
Abstract
Community-level social capital has been theorized to shape mental health, particularly in disaster contexts, but methodological complexities hamper prior studies. Pairing zip-code-level data on social capital from Opportunity Insights with repeated cross-sectional health survey data before and after Hurricane Harvey in Houston, Texas, we examine how local social capital moderated the mental health consequences of disaster housing damage. We first document null associations between local social capital and residents’ mental health before the disaster. Next, we fit models predicting psychological distress and poor mental health days, revealing that local levels of economic connectedness and rates of volunteering offset adverse mental health effects of home damage after the storm and patterned disaster assistance receipt. These findings have broader implications for literatures on community resilience, mental health, and disaster recovery.
Introduction
A longstanding interest in medical sociology is the salutary benefits or downsides of social capital—the social network-based resources that support collective action, reciprocity, and trust (Kawachi and Berkman 2001; Portes 1998; Putnam 2000). Alongside studies focused on individual-level social capital, a growing body of empirical scholarship examines the association between local levels of social capital and residents’ mental health and well-being (Linde and Egede 2023; Muennig et al. 2013; Rodgers et al. 2019). While some evidence suggests that local social capital improves mental and physical health through collective support mechanisms (Kawachi and Berkman 2001), others have documented potential downsides of social capital stemming from burden and stress (Portes 1998), or no effect on health because of competing processes or other community factors, like income level, that covary with social capital and also affect well-being (Lindström and Lindström 2006).
While social capital is built into the fabric of everyday social life, it can become especially important when natural disasters strike. Disasters occur when vulnerability intersects realized risks (Tierney 2019). Disaster affected residents may help others recover from these impacts through informal social ties and formal organizations as part of therapeutic community building (Fritz 1996; Quarantelli and Dynes 1977; Solnit 2009). Others have noted that competition between local community organizations can corrode community cohesion and recovery (Peacock and Ragsdale 1997; Tierney 2015). In these ways, local forms of social capital are theorized to shape resilience and mental well-being among those affected by disasters, above and beyond individual-level social capital (Aldrich 2012; Aldrich and Sawada 2015; Hall et al. 2023; Noel, Cork, and White 2018; Wind and Komproe 2012). Yet existing research on social capital and post-disaster mental health is beset by methodological complexities: widely varying measurement strategies for social capital (Hall et al. 2023; Meyer 2018), a lack of before-and-after data or the presence of control groups (as is inherent in much disasters research given the unpredictable nature of events), and often large, aggregated units of community, such as counties, that may mask more local forms of heterogeneity in social capital.
To address these gaps, we examine zip-code-level social capital and disaster mental health in Houston, Texas. Our data come from the Health of Houston Survey, a large-scale, public health survey that was unexpectedly interrupted by Hurricane Harvey in August 2017 and resumed six months later in Spring 2018, giving researchers two, population-representative samples of adults in Houston before Harvey in 2017 and shortly after in 2018. Using these data, we extend prior work on social capital and mental health in three distinct ways, which in combination begin to address the methodological issues raised above.
First, our empirical strategy uses techniques to reduce two potential sources of bias: (1) selection into neighborhoods and (2) selection into disaster exposure (i.e., home damage). Specifically, we address neighborhood selection by using the pre-disaster survey data to assess associations between local social capital and mental health before Hurricane Harvey, and in our post-Harvey analysis of disaster housing damage and mental health, we use a fixed effect term for urban regions within Houston. These models also address selection into disaster exposure by estimating associations with inverse probability of treatment weights to construct a statistically similar group of respondents with and without home damage. Second, we use novel data on local social capital at the zip code level from Opportunity Insights, representing the first study of a disaster to our knowledge to pair these social capital estimates from large-scale data to test for mental health outcomes. Finally, we assess the relationship between local social capital and the receipt of disaster assistance—one process through which local factors are theorized to shape mental well-being.
Our results show that before Hurricane Harvey there were no associations between residents’ mental health and zip-code-level measures of social capital. After the disaster, zip code levels of economic connectedness (bridging capital) and rates of volunteering (civic engagement) were correlated with mental health in unadjusted models, but not after controlling for individual- and zip-code-level controls. Home damage was strongly associated with psychological distress and poor mental health days. Yet for people who experienced home damage, local social capital patterned mental health. Among those with home damage, residing in a zip code with higher levels of economic connectedness and higher volunteering rates were significantly less likely to experience mental health adversity than otherwise similar people living in zip codes with low levels of social capital. In communities with social capital one standard deviation above the mean, the predicted probabilities of psychological distress for residents with and without home damage were not statistically distinguishable. Moreover, we find that rates of economic connectedness and volunteering increased the probability of receiving assistance for those with home damage and decreased the probability for those without home damage. Following work in this field (Aldrich 2012; Gallagher et al. 2019; Hall et al. 2023; Wind and Komproe 2012), our findings clarify and extend previous research to suggest how community-level social capital is a strong form of resilience in post-disaster communities.
Background
Measuring social capital beguiles social capital research generally and disasters and health research specifically (Hall et al. 2023; Meyer 2018). Previous ways of measuring social capital in the field can range from types of social ties (Hawkins and Maurer 2010) to densities of local organizations (Smiley, Howell, and Elliott 2018), rates of civic engagement (Gallagher et al. 2019), and generalized trust (Wind, Fordham, and Komproe 2011). The theories informing these measurements range from trust-boosted civic action (Putnam 2000), the emphasis on relations in Coleman (1988) and Lin (2001), and the convertibility of different kinds of capitals toward unequal outcomes in Bourdieu and Wacquant (1992), among others (see Portes 1998). At the community level, social capital is foundational for resilience in that greater community social capital can lead to greater resilience post-disaster (Aldrich and Meyer 2015).
The need for new ways of measuring social capital concepts is ongoing and critical to advance the field. In a major project, Chetty et al. (2022a) draws on data on social networks of 72 million Facebook users totaling 21 billion network ties to measure three different concepts of social capital: connectedness, civic engagement, and cohesiveness. Chetty’s work (see Methods) links these types of social capital to social outcomes such as economic mobility. Important to the measurement of social capital, Chetty uses new data with a familiar approach of aggregating individual social ties to delineate community social capital (Norris et al. 2008). This move retains theoretical emphasis on relations (Coleman 1988; Lin 2001) and how they can affect social outcomes and generate inequalities (Bourdieu and Wacquant 1992).
The first type of social capital, connectedness, can be defined as “.. . the extent to which different types of people (for example, high income versus low income) are friends with each other)” (Chetty et al. 2022a, 2022b) Bridging social capital is most closely associated with connectedness (Putnam 2000). Although Chetty’s work has yet to be directly applied to research on disasters, place, and health, the concept of connectedness has parallels to previous work especially with bridging social capital. Multiple studies link greater community bridging social capital as protective of health (Gilbert et al. 2013; Kim, Subramanian, and Kawachi 2006), although its protective effect can come into question for disparities such as by race given measurement issues in social capital research (Villalonga-Olives et al. 2023). Some research on disasters and mental health suggest that greater community linkages can be protective of mental health impacts (Hall et al. 2023; Raifey et al. 2022; Wang 2022; Wind and Komproe 2012) although other work casts doubt on how these mechanisms may operate (Smiley, Clay, et al. 2022; Wind et al. 2011; Zahnow et al. 2019).
The second type of social capital, civic engagement, primarily relates to volunteering and rates of participation in local organizations. These local organizations and their volunteers are critical conduits of social capital that broker resources that can be shared in communities (Small 2009). Civic engagement in the context of disasters often involves existing local organizations springing into recovery efforts alongside informal efforts to aid others in disaster response (Aldrich and Meyer 2015; Medwinter 2021; Solnit 2009). Individual civic engagement in disasters context can have adverse effects on mental health (Fitzpatrick and Spialek 2020; Smiley et al. 2022; Weil, Lee, and Shihadeh 2012), but residing in a community with more civic engagement has been found to be protective in some studies (Gallagher et al. 2019) or leading to negative mental health outcomes in others (Lowe et al. 2015; Sato et al. 2020). The protective effects of civic engagement have similar theoretical roots in bridging social capital as was the case for connectedness. The adverse effects of civic engagement on mental health have theoretical roots in the idea that civically engaged individuals or communities high in civic engagement may experience fatigue from response and recovery efforts. They may also perceive community as more central to their identities, and therefore perceive a greater emotional loss.
A final important distinction for the use of place-based social capital concerns what scholars have termed a “dark side” of social capital (Elliott, Haney, and Sams-Abiodun 2010; Villalonga-Olives and Kawachi 2017) or its “Janus-faced” nature (Aldrich 2012) that can shape uneven resilience (Tierney 2015). This distinction refers to how disparities in social capital across places can contribute to widening disparities in social outcomes (such as health) as high social capital communities use denser networks and greater resources to recover more efficaciously than communities with less social capital (Smiley et al. 2018). In the context of connectedness and civic engagement, two dynamics may come to the fore: (1) higher levels of each type of community social capital could be protective of mental health, and (2) inequalities in each type of community social capital can contribute to disparities in mental health. This second dynamic—inequalities in social capital widening mental health disparities—is a central element examined in our research design. Further, while much of the foregoing work advances our understanding of social capital connectedness and mental health, Chetty et al. (2022a) can transform the field with stronger data to measure existing conceptualizations of community social capital by using large-scale data on a social media platform whose usage is widespread and important in disaster contexts (Houston et al. 2015). We center the community level over the individual level to understand these spatially uneven effects. Studying social capital is therefore crucial to unlocking a key mechanism that creates community-based resilience including inequalities in resilience.
In all, our approach synthesizes and advances previous research on social capital and disaster impacts on mental health. The upshot of using Chetty et al. (2022b) data is that our community-level measures have much more comprehensive data on social ties than is typical of previous research. Further, empirically estimating the effect of community social capital on mental health is difficult given the potential for selection bias resulting from neighborhood sorting. Past analyses finding both beneficial and deleterious effects on health have overwhelming relied on associational strategies (Villalonga-Olives and Kawachi 2017). We address these concerns by examining pre-disaster associations between local social capital and mental health, and by estimating differential effects of social capital on mental health across individual-level exposure, in terms of reported housing damage, using urban region fixed effects and weighting for selection into housing damage, discussed further below.
The Case
The case for this study is Greater Houston during Hurricane Harvey. The storm was the wettest tropical cyclone ever recorded in the United States, caused an estimated $125 billion in damages (tied with Hurricane Katrina for the costliest hurricane on record in the United States), and led to more than 100 deaths. The 1-in-2,000-year hurricane by twentieth-century standards was partly fueled by climate change (Smiley et al. 2022). Effects on health were far-reaching from the storm with studies reporting impacts including to mental health (Bevilacqua et al. 2020; Bozick 2021; Cohen et al. 2023; Fitzpatrick and Spialek 2020; Karaye et al. 2019; Schwartz et al. 2018; Taioli et al. 2018). Most notable for our study is Bozick (2021) who found that days of poor mental health increased after the storm especially in places with more damage. Our methodological approach builds on this work by employing an inverse probability of treatment weighting (IPTW) technique to adjust selection into respondent-level disaster housing damage, as compared to Bozick’s (2021) propensity score matching to match on community-level housing damage, and to build community social capital metrics in the approach.
Data
Health, Assistance, and Disaster Data
Individual-level information on mental health, residential location, disaster assistance, and disaster damage come from the Health of Houston Survey (HHS), a large-scale public health survey administered annually by the University of Texas at Houston School of Population Health (Linder et al. 2019). Beginning in May 2017, the study was in the field, but it was unexpectedly interrupted by Hurricane Harvey in late August 2017. Surveying resumed six months later in February 2018 and concluded in late April 2018, providing two cross-sections of representative data on Houston residents with a total of N = 5,694 respondents. The overall response rate was 32.8 percent. After listwise deletion of missing cases on covariates (total <3 percent), we use pre-disaster (N = 2,508) and post-disaster (N = 2,755) data on mental health and residential zip code, including the zip code of residence at the time of Hurricane Harvey for the post-disaster sample.
We focus on two measures of mental health: psychological distress and poor mental health days. We operationalize psychological distress using the Kessler-6 scale, a measure constructed from a series of six questions about distressful feelings over the past month, including nervousness, hopelessness, restlessness, depression, worthlessness, and effortfulness (Kessler et al. 2002). Responses to each question are scored from 0 “None of the time” to 4 “All the time,” and summed for a score ranging from 0 to 24 (Cronbach’s α = .86). The K-6 score has been validated for screening for mental illness and mental healthcare utilization with research suggesting a score of greater or equal to 13 correlates strongly with severe mental distress (Kessler et al. 2003). As such, we model the probability of a psychological distress using this threshold. For poor mental health, we model the probability of reporting greater than or equal to 14 poor mental health days in the last month. This question first developed in 1993 by the BRFSS to measure the burden of mental health in the United States, and the threshold of 14 days in the last 30 has been widely used in studies and reported by the CDC (Moriarty, Zack, and Kobau 2003). Note that both measures are asked with respect to the last 30 days, which for the post-Harvey sample ensures a temporal reference that does not overlap with the occurrence of the disaster.
From the post-disaster survey, we also collect several additional pieces of information. To measure home damage, we construct a binary measure that takes a 1 if a respondent reported any flood damage to their home (“limited,”“fair,” or “complete”) and 0 otherwise (“none,”“flooding in street, but not in home”). We follow others in using self-reported home damage to assess the mental health effects of disasters, given data availability (Raker et al. 2019). By using a parsimonious assessment of any home damage, we heed concerns regarding unobservable ideocracies in individuals’ assessment of the level of damage. For disaster assistance receipt, we rely on a yes/no question asked of respondents regarding if they received any assistance to help prepare or cope with Hurricane Harvey (coded 1 for yes). We supplement our analysis with two additional variables. The first is a similarly constructed binary measure for whether respondents provided disaster assistance to others. The second variable comes from a question asked of all who indicated receiving assistance about from whom aid was received. Options include from coworkers, church groups, city officials, FEMA, family/friends, and neighbors, among others. Given our interest in place-based processes of exchange, we construct a dummy variable coded as 1 for reporting aid from neighbors and 0 for all other sources. Respondents could report assistance from multiple sources, but 87.3 percent reported aid from only one source. Note that a similar question was not asked among aid providers.
Finally, we gather information on a series of individual sociodemographic characteristics for use as controls in all models: race (four-part coded non-Hispanic White, Hispanic, non-Hispanic Black, and non-Hispanic Asian/other), household size (number of people living in the household), home ownership, age, nativity, education level (dummy for bachelor’s degree or higher), marital status (dummy for single, never married), and annual household income. For full coding, please see Table 1.
Descriptive Statistics of the Analytic Samples.
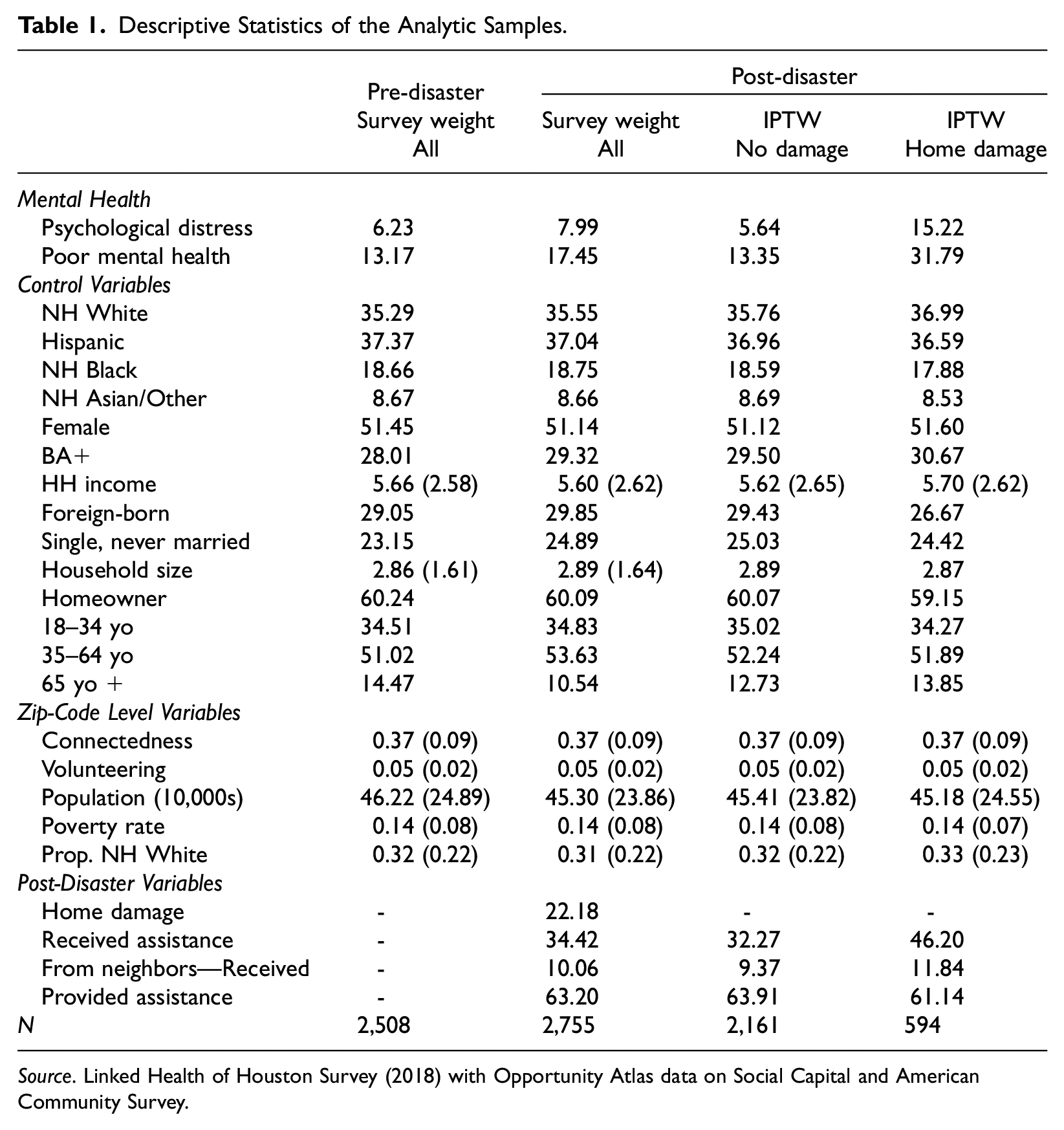
Source. Linked Health of Houston Survey (2018) with Opportunity Atlas data on Social Capital and American Community Survey.
Local Social Capital Data
Using the zip code level, we link data on local social capital produced in the Social Capital Atlas from Opportunity Insights (Chetty et al. 2022a). Chetty et al. (2022a) compiled data on social capital across the United States at the zip code level as part of project to estimate neighborhood effects on economic mobility. Data from more than 72 million frequent Facebook users ages 25–44 were used to construct zip-code-level estimates of community social capital (Chetty et al. 2022a). We use two measures that each correspond to a constitutive element of community social capital. 1 In terms of local network diversity, we focus on connectedness 2 using the zip-code-level estimates of the extent to which people of different socioeconomic status in a zip code are friends with others, whereby a value of 0 corresponds to local networks with no connections between low- and high-SES people, while a value of 1 implies that all low-SES people in a zip code have an equal number of low- and high-SES connections. In terms of civic engagement, we focus on volunteering, operationalized by the proportion of people in a zip code who are members of an activism or volunteering group on Facebook. Given our interest in zip-code-level effects, we also gather three variables from the American Community Survey (ACS) 2013-2017 five-year estimates to use as controls: total population (logged), proportion of the population who are non-Hispanic White, and the adult poverty rate, which may be correlated with both community-level social capital and locals’ mental health.
Note that the Facebook data used by Chetty et al. (2022a) to construct social capital measures were collected in 2022, after Hurricane Harvey occurred, raising concerns about the extent to which local social capital measured after the disaster reflect the state of social capital at the time of the disaster. Similar to this study, others have used these data as independent variables to predict outcomes prior to 2022 (Brown and Ravallion 2023; Linde and Egede 2023). We believe that our strategy is justified on both theoretical and empirical grounds. Theoretically, insights from urban sociology on the durability of neighborhoods, such as local poverty and culture, suggest that neighborhood factors persist over time and are not easily changed (Sampson 2015). Empirically, prior research in disaster contexts has documented stability in pre- and post-disaster measures of social capital (Rayamajhee et al. 2024; Wickes et al. 2019).
As further reassurance, we conducted two additional tests. First, large population shifts from disaster migration that correlates with social capital may bias the measure. To check for this, we examined zip-code-level migration rates using data from the ACS 2017-2021 estimates. We calculated that in the average urban zip code across the United States (i.e., zip codes located in central cities), 10.4 percent of people had moved residences since 2019. This was not statistically different in the Houston area, the context of our study, where an estimated 11.5 percent of people in the average zip code had moved since 2019. Compared to zip codes in the five other largest cities in Texas (San Antonio, Austin, Dallas, Fort Worth, and El Paso), the share of people who had moved in the average Houston zip code was comparable (11.5–11.9 percent). Moreover, using our sample of zip codes, we estimated the associations between the proportion of people who moved and our two measures of local social capital, and neither were statistically significant. Second, to directly observe change in social capital using a different measure, we examined zip-code-level business patterns for social capital organizations as compiled by Rupasingha, Goetz, and Freshwater (2006) in April 2017 and April 2022. The correlation between the number of social capital organizations 2017 and 2019 in our sample of zip codes was r=0.95. This indicates that the organizational imprint of social capital remained highly similar before and after Hurricane Harvey, and suggests further confidence in the spatial stability of social capital in Houston. Nevertheless, our models rest on the assumption that there was no large shift in local friendship networks or joining of civic groups in the five years from 2017 to 2022 that correlated with both health and home damage at the community level. We return to this decision in the discussion.
Methods
Comparatively few studies of community-level social capital attend to the potential selection bias resulting from neighborhood sorting of healthier people into communities with higher social capital (Noel et al. 2018). A key purpose of our study is to directly address this issue which we do using two strategies. First, we leverage the unique availability of pre-disaster survey data to estimate the associations between community-level connectedness and volunteering and our two mental health outcomes in the four months before Harvey made landfall. Any significant associations would point to differences across communities by social capital in the health of residents. Second, in our primary analysis using post-disaster data, we estimate associations using across-zip-code variation in social capital within urban regions, using an “urban region” fixed effect. Specifically, we use data from the Houston Mayor’s Assistance Office (MAO), which divides the city of Houston into eight regions with a specific office and staff assigned to the super-neighborhood councils in each region. We create an additional indicator for zip codes located outside of the city of Houston but still within Harris County and therefore included in our study. Because zip codes (ZCTAs) are not always nested perfectly within the urban regions outlined by the MAO, we assign each zip code to the region that contained the greatest land area. By including these fixed effects, our estimates address both broader regional-level sorting processes and public service providing in the Houston area.
Our empirical analysis proceeds as follows. To begin, we first examine both pre-disaster and post-disaster associations between our two measures of local social capital and our two measures of mental health. A fully adjusted multivariable regression model is fit as follows:

where
We next use the post-disaster survey to estimate the effects of home damage on mental health, and the extent to which the estimated effects of this form of individual-level disaster exposure differ across local levels of social capital. We begin by regressing the probability of each mental health outcome on home damage, using the following equation:

We then extend equation (2) into a moderation model by including an interaction between housing damage, D, and standardized local measures of social capital, SC. We fit a series of the following equation predicting each mental health outcome:

In this specification,
In the final stage of the analysis, we examine the dynamics of disaster assistance, assessing one mechanism by which community social capital may promote resilience and well-being at an interpersonal level. 3 We examine the probability of receiving disaster assistance across levels of social capital conditional on home damage, and interacted with home damage, by reusing equations (2) and (3). In the supplement, we run the same models on the probability of providing disaster assistance and of receiving assistance from neighbors, conditional on any assistance.
Throughout our analysis, we use clustered robust standard errors at the zip code level for statistical inference. Intraclass correlation coefficients from null, unweighted multilevel models revealed little clustering: less than 10 percent of the variation in both mental health outcomes were attributable to the zip code level. Multilevel models using random slopes did not reach convergence in equation (3) and the use of observation-level IPTW or survey weights may bias results given multilevel models assume equal probabilities at the zip code level. Random slope models using covariate adjustment without weights yielded qualitatively similar results. Given these factors, we proceeded to account for grouping by clustering our standard errors. This study was approved by UBC REB (H22-00318).
Results
We begin the results by describing the data. Table 1 provides the descriptive statistics for the analytic samples. The total pre-disaster and post-disaster statistics are weighted using the survey weights provided by the HHS, and the descriptive statistics by home damage in the post-disaster sample are weighted by the IPTW. The pre-disaster and post-disaster samples do not differ on observable sociodemographic characteristics. Overall rates of both mental health measures increased from pre- to post-Harvey by around 30 percent (e.g., 6.23 before the disaster and 7.99 after the disaster for psychological distress) relative to the pre-disaster rates. From the post-disaster sample, 1 in 5 (22 percent) reported home damage. Over 1/3 reported receiving any assistance, of whom 10 percent reported help from a neighbor, and on average, 63 percent gave assistance to others. The last two columns of Table 1 show the descriptive statistics by home damage, weighted using the IPTW. The procedure led to statistically similar groups across all control variables. No sociodemographic or zip-code-level variable is significantly different from 0 (t-tests and chi-squared). Unweighted statistics among the post-disaster sample by home damage are provided in Supplemental Appendix Table A1, demonstrating that IPTW particularly reduced imbalance on race, education, sex, and household income.
Of note, the rates of both mental health outcomes for those with home damage were nearly triple that rates of those without home damage. Home damage also significantly differentiated rates of receiving assistance. Figure 1 maps local connectedness and volunteering across the 150 zip codes used in the analysis. Our two measures of local social capital are strongly correlated (r = .847). There was significant variation across zip codes. Among the Houston zip codes used in our analysis, the average volunteering rate was 5 percent, ranging from 1.5 to 12.5 percent, meaning that in the mean zip code, 5 percent of people were members of an activism or volunteering group on Facebook. The average level of connectedness was 37 percent and ranged from 20 to 59 percent, meaning that the mean share of low-income people’s networks who were high-income at the zip code level was 37 percent.
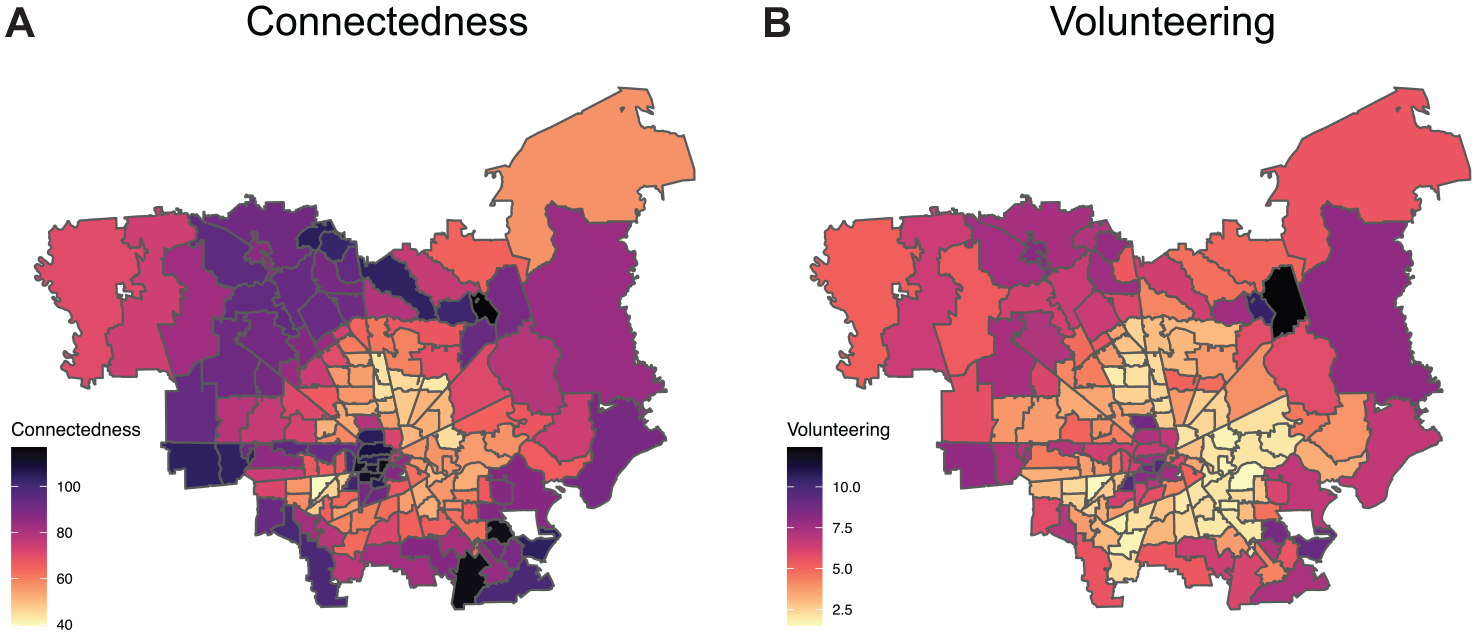
Zip-code level measures of social capital across Houston, Texas.
Figure 2 visualizes the unadjusted and fully adjusted associations between local social capital and our two mental health outcomes before and after Hurricane Harvey. The first column of coefficient plots is for the pre-Harvey sample and the second column presents the coefficients on the post-Harvey sample. Before the disaster, there were no significant associations between either social capital measures and our two mental health outcomes. These plots provide evidence against selection bias, although they do not account for potential temporal variation in the relationship between social capital and health. After Hurricane Harvey, residing in a community with greater connectedness and rates of volunteering were both associated with lower probability of psychological distress in the unadjusted models. Controlling for sociodemographic characteristics and netting out regional variation attenuated these associations and rendered them statistically insignificant. Thus, these findings reveal little evidence that, after adjusting for confounding, social capital correlated with mental health, on average. In the following analyses, we focus on the post-disaster period to examine differences in the effect of social capital and health based on an acute form of individual-level exposure: home damage.
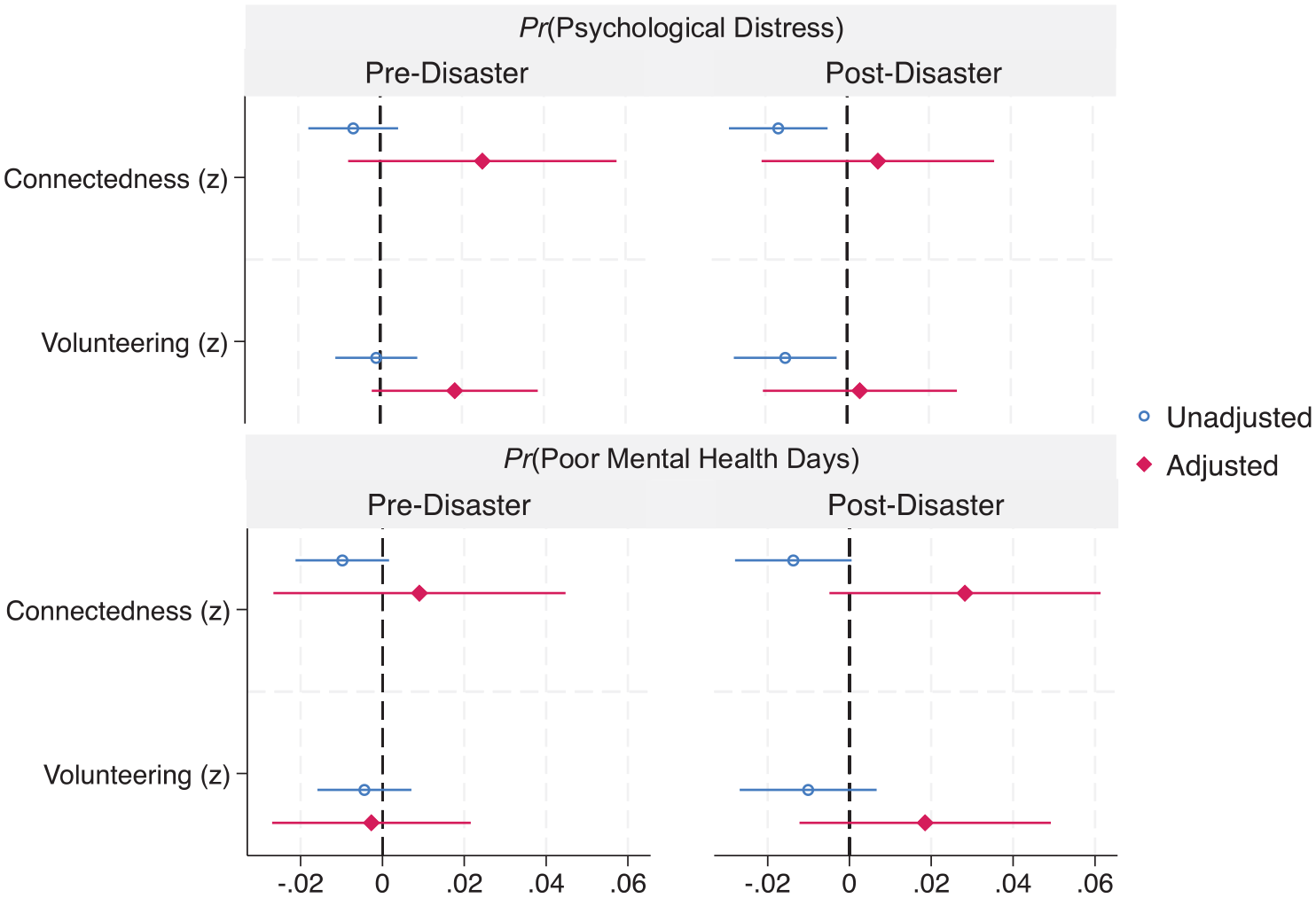
Coefficient plots for the unadjusted and adjusted associations between local social capital and two mental health outcomes before and after Hurricane Harvey in Houston, Texas.
Table 2 presents the results from linear probability estimates of the effect of home damage on mental health, and moderation models for effect variation across local levels of social capital. We first find that home damage was strongly and significantly associated with adverse mental health outcomes, specifically, a 9.3-percentage point increase in the probability of psychological distress (p < .001), and between 18.0 and 18.1-percentage point increase in the probability of poor mental health (p < .001) at average levels of social capital (columns 1, 3, 5, and 7). The main effects in the moderation models on connectedness and volunteering show that neither measure is associated with differences in mental health among people who did not experience home damage (columns 2, 4, 6, and 8). However, three of the four interaction terms reveal at least marginally statistically significant differences by home damage in the relationship between social capital and mental health.
Linear Probability Estimates of Mental Health on Home Damage and Local Social Capital.
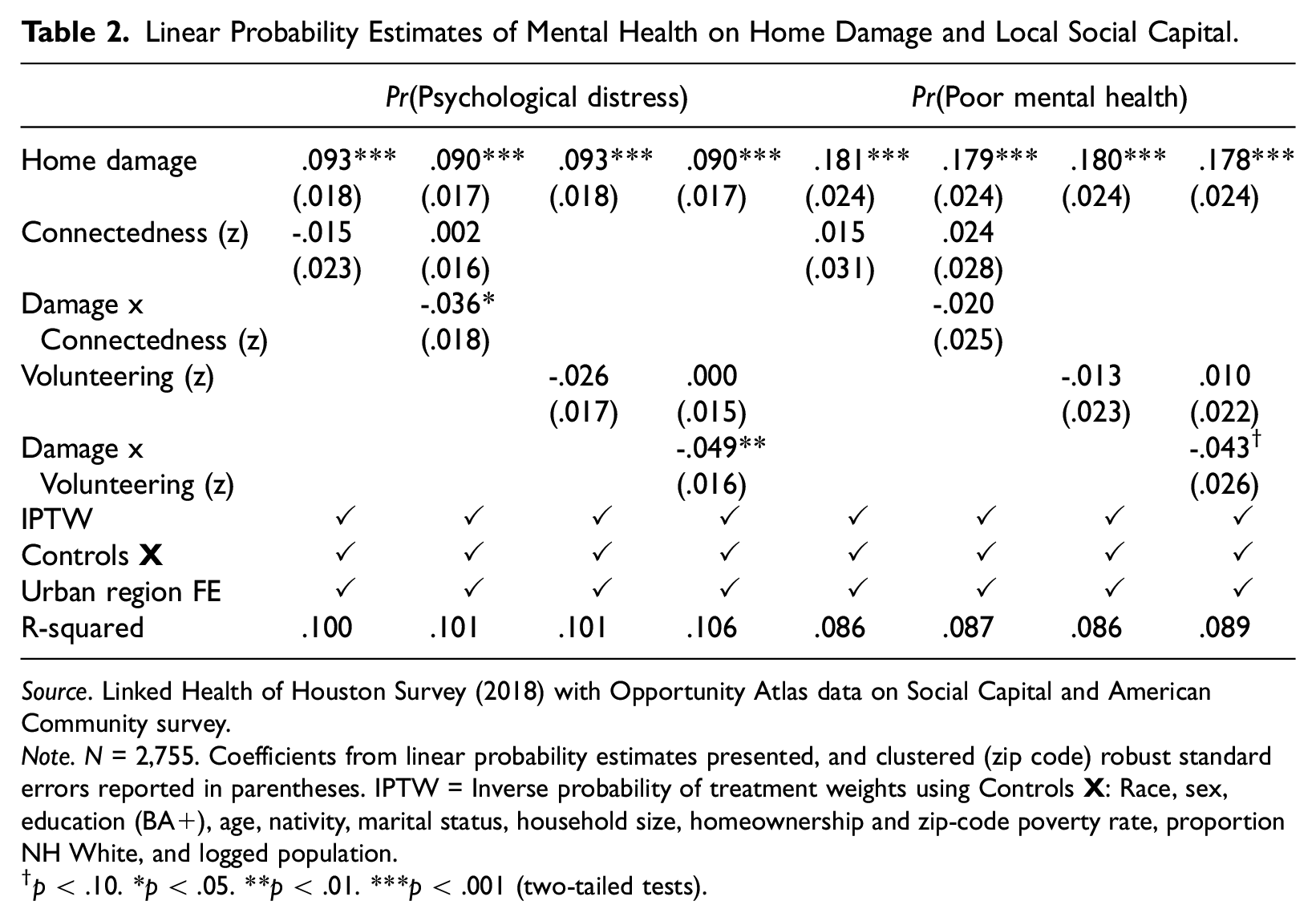
Source. Linked Health of Houston Survey (2018) with Opportunity Atlas data on Social Capital and American Community survey.
Note. N = 2,755. Coefficients from linear probability estimates presented, and clustered (zip code) robust standard errors reported in parentheses. IPTW = Inverse probability of treatment weights using Controls
p < .10. *p < .05. **p < .01. ***p < .001 (two-tailed tests).
To visualize these interactions, Figure 3 displays the predicted probabilities and confidence intervals recovered from the moderation models in Table 2, holding all other variables constant. The predicted probabilities (y-axis) are displayed separately for those with home damage (purple) and without damage (green) home damage across +/- 2 standard deviations of each social capital measure (x-axis). From the first row, we show that among those with home damage, living in a community with higher rates of volunteering and greater levels of connectedness was associated with a lower probability of psychological distress. For example, holding all other variables at their means, respondents with home damage living in a community with 10.5 percent volunteering rate (1.5 SD) had a predicted probability of psychological distress of 0.07 and those with home damage living in a community where 1.5 percent volunteered (−1.5 SD) had a predicted probability of 0.22, nearly triple. Additionally, in every plot of Figure 3, there were significant differences by home damage in the probability of adverse mental health for those living in communities with low social capital (below the mean 0). However, for those residing in high social capital communities (above 1.5 SD of connectedness and volunteering), home damage was not statistically associated with different probabilities of poor mental health or psychological distress. In all cases, this was largely driven by the negative slope of our social capital measures among those with damage. Put another way, mental health impacts were larger among respondents with home damage who resided in low social capital communities compared to those who resided in high social capital communities.
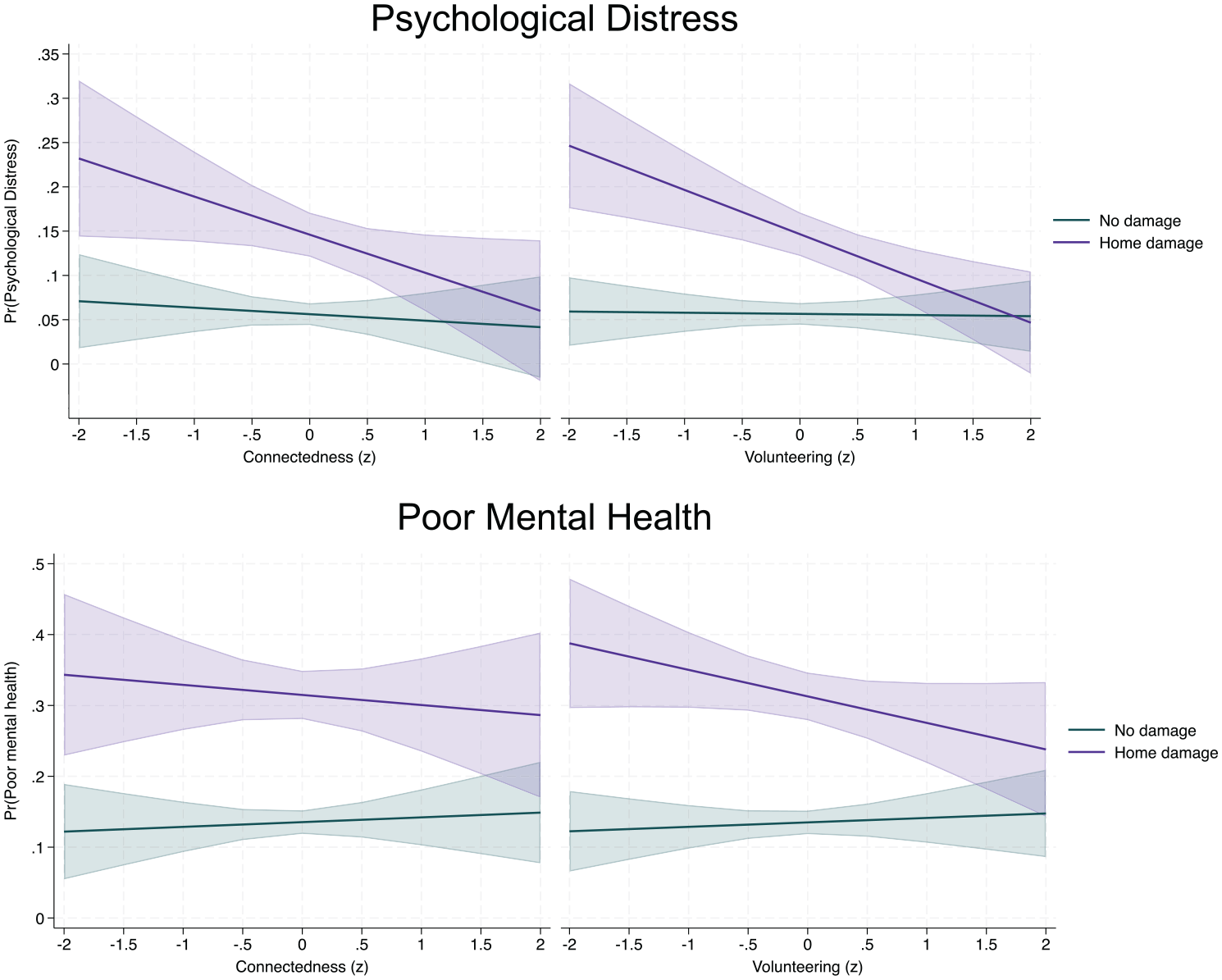
Differential associations between local social capital and mental health outcomes after Hurricane Harvey by home damage.
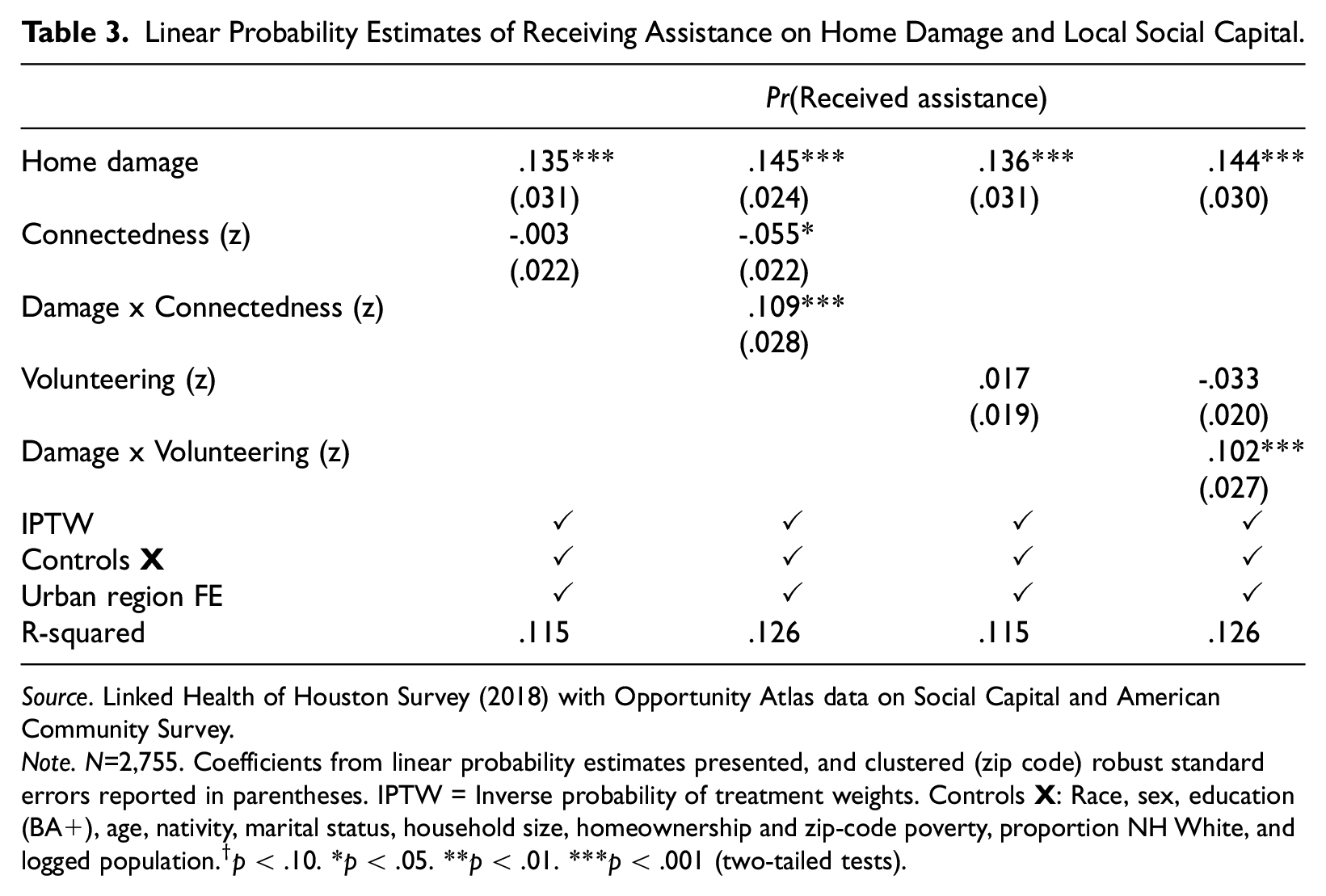
To next test for one potentially health-promoting mechanism correlated with local social capital, we examine differences in the probability of receiving disaster assistance. Table 3 presents the results, and Figure 4 visualizes the interaction models. Overall, those with home damage in the average community were 13.5 to 13.6 percentage points more likely to report receiving assistance (columns 1 and 3). Critically, the probability of receiving assistance was highly influenced by local levels of social capital. For those with home damage, a 1-SD increase in connectedness was associated with a 5.4 percentage-point increase in the probability of assistance receipt (p < .05) (.109–.055), while for those without damage it was associated with a 5.5 percentage-point reduction (p < .05). For those with home damage, 1-SD increase in the local volunteering rate was associated with a 6.9 percentage-point increase in the probability of receiving assistance (p < .05), while the association among those without home damage was negative, it was not different from zero. Figure 4 displays the predicted probabilities holding all other variables at their means, demonstrating that in low social capital communities (less than 1 SD below the mean), there is no difference in the probability of receiving assistance for those with and without home damage. Taken together, the evidence suggests that assistance dynamics are more targeted in higher social capital communities, as those with less need (i.e., no home damage) are relatively less likely to receive assistance and those with home damage are more likely to receive assistance.
Linear Probability Estimates of Receiving Assistance on Home Damage and Local Social Capital.
Source. Linked Health of Houston Survey (2018) with Opportunity Atlas data on Social Capital and American Community Survey.
Note. N=2,755. Coefficients from linear probability estimates presented, and clustered (zip code) robust standard errors reported in parentheses. IPTW = Inverse probability of treatment weights. Controls
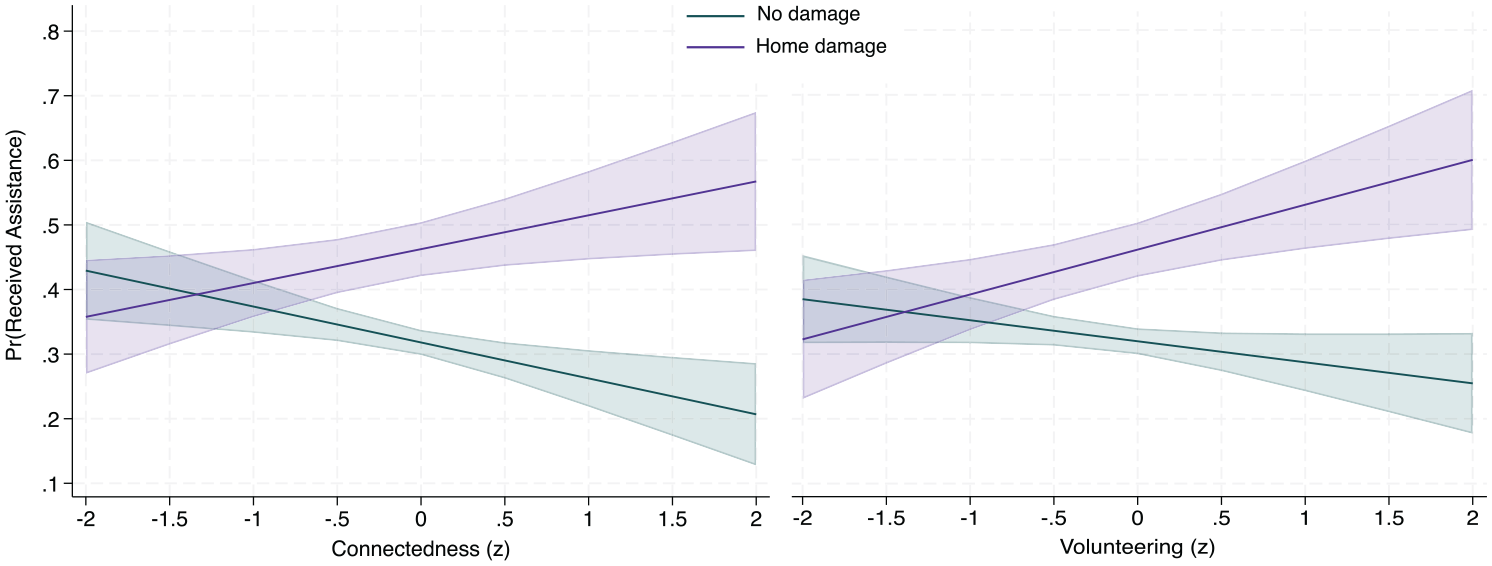
Predicted probabilities of receiving disaster assistance across local social capital, by home damage.
Supplemental Analyses
We conducted supplemental analyses of assistance dynamics and describe the results briefly here. First, to glean further insight into community-level social capital and individual assistance dynamics, we examined two other survey measures: providing assistance, and receiving assistance specifically from neighbors, described above. We replicated the models from results presented in Table 3 but use as dependent variables (1) the probability of providing assistance to others and (2) the probability of receiving assistance from neighbors, conditional on receiving any assistance. Modeling the likelihood that respondents provided assistance to others offers preliminary insights into reciprocity, as social capital may lead to mutual exchanges that reinforce social bonds and trust (Putnam 2000). Results show that, net of reported home damage, individuals living in communities with greater connectedness and volunteering were more likely to report giving assistance and receiving assistance from neighbors, specifically, relative to those living in lower social capital communities (Supplemental Appendix Table A2). However, none of the interaction terms between home damage the two supplemental assistance measures were significant, suggesting no differential impact of community social capital for those with or without home damage.
Discussion
In this article, we examined the relationships between local social capital, mental health, and assistance dynamics in a context of a relatively unexpected and acute form of need–disaster housing damage. We interpret our findings as follows. First, we provided one form of direct evidence against selection bias by showing that before Hurricane Harvey, local levels of connectedness and volunteering were statistically uncorrelated with mental health. Proceeding with this reassurance and by employing region fixed effects to correct for broader forms of residential sorting, we find that the adverse mental health effects of home damage were partially offset for people living in communities with higher levels of social capital, with the strongest evidence for the protective benefits of living in a community with a high rate of civic engagement—that is, volunteering. In line with past research on disaster volunteerism and health (Adams and Boscarino 2015), our findings suggest that civic engagement programs, such as organized neighborhood cleanups or volunteer days at local charities, can have public health benefits in tandem to the civic benefits that promote a sense of belonging in a community.
Situating our findings vis-à-vis past research conclusions clarifies the important role social capital plays in the disaster-health nexus especially given that social capital is a crucial component of resilience (Aldrich and Meyer 2015). Namely, our findings point to the idea that community social capital can be protective of mental health (Wind and Komproe 2012), but that its effect is conditional, namely on home damage. Additionally, there is the key implication that a dark side of social capital (Aldrich 2012; Elliott, Haney, and Sams-Abiodun 2010) may operate insofar as low social capital communities are not protected, which may exacerbate health disparities across places. For leaders of local civic groups and public officials, these findings suggest strong public health benefits from targeting network-based resources to those in acute need in high-social capital communities and widely for residents of resource-low communities.
Our findings also add to our understanding of the impact of community-level social capital on mental health outcomes by exploring the individual-level dynamics of assistance. For one, local patterns of assistance dynamics varied across communities depending on their levels of connectedness and volunteering. While high levels of assistance giving were reporting across various degrees of social capital, people with home damage in higher social capital communities were more likely to receive assistance, relative to those with home damage in lower social capital communities. The difference was such that in the highest social capital communities, people who experienced damage reported statistically similar probabilities of giving and receiving assistance. This suggests potentially more effective targeting and/or widespread availability of assistance in high social capital communities, while lower probabilities of assistance regardless of home damage in low social capital communities points to the opposite case.
Several limitations are necessary to consider. First, as noted previously, we used zip-code-level measures of community social capital that were gathered in 2022, several years after Hurricane Harvey. While we motivated this decision based on theoretical and empirical grounds, we cannot entirely rule out the possibility of unobserved changes in local environments that may lead to bias. Relatedly, the use of Facebook data to measure social capital has benefits discussed above but also potential downsides. For example, the processes by which friendship formation and civic group joining online translates to meaningful social capital in the community remains relatively unclear. Within the growing field of social media studies in disaster (e.g., Houston et al. 2015), future research should address questions regarding the extent to which and how online behaviors affect offline collective processes. Second, our examination of assistance dynamics was reason agnostic and did not principally distinguish formal from informal support. We used survey questions about assistance receiving that did not ask specifically about the reason for accepting assistance. It may be the case that we are capturing aid that was not used to offset the mental health burden of home damage. Future research on disaster assistance dynamics would benefit from more specific inquiry into the acceptance and use of post-disaster resources acquired from others. Third, in the absence of longitudinal data on individuals over time, our empirical strategy used repeated cross-sectional data and a variety of analytical techniques to address bias. Future research should deploy similar techniques to panel data which have the added benefit of controlling for certain types of unobserved confounding. Finally, our social capital data documented very little spatial variation in cohesiveness across zip codes in Houston, a measure of bonding social capital. Future research should seek out contexts in which variation exists to examine this critical form of social capital on post-disaster mental health.
In sum, this article made several advances in the literature on social capital, disasters, and mental health: exploiting pre-disaster survey data to address concerns about selection bias in neighborhood sorting, using state-of-the-art social capital data un-tested in disasters and health research, and a careful review of how mechanisms like disaster assistance do or do not relate to mental health. This transferrable research design not only yields insights for future researchers in the field, but also showcases the critical role that social capital can play in protecting residents with damaged homes from mental health impacts.
Supplemental Material
sj-docx-1-smh-10.1177_21568693241290307 – Supplemental material for Local Social Capital, Disaster Housing Damage, and Mental Health: Insights from Hurricane Harvey
Supplemental material, sj-docx-1-smh-10.1177_21568693241290307 for Local Social Capital, Disaster Housing Damage, and Mental Health: Insights from Hurricane Harvey by Ethan J. Raker and Kevin T. Smiley in Society and Mental Health
Footnotes
Acknowledgements
We are grateful to seminar attendees at UBC School of Architecture and Regional Planning and support from the Peter Wall Institute for Advanced Studies, and to Dritana Marko and Stephen Linder for facilitating access to the restricted-use Health of Houston Survey data. This study was approved by UBC REB (H22-00318).
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.