
Abstract
Prior research yields mixed results about black–white difference in trust in their doctors, and existing studies are often based on nonrepresentative, local, or cross-sectional samples. Using data from the 1998, 2002, and 2006 General Social Surveys—nationally representative samples—and ordinary least squares regression, this study reexamines this issue. It was expected that blacks are less likely to trust their doctors than whites either before or after controlling for other predictors of trust and that there was no significant change in this relationship over the time period under study. The results indicate that blacks were less likely to trust their doctors than whites only in 2002, but not in 1998 and 2006. This finding suggests that, even with the same source of data, empirical support for the claim about the less trust of blacks in doctors than whites is less robust than conventional belief, and it calls for additional, careful reexamination.
Trust plays an important role in the relationship between patients and their medical doctors. Patients who have greater trust in their doctors are more likely to adhere to their doctor’s advice, experience greater satisfaction with the care they receive, and report an improved health status (Safran, Kosinski, Tarlov, Rogers, Taira, Lieberman, & Ware, 1998; Thom, Ribisl, Stewart, Luke, & the Stanford Trust Study Physicians, 1999). Greater trust is related to greater self-efficacy in treatment regimens and positive expected health outcomes (Lee & Lin, 2009). Trust has also been shown to positively influence use of preventive services such as cancer screening and routine checkups (Musa, Schulz, Harris, Silverman, & Thomas, 2009; O’Malley, Scheppard, Schwartz, & Mandelblatt, 2004).
Trust, as it pertains to health care, has been described as the result of both interpersonal experiences with doctors and trust in health care as a system (Hall, Zheng, Dugan, Camacho, Kidd, Mishra, & Balkrishnan, 2002). Most commonly, studies have examined outcomes and differences in interpersonal trust, or trust in doctors. Interpersonal trust includes both direct and indirect dimensions. Direct trust relates to the patient’s trust in his or her physician whereas indirect trust relates to the patient’s trust in behaviors of physicians in general. Commonly, research has relied on global measures of trust that are a composite scale measure of indirect and direct measures of trust (Stepanikova, Mollborn, Cook, Thom, & Kramer, 2006).
Prior research yields mixed results about black–white difference in trust in their doctors. Some studies have concluded that there is no significant difference between blacks and whites in trust in their doctors (Benjamins, 2006; Bonds, Foley, Dugan, Hall, & Extrom, 2004; Hall, Dugan, Zheng, & Mishra, 2001; Pescosolido, Tuch, & Martin, 2001), or that differences in trust can be explained by other factors such as perception of racism or community-level factors (Adegbembo, Tomar, & Logan, 2006). Other studies, including those using nationally representative samples, draw an opposing conclusion that blacks are less trusting in a range of health care settings, including trust in physicians, trust in health care as a system, and trust in medical research (Berrios-Rivera, Street, Popa-Lisseanu, Kallen, Richardson, Janssen, & Suarez-Almazor, 2006; Boulware, Cooper, Ratner, LaVeist, & Powe, 2003; Corbie-Smith, Thomas, & St. George, 2002; Doescher, Saver, Franks, & Fiscella, 2000; Hunt, Gaba, & Lavizzo-Mourey, 2005; Musa et al., 2009).
Existing studies are often based on nonrepresentative, local, or cross-sectional samples. A few longitudinal studies, however, have been conducted to analyze black–white difference in trust in doctors. While those that have done so have found no difference between blacks and whites, attempts to study the role of trust longitudinally have not used a nationally representative sample (Safran, Kosinski et al., 1998; Safran, Taira, Rogers, Kosinski, Ware, & Tarlov, 1998; Taira, Safran, Seto, Rogers, Inui, Montgomery, & Tarlov, 2001) or are limited to general measures of trust in doctors as a professional group (e.g., “doctors always do their best to keep the patient from worrying”; Pescosolido et al., 2001).
This study seeks to contribute to the literature by providing additional insights into the black–white difference in trust in doctors. The current study differs from previous studies by using nationally representative data from the General Social Surveys (GSSs) for the years 1998, 2002, and 2006 to examine black–white difference in trust in doctors longitudinally. It does so using a global measure of trust that reflects measures of direct and indirect trust in doctors similar to those found in previous studies.
Hypotheses
The first hypothesis to be tested in this study is that African Americans are less likely to trust their doctors than white Americans, holding other factors constant. Historically, black Americans were less likely to trust the health care system and health care professionals because of a history of institutional discrimination and exploitation by the medical community reflected in such events as the Tuskegee Syphilis Study (Gamble, 1997; Kennedy, Mathis, & Woods, 2007). This hypothesis is also partly grounded on findings of some previous studies that blacks are less likely than whites to trust their doctors (Musa et al., 2009) and the health care system as a whole (Boulware et al., 2003). Furthermore, research has shown that blacks have less positive perceptions of their relationship with their doctors (Doescher et al., 2000) and report a lower level of trust in their physician regardless of factors such as health plan type (Hunt et al., 2005) or characteristics of doctor–patient communication (Berrios-Rivera et al., 2006). Also as an issue of trust, black Americans are less likely to participate in medical research (Corbie-Smith et al., 2002; Shavers, Lynch, & Burmeister, 2002) and are less likely to donate organs because of the perception that they may not receive necessary medical care (Minniefield, Yang, & Muti, 2001).
The second hypothesis is that there was no significant change in the black–white difference in trust in doctors over time in the period under study. Historical factors that have influenced trust in the black community cannot be erased in a short period of time and will have lingering impact on trust in doctors. As there was no significant change in the general social environment that could significantly alter black–white difference in trust in their doctors in the period under study (1998-2006), we expect a relatively stable relationship between race and trust in doctor.
Data and Method
The data for this study come from the GSSs for the years 1998, 2002, and 2006. These years were selected because the GSSs included questions pertinent to direct trust in doctors in each of these years. Each survey was a nationally representative sample of adult men and women in the United States. The samples used for this analysis consisted of only black and white respondents who supplied a valid response to a series of indicators on trust in doctors. The sample was restricted to only black and white respondents because of the focus of this study and because of the very small numbers of respondents in the other race category. After the restrictions, the sample sizes are 1,190 for 1998; 1,267 for 2002; and 1,216 for 2006. The data were weighted so that only one adult per household was included in the samples. Because the samples are nationally representative, the findings can be generalized to the population.
The dependent variable for this analysis is respondent’s trust in his or her doctor. This variable is measured by creating a simple-summated scale based on four indicators in GSSs 1998, 2002, and 2006. Respondents were asked to rate on a Likert-type scale (1 = strongly agreed, 2 = agree, 3 = neither agree nor disagree, 4 = disagreed, or 5 = strongly disagreed) each of the following statements: (a) “I trust my doctor’s judgments about my medical care,” (b) “I trust my doctor to put my medical needs above all other considerations when treating my medical problems,” (c) “My doctor is a real expert at taking care of problems like mine,” and (d) “I trust my doctor to tell me if a mistake was made about my treatment.” Each indicator was reverse recoded using a new scale of 0 to 4 (0 = strongly disagree . . . 4 = strongly agree) so that a higher score reflected stronger agreement with each statement. The scores of the four indicators of trust were then summed. The result was a scale of trust in doctors (0 = lowest trust and 16 = greatest trust) with a good level of reliability (Cronbach’s α = .80). Indicators 1, 2, and 3 are considered direct measures of trust as they reflect respondent’s trust in his or her personal doctor. Indicator 4 is considered to be an indirect measure because it measures respondent’s trust in his or her doctor’s behavior and not as a person. The resulting scale represents a global measure of trust that contains previously validated measures and is similar to those used in previous studies (Stepanikova et al., 2006; Thom et al., 1999).
The independent variable is race, which is measured by a dummy variable with 1 indicating black and 0 indicating white.
In order to ascertain black–white difference in trust in doctors, a number of predictors are included as control variables. Gender is measured as a dummy variable with male coded as 1 and female coded as 0. Age is a continuous variable measured by years. Education is also a continuous variable measured by years of schooling completed ranging from 0 to 20. Family income is a continuous variable designed to reflect respondent’s family income measured by thousands of U.S. dollars. Marital status is coded as a dummy variable that reflects whether a respondent had ever been married (1) or never married (0). Having children is a dummy variable that reflects whether a respondent had one or more children coded 1 or no children coded 0. Likewise, self-employed, Christian, or Democrat are also coded as dummy variables with 1 indicating the designated category and 0 otherwise. The final variable in the analysis is the respondent’s subjective social class, an ordinal variable with four categories (1 = lower class, 2 = working class, 3 = middle class, or 4 = upper class).
Some limitations of the data should be acknowledged. Some factors that have been shown to be positively correlated with trust in doctors such as general health of the respondent, 1 general trust in people (Benjamins, 2006), 2 patient’s choice of physician, and length of relationship (Kao, Green, Davis, Koplan, & Cleary, 1998; Thom et al., 1999) are not included in the analysis because they were either not asked of the same respondents or were not asked in each year. The surveys were not consistent in asking questions that may have allowed for a more precise measure for trust in doctors. Among these were questions of general trust such as, “Doctors aren’t as thorough as they should be.” As a result, these were not included in the analysis. Ideally, a longer time span for the surveys would be better to observe changes over time, but only three surveys from 1998 to 2006 are available. Despite these limitations, the samples for this study are unique compared with other studies on trust in doctors because they permit a longitudinal analysis.
Descriptive statistics including the means and standard deviations for each variable were calculated to assess the similarities between the samples in each year. Bivariate correlations are used to test for multicollinearity between the variables and to show the relationship between each variable and trust in doctors. The main method of data analysis is ordinary least squares regression because the dependent variable is a 17-point scale—a proximate interval/ratio measurement.
Results
Table 1 shows the means and standard deviations of all the variables used in the analysis. Figure 1 based on scores of the dependent variables in Table 1 indicates that there is a similar pattern for each predictor that was used to construct the Trust in Doctors scale. The mean score of each predictor rose from 1998 to 2002, and fell from 2002 to 2006. The Trust in Doctors scale followed the same trajectory. Trust was highest in 2002 (M = 12.36), was lower in 2006 (M = 11.53), and lowest in 1998 (M = 10.62).
Mean and Standard Deviations of Variables Used for Analysis, U.S. black and white Adults, GSSs 1998, 2002, 2006
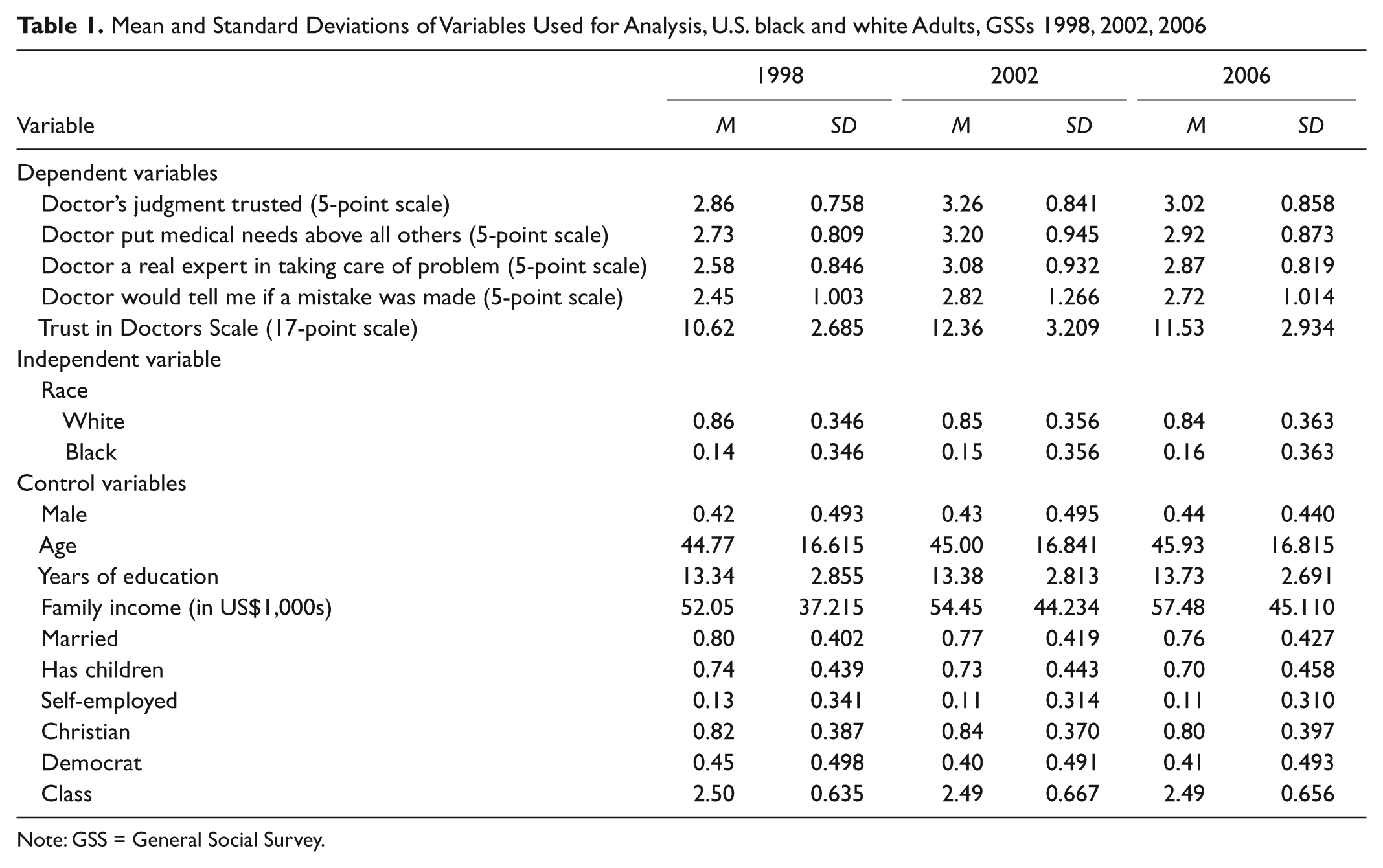
Note: GSS = General Social Survey.

Means of the Trust in Doctors scale and its indicators, GSSs 1998, 2002, and 2006
Table 1 also shows that the sample for each year had similar characteristics. The mean of a dummy variable can be interpreted as a percentage after multiplying the value by 100. Hence, blacks made up 14% of the sample in 1998, 15% of the sample in 2002, and 16% of the sample in 2006. Males accounted for about 43% of each sample. The samples were also similar in age (about 45 in mean age), education (about 13 years in schooling), percentage ever married (between 76% and 80%), if had children (between 70% and 74% with children), and percentage self-employed (between 11% and 13% self-employed). Their religious orientation (largely Christian), political party affiliation (between 40% and 45% Democrat), and reported subjective class (close to middle class) were also similar.
Tables 2, 3, and 4 show the results of the bivariate correlations. The black dummy variable shows a negative relationship with trust in doctors in 1998 (r = −.012, n.s.) and 2002 (r = −.056, p ≤ .005), but a positive relationship in 2006 (r = .017, n.s.), although it is only significant in 2002. Other predictors also show varying relationships with trust in doctors. Age has a significant positive association with trust in 1998 and 2002, but is not significant at the .05 level in 2006. Christians were significantly more likely to trust their doctors than non-Christians in 1998 and 2002, but not in 2006. Self-employed individuals displayed less trust in doctors in the 2002 and 2006 samples, but not in the 1998 sample. Democrats trusted doctors more than non-Democrats in 1998 and 2006. Males were less likely than females to trust their doctors significantly in 2006. Education was negatively correlated with trust in 2002, and family income was negatively correlated with trust in 1998. Social class and the dummy variables for “ever married” and “having children” were not significantly correlated with trust in any of the 3 years. The bivariate correlations also show that there were no issues of multicollinearity between the variables.
Correlation Matrix for the Variables Used in Analysis, GSS 1998

Note: GSS = General Social Survey.
p ≤ .05 **p ≤ .01 ***p ≤ .001 (one-tailed test)
Correlation Matrix for the Variables Used in Analysis, GSS 2002
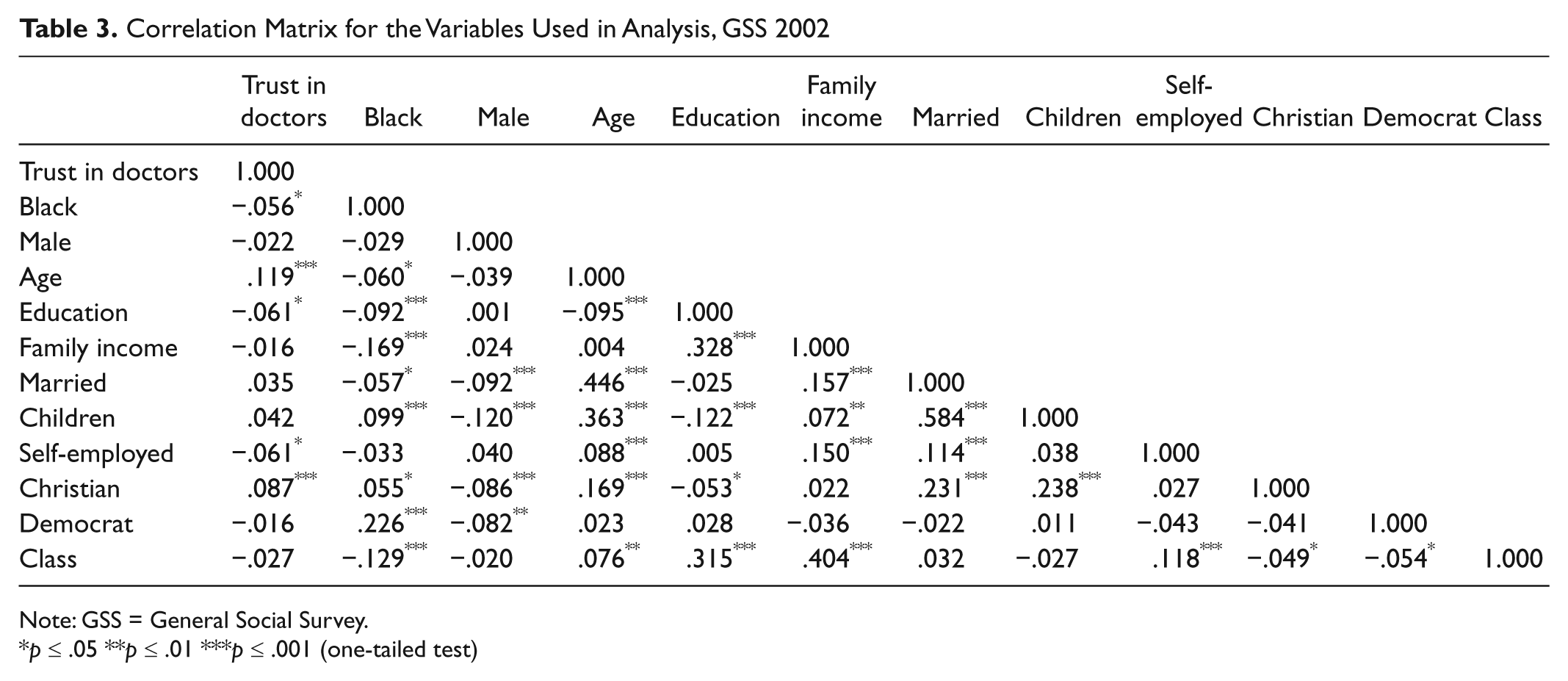
Note: GSS = General Social Survey.
p ≤ .05 **p ≤ .01 ***p ≤ .001 (one-tailed test)
Correlation Matrix for the Variables Used in Analysis, GSS 2006
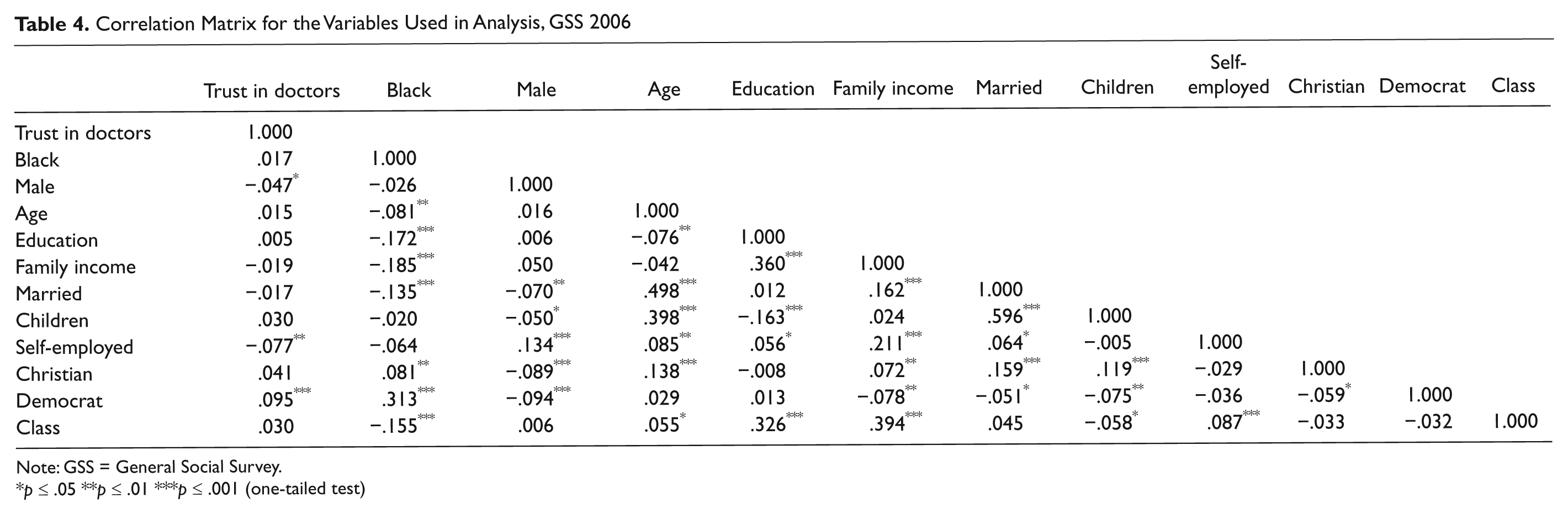
Note: GSS = General Social Survey.
p ≤ .05 **p ≤ .01 ***p ≤ .001 (one-tailed test)
Table 5 shows the results of the linear regression models. Model 1 reflects the association between being black and trust in doctors without any additional predictors. Model 1 was significant only in 2002 (F = 3.909, p ≤ .05). The race variable accounted for less than 1% of the variance in trust in doctors (R2 = .003). In 2002, blacks were significantly less likely to trust their doctors than whites (B = −.500, p ≤ .05). In 1998 and 2006, the difference between blacks and whites in trust in doctors was not significant, although blacks were slightly less likely to trust doctors than whites in 1998. These results partially support the first hypothesis that blacks are less likely to trust their doctors than whites, but do not support the second hypothesis that this relationship is consistent over time.
OLS Regression Models Predicting Respondent’s Trust in Doctor, U.S. black and white Adults, 1998, 2002, 2006

Source: General Social Surveys 1998, 2002, and 2006.
Note: OLS = ordinary least squares. Standard errors are given in parentheses.
p ≤ .05 **p ≤ .01 ***p ≤ .001 (one-tailed test)
Model 2 includes additional predictors as control variables. This model improves on Model 1 as the F value is significant for all 3 years, and it explains about 5% of the variance in trust in doctors in 1998, about 4% in 2002, and 2% in 2006. One-tailed tests were used to determine statistical significance because a directional relationship was assumed between each predictor variable and the independent variable. Trust was highest in the 2002 sample (B = 11.931) followed by the 2006 sample (B = 10.135), and lowest in the 1998 sample (B = 8.977).
Blacks continued to display a lower level of trust in their doctors than whites in 2002 after controlling for other variables (B = −.497, p ≤ .05). However, the black–white difference in trust was statistically insignificant in 1998 and 2006 as the regression coefficients for being black for those years did not reach statistical significance at the .05 level, albeit negative in 1998 (B = −.283, n.s.) but positive in 2006 (B = .009, n.s.). The results continue to partially support the first hypothesis after controlling for other variables but not the second hypothesis that the relationship is consistent.
The control variables display varying effects. Age was a significant predictor of trust in 1998 and 2002 but was not in 2006. Self-employed individuals reported a lower level of trust in their doctor, but this effect was significant only in 1998 and 2002. Christians were more likely to trust their doctors than non-Christians, but this predictor was also only significant in 1998 and 2002. Democrats showed a higher level of trust than non-Democrats in both 1998 and 2006, but this predictor had an insignificant positive association with trust in doctors in 2002. Family income was significant in 1998 but showed a very weak positive association. Ever married respondents were less likely to trust their doctors in 2006 than their never married counterparts. Respondents who had had children were more likely to trust their doctors in 2006 than those without children. Neither marriage nor having children was a significant predictor of trust in 1998 or 2002. Social class displayed a significant positive relationship with trust in 2006 but an insignificant relationship in 1998 or 2002.
Conclusion
The most important finding of this study is that blacks were significantly less likely to trust their doctors than whites only in 2002, but not in 1998 3 or in 2006. This finding suggests that, even with the same source of data, empirical support for the claim about the less trust of blacks in doctors than whites is less robust than conventional belief, and it calls for additional, careful reexamination. The inconsistent results in the black–white difference in trust could be taken as evidence that trust in doctors may or may not depend on the race of respondents. This study does not rule out the possibility that trust could be the result of individuals’ personal interaction and experience with their doctors, including the length of their relationship and frequency of contact (Hall et al., 2002; Safran, Kosinski et al., 1998; Thom et al., 1999). It is also possible that there are other factors that mitigate the black–white difference in trust in doctors such as perception of racism or community-level factors (Adegbembo et al., 2006). The results should also be interpreted cautiously due to the reliance on samples of different respondents as opposed to the same respondents over time.
Associated with the first major finding, another finding is that the black–white difference in trust in their doctors varied over time in the period under the study. The data also reveal that trust was relatively dynamic. Whereas previous studies displayed high trust in physicians (Bonds et al., 2004; Doescher et al., 2000; Hall et al., 2001), the findings here show mixed results. The variance of mean trust scores was greater for whites than that for blacks across the samples, although black trust scores varied as well. Therefore, there may be additional factors in these years that have not been considered but may have influenced trust in physicians. In all, whites show almost three points of variance in mean trust between 1998 and 2002, whereas blacks show closer to two and half points of variance. Understanding why trust scores can vary in a short period of time may be significant because there is evidence that medical skepticism influences medical outcomes (Doescher et al., 2000).
The results of the control variables suggest that social predictors of trust in doctors are inconsistent. Several control variables are significantly associated with trust in doctors in 1 or 2 years, but none of these predictors were consistent across the samples. The finding that age is positively associated with trust might be considered intuitive because of the association of trust with frequency of contact between the patient and the doctor. As older individuals may be more subject to health problems, they may also have more opportunities to build a relationship with their doctor. This is speculative as age is not a significant predictor in all three samples, but this suggestion is consistent with results reported elsewhere (Thom et al., 1999). Self-employment may be a significant predictor of trust for similar reasons, as self-employed individuals are less likely to have access to health care and therefore have less contact with a regular doctor. Also, the finding that Christians were more likely to trust doctors in 1998 and 2002 is consistent with previous research (Benjamins, 2006), but, like age and self-employment, this is not a significant predictor in the 2006 sample. It is interesting that this study finds that Democrats were more likely to trust their doctors than non-Democrats. This suggests that Democrats may have a differing relationship with physicians in some way than those of another political affiliation.
Overall, the results of this study do little to settle the debate about whether blacks are less likely to trust their doctors than whites. The study offers bullets for both sides of the debate. Even when using the same data set, there was considerable variance in trust levels of both whites and blacks, and the black–white difference was not consistent across years. Thus, more longitudinal analysis is necessary for future research in order to ascertain differences in trust in doctors between blacks and whites. Including a greater number of relevant predictors not yet included in existing studies could produce more accurate estimates and help an eventual settlement of the controversy over black–white differential in trust in medical doctors.
Footnotes
Acknowledgements
An early version of this paper was presented at the 2012 Annual Conference of the Southwestern Social Science Association in San Diego in April 2012. We would like to thank the participants of the conference for their useful comments and suggestions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.