
Abstract
Although researchers have consistently linked structural neighborhood disadvantage with poorer mental health, they continue to search for underlying mechanisms. In this article, we test whether the association between structural neighborhood disadvantage and psychological distress is mediated by perceived neighborhood disorder and divine struggles. Using longitudinal national survey data from the Midlife in the United States (MIDUS 2 and 3) study (n = 2,083), we employed structural equation modeling and marginal models with unstructured covariances. Our mediation analysis confirmed the indirect effect of neighborhood structural disadvantage (concentrated socioeconomic disadvantage) on psychological distress (depression and anxiety) through perceived neighborhood disorder (perceptions of neighborhood safety and the built environment) and divine struggles (strained relations with God). Our analyses build on previous work by demonstrating that divine struggles may play a role in explaining why living in a neighborhood that is characterized by structural disadvantage and disorder is often associated with poorer mental health.
Introduction
For decades, studies have shown that residents of structurally disadvantaged neighborhoods, especially neighborhoods characterized by concentrated socioeconomic disadvantage, tend to exhibit poorer mental health (e.g., higher levels of anxiety, depression, and nonspecific psychological distress) than residents of neighborhoods that are more structurally advantaged (for reviews and meta-analyses, see Barnett et al. 2018; Hill and Maimon 2013; D. Kim 2008; Mair, Diez Roux, and Galea 2008; Richardson et al. 2015; Sui, Ettema, and Helbich 2022). Although previous research suggests that neighborhood disadvantage may undermine the mental health of residents by fostering chronic social stressors (e.g., neighborhood disorder), social disintegration (e.g., mistrust and social isolation), self-conceptions that are pessimistic and fatalistic (e.g., low self-esteem and low sense of control), and risky health-related behaviors (e.g., sleep disturbance and heavy drinking) (Hill and Maimon 2013; Huang et al. 2020; D. Kim 2008; Mair et al. 2008), Hill and colleagues (2024) argue that our understanding of neighborhood context could be advanced by further integration with the sociology and psychology of religion. In this article, we build on previous work by using national survey data from the Midlife in the United States (MIDUS) study to test the indirect effect of concentrated structural neighborhood disadvantage on psychological distress through perceived neighborhood disorder and divine struggles.
Mediation Model
Figure 1 presents our proposed mediation model, which synthesizes three propositions: (1) neighborhood structure shapes neighborhood experience, (2) neighborhood experience shapes religious experience, and (3) religious experience shapes emotional experience. Our model is informed by the stress process framework for documenting how socially patterned stressors undermine mental health (Aneshensel and Avison 2015; McLeod 2012; Pearlin 1989; Thoits 1995). The stress process has three essential components. The first component of the stress process is social context. According to Jane D. McLeod (2012:176), social context “encompasses structures—stratification systems, historical circumstances, and other macro-social processes such as capitalism and deindustrialization—as well as cultures—ideologies, traditions, and commonsense assumptions.” In our mediation model, we conceptualize social context as structural neighborhood disadvantage, which we operationalize with census tract indicators of per capita income, poverty rate, unemployment rate, percentage of households receiving public assistance, percentage of adults aged 25 or older without a high school diploma, and the percentage of female-headed households (Mirowsky and Ross 2003).
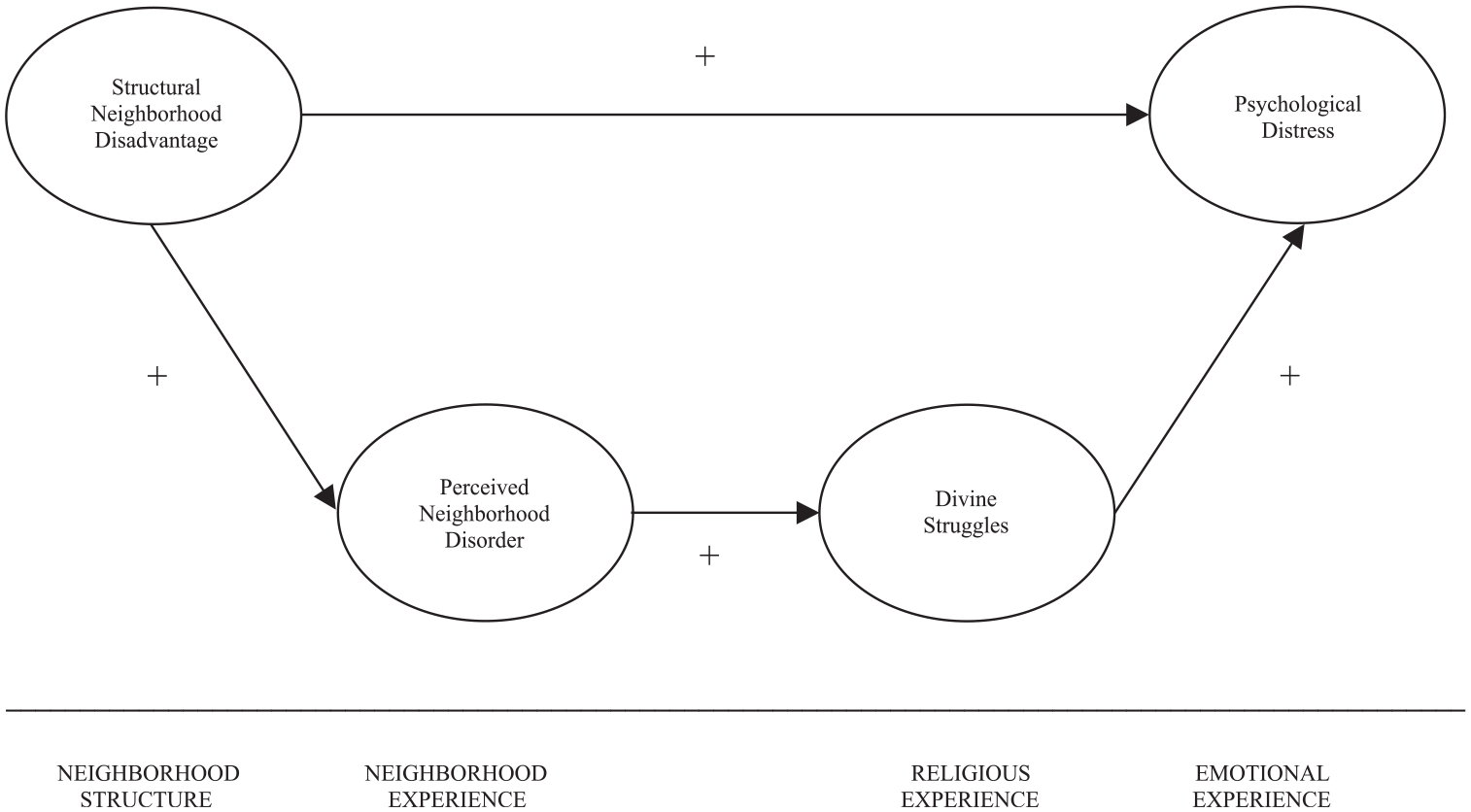
Theoretical model of the indirect effect of structural neighborhood disadvantage on psychological distress.
The second component of the stress process model specifies a social stressor, a taxing life event, or chronic strain that can be “traced back to surrounding social structures and people's locations within them” (Pearlin 1989:242). Our mediation model conceptualizes social stress as the “ambient” chronic strain of perceived neighborhood disorder, which we operationalize as an index of social disorder (perceptions of neighborhood safety) and physical disorder (perceptions of the neighborhood built environment). Leonard Pearlin (1989:246) explained that “residing in neighborhoods where there is reason to fear crime or violence” is “among the ambient strains that cut across roles and envelop people.”
Following previous research, our mediation model suggests that the primary mechanism through which structural neighborhood disadvantage tends to undermine mental health is through the production of objective conditions of neighborhood disorder and, as a consequence, personal subjective experiences with physical and social disorder (Aneshensel and Sucoff 1996; Blair et al. 2014; Fong et al. 2019; Hill and Maimon 2013; Jakobsen et al. 2022; Joshi et al. 2017; D. Kim 2008; J. Kim 2010; Kowitt et al. 2020; Ross 2000). While physical neighborhood disorder refers to the state or appearance of the built environment (e.g., trash on sidewalks and streets, overgrown lots, buildings that are in disrepair or abandoned, and other signs of neglect), social neighborhood disorder refers to the quality of the sociocultural environment (e.g., strained interactions and relationships with neighbors, crime, violence, drinking and drug use in the open, and other cues that may be perceived as dangerous or threatening) (Ross and Mirowsky 1999; Skogan 1990). Researchers have long theorized and demonstrated that structural neighborhood disadvantage tends to support and sustain the conditions of neighborhood disorder by limiting the resources (e.g., lower tax bases and capital investments and scarcity of institutional assets and public services), opportunities (e.g., limited prospects for status attainment through formal education and employment), and social organization (e.g., social disintegration within neighborhoods and social isolation from more advantaged neighborhoods) of communities (Massey and Denton 1993; Sampson and Groves 1989; Schieman and Pearlin 2006; Shaw and McKay 1942; Wilson 1987). Catherine E. Ross (2000:1985) argued that “all of the impact of living in a disadvantaged neighborhood on psychological well-being is mediated by perceptions of disorder in the neighborhood” because “residents in these neighborhoods face a threatening environment characterized by crime, incivility, and harassment, which they find distressing.”
The third component of the stress process specifies psychosocial mediators and moderators that, respectively, explain and condition any underlying associations between social stress and mental health. Although the stress process literature has traditionally highlighted psychosocial processes related to self-esteem, mastery, and social support (Aneshensel and Avison 2015; Pearlin 1989; Thoits 1995), prominent scholars have made compelling arguments for incorporating indicators of religious experience (e.g., religious beliefs, cognitions, and behaviors) into mainstream sociology of mental health research. For example, Christopher G. Ellison and Andrea K. Henderson (2011:37) maintained that by “building upon the core constructs and models of the `stress process’ tradition and integrating them with findings from other relevant fields, social scientists can make vital contributions to our understanding of the complex relationships between religion and mental health outcomes.”
Schieman, Bierman, and Ellison (2013:473) also noted that it is important to “integrate theoretical and empirical insights from both the sociological study of religion and the sociological study of mental health.”
Our model points to the mediating influence of religious struggles because this concept represents a unique facet of the religious experience that captures psychosocial “tension and conflict about sacred matters within oneself, with others, and with the supernatural” (Stauner et al. 2016:1). Along these lines, Exline and colleagues (2014) described three general dimensions of religious struggles, including (1) the interpersonal, (2) the intrapersonal, and (3) the divine. Interpersonal struggles are religion-based conflicts with family, friends, and other relations within one's religious group or community. Intrapersonal struggles are intrapsychic battles with one's own internalized morality standards, religious doubts, and quest for meaning and purpose. Divine struggles, the focus of subsequent analyses, refer to ominous beliefs about or strained relationships with God, the Devil, and other supernatural powers or evil spirits.
With this conceptualization in mind, our mediation model suggests that neighborhood disorder could undermine mental health by contributing to the experience of divine struggles. This portion of our model integrates research from the psychology of trauma and the psychology of religion. Over 30 years ago, Ronnie Janoff-Bulman (1992) argued that stressful or traumatic conditions in life, especially those that threaten “survival” and “abandonment,” are generally devastating to mental health because these conditions often call into question three fundamental assumptions that people make about the world and self. The first assumption is that “the world is benevolent” (i.e., a good place filled with good people). The second assumption is that “the world is meaningful” (i.e., understandable, predictable, and just). The last assumption is that the self is worthy (i.e., moral and competent). When these assumptions are challenged by extreme adversity, people tend to experience chronic emotional distress because they come to realize (1) that their “deeply accepted” conceptual system “is in a state of upheaval and disintegration” and (2) that their “survival is no longer secure, that their self-preservation can be jeopardized in a world that is frightening and unsafe” (Janoff-Bulman 1992:64).
Integrating Ronnie Janoff-Bulman’s (1992) psychology of trauma with the psychology of religion, Gina Magyar-Russell and Kenneth Pargament (2006:102) explained that “. . . negative life events, loss, and trauma often shatter previously held assumptions about the benevolence, fairness, and meaningfulness of the world,” and, for many, “this shattering of assumptions extends to the spiritual dimension of their lives.” Indeed, several studies have linked religious struggles with a range of social strains, including adverse financial difficulties, discrimination, the outcomes of presidential elections, disability, health conditions, and other stressful or traumatic life events (Ai et al. 2010; Ellison and Lee 2010; Exline et al. 2011; Exline et al. 2023; Fitchett et al. 2004; Hill et al. 2017; Koenig, Pargament, and Nielsen 1998; Krause and Hayward 2012; Krause, Pargament, and Ironson 2017; Pargament et al. 1998; Stauner et al. 2019; Wortmann, Park, and Edmondson 2011). While people often turn to religion for guidance and comfort to cope with adversity, others turn away from their faith and deeply held religious beliefs when they can no longer make coherent religious meaning in their lives. The chronic stress associated with perceiving neighborhood disorder could conceivably contribute to divine struggles by challenging core religious beliefs and raising existential questions about the benevolence of God, fairness in the world that is bestowed on the faithful, and the sense of meaning that accompanies religious devotion (Hill et al. 2024).
Although most studies of religion and health underscore potential health benefits (Koenig, VanderWeele, and Peteet 2024), a growing body of research has linked various indicators of religious struggles (e.g., religious doubts, strained divine relations, and negative religious coping) with poorer mental health (e.g., anger, anxiety, depression, and suicidal ideation) (Bockrath et al. 2022; Cowden et al. 2022; Ellison and Lee 2010; Hill et al. 2017; Hill et al. 2021; Pargament et al. 2004; Park, Wortmann, and Edmondson 2011; Silton et al. 2014; Upenieks 2021, 2022; Wilt, Exline, and Pargament 2022). The most common explanations for why religious struggles tend to undermine mental health emphasize unique stress processes associated with “intrapsychic” strains (e.g., nagging reservations about matters of faith and perceived moral or spiritual injustice) and the loss of psychosocial resources (e.g., social support, identity, self-esteem, and meaning in life) that stem from interpersonal (e.g., strained relationships and ideological divisions within religious communities), intrapersonal (e.g., internalization of stigma associated with deviating from religious norms), and divine (e.g., the loss of security and coherence from strained divine relations) struggles (Ellison and Lee 2010; Exline 2002; Hill et al. 2021; Magyar-Russell and Pargament 2006; Upenieks 2021).
In support of our proposed mediation model, Hill and colleagues (2024) recently reported consistent indirect effects of perceived neighborhood disorder (e.g., perceptions of crime and the built environment) on anger, nonspecific psychological distress (depression and anxiety), sleep disturbance, poorer self-rated health, and shorter subjective life expectancy through the experience of religious struggles (e.g., religious doubts and strained relations with God). Although Hill and colleagues (2024) clearly advanced our understanding of the indirect effects of perceived neighborhood disorder on mental health (neighborhood disorder → religious struggles → mental health), this model is likely endogenous to the omission of objective neighborhood structure. The current analysis incorporates neighborhood structure by testing the indirect effect of structural neighborhood disadvantage on psychological distress through perceived neighborhood disorder and divine struggles (neighborhood disadvantage→ neighborhood disorder → divine struggles → mental health). Our proposed theoretical model represents a more comprehensive and multilevel assessment of the indirect effects of neighborhood context on mental health.
Data
We employ data from the MIDUS study to test our proposed mediation model. MIDUS used computer-assisted telephone interviews and self-administered questionnaires to collect longitudinal data from a national probability sample of American adults. MIDUS 1 was conducted in 1995 and 1996 (n = 7,108) and produced an overall response rate of 60.8 percent (Brim, Ryff, and Kessler 2004). MIDUS 2 was conducted in 2004 and 2005 (n = 4,963) and retained 70 percent of the MIDUS 1 sample (Radler and Ryff 2010). Finally, MIDUS 3 (n = 3,293) was conducted in 2013 and 2014 and retained 46 percent of the MIDUS 1 sample (Liang 2024; Song et al. 2021). Our final analytic sample includes 2,083 adults who participated in MIDUS 2 and 3. Our sample includes all respondents from MIDUS 2 who also participated in MIDUS 3 (see Supplemental Attrition Analyses). We did not use MIDUS 1 in our main analysis because the timing of the measurement of neighborhood structural disadvantage was closer to MIDUS 2. Our access to geographically matched census tract–level characteristics was limited to the 2006–2010 American Community Survey five-year estimates.
Measures
Psychological Distress
Psychological distress is a latent variable indicated by six items drawn from the K6 Psychological Distress Scale (Kessler et al. 2002). Respondents were asked to indicate how often in the past 30 days they felt: (1) nervous, (2) restless or fidgety, (3) so sad nothing could cheer them up, (4) hopeless, (5) everything was an effort, and (6) worthless. Response categories for these items range from (1) none of the time to (5) all the time so that higher index scores would indicate greater psychological distress. Table 1 presents our final standardized factor loadings for all latent variables. In our analyses, we retained items with standardized factor loadings that equal or exceed 0.40 (Gana and Broc 2019). The six psychological distress items produced a single factor with standardized loadings ranging between 0.71 and 0.89. Given that the threshold for McDonald's omega is 0.70 (Gana and Broc 2019), our reliability analysis also suggested excellent internal consistency for six items in MIDUS 2 (ω = 0.85) and MIDUS 3 (ω = 0.86).
Final Standardized Factor Loadings for All Latent Variables.
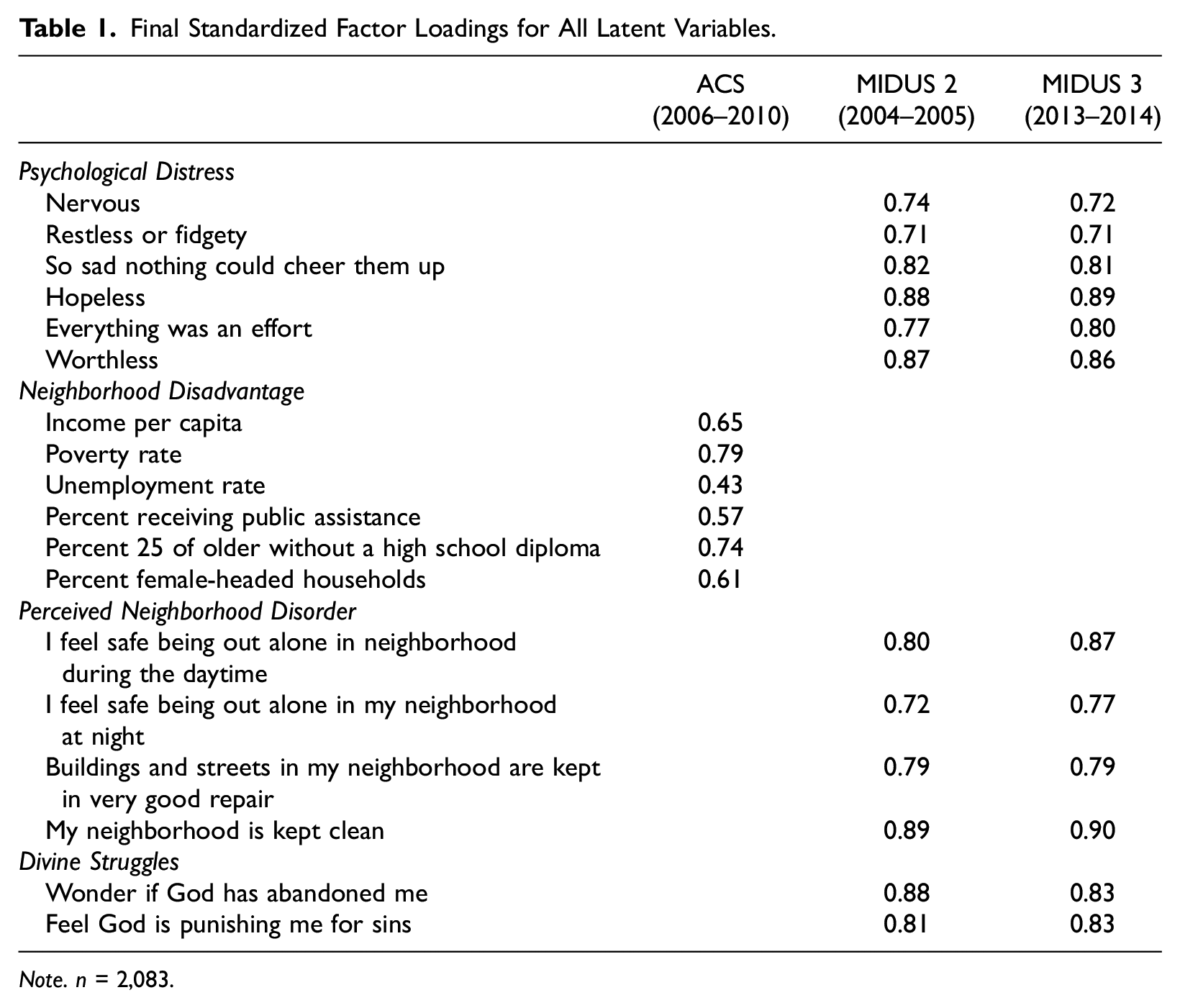
Note. n = 2,083.
Structural Neighborhood Disadvantage
Structural neighborhood disadvantage is a latent variable indicated by five-year census tract estimates from the American Community Survey (2006–2010), including (1) income per capita (reverse-coded), (2) poverty rate, (3) unemployment rate, (4) percentage of households receiving public assistance, (5) percentage of adults aged 25 or older without a high school diploma, and (6) percentage of female-headed households with children (Arcaya et al. 2016; Mirowsky and Ross 2003). The six structural neighborhood disadvantage items produced a single factor with standardized loadings ranging between 0.43 and 0.79. Reliability analysis also suggested adequate internal consistency for six items (ω = 0.78).
Perceived Neighborhood Disorder
Perceived neighborhood disorder is a latent variable that was measured with four indicators of social and physical disorder: (1) I feel safe being out alone in my neighborhood during the daytime, (2) I feel safe being out alone in my neighborhood at night, (3) Buildings and streets in my neighborhood are kept in very good repair, and (4) My neighborhood is kept clean (Ross and Mirowsky 1999). Response categories for these items range from 1 (not at all) to 4 (a lot). All items were reverse-coded so that higher values would indicate greater perceptions of neighborhood disorder. The four perceived neighborhood disorder items produced a single factor with standardized loadings ranging between 0.72 and 0.89. Reliability analysis also suggested excellent internal consistency for four items in MIDUS 2 (ω = 0.85) and MIDUS 3 (ω = 0.93). We acknowledge that perceived neighborhood disorder and fear of crime are sometimes treated as conceptually distinct (Wallace 2012); however, we argue that these concepts are not necessarily conceptually distinct. Our indicators of social disorder are clearly in line with items from the original Ross-Mirowsky Perceived Neighborhood Disorder Scale (Ross and Mirowsky 1999): “My neighborhood is safe.”“There is a lot of crime in my neighborhood.”“I’m always having trouble with my neighbors.” Asking someone whether they “feel safe” in their neighborhood is another way of asking whether someone's “neighborhood is safe.”
Divine Struggles
Divine struggles refer to a latent variable that is measured with two indicators of strained relations with God: (1) Wonder if God has abandoned me and (2) Feel God is punishing me for sins. Response categories for these items range from 1 (not at all) to 4 (a great deal). All items are coded so that higher values would indicate greater divine struggles. The two divine struggles items produced a single factor with standardized loadings ranging between 0.81 and 0.88. Although we omitted a third item (Congregation makes too many demands) from subsequent analyses for having a low standardized factor loading (<0.40), we note that our mediation model was replicated with all three indicators. Reliability analysis also suggested good internal consistency for two items in MIDUS 2 (ω = 0.71) and MIDUS 3 (ω = 0.69).
Background Variables
All regression analyses include adjustments for a range of observed (not latent) background variables, including age (years), gender (1 = male; 0 = female), race/ethnicity (1= non-White; 0 = non-Hispanic White), education (1 = college degree; 0 = less than a college degree), household income (in dollars), religious attendance (Within your religious or spiritual tradition, how often do you attend religious or spiritual services? 1 = never to 6 = once a day or more), prayer frequency (Within your religious or spiritual tradition, how often do you pray in private? 1 = never to 6 = once a day or more), religiosity (How religious are you? 1 = not at all to 4 = very), religious salience (How important is religion in your life? 1 = not at all to 4 = very), spirituality (How spiritual are you? 1 = not at all to 4 = very), spiritual salience (How important is spirituality in your life? 1 = not at all to 4 = very), and residential tenure (How many years have you lived in your current neighborhood, or if you live in a rural area, in your current township?). In preliminary analyses, we attempted to reduce our background religion variables by estimating a latent religiosity factor. Because this strategy compromised our model fit, subsequent analyses employ all background religion variables separately.
Analyses
Our analyses begin with the presentation of descriptive statistics for all study variables, including variable ranges, sample means, and standard deviations (Table 2). We then regress our proposed mediators (perceived neighborhood disorder and divine struggles) on structural neighborhood disadvantage and background variables in structural models (Table 3). Next, we regress psychological distress on structural neighborhood disadvantage, perceived neighborhood disorder, divine struggles, and background variables in more elaborated models (Table 4).
Descriptive Statistics (MIDUS 2 AND 3).
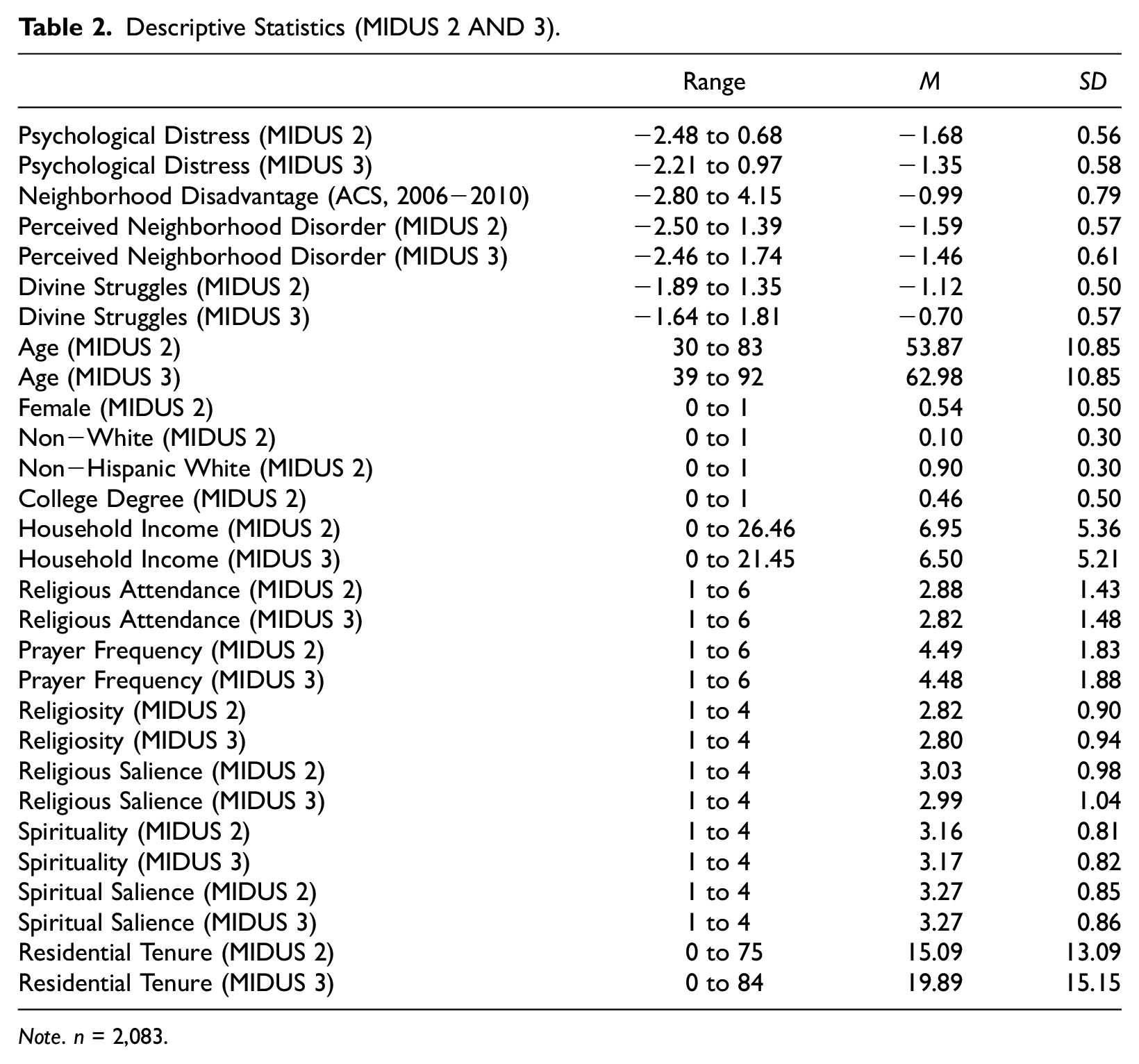
Note. n = 2,083.
Regression of Perceived Neighborhood Disorder and Divine Struggles (MIDUS 2 AND 3).
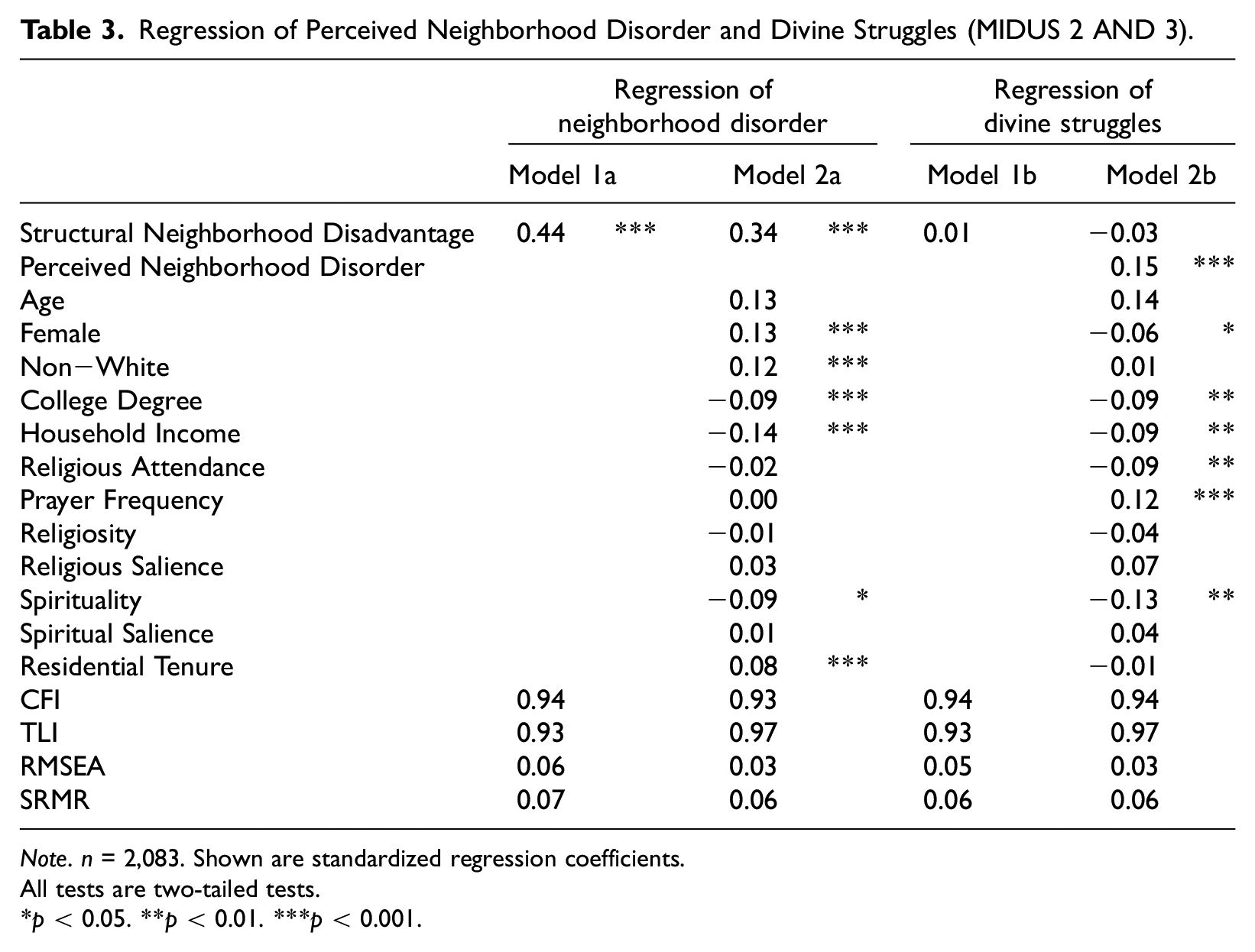
Note. n = 2,083. Shown are standardized regression coefficients. All tests are two-tailed tests.
p < 0.05. **p < 0.01. ***p < 0.001.
Regression of Psychological Distress (MIDUS 2 AND 3).
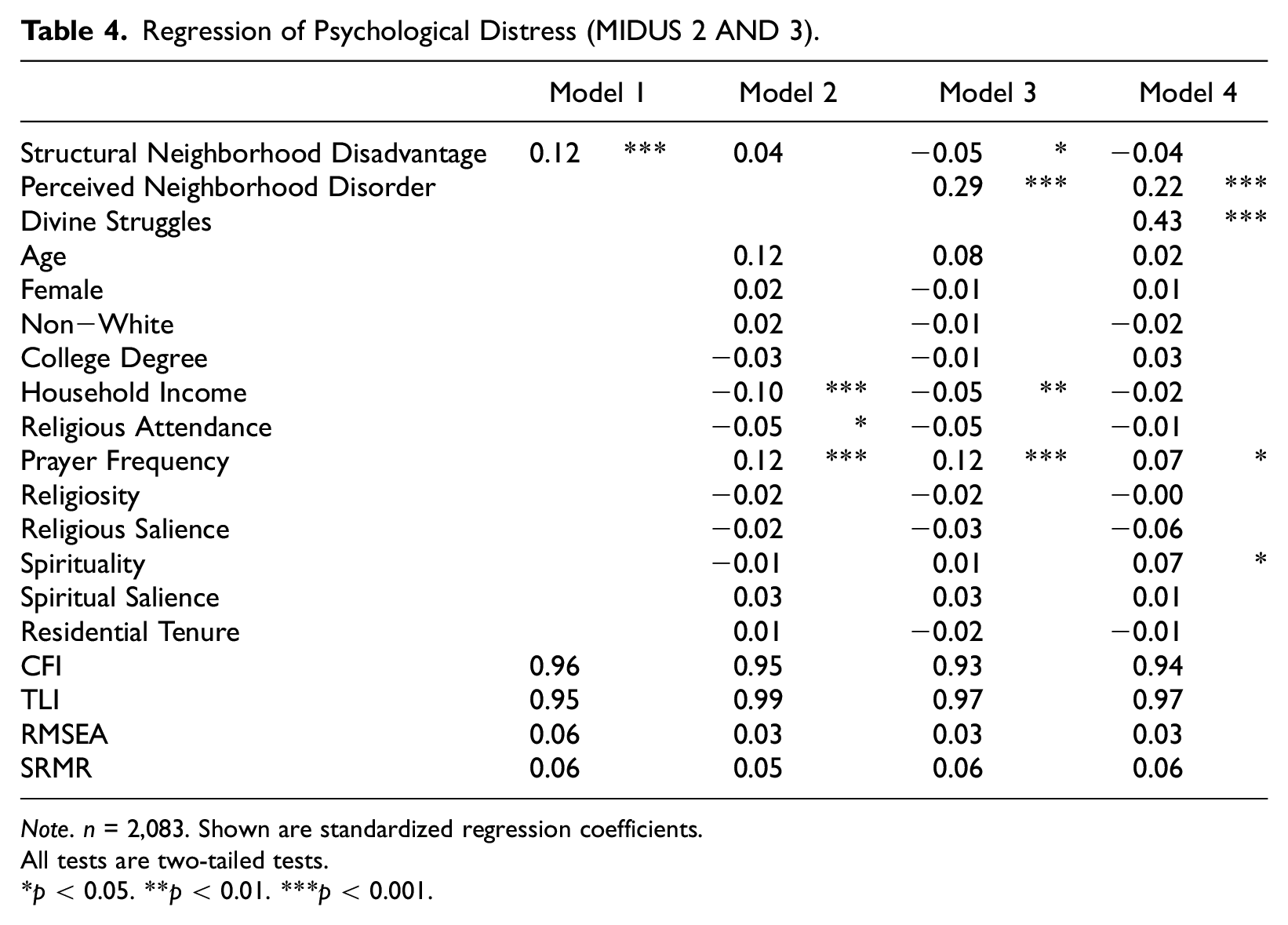
Note. n = 2,083. Shown are standardized regression coefficients. All tests are two-tailed tests.
p < 0.05. **p < 0.01. ***p < 0.001.
To formally test our proposed mediation model, we employed structural equation modeling (SEM) with marginal models and unstructured covariances (Fitzmaurice, Laird, and Ware 2011; Rabe-Hesketh and Skrondal 2012). Marginal models with unstructured covariances effectively account for autocorrelation by assuming unrestricted covariances between residual terms across time points. This approach is well-suited to longitudinal data and tends to yield more accurate results than methods that do not account for autocorrelation (Fitzmaurice et al. 2011).
As emphasized in our theoretical model, we investigated two primary indirect effects: (1) structural neighborhood disadvantage → perceived neighborhood disorder → psychological distress and (2) structural neighborhood disadvantage → perceived neighborhood disorder → divine struggles → psychological distress. These indirect effects were modeled with the following six equations that employ latent variables to represent structural neighborhood disadvantage, perceived neighborhood disorder, divine struggles, and psychological distress:
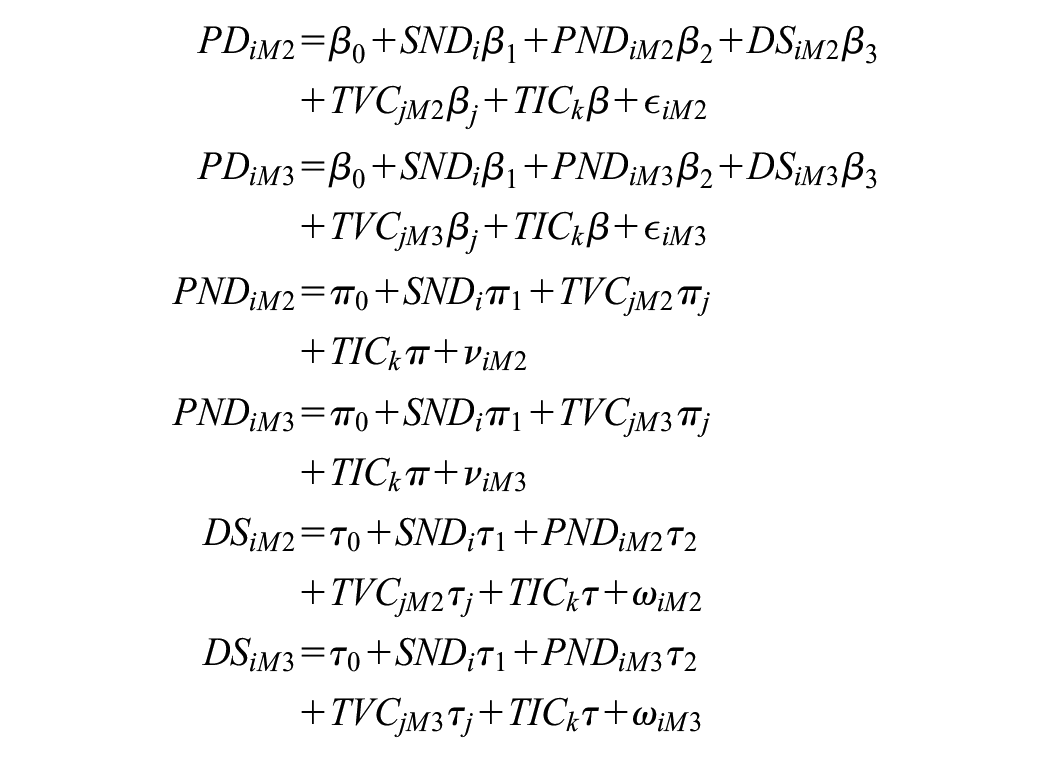
In these equations,
All model estimation was conducted using the lavaan package in R (Rosseel 2012). Because we present our models in a stepwise fashion—from the simplest SEM with no control variables to the fullest SEM with all control variables—to facilitate a more comprehensive understanding of how our proposed mediators (perceived neighborhood disorder and divine struggles) help to explain the relationship between structural neighborhood disadvantage and psychological distress, our models have different fit statistics. We also note that since latent variables in SEM have arbitrary metrics, latent variable ranges can be entirely positive, entirely negative, or anywhere in between. Each indicator in the measurement model of an SEM has an error term with a mean of zero. According to this convention, the lavaan package in R produces “observed” values of latent variables or latent scales that are conceptually akin to predicted values in linear regression. Finally, we calculated indirect effects using the product-of-coefficients method (MacKinnon, Fairchild, and Fritz 2007). We present conservative p values and confidence intervals based on a standard normal distribution (Hayes 2022).
Results
Descriptive Statistics
According to Table 2, respondents exhibited low mean levels of psychological distress (based on the range of values). In terms of neighborhood context, the average respondent lived in neighborhoods characterized by low to moderate levels of structural neighborhood disadvantage and perceived neighborhood disorder. The mean for residential tenure suggests that the average respondent lived in their neighborhood between 15 and 19 years. Finally, respondents reported low to moderate levels of divine struggles.
Regression of Perceived Neighborhood Disorder and Divine Struggles
In Table 3, we assessed model fit using the comparative fit index (CFI), the Tucker-Lewis index (TLI), the root mean square error of approximation (RMSEA), and the standardized root mean square residual (SRMR). Following previous research (Gana and Broc 2019), we employed the following thresholds for model fit: CFI (≥0.90), TLI (≥0.90), RMSEA (≤0.08), and SRMR (≤0.08). Based on these guidelines, we observed adequate to excellent model fit in our full models (Models 2a and 2b). In the context of marginal models, our coefficients should be interpreted as the estimated average cross-sectional difference (averaged between MIDUS 2 and 3) in the mean of Y for those who are one unit apart on X.
Models 1a and 2a regress perceived neighborhood disorder on structural neighborhood disadvantage and background variables. Both models indicate that structural neighborhood disadvantage is positively associated with perceived neighborhood disorder. In other words, respondents who live in neighborhoods characterized by greater socioeconomic disadvantage tend to report more concerns about their neighborhood safety and more problems with their built environment.
Models 1b and 2b regress divine struggles on structural neighborhood disadvantage, perceived neighborhood disorder, and background variables. Although structural neighborhood disadvantage is unrelated with divine struggles across models, perceived neighborhood disorder is positively associated with divine struggles in Model 2b. This suggests that respondents who report more problems with crime and dilapidation in their neighborhood also tend to report more struggles with their divine relations.
Regression of Psychological Distress and Mediation Analysis
In Table 4, model fit was adequate to excellent across our structural models predicting psychological distress (Models 2-4). Although Model 1 indicated that structural neighborhood disadvantage is positively associated with psychological distress, this association was attenuated to insignificance with the addition of background variables in Model 2. In Model 3, we observe that the association between structural neighborhood disadvantage and psychological distress is suppressed by perceived neighborhood disorder. This suppressor pattern is explained by the opposite signs of the direct effect of structural neighborhood disadvantage (−) on psychological distress and the product of the effect of structural neighborhood disadvantage on perceived neighborhood disorder and the effect of perceived neighborhood disorder on psychological distress (+). In Model 3, we also observe that perceived neighborhood disorder is positively associated with psychological distress. In other words, respondents who report more concerns about their neighborhood safety and more problems with their built environment also tend to report higher levels of psychological distress. From Model 3 to Model 4, the association between structural neighborhood disadvantage and psychological distress is no longer different from zero. We also see that the association between perceived neighborhood disorder and psychological distress is attenuated by approximately 23 percent when adjusting for divine struggles. In Model 4, divine struggles are positively associated with psychological distress. This indicates that respondents who report more problems with their divine relations also tend to exhibit higher levels of psychological distress. These patterns support the hypothesis that the association between perceived neighborhood disorder and psychological distress is mediated by divine struggles.
In Figure 2, we present the standardized indirect effects of structural neighborhood disadvantage on psychological distress through perceived neighborhood disorder and divine struggles. This figure represents the full SEM with all paths (Models 2a and 2b in Table 3 and Model 4 in Table 4). The key finding in Figure 2 is that our proposed model is confirmed by an indirect effect that is different from zero (neighborhood disadvantage → perceived neighborhood disorder → divine struggles → psychological distress).
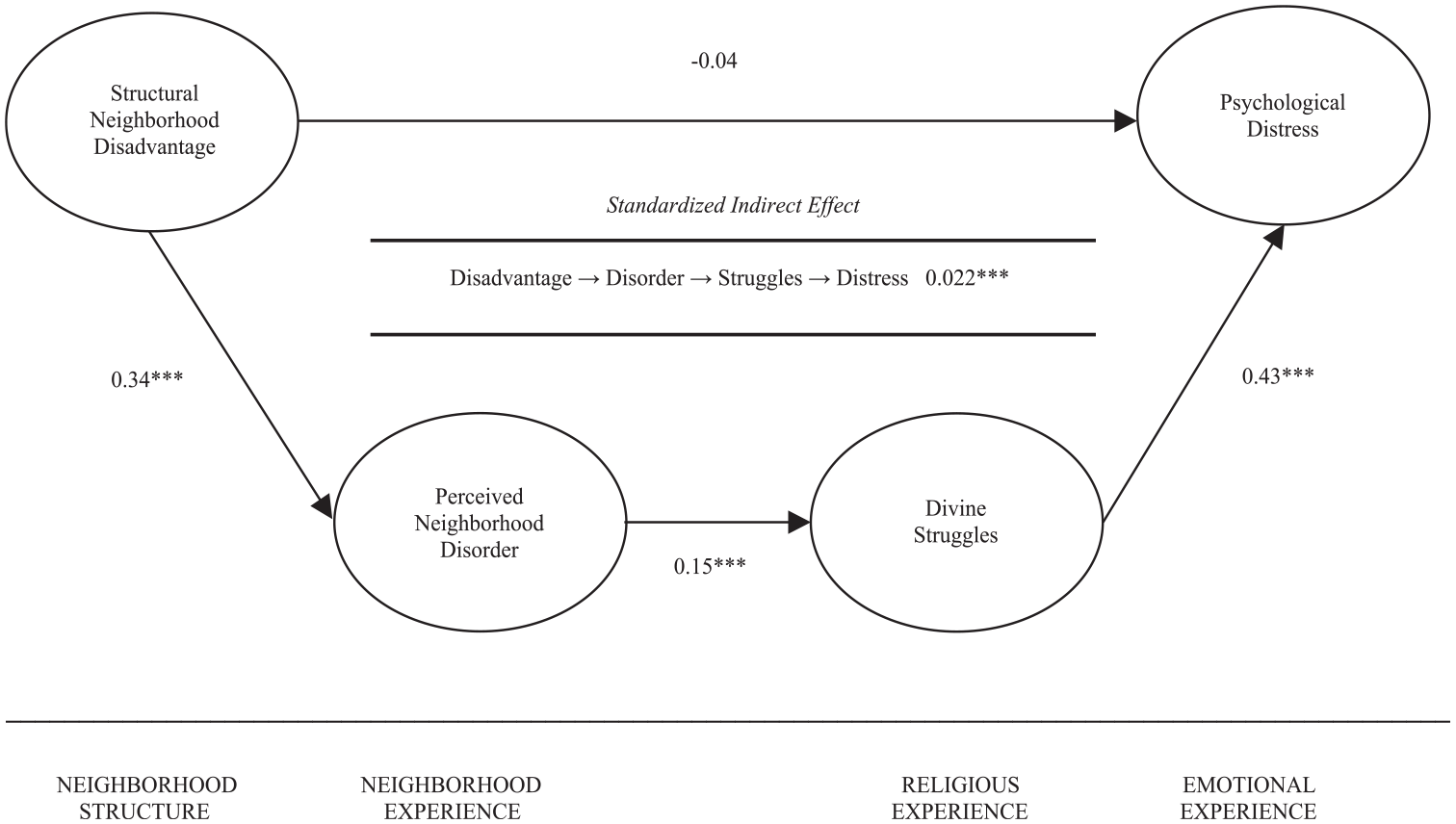
Empirical model of the indirect effect of structural neighborhood disadvantage on psychological distress.
Supplemental Attrition Analyses
Previous research has reported higher attrition rates for MIDUS respondents who reported being non-White, male, unmarried, parents, less educated, and less physically and mentally healthy (Liang 2024; Radler and Ryff 2010; Song et al. 2021). We are not overly concerned with attrition in our longitudinal sample for two main reasons. First and foremost, the results of our mediation model are consistent with previous theory and research. Second, attrition is unlikely to have biased our mediation analysis because we were able to replicate our results using multivariate imputation by chained equations (MICE) with 32 multiply imputed datasets that were pooled according to Rubin's rule (Rubin 1987; Van Buuren 2018). Although missing data can also be handled with full information maximum likelihood (FIML) estimation, FIML is not available in lavaan with ordinal indicators for latent variables.
Supplemental Endogeneity Analyses
To assess the impact of mental health selection in our analyses, we assessed our mediation model controlling for baseline psychological distress (MIDUS 1). With this new adjustment, (1) structural neighborhood disadvantage was positively associated with perceived neighborhood disorder (β = 0.360, p < .001), (2) perceived neighborhood disorder was positively associated with divine struggles (β = 0.142, p < .001), and (3) divine struggles were positively associated with psychological distress (β = 0.473, p < .001). Although we were able to replicate the indirect effect of neighborhood structural disadvantage on psychological distress through perceived neighborhood disorder and divine struggles (I.E. = 0.024, p < 0.001), we do not control for baseline psychological distress in our main analysis due to poor model fit on three of the four indices (CFI = 0.789, TLI = 0.777, RMSEA = 0.062, and SRMR = 0.100).
Supplemental Mediation Analyses
We estimated Monte Carlo confidence intervals for all coefficients as a robustness check (MacKinnon, Lockwood, and Williams 2004; Preacher and Selig 2012). Since Monte Carlo simulation does not assume a normal distribution of indirect effects, p values cannot be computed. Our Monte Carlo mediation analysis was substantively identical to our reported mediation analysis (available upon request).
Although not represented in our simplified empirical model, we note that the indirect effects of structural neighborhood disadvantage on psychological distress through divine struggles alone (neighborhood disadvantage → divine struggles → mental health) was not different from zero (I.E. = −0.015, p > .05). This null pattern supports the primacy of the more comprehensive indirect effect of structural neighborhood disadvantage through perceived neighborhood disorder and divine struggles.
Finally, we replaced divine struggles in our mediation model with several other potential mediators, including positive religious coping (turning to religious and spiritual beliefs for guidance in daily life), divine control beliefs (looking to God for strength, support, and guidance), self-esteem (self-worth), and the sense of control (mastery). Perceived neighborhood disorder was associated with lower levels of positive religious coping (β = −0.168, p < .001); however, positive religious coping failed as a mediator (I.E. = −0.261, p > .10) because it was not directly associated with psychological distress (β = 1.553, p > .05). Because our mediation analysis of divine control failed to converge, we were unable to produce any coefficient estimates. Perceived neighborhood disorder was associated with lower levels of self-esteem (β = −0.244, p < .001) and the sense of control (β = −0.357, p < .001). Although we observed statistically significant indirect effects of perceived neighborhood disorder on psychological distress through self-esteem (I.E. = 0.181, p < .001) and the sense of control (I.E. = 0.210, p < 0.001), we were unable to compare the model fit of these models with our divine struggles models. We employed weighted least squares estimation to account for our ordinal indicators because maximum likelihood estimation can be biased under these conditions. The issue is that weighted least squares estimation cannot produce Akaike information criterion (AIC) or Bayesian information criterion (BIC) estimates to compare the model fit of non-nested models. To our knowledge, there is no established way to directly compare the model fit of non-nested models. All we can really conclude from our supplemental mediation analyses is that divine struggles is a better mediator than positive religious coping or divine control beliefs because we failed to observe any indirect effects for these alternative mediators. The case of self-esteem and the sense of control are more complicated because we did, in fact, observe indirect effects for these alternative mediators. In the context of our analyses, divine struggles, self-esteem, and the sense of control all work as mediators of neighborhood context. To our knowledge, there is no a priori theory to suggest that any of these three mediators would be especially pronounced. For this reason, our intention was to establish divine struggles and a new mediator of neighborhood context, not to compare the mediating effect of divine struggles with other established mediators such as self-esteem and the sense of control. It is our view that the relative strength of these mediators would be of little value in the absence of theory.
Discussion
Although researchers have consistently linked structural neighborhood disadvantage with poorer mental health, they continue to search for underlying mechanisms. Previous studies have emphasized several classes of traditional mediators, including chronic social stressors, social disintegration, poorer self-conceptions, and risky health-related behaviors (Barnett et al. 2018; Hill and Maimon 2013; D. Kim 2008; Mair et al. 2008; Richardson et al. 2015; Sui et al. 2022); however, Hill and colleagues (2024) have recently argued that we could advance this discussion by integrating insights from the study of religion. In this article, we applied the stress process framework to propose a mediation model of the indirect effect of structural neighborhood disadvantage on psychological distress through perceived neighborhood disorder and divine struggles. We formally tested our model using longitudinal national survey data from the MIDUS study.
Our proposed mediation model synthesized three propositions that we derived from prior research on neighborhood context and mental health. The first proposition stated that neighborhood structure (structural neighborhood disadvantage) would shape neighborhood experience (perceptions of neighborhood disorder). In support of this proposition, we found that respondents who lived in neighborhoods characterized by greater socioeconomic disadvantage tended to report more concerns about their neighborhood safety and more problems with their neighborhood built environment. This pattern confirms previous neighborhood theory and research (Massey and Denton 1993; Sampson and Groves 1989; Schieman and Pearlin 2006; Shaw and McKay 1942; Wilson 1987).
The second proposition suggested that neighborhood experience would shape religious experience. Along these lines, our results indicated that respondents who reported more problems with neighborhood disorder also tended to report more divine struggles. This finding is generally consistent with previous studies of various social stressors and religious struggles (Ai et al. 2010; Ellison and Lee 2010; Exline et al. 2011; Exline et al. 2023; Fitchett et al. 2004; Hill et al. 2017; Koenig et al. 1998; Krause and Hayward 2012; Krause et al. 2017; Pargament et al. 1998; Stauner et al. 2019; Wortmann et al. 2011), including recent research linking perceptions of neighborhood disorder with greater religious struggles (Hill et al. 2024). Over the years, perceived neighborhood disorder has been linked with lower levels of trust, social support, self-esteem, and the sense of control (Ellison et al. 2023; Hill et al. 2013; J. Kim 2010; J. Kim and M. E. Conley 2011; O’Brien, Farrell, and Welsh 2019; Ross 2011; Ross and Jang 2000; Ross and Mirowsky 2009). Our research provides additional evidence to suggest that the noxious effects of perceived neighborhood disorder may also extend to the “spiritual dimension” of psychosocial functioning.
The final proposition specified that religious experience would shape emotional experience (psychological distress). In fact, we observed that respondents who reported more problems with their divine relations also tended to exhibit higher levels of psychological distress. This pattern dovetails with numerous previous studies of religious struggles and mental health (Bockrath et al. 2022; Cowden et al. 2022; Ellison and Lee 2010; Hill et al. 2021; Pargament et al. 2004; Park et al. 2011; Silton et al. 2014; Upenieks 2021, 2022; Wilt et al. 2022).
In addition to these contributions, our formal mediation analysis substantiated the indirect effect of structural neighborhood disadvantage on psychological distress through perceived neighborhood disorder and divine struggles (neighborhood disadvantage → perceived neighborhood disorder → divine struggles → mental health). This finding builds on the original model proposed by Hill and colleagues (2024), which was limited by the omission of neighborhood structure (perceived neighborhood disorder → religious struggles → mental health). The model proposed and tested in this article provides a more comprehensive assessment of the indirect effects of neighborhood context on mental health. Although the direct neighborhood experience remains important for our understanding of neighborhood context and mental health, the stress process framework reminds us that the fundamental problem is social structural disadvantage, not perceptions of problems in the neighborhood. For decades, scholars argued that neighborhood disadvantage and perceived neighborhood disorder are likely to undermine mental health through processes related to stress, psychosocial functioning, and health behavior (Aneshensel and Sucoff 1996; Barnett et al. 2018; Hill and Maimon 2013; D. Kim 2008; J. Kim 2010; Kowitt et al. 2020; Mair et al. 2008; O’Brien et al. 2019; Richardson et al. 2015; Ross 2000; Ross and Mirowsky 2009; Sui et al. 2022). Building on previous work, our analyses suggest that divine struggles are an important class of stressors that may also play a role in explaining why living in a neighborhood that is characterized by structural disadvantage and disorder is often associated with poorer mental health.
We acknowledge that our analyses are limited in two key respects. Our primary limitation is causality. Contrary to our proposed mediation model, psychological distress could precede perceptions of neighborhood disorder and the experience of divine struggles through processes related to health selection, negative cognitive bias, and negative religious coping. In other words, people with pre-existing mental health issues could be selected into poorer neighborhoods through social drift or downward social mobility (e.g., being unable to work or to earn money due to pre-existing mental health issues). Given that negative cognitive bias can be a symptom of psychological distress, pre-existing mental health issues could lead some people to report more negative information about their neighborhood and religious experiences. Finally, pre-existing mental health issues could also be a source of negative religious coping. For example, some people with mental health issues may blame God for their misery or feel like they have been abandoned by God. Given that many of our focal associations are likely to be bidirectional or mutually reinforcing, we cannot exclude, theoretically or empirically, viable alternatives to our proposed mediation model. In other words, our model is only one of many potential models. We note that, aside from the association between perceived neighborhood disorder and religious struggles, our model is well supported by previous theory and longitudinal research (e.g., previous cited studies linking neighborhood structure with neighborhood disorder and religious struggles with poorer mental health). Our supplemental analyses also suggest that the focal associations in our mediation analyses are robust to lagged adjustments for baseline levels of psychological distress.
Our second limitation is measurement. Although MIDUS is unique in its assessment of valid and reliable indicators of perceived neighborhood disorder, divine struggles, and psychological distress, the survey was limited with respect to some of our focal measurements. We direct future research to employ more detailed and traditional assessments of perceived neighborhood disorder and religious struggles (Exline et al. 2014; Exline et al. 2022; Ross and Mirowsky 1999). For example, additional indicators of perceived neighborhood disorder could focus more on neighborhood problems than neighborhood fear (e.g., perceptions of noise, specific criminal behaviors, and other threatening activities). More detailed assessment of religious struggles should also be considered (e.g., religious doubts, moral struggles, and demonic struggles).
Conclusion
With these limitations in mind, our analyses offer new insights into the study of neighborhood context and mental health by integrating the study of religion. We show that the association between structural neighborhood disadvantage and poorer mental health is mediated by perceived neighborhood disorder and religious struggles. Future research should replicate our model with more comprehensive assessments of perceived neighborhood disorder and religious struggles. Our work might also be extended through the exploration of additional indicators of structural neighborhood disadvantage (e.g., residential segregation) and different dimensions of religion (e.g., beliefs about hell, God images, positive religious coping, and religious attendance). Although we focused on nonspecific psychological distress, other mental health outcomes should be examined (e.g., depression, anxiety, chemical dependency, and indicators of positive affect and well-being). It is also possible that our proposed mediation model could vary according to theoretically relevant subgroups such as gender and race/ethnicity (i.e., moderated mediation). Research along these lines would help to further develop our understanding of the psychosocial processes underlying the association between neighborhood context and mental health.