
Abstract
How does race-gender status shape the medicalization and criminalization of those with mental illness? Using data from the 2022 wave of the National Survey on Drug Use and Health, I examine the associations between mental illness and arrest versus mental health treatment, and how these associations vary by race-gender status. I find significant patterns of difference among Black, Hispanic, and White men and women. Having mental illness is significantly, positively associated with arrest for all groups, however the magnitude of this relationship is statistically greater for Hispanic men. In addition, Hispanic men, along with Black men, have the smallest associations between mental illness and mental health treatment. Conversely, White women have the highest probability of mental health treatment compared to other race-gender groups, and the lowest probability of arrest. This pattern suggests Black and Hispanic men are disproportionately criminalized for their mental illness compared to other race-gender groups, while White women are most often medicalized. I discuss the implications of these findings and offer suggestions for future research.
Introduction
How does race-gender status influence the likelihood of medical treatment or criminal justice involvement for those with mental illness? With the closure of state mental institutions in the second half of the twentieth century, and insufficient resources to fill the resulting gap in treatment, many individuals with mental illness are at an increased risk of entering shelters, prisons, and jails (Erickson and Erickson 2008; Torrey 2014). Today, it is estimated that 37 percent of prison inmates and 44 percent of jail inmates have been diagnosed with a mental illness, and while budgets vary by state and institution, it has been estimated that incarcerating those with psychiatric disorders costs $15 billion annually (Bao 2020; Bronson and Berzofsky 2017). For those with mental illness, criminal justice involvement does little to improve their well-being or reduce their likelihood of future arrest. Instead, arrest, processing, and incarceration compound stressors and can trigger psychological distress (Massoglia and Pridemore 2015; Sugie and Turney 2017; Turney 2022). This can create a negative, cyclical relationship between criminal justice involvement and mental distress. Furthermore, a criminal record limits access to employment, housing, and other necessary resources (Pager 2003; Sykes and Maroto 2016). Research also shows that police contact is more often life-threatening for those with mental illness, especially for Black men (Fuller et al. 2015; Thomas, Jewell, and Allen 2021).
Nevertheless, not all those who have mental illness find themselves under criminal justice jurisdiction. Individuals with greater social and economic resources still access medical care such as in-patient clinics, counseling, and various forms of outpatient treatment for assistance with symptoms. It is important to understand for whom mental illness is linked with criminal justice involvement, and for whom it is linked with medical care, not only because the extent of this trans-institutionalization from asylum to prison has been debated in the literature (Kim 2016; Steadman et al. 1984), but also because disparities in treatment and in criminal justice contact contribute to disparities in life chances for individuals with mental illness in the United States. Given racial and gender inequalities prevalent in the criminal justice and healthcare systems, it is crucial to understand whether the associations between mental illness, treatment, and arrest vary by race-gender status.
To examine these relationships, I use cross-sectional data on Black, Hispanic, and White men and women from the 2022 wave of the National Survey on Drug Use and Health (U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration [SAMHSA], Center for Behavioral Health Statistics and Quality 2023). Specifically, I assess the association between mental illness and the probability of arrest in the past year versus the probability of mental health treatment in the past year, by race-gender status. My primary goal in this study is to understand how the criminalization and medicalization of mental illness varies by race-gender status (e.g., for Black Women vs Hispanic men). Racial and gender inequalities in criminal justice involvement and mental health treatment can further harm mental health and dampen overall life chances for marginalized groups (Edgemon and Clay-Warner 2018; Sykes and Maroto 2016).
This work provides three key innovations for the research literature in this area. First, this study expands our understanding of the factors that contribute to racial and gender disparities in criminal justice involvement by examining differential associations between mental illness and arrest as a possible mechanism (James and Glaze 2016). Second, this study offers a broader view of the institutional experiences of those with mental illness, by comparing treatment and arrests as outcomes that represent medicalization and criminalization, respectively. The exact effect of the de-institutionalization of asylums on incarceration rates has been debated and this research would show whether certain groups are more likely to have criminal justice involvement, and whether certain groups are more likely to receive medical care (Kim 2016; Steadman et al. 1984). Third, this investigation incorporates an intersectional lens into our understanding of the experiences of those with mental illness by studying substantial sample sizes of different race-gender statuses.
Literature Review
Mental illness affects a little over one in five adults in the United States, a number that has risen in recent years (SAMHSA 2023). Despite being a prevalent condition in the United States, there are significant disparities in the experiences of those with mental illness. Some of the best-known sociological studies of mental illness focus on the forms of institutional social control that arise to manage and make sense of it (see, for example, Conrad 1975; Goffman 1961; Parsons 1951). Within this discussion, social scientists have highlighted medicalization and criminalization as alternative institutional pathways for those with mental illness. Medicalization is the process of “defining a problem in medical terms, usually as an illness or disorder, or using a medical intervention to treat it” (Conrad 2005). Most studies operationalize medicalization by examining the presence of medical treatments and medical definitions for behaviors (Conrad 2013). Similarly, criminalization is the process of defining a problem in criminal or legal terms and using criminal justice intervention to address it (Dvoskin, Knoll, and Silva 2020; Jenness 2004). Many studies operationalize criminalization either through tracing the development of legislation (see, for example, Halfmann 2019) or by examining rates of criminal justice involvement (see, for example, Pager et al. 2022). Whether mental illness is framed as a medical condition or a criminal one results in different outcomes for well-being (Conrad and Schneider 2010; Conrad and Slodden 2013). Medical care such as medication and therapy can reduce distress, increase autonomy, and improve social and financial opportunities (Campbell et al. 2013). Criminal justice involvement, including arrests, negatively impacts financial opportunities and well-being, creating worsened life outcomes for those with mental illness (Maroto and Sykes 2020; Sugie and Turney 2017).
Many scholars have documented the ways mental illness has been understood as criminal or medical (Conrad and Slodden 2013; Dvoskin et al. 2020; Erickson and Erickson 2008). Less is known, however, about whether race-gender status influences the criminalization or medicalization of mental illness. Given the prevalence of racial and gender inequality in the criminal justice and healthcare systems, I expect to find that mental illness may be differentially associated with criminal justice involvement and medical treatment based on one’s race-gender status. I specifically use race-gender status to account for the intersectionality of race and gender in the experiences of stigma, discrimination, and other barriers within both the criminal justice system and the healthcare system. Below, I describe how different forms of race-gender discrimination that influence criminalization and medicalization may influence the association of mental illness, treatment, and criminal justice involvement.
Race-Gender Differences in Criminalization
Critical criminologists have pointed to the important role of the social constructs of race and gender in understanding disparities in criminal justice involvement in the United States. Compared to White individuals, racial minorities are more likely to be stopped, arrested, booked, and incarcerated, with the most severe consequences for men of color (Jones-Brown 2007). Bias in these encounters is not always related to the personal malice of officers or judges toward specific individuals, but rather cultural stereotypes that position Black and minority individuals as criminals (Correll et al. 2007; Jones-Brown 2007; Kovera 2019). For example, Black offenders are less likely to be granted parole than White offenders, and this difference is related to racial biases in professionals’ assessments of psychological and behavioral readiness, rather than individuals failing to demonstrative self-rehabilitation (Young and Pearlman 2022). Racial anxieties also fuel the criminalization of immigration, and the stereotyping of Hispanic individuals as criminal (Gardner and Kohli 2009; Provine and Doty 2011). As a result, Hispanic individuals are more likely to be stopped, arrested, and convicted of a crime, compared to their White counterparts (Lanuza, Petersen, and Omori 2021; Lopez, Livingston, and Center 2009).
Men are also more likely to be arrested and incarcerated than women, and often their criminal charges and recidivism are understood in different ways from women. While rationality historically has been a dominant frame for understanding men’s criminal behavior, women’s behavior is more often understood as stemming from emotional distress, insanity, irrationality, or relationships with offending men (Breheney, Groscup, and Galietta 2007; Chesney-Lind and Pasko 2012; Weare 2013; Wyse 2013). Men may be more likely to receive harsher sentencing than women as a result (Breheney et al. 2007; Spohn and Beichner 2000). In addition, gender differences in socialized behaviors contribute to differences in criminal justice involvement. Men are more likely to commit crimes, including violent crimes, and are more likely to abuse drugs or alcohol than women (Courtenay 2000; Wilkinson et al. 2018; Zimmerman and Messner 2010).
Kimberlé Crenshaw, in her discussion of intersectionality, highlighted that gender inequality cannot be understood absent from racial inequality (Crenshaw 2013). This is particularly true when examining criminalization. For example, Black and Hispanic men are stereotyped as criminal or dangerous (Jones-Brown 2007; Rios 2020), and as a result are more often stopped by police, booked, charged with a crime, incarcerated, and otherwise involved in the criminal justice system than White men (Pierson et al. 2020; Smiley and Fakunle 2016). While Black women are less often viewed through the stereotypes of “thug” or “criminal predator” than Black men, they are often stereotyped as sexually and criminally deviant (Henry 2023; Ritchie and Jones-Brown 2017). In contrast to women of other racial identities, Hispanic women are more likely to be portrayed in media as breaking immigration laws, abusing welfare or social services, and sometimes as gangsters playing subordinate roles (Slakoff 2020).
To explain how these race and gender stereotypes lead to disparities in arrests, the focal concerns literature theorizes that often police experience an overload of non-definitive information in calls. To better process this information, they often rely on a “perceptual shorthand” of clues about dangerousness and blameworthiness from the characteristics of those involved, which opens them to racial and gender biases. Within these situations, mental illness symptoms create more informational dissonance and may generate or reinforce false positives of dangerousness or blameworthiness (Higgins, Vito, and Grossi 2012). This could potentially lead to higher rates of arrest for individuals of certain race-gender statuses who have mental illness. In addition, as arrest can worsen mental distress, and may possibly lead to mental illness, inequality in arrests may lead to inequality of mental illness across race-gender statuses (Jäggi et al. 2016). These perspectives suggest that mental illness may be differentially associated with criminal justice involvement across race-gender statuses.
Race-Gender Differences in Medicalization
Similar to criminalization, race and gender also shape medicalization. White individuals are more likely to have access to mental health treatment, such as psychotherapy (Feagin and Bennefield 2014; Lê Cook et al. 2013), and their behavior is more often portrayed as medical rather than criminal in media reporting (Lindsay and Vuolo 2021). Even mental health diagnostic categories can be influenced by racial bias; for example, racially coded media portrayals of schizophrenia that emerged during the civil rights movement influenced the rates of schizophrenia diagnoses among Black men (Metzl 2010). Such stereotypes and racial “othering” can contribute to racial inequities in mental health diagnosis and treatment (Shifrer and Fish 2020; Thompson, Wilkinson, and Woo 2021).
Women are more likely to use mental health services than are men, and their symptoms are also framed in different ways than mens symptoms (Courtenay 2000; Mirowsky and Ross 1995). Womens mental health has historically been tied to their womanhood. A common example is the case of hysteria, a diagnosis applied almost exclusively to women through the nineteenth century (Tasca et al. 2012). The word hysteria stems from the Greek word for uterus, hystera, as womens nonconforming behavior was originally believed to be a medical condition caused by their wombs wandering their bodies (Tasca et al. 2012). Feminist scholars argue that today, womens bodies are still often framed as deviant in ways that can subject them to greater oversight from the medical system, for better or worse (Kempner 2017; Offman and Kleinplatz 2004; Parens 2013).
Intersectional race-gender statuses represent unique sets of resources, histories, and experiences related to mental illness and treatment. For example, Black men are more likely to experience what has been termed “John Henryism”—the pressure to cope with stress through expending high levels of effort at the expense of their well-being—which contributes to stigma of seeking care (Cadaret and Speight 2018; Robinson and Thomas Tobin 2021). Black women also experience similar pressures to cope with stress and discrimination through what is referred to as “Superwoman Schema,” which is similar to John Henryism but differs in that it includes prioritizing others needs ahead of ones own (Perez et al. 2023). As another example, many Hispanic men experience mental health stigma through the culture of machismo, which emphasizes bravado, physical dominance, and emotional invulnerability as masculine ideals (Lindinger-Sternart 2015; Rastogi, Massey-Hastings, and Wieling 2012; Schmitz et al. 2020). Beyond stereotyping, historic and ongoing discrimination in healthcare has negatively impacted racial minorities in the United States, particularly women of color. As a result, not only do women of color experience poorer quality healthcare, but they are also less likely to pursue care (Burgess et al. 2008; Cuffee et al. 2024). These patterns suggest that mental illness may be less strongly associated with care for some race-gender statuses compared to others.
Medicalization Versus Criminalization of Mental Illness
Healthcare and criminal justice involvement can often overlap, as evidenced by the fact that the largest psychiatric care facilities in the United States are jails (Chang 2018). By examining both medical and criminal justice involvement simultaneously, one is better able to see the broader institutional experience of those with mental illness, as well as inequalities in that experience. For example, Heitzeg (2015) argues that White individuals are typically medicalized, and their deviant behavior more often treated medically. However, within this same racial framework, Black individuals are more often viewed as criminal (Heitzeg 2015). This double standard of medicalizing White individuals while criminalizing individuals of color is evidenced by studies of disruptive behavior in schools (Fish 2022; Ramey 2018) and substance use (Heitzeg 2015; Kerrison 2015; Lindsay and Vuolo 2021). In studies of mental illness, some evidence suggests racial variation in criminalization and medicalization as well. For example, White male defendants are more likely to be identified as having a mental health issue and diverted from incarceration than Black and Hispanic male defendants (Appel et al. 2020; Prins et al. 2012; Schlesinger 2013). Other studies of incarcerated individuals find that Black and Hispanic men and women are often overrepresented among those with mental illness (Appel et al. 2020; Teplin, Abram, and McClelland 1996; Teplin et al. 2002). These findings suggest that in the case of mental illness, Black and Hispanic men are more often involved in the criminal justice system than White men. However, this area of research is often limited in scope to specific cities or counties and limited to either men or women.
Mental illness is a socially stigmatized condition that, when untreated, is associated with greater risks of unemployment, homelessness, substance abuse, suicide, and poor quality of life (National Alliance on Mental Illness [NAMI] 2020; U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality 2020). Clarifying variation in the medicalization and criminalization of mental illness by race-gender status will deepen our understanding of the factors that shape disparities in life trajectories. Furthermore, awareness of these disparities can inform policies to proactively support populations that are more likely to be penalized rather than treated in the case of mental illness.
Hypotheses
This study examines the criminalization and medicalization of mental illness by race-gender status using data from a nationally representative survey. To operationalize criminalization, I rely on past research traditions established by scholars such as Pager et al. (2022) and Ramey (2015, 2018) who use the concepts of discipline or criminal justice contact (e.g., arrest) as evidence for criminalization. Similarly, I rely on past sociological work that operationalizes treatment utilization as a proxy for medicalization (Dollar 2019; Ramey 2018). I consider arrest and treatment utilization as evidence of criminalization and medicalization, respectively. My specific hypotheses are as follows:
Hypothesis 1: Mental illness will be positively associated with being arrested in the past year.
Hypothesis 2: Mental illness will be positively associated with receiving mental health treatment in the past year.
I will further examine each of the above hypotheses by race-gender status to test if these relationships are consistent across race-gender groups. I expect to find that the associations between mental illness, arrest, and treatment will significantly vary across race-gender groups, after controlling for socioeconomic, social, and demographic factors.
Data and Methods
For this study, I use data from the 2022 wave of the National Survey on Drug Use and Health (NSDUH), which is a nationally representative cross-sectional survey administered by the Substance Abuse and Mental Health Services Administration (SAMHSA) to roughly 70,000 individuals across all 50 states. The NSDUH collects data on substance use, health and psychological well-being, criminal justice involvement, and factors that contribute to substance abuse such as youth experiences. This instrument is the most extensive survey which measures mental health treatment, history of arrest, and mental health collected in the United States over recent years. SAMHSA administers this survey primarily to estimate rates of substance use and mental disorder across states and counties across different subpopulations for use by local and federal governments. This survey also includes measures of socioeconomic status, demographics, and family life. Participants were selected using a multistage area probability sampling technique, identifying segments from census blocks from census tracts, spread out within and across all 50 states (Center for Behavioral Health Statistics and Quality [CBHSQ] 2022).
The NSDUH surveys a cross-sectional sample every year since 1971; in this study, I use the most recent wave of data, collected in 2022. 1 In the NSDUH Black and Hispanic individuals are oversampled to provide a stronger understanding of these groups. In addition, adolescents (12–17 years old) and young adults (18–25 years old) are oversampled compared to older age groups. I limit my sample to adults 18 and older who were asked questions related to mental illness, arrest, and healthcare. I also limit my sample to Black, Hispanic, and White men and women. This results in a sample of 39,246 individuals (2,123 Black men, 2,860 Black women, 3,258 Hispanic men, 4,159 Hispanic women, 11,903 White men, and 14.943 White women). 2
Dependent Variables
To operationalize arrest, I use a dichotomous measure of whether the respondent reported being arrested and booked in the past year (1=yes, 0=never arrested and booked). Due to small cell sizes, I include all arrests, regardless of offense type. To operationalize medical care, I use a dichotomous measure of whether the respondent reported mental health treatment in the past year. 3 Only 4 percent of respondents reported both arrest and treatment history in the past year (see supplemental files).
Predictor Variables
A unique benefit to this data is that the NSDUHs measure of mental illness does not rely on whether the participant had previously received a diagnosis from a medical professional, which would be confounded with the dependent variable of mental health treatment. Instead, the NSDUH employs a statistical model, refined using clinical data in 2012, to predict whether adult respondents had serious, moderate, mild, or no mental illness based on their self-reported symptoms and behaviors. In the 2022 NSDUH, adults aged 18 years or older were administered a battery of questions relating to their emotional, mental, and behavioral states. Adults were classified as having Any Mental Illness (AMI) if they had any mental, behavioral, or emotional disorder in the past year of sufficient duration to meet criteria listed in the DSM-5. 4 This category excludes developmental disorders and substance use disorders. This creates a dichotomous variable, where adults expected to have any mental illness based on their answers are coded as “1” and those who are not expected to have mental illness are coded as “0.” 5 Race and ethnicity are measured in the NSDUH as seven discrete categories: White, Black, Native American/Alaska Native, Native Hawaiian/Pacific Islander, Asian, Mixed Race, and Hispanic. I drew from this measure to create a categorical variable with three possible options: Black, Hispanic, and White. Due to small sample sizes, I excluded other designations from the final sample for analysis. Respondents were also asked to identify as either male or female in the survey. From these questions I created six discrete categories: Black men, Black women, Hispanic men, Hispanic women, White men, and White women.
Control Variables
It is expected that mental illness, treatment, and arrest histories are likely influenced by ones age, socioeconomic status, insurance, urbanicity, and social integration (including education, employment, family roles, and religiosity) (Agnew and Brezina 2019; Hirschi 2017; Yang et al. 2019). I include several control variables to account for these factors. Age is measured categorically in the survey. Since young adults (ages 18–25 years) were oversampled, I compare them to older adults by including a dichotomous measure of whether an individual was aged 18–25 years old (1 = yes). I include two variables related to economic resources that influence both the likelihood of arrest and the likelihood of mental health treatment. Income is measured as four ordered categories in the NSDUH: less than $20K, $20K to $50K, $50K to $75K, and over $75K in total annual family income. After running some preliminary analyses, I code each of these categories as its own dummy variable and exclude those above $75K as the reference category. I also include whether the individual had health insurance (1=yes, 0=did not have insurance) and a categorical measure of urbanicity (1=large metropolitan area, 2=small metropolitan area, 3=nonmetropolitan area) as these factors are expected to shape access to treatment.
I included five measures of social integration that would influence the likelihood of arrest and the likelihood of treatment. Education is measured categorically, and I compare those with less than a high school degree to those who graduated from high school, those who have completed some college, and those who graduated from college. Employment status is collected by the NSDUH as nine possible categories, which I collapse into four groups: employed (which includes both full and part time work), unemployed, retired, and otherwise not in the labor force (which includes those who are disabled, students, keeping house, and other). Employed individuals are excluded as the reference group. The third measure of social integration is marital status, measured as four discrete categories: married, single, divorced or separated, and widowed. I omit those who are married as the reference group. The fourth is parenthood, measured as whether the respondent has children living at home (1=yes, 0=does not have children at home). The final measure of social integration is religious attendance. I include both whether the respondent attended religious services in the past year (1=yes, 0=did not attend yearly) and whether the respondent attended at least once a week in the past year, on average (1=yes, 0=did not attend weekly).
Analytic strategy
Since the outcome variables (arrest and treatment history) are both dichotomous, I estimate logistic regression models. Four percent of respondents reported both an arrest and treatment history (see supplemental files). 6 I retain all outliers and use listwise deletion for missing responses.
I aim to see whether the relationship between mental illness and these two outcome variables are different across the race-gender statuses that I have included. I use interaction terms between race-gender status and my measures of mental illness to estimate these relationships. As Black men have the highest reported rates of arrest and the lowest rates of treatment history, they are excluded as the reference category in all models. In the first model, I examine the relationship between mental illness and arrest (see Table 2). In the second model, I examine the relationship between mental illness and treatment (see Table 3). 7 For better ease of interpretation, I present two figures displaying the predicted probabilities of arrest history and of treatment history by mental illness and race-gender status.
Given the unreliability in interpreting the coefficients and p-values of nonlinear models (Breen, Karlson, and Holm 2018; Mize 2019), I use STATAs postestimation command margins to examine the predicted probability of arrest and predicted probability of treatment for each race-gender status with and without mental illness, controlling for the relevant covariates. In addition, I present the Average Marginal Effects (AMEs) between those with and without mental illness (i.e., the difference in probability of arrest (in Table 2) or treatment (in Table 3) for those with and without mental illness in each race-gender group). For example, Table 2 shows that Black men without mental illness have a .177 probability of arrest (column 2), and that Black men with mental illness have a .231 probability of arrest (column 3), all else equal. The difference between these values is .054, and this difference is statistically significant (p < .05) (column 4).
Important to testing my hypotheses is that the associations between mental illness and arrest or treatment are statistically significantly different across race-gender statuses. In other words, that race-gender moderates the relationship between mental illness and arrest, and the relationship between mental illness and treatment. I use second difference testing to calculate these differences and their significance in the final columns of Tables 2 and 3 (labeled “contrasts”). In other words, the reported AMEs indicate the size and the significance of the relationship between mental illness and the dependent variable, and the contrasts indicate for which race-gender statuses these AMEs significantly differ. For example, the difference in arrest by mental illness status for Hispanic men is significantly different from the differences of Black Women, Hispanic women, and White women (Table 2, column 5).
Since I am comparing two models with different outcome variables (arrest and treatment), I use seemingly unrelated estimation to combine stratified models in order to determine the size of these cross-model differences and their significance (see column 4 of Table 4) (Mize, Doan, and Long 2019). I additionally compare whether these cross-model differences are significantly different across race-gender statuses—in other words, whether the difference between the AME of arrest and the AME of treatment are significantly greater for some race-gender groups than others. This information is reported in the final column (“contrasts”) of Table 4.
Results
In Table 1, I present weighted descriptive statistics for my study measures by each race-gender status. 8 Because all variables are categorical or dichotomous, I report percentages. The sample sizes for each race-gender status are listed at the bottom of the table. More men report arrests in the past year than do women, with Black men reporting the highest rates of arrest (26 percent) followed by White men (22 percent). Hispanic women report the lowest rates of arrest (7 percent) (Table 1). White women report the highest rates of mental health treatment utilization (32 percent) followed by White men and Black women (19 percent, both). Hispanic men and Black men (12 percent, both) report the lowest rates of treatment utilization. Almost one in three White women reported answers that qualified them as having any mental illness (28 percent). Hispanic women (24 percent) and Black women (21 percent) also reported higher rates of any mental illness. Black and Hispanic men reported the lowest incidence of any mental illness (18 percent, both) (Table 1). 9
Percentages for All Study Variables by Race-gender Status, Adjusted for Sampling Method.

Note. National Survey on Drug Use and Health (NSDUH) 2022 (N = 39,246).
Asterisks denote significance between Black men (reference category) and other race-gender subsamples at *p < .05.
Includes those with an associate degree.
Includes disabled, keeping house, student, and does not have job for other reasons.
I first ran an analysis without interaction effects (see supplemental files). I find that mental illness is positively, significantly associated with both arrest and mental health treatment, controlling for race-gender status and other covariates. In addition, Black and White men are most likely to be arrested compared to other race-gender statuses, after controlling for mental illness and other covariates. White women are the most likely to be treated, after controlling for mental illness and other covariates.
Table 2 and Figure 1 display the results from the model examining arrest. Generally, men report higher probabilities of arrest than their female counterparts, both among those with mental illness and those without (see Figure 1). Among those without mental illness, Black men have the highest predicted probability of arrest (.177), while Hispanic women have the lowest probability of arrest (.040), all else being equal (see Table 2). Similarly, among those with mental illness, Black men have the highest predicted probability of arrest (.231) while Hispanic women have the lowest probability of arrest (.076) (see Table 2).
Probability of Arrest by Mental Illness and Race-gender status: Marginal Effects of Mental Illness and Differences in Effects of Mental Illness across Race-Gender Status.
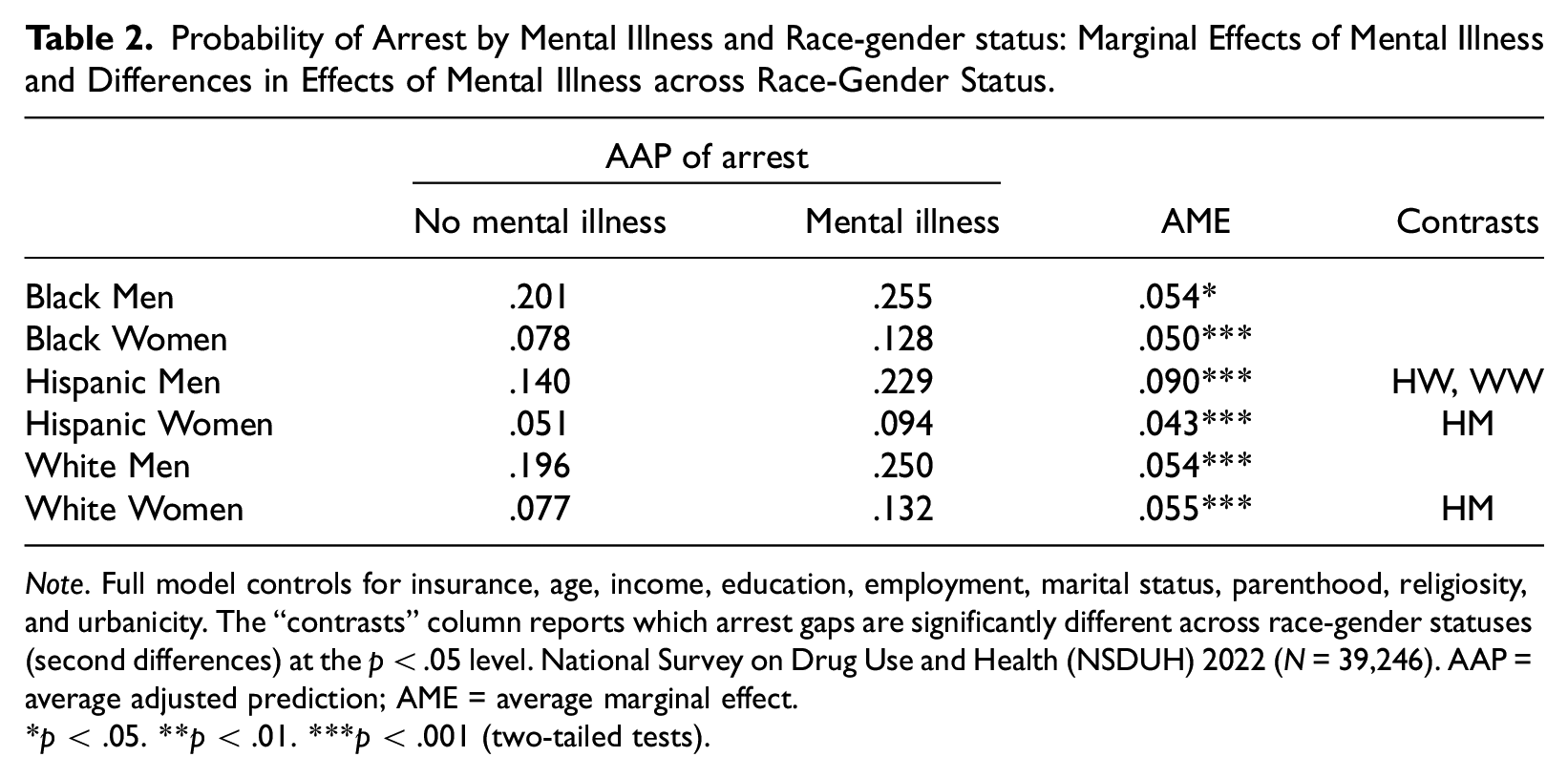
Note. Full model controls for insurance, age, income, education, employment, marital status, parenthood, religiosity, and urbanicity. The “contrasts” column reports which arrest gaps are significantly different across race-gender statuses (second differences) at the p < .05 level. National Survey on Drug Use and Health (NSDUH) 2022 (N = 39,246). AAP = average adjusted prediction; AME = average marginal effect.
p < .05. **p < .01. ***p < .001 (two-tailed tests).
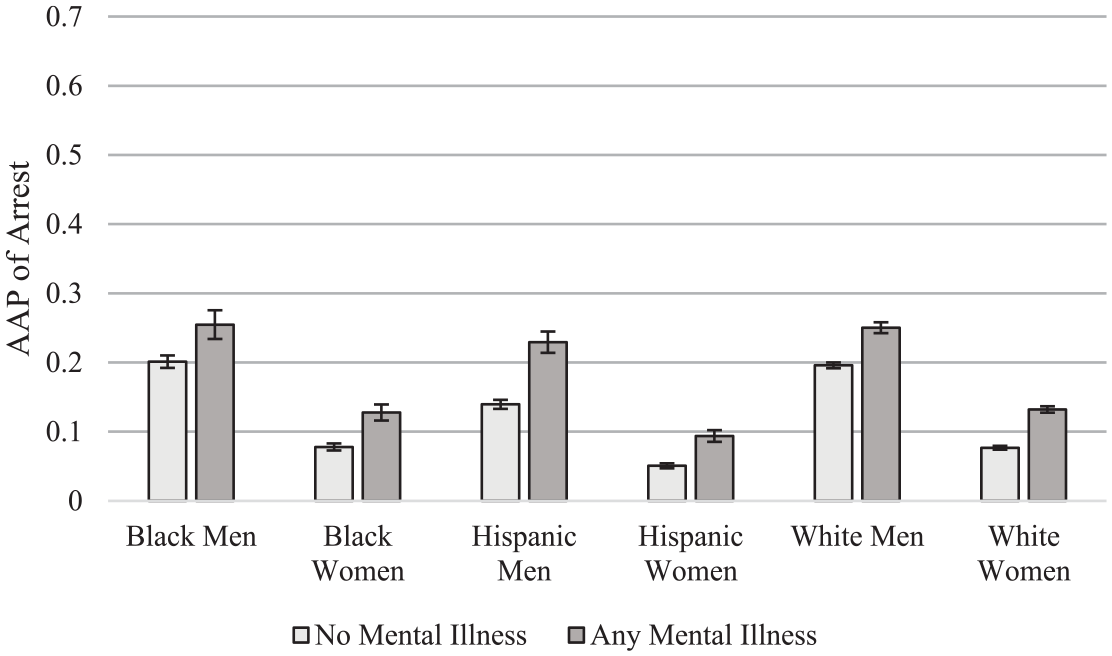
Relationship between mental illness and arrest by race-gender status.
Average marginal effects show that mental illness was significantly associated with an increase in the probability of arrest for all race-gender groups (Table 2, Figure 1). However, the association of mental illness and arrest was significantly greater for Hispanic men than for Black women, Hispanic women, and White men (see Table 2, final column).
Table 3 and Figure 2 display the results from the model examining mental health treatment. Generally, women have higher probabilities of treatment than their male counterparts, both for those with mental illness and those without mental illness. Among those without mental illness, White women have the highest predicted probability of reporting mental health treatment (.221), all else equal. Hispanic men have the lowest probability of reporting mental health treatment (.077), followed closely by Black men (.079) (see Table 3). Among those with mental illness, White women have the highest predicted probability of treatment (.663) and Black men have the lowest predicted probability of reporting treatment (.261), all else being equal (see Table 3).
Probability of Treatment by Mental Illness and Race-gender status: Marginal Effects of Mental Illness and Differences in Effects of Mental Illness across Race-Gender Status.
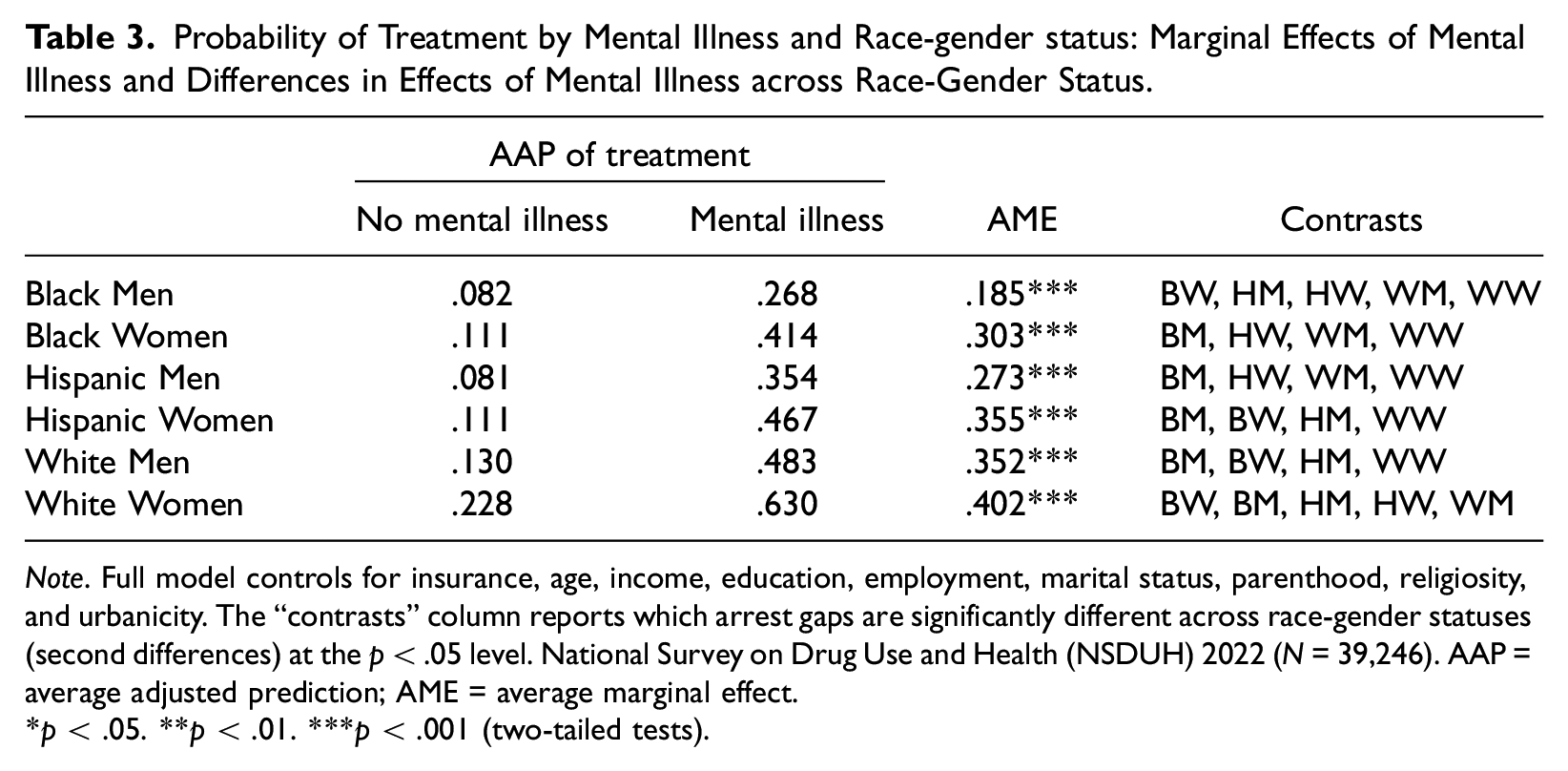
Note. Full model controls for insurance, age, income, education, employment, marital status, parenthood, religiosity, and urbanicity. The “contrasts” column reports which arrest gaps are significantly different across race-gender statuses (second differences) at the p < .05 level. National Survey on Drug Use and Health (NSDUH) 2022 (N = 39,246). AAP = average adjusted prediction; AME = average marginal effect.
p < .05. **p < .01. ***p < .001 (two-tailed tests).
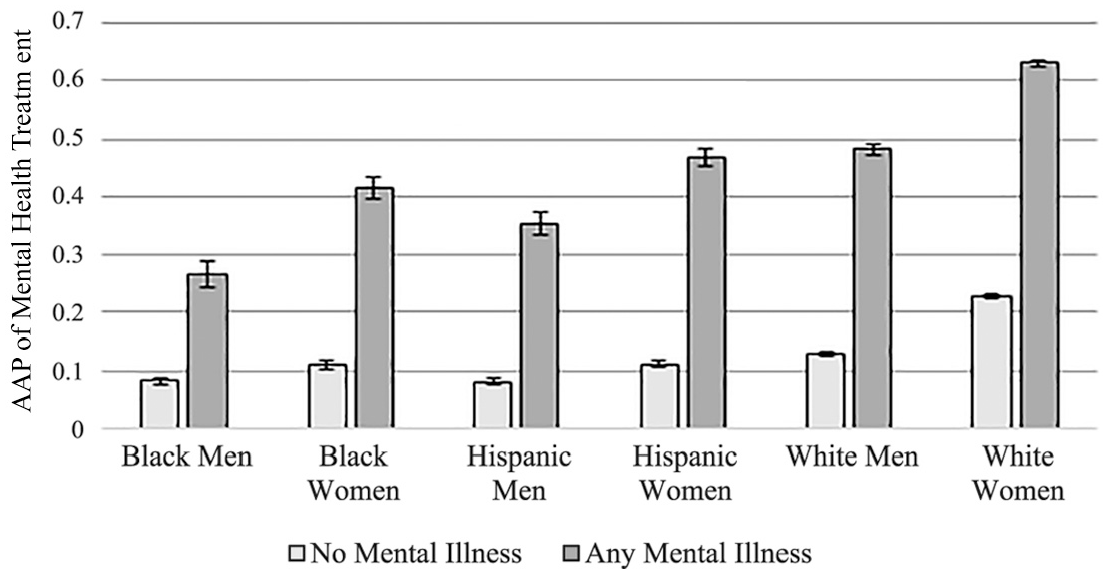
Relationship between mental illness and mental health treatment by race-gender status.
Average marginal effects show that not surprisingly, for all race-gender groups, those with mental illness are statistically significantly more likely to have reported mental health treatment than those without mental illness (see Table 3). However, tests of second differences show significant variation in the size of the average marginal effects across race-gender groups. The association between mental illness and mental health treatment was the greatest for White women compared to all other groups, followed by White men and Hispanic women who were not significantly different from each other but were significantly greater than Hispanic men, Black women, and Black men. The average marginal effects of Hispanic men and Black women were not significantly different from each other and represent the second-to-smallest association. The average marginal effect for Black men was significantly smaller than all other race-gender groups, meaning that the difference in probability of treatment between those with and without mental illness is smallest for Black men (see Table 3).
In Table 4, I present a comparison of the average marginal effects between these two models using SUEST. For all race-gender groups, the association between mental illness and treatment is significantly greater than the association between mental illness and arrest. However, this difference is significantly smaller for Black men than for Black women, Hispanic women, or White women. As Black men have high probabilities of arrest but low probabilities of treatment, the difference in probabilities of treatment is only .128 greater than the difference in probabilities of arrest. Similar patterns are found for Hispanic men. On the contrary, for White women, the difference in probability of treatment is .363 greater than the difference in probabilities of arrest (see Table 4), which is significantly greater than the cross-model differences of Black men and Hispanic men. White men, though they have higher rates of arrest and lower rates of treatment than White women, exhibit statistically similar cross-model differences to White women (.301). Hispanic women report larger cross-model differences compared to Hispanic men (.322), in other words, Hispanic women are far more likely to get treatment than to be arrested compared to their male counterparts.
Average Marginal Effects of Mental Illness on Arrest and Treatment by Race-gender Status.
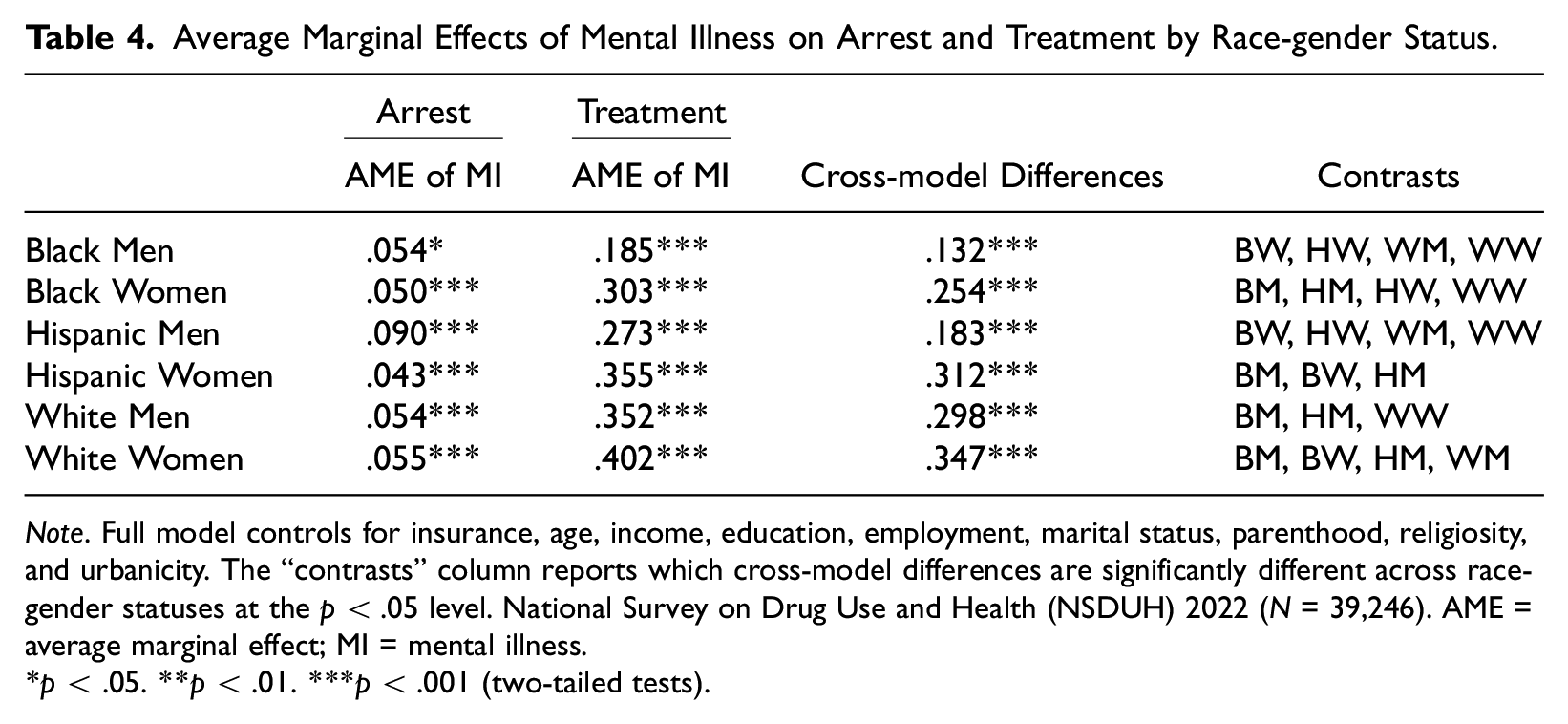
Note. Full model controls for insurance, age, income, education, employment, marital status, parenthood, religiosity, and urbanicity. The “contrasts” column reports which cross-model differences are significantly different across race-gender statuses at the p < .05 level. National Survey on Drug Use and Health (NSDUH) 2022 (N = 39,246). AME = average marginal effect; MI = mental illness.
p < .05. **p < .01. ***p < .001 (two-tailed tests).
Discussion
Mental illness is positively associated with arrest and treatment for all race-gender groups, however, the results show race-gender variation in the experience of criminal justice involvement and mental health treatment. White individuals are more likely to report mental health care than their Black and Hispanic counterparts; and Black individuals are more likely to report arrests than their White counterparts. This mirrors a pattern found in other studies (see, for example, Heitzeg 2015; Ramey 2018) which suggests that White individuals are more often medicalized while Black and Hispanic individuals are more often criminalized in the case of mental illness. In examining race-gender status, however, the pattern of racial inequality in treatment and arrests becomes more complex. Black, Hispanic, and White women are less likely to report arrests than their male counterparts, and are more likely to report treatment than their male counterparts. White women were the most likely to report treatment, even when their responses were not sufficient to be classified as mental illness in the survey. White women report the greatest cross-model differences; in other words, they report a much greater association between mental illness and treatment than between mental illness and arrest relative to other groups. This result is consistent with research by feminist scholars that has shown the medicalization of womens mental health (Tasca et al. 2012; Ussher 2010). However, Black (and to a lesser extent, Hispanic) women do not follow the same patterns as White women. Black women report arrests at similar rates to White women both among those with and without mental illness, and Hispanic women report arrests at the lowest rates of either those with or without mental illness. This gives women of all racial/ethnic groups a statistically similar association between mental illness and arrest. However, Hispanic women report a lower association between mental illness and treatment than White women, and Black women report an even lower association between mental illness and treatment than either Hispanic or White women.
That Black women receive less medical support than White or Hispanic women is consistent with past literature on their intersectional experience within healthcare. Black women have experienced high rates of discrimination in both psychiatry and healthcare as a whole (Conteh et al. 2022; Washington 2006). For example, stereotypes, such as the stereotype of the “angry Black woman,” can distort how Black womens mental distress is perceived. When Black women are presumed to be irate, hostile, and aggressive, their legitimate emotional expressions are more likely to be misinterpreted and invalidated by psychiatric professionals and by others (Ashley 2014). Such discrimination contributes to a general distrust of psychiatric care among Black women (Kokaliari, Roy, and Taylor 2019; Nelson, Shahid, and Cardemil 2020). These new findings raise the concern that not only are Black women less likely to access care, but they are also more likely to have been arrested if they have mental illness, compared to women of other ethnicities.
While men have greater probabilities of arrest and lower probabilities of treatment than their female counterparts, this also varies by race/ethnicity. White men and Black men report similar associations between mental illness and arrest (.055 and .054 respectively). Although Black men report the highest probabilities of arrest of all race-gender groups with mental illness, they also report a high probability of arrest without mental illness, which somewhat diminishes the size and significance of the relationship between mental illness and arrest. As previously discussed, Black men are hyper-criminalized relative to White men (Jones-Brown 2007), and this appears to be the case regardless of mental illness. Hispanic men follow a different pattern, however; among those without mental illness, Hispanic men have very low probabilities of arrest. Among those with mental illness, Hispanic men report very high probabilities of arrest. This creates a statistically greater relationship between mental illness and arrest than other groups. Studies of Hispanic and Latino men show that–like Black men–they are at greater risk of criminal justice involvement due to racial biases (Rios 2020). This finding suggests that either the risk of criminal justice involvement is greater among those with mental illness (as would be posited by focal concerns research), or that this involvement generates greater mental distress and disorder among Hispanic men compared to other race-gender groups, such as Hispanic women. This second possibility would be unexpected as past research has found women typically report worse psychological distress resulting from arrest or incarceration compared to men (Crewe, Hulley, and Wright 2017; Turney 2021).
In addition, Hispanic men report very low associations between mental illness and mental health treatment, second only to Black men. This suggests that Hispanic men are at greater risk of criminal justice involvement relative to medical treatment when experiencing mental illness. This is reflected in the small cross-model differences in Table 4. In investigating the literature for evidence of why Hispanic men would experience such a large association between mental illness and arrest, I found evidence of an interesting pattern. Within the criminal justice system, Hispanic men are less likely to receive mental health treatment. For example, in a study of the Los Angeles County jail system, Hispanic men were overrepresented among those incarcerated but underrepresented in mental health diversion programs, and this was not attributable to differences in rates of mental illness (Appel et al. 2020). In general, being Hispanic and being male is associated with a lower likelihood of utilizing mental health services among those involved in the criminal justice system, although this is also true of Black men in many studies (Baglivio et al. 2017; Rawal et al. 2004; Teplin et al. 2002). Cultural differences between US residents and Hispanic immigrants are offered as a possible explanation; in essence, that Hispanic men may be less able to access psychiatric services due to cultural and linguistic barriers (Appel et al. 2020). I attempted to test this relationship using English language speaking ability as a measure of linguistic barriers, but found it was not significant. In addition, it is unlikely that language barriers would affect only Hispanic men but not Hispanic women. It is possible, however, that stereotypes surrounding Hispanic masculinity (i.e., machismo) may influence Hispanic mens expression of distress, their treatment-seeking behavior, and the perception of their symptoms as criminal or medical by institutional actors (Rastogi et al. 2012; Schmitz et al. 2020). Given that this study does not account for such perceptions, there is an opportunity for more robust theorizing in explaining the unique experiences of Hispanic men with mental illness in the criminal justice system.
Although I did not find a strong relationship between mental illness and arrest among Black men, overall, Black men with mental illness have the highest probability of an arrest history of any race-gender group regardless of mental health status. In addition, Black men have the smallest association between mental illness and mental health treatment. While White women appear to be the most medicalized, Black men appear to be the least medicalized, in the sense that they are least likely to report medical treatment. Alongside literature that describes the criminalization of Black men, this finding highlights a potential need not only for the de-criminalization of Black men but for greater efforts to provide high-quality, supportive care to Black men with mental illness.
To explore the mechanisms that mediate the relationship between mental illness and arrest, I turn to literature on mental illness and deviant behavior. Mental illness is often associated with higher risk-taking behaviors and greater rates of substance abuse, both of which can increase risk of criminal justice involvement (Pollak et al. 2019; Turner et al. 2018). Supplemental analyses suggest that substance use and risk-taking partially explain the relationship between mental illness and arrest, particularly for Black and Hispanic men and women, but not for White men and women (analyses available upon request). This correlates with research that finds racial inequality in the criminalization or medicalization of substance abuse (Lindsay and Vuolo 2021). Such a finding would suggest that the relationship between mental illness and arrest may be facilitated through a racially unequal system of criminalizing substance use. Future research should examine this possible mechanism.
Beyond substance use, the relationship of mental illness to criminal offenses is more complex. The majority of people who have mental illness do not commit violent crimes, and the majority of violent crimes are not committed by people with mental illness (Glied and Frank 2014). However, supplemental analyses suggest that self-reported criminal behaviors such as selling drugs may explain the relationship between mental illness and arrest for Black men only (available upon request). Future research is needed to explore whether mental illness influences the likelihood of non-violent deviant offenses, and whether these offenses are more likely result in arrest for Black men with mental illness than other groups.
This study is not without limitations, some of which I describe here. First, the NSDUH data are cross-sectional and ask individuals to self-report their experiences in the past year. The direction of the relationship may possibly be reversed, most plausibly in the case of arrest. Longitudinal studies suggest a cyclical relationship between criminal justice involvement and mental illness (see, for example, Semenza and Silver 2022). More longitudinal research is needed to examine the effect of mental illness on arrest and treatment over time for individuals of different race-gender statuses. Second, as these measures are self-reported, they are subject to recall bias and social desirability bias. The true rates of treatment and arrest may be, in fact, higher, and these presented results are likely conservative estimates of the rates of treatment and arrest.
Third, this study is limited to two specific measures of institutional interaction along a wide continuum of care and experiences for those with mental illness (Hirdes et al. 2020). Due to small cell sizes, this study examines arrest and mental health treatment separately, without separating out those who experienced both (4 percent). Past research finds that care provided within a context of policing can reduce the effectiveness of the care, and that Black and Hispanic individuals are more likely to be ordered care than seek treatment voluntarily (Alang and McAlpine 2019; Nichols and Malenfant 2022). Given that the criminal justice system provides care for over a million individuals with mental illness (Bronson and Berzofsky 2017), future research should examine whether pathways to care (treatment courts, incarceration, doctor referrals, or voluntary healthcare routes) vary by race-gender status. This analysis specifically focuses on being arrested, but other forms of criminal justice involvement such as probation, incarceration, and parole should be examined in future work as these represent additional steps along the pathway to incarceration where those with mental illness could be re-routed to supportive care (Heilbrun et al. 2015). The NSDUHs measure of arrest includes those who have been booked rather than released, and future work should examine booking separately from arrest. This study uses self-reported symptoms of mental illness, rather than formal diagnoses. The diagnostic process in and of itself is a step along the trajectories of those with mental illness that should be examined further.
Fourth, this study uses a broad measure of mental illness, which may obscure race-gender variation in symptoms and behaviors. For example, some studies find that men more often externalize symptoms of their distress than do women, which could explain some of the gender variation in arrests (Simon 2020). Race-gender variation in specific symptoms and specific diagnostic categories should be examined in future work.
Fifth, I limited my analyses to racial and ethnic groups for which I had substantial sample sizes, but Asian, Pacific Islander, and Native American individuals have unique experiences and histories within the criminal justice and healthcare systems (Baluran 2022; Findling et al. 2022; Hu and Esthappan 2017; Tighe 2014). Future studies should examine how mental illness may be medicalized or criminalized for these communities. Finally, I assume gender identity based on the indicated sex of the individual, as this survey is limited to the discrete categories of “male” and “female.” Gender and sexual minorities are not examined in this study but are at particular risk for mental distress and are overrepresented in the criminal justice system (Argüello 2020). Even cisgender individuals can express their gender in different ways that hold different social meanings in the interaction between patient and doctor, or citizen and state.
Conclusion
Those with mental illness are more likely to be arrested and incarcerated, which negatively impacts their ability to pursue employment, apply for services such as public housing, and otherwise support themselves (Pager 2003). Furthermore, the many experiences that make up criminal justice involvement (e.g., arrests, sentencing, and incarceration) all have documented, severe consequences for mental health (Edgemon and Clay-Warner 2018; Sugie and Turney 2017; Turney 2021). The current study highlights that race-gender status matters in shaping the institutional trajectories of those with mental illness. I find evidence for gender differences in the criminalization and medicalization of mental illness, specifically that women report greater probabilities of treatment than arrest if they have mental illness. But exploring this relationship by race and ethnicity offers us a more complex picture. Rather than seeing that women are all equally likely to be medicalized, I find that White women have an advantage in accessing those resources. I also find evidence suggesting Hispanic and Black men are at greater risk of criminalization than other race-gender statuses.
These findings offer theoretically fruitful avenues for future study. Efforts should be made to better understand the factors contributing to Hispanic mens institutional trajectories with regards to mental illness. If cultural differences play a role as others have speculated (Appel et al. 2020; Rawal et al. 2004), then the specific elements of culture that act as a barrier or mechanism need to be identified. These identified differences would also need to be tested against the cultural assumptions/stereotypes of normative and nonnormative behavior associated with Hispanic persons by the dominant culture within the United Status. Additional research is also needed to understand the ways in which Black and Hispanic women with mental illness experience criminalization in the United States context in ways distinct from men, and the factors that prevent Black and Hispanic women with mental illness from receiving supportive, high quality, mental health treatment. It is possible that these gaps may be greatest under specific state policy contexts, which is not explored in this study. Finally, more research is needed to examine the role of substance use and other deviant behaviors as mediators in the relationship between mental illness, criminal justice involvement, and mental health treatment, and how these mechanisms vary by race-gender status.
Supplemental Material
sj-docx-1-smh-10.1177_21568693251335336 – Supplemental material for Race-gender Disparities in the Criminalization and Medicalization of Mental Illness
Supplemental material, sj-docx-1-smh-10.1177_21568693251335336 for Race-gender Disparities in the Criminalization and Medicalization of Mental Illness by Meagan Rainock in Society and Mental Health
Footnotes
Acknowledgements
I would like to thank the anonymous reviewers for their time and expertise, and Drs Andre Christie-Mizell, Evelyn Patterson, Jonathan Metzl, Dan Cornfield, and Velma McBride Murry for their valuable feedback and support.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.