aging has influenced their perceptions of self and getting older and the possibility of declining health. One study participant, age 62, a nurse who also was a well-known female impersonator in the community, was interviewed shortly after having a below-the-knee amputation as a consequence of a diabetic infection. He described his perception of health and health care and aging as a gay male: When you’re young you don’t really worry about health care. You know, it’s just not on the top of your priority list. Being older and gay you kind of learn that the future is very unsure because, you know, so many gay people are alienated from friends and family because they are gay, and that the older they get, it’s much more frightening to think that they’re gonna be alone. So, prepare, tell, people, especially gay people because they have that tendency of not doing that because they live the carefree life all their life, that this is part of their way of living, prepare, prepare, ’cause you don’t know, and it’s not easy being, a charity case now when I’m used to asking people for help and now I have to survive. So that’s a big change in my life right now is that I have to ask people for help.
Although study participants described the realities related to aging in terms of what they perceived to be the challenges confronting them as they age, they generally did so with an optimistic perspective. However, optimistically engaging in the present requires more than just an optimistic perspective; it also involves resources that facilitate the successful negotiation of the realities of aging. Study participants described a variety of resources that facilitated that process.
The process of developing resources, third of the three processes, emerged as another important category of the basic social process of optimistically engaging in the present. The process of developing resources has meaning and applicability for the study participants as the resources were developed over the course of a lifetime and were often developed in response to having to resolve the adversities they encountered, either as individuals or as members of a potentially stigmatized population. The development of these resources and their usefulness in application to the challenges of aging contribute to the basic social process of optimistically engaging in the present and are inherently connected with the processes of resolving adversity and negotiating realities. Study participants described a variety of resources. These resources included being active in the community, having a sense of faith or spirituality, having feelings of acceptance both of oneself and by one’s community, seeking out gay-friendly health care providers, maintaining a positive outlook on life, having a strong social support network, being satisfied with one’s life, having a positive perception of self, and acknowledging the significance of being partnered. One participant, aged 67, described faith and spirituality in terms of the unique opportunity he perceived gay men to have over their heterosexual counterparts from a more secular angle: I want to be 80 and I want to be enjoying life. I see a lot of spiritual groups. I see a lot of weeklong retreats, a lot of, you know, organizations that are doing positive things for the gay community and people are involved with, and I think all of that is because we are demanding more. We’re demanding that life be good, we’re demanding that we’re fulfilled in this world. And because of that, all these things are popping up that will allow people to get together and discuss issues like that and, you know, the straight world may have that, but I think the straight world has it probably through religious organizations. And because so many gay people aren’t tied into specific religious organizations, I think we’re freer to create the secular organizations that treat our spiritual needs.
Again, this participant provides further insight into how gay men perceive themselves in the aging process and subsequently describes how their needs in advanced age can be met in a more culturally competent approach. Cultural competence is also relevant to the health care needs of older gay men. When asked about health care, most study participants described being most comfortable with what they described as “gay friendly” providers. Gay-friendly providers were providers that were either gay themselves or providers that served a population of gay men. Gay-friendly providers were perceived as being more open to discussion related to gay male sexual health and more aware of the psychosocial challenges that may be specific to older gay men such as loss of a partner. Table 2 provides an overview of the specific categories and components that emerged as part of the process of optimistically engaging in the present. These categories and components are relevant and particularly helpful as a framework for assessing the needs of older adults who identify as gay, as well as relevant for other older adults.
Summary of Category Components.

Implications for Research and Practice
The population of self-identifying older gay men is growing. This is the result of both the growing population of older adults in general as well as the growing visibility of people who identify as gay (Cahill, South, & Spade, 2000; Grant, 2010; Price, 2005). As the older gay community grows in both size and visibility, so too will the need for an evidence-based understanding of the issues that are unique to this population. The findings of this qualitative study are unique to the particular time and place in which the study data was collected and no claims can be asserted with regard to the generalizability of these findings to other samples of gay men in other geographic area. However, these findings do in fact reinforce the argument that sexual minorities such as gay men are more optimistic about their lives when living in an environment that is supportive, more inclusive, and less stigmatizing. In spite of the optimism that was evident in participants in this study, it is important to note that LGBT Americans are recognized by The U.S. Department of Health and Human Services (2011) as one of six groups affected by health disparities. In addition, there are long-lasting effects on the individual and the community from frequent experiences of violence and victimization, as well as struggling with issues of acceptance, personal, family, and societal (Simone & Appelbaum, 2011). The question that begs an answer for practitioners is how to make environments more supportive and inclusive, and less stigmatizing when the community at large is not necessarily so. In terms of research, perhaps the greatest threat to the health of lesbian, gay, and bisexual Americans is the lack of scientific information about their health and the lack of knowledge related to LGBT patient centered outcomes. While the findings of this study contribute to an increased understanding of the health and psychosocial needs of gay men in a geographic location that is welcoming to gay men and provides a supportive environment, both through the resources available and the sheer number of gay men living in the geographical area, further similar research is warranted that targets more diverse gay male populations in less supportive environments, particularly among men who are not openly gay and live closeted lives. Such research is likely to reveal a myriad of findings related to gay male aging experiences. This is important as the expansion of the knowledge base to include groups who have been overlooked, such as gay men, provides health care professionals with a heightened awareness of the challenges encountered by such groups, and is foundational to culturally appropriate and individualized care. It is also important to note that in spite of the optimism revealed in the findings here, stigma stills plays a prominent role in the delivery of LGBT health care. The potential stigmatization that older gay men encounter in health care settings can be decreased when health care professionals have a greater understanding of the life experiences and perspectives that this population brings into the health care setting. This is a pivotal point as the local health care environment determines one’s experiences and is highly variable. For example, the findings of the study presented in this article demonstrated that the sample population preferred gay-friendly health care providers and thrived in a supportive social environment. Gay men who are not comfortable disclosing their sexual orientation to health care providers may be at risk of not receiving an appropriate health care screening. In addition, participants of this study reported concerns related to physical changes, financial status, isolation, loss of independence, and sexual relations and functioning. This greater understanding of the superimposed conditions that accompany aging among gay men is imperative for health care and other professionals across a spectrum of practice. Based on these findings, strategies for addressing sexual orientation with clients that promote feelings of acceptance and understanding should be considered, as disclosure of one’s sexual identity is often related to perceived safety, and the pervasive expectation of gender conformity on the part of health care professionals can be alienating. In addition, assessments that may be of concern to older gay male clients such as alterations in physical appearance, perceptions of feeling isolated or lonely, relationship status, and sexual functioning and satisfaction should be considered. Equally important is the assessment of caregiver-role stress of the older gay male client. As this population ages, the likelihood that they will find themselves in a caregiver role is also likely to increase, particularly for those who have been long-term partnered. Within the context of this study, agencies and organizations were identified that were geared specifically toward the needs of older LGBT individuals. Based on these findings, professionals working with an older population should consider the supportive environments that can most benefit this population in the community, and even consider partnering with these organizations to better serve the needs of their clients (Rosenfeld, Bartlam, & Smith, 2012). These interventions would include an understanding of the resources that are available in the community that can facilitate peer support as well as the referral to agencies and organizations that are best suited to meeting the needs of an older gay population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.