
Abstract
As well as affecting physical health, COVID-19 can impact mental health. While many studies have examined stigma related to having COVID-19, almost none have examined the larger issue of attitudes toward mental health and stigma since the pandemic began. This study examined public/external mental health stigma among Israelis after the COVID-19 outbreak, including whether there were changes to it. Surveys were administered to a sample of 1,099 Israelis aged 18–55 and multivariate analyses were performed. Israelis were found to have faced increased mental health risks since the COVID-19 outbreak and extensive mental health stigma was found among many of them. However, the stigma was reduced in later months as well as during lockdown periods. Variations in stigma were found by types of stigma and mental health illness, as well as by sociodemographic groups. COVID-19 can negatively impact mental health and appropriate mental healthcare utilization, although there may be positive effects as well. A crisis such as COVID-19 which began as a physical threat can cause society to reconsider how it views mental health, with important and potentially positive implications in the long term, and potential lessons learned for future crises. Interventions are needed, especially when appropriately tailored for vulnerable populations.
Introduction
While there has been great attention given internationally to the dangers of getting infected by COVID-19 and to the associated risks to physical health of morbidity and mortality, there has also been growing awareness of its risks to mental health, both short term and long term (Alimoradi et al. 2022; Czeisler, Howard, and Rajaratnam 2021; Shapiro, Levine, and Kay 2020). Mental health concerns should be viewed not only as a consequence of the stresses of the COVID-19 pandemic, but also as a concurrent epidemic (Castaldelli-Maia et al. 2021). The risks to mental health of COVID-19 have been found in Israel as well, with a concomitant need for appropriate care, and with a number of factors affecting mental healthcare seeking, including potentially positive and negative ones (Hadar-Shoval et al. 2021; Shapiro et al. 2020; Shechory Bitton and Laufer 2021).
It is not only mental health status and access to mental health care that affect the utilization of mental health services (Bauldry and Szaflarski 2017; Hirsch 2016; Shapiro et al. 2020). Another important factor is stigma which can serve as a barrier to the public in consuming appropriate mental health services, with important health policy implications. There are several types of mental health stigma, including public stigma, sometimes called external or enacted stigma. This is the stigma directed from members of the community toward the person with the stigmatized condition, often resulting in negative mental health outcomes (Corrigan, Palermo, and Sheehan 2022; Corrigan et al. 2012). In particular, public stigma has been found to be an important cause of social exclusion, which has been strongly associated with poorer mental health outcomes (Boardman 2011; Morgan et al. 2007).
However, not enough is known in general about mental health stigma and, in particular, about how the COVID-19 pandemic may have impacted public stigma. To help fill this gap, this cross-sectional study analyzed a sample of Israelis to examine both the mental health challenges experienced by this community during COVID-19 and barriers to utilization, in particular levels of stigma that can reduce mental health care (Shidhaye and Kermode 2013; Sickel, Seacat, and Nabors 2019).
Background
Mental Health Stigma and Its Consequences
Stigma is a potentially important barrier to people receiving needed health services as people are not willing to get care even when it is available. It is a term originally invented in Ancient Greece (Economou, Bechraki, and Charitsi 2020) and developed and popularized in more modern times from Goffman’s (1963) pioneering work. Stigma that is mental illness-related often reduces people’s willingness to seek out needed mental healthcare services and creates serious barriers to access and quality care (Greenberg and Witztum 2013; Knaak, Mantler, and Szeto 2017).
There are a number of sociological styles of thinking about mental disorders (Horwitz 2013). While some focus on how symptoms arise in individuals and the most common style accepts the prevailing definitions of mental illness and searches for the social causes of these conditions, other styles focus less on the illness itself and more on how social factors affect responses to mental disorder. One of these latter styles analyzes the variation in the reaction of others to individuals’ symptoms. Mental health stigma is an important example of this type of reaction and it is typically associated with worse mental health outcomes (Knaak et al. 2017; Miconi et al. 2021; Parcesepe and Cabassa 2013).
The extent of stigma toward others, often called public stigma (Corrigan et al. 2022), is influenced by the society that surrounds the person. It has culture-dependent characteristics and can lead to the avoidance of appropriate mental health services utilization (Al-Krenawi et al. 2009; Bracke, Delaruelle, and Verhaeghe 2019; Miconi et al. 2021). Public stigma can lead to discrimination against and stereotyping of those individuals who seek needed mental health care (Corrigan et al. 2012). It can also lead to self-stigma, whereby people with mental illness apply negative stereotypes about mental illness to themselves, thus harming their mental health (Corrigan et al. 2022).
Causes of Stigma
There are a number of potential causes of public stigma (Corrigan et al. 2022). For example, two prominent researchers about stigma, Link and Phelan (2001), described a process whereby differences are perceived between groups, negative stereotypes about the group develop on a societal level, an “us versus them” mentality forms, and thus people in one group experience discrimination and loss of status from being labeled (Link and Phelan 2001).
However, even half a century after Goffman (1963) wrote his book about stigma, Link and Phelan (2014) wrote that large gaps in understanding about it remain. In particular, they emphasized that there was much that needs to be done in terms of fulfilling the promise of some of the concepts and theories already introduced. Their primary recommendation was for the development of a sociologically informed approach to stigma change.
In the decade since, there has indeed been more emphasis on aspects of the social environment which can affect stigma. People’s interactions with others with mental illness can affect levels of public stigma. Sociological factors, including social support, social networks, and social interactions, can be related to stigma (Brown and Ciciurkaite 2017; Felix and Lynn 2022; Pescosolido and Manago 2018). While the literature is mixed about the exact impact of these factors on stigma, both the quantity and quality of them can have an effect, although there can be nuances to the nature of the interaction. For example, a recent study found that more contacts with those suffering from mental health illness is associated with less stigma but it depends on whether those relations are characterized by closeness and a lack of negativity (Felix and Lynn 2022).
The extent of stigma can also be related to different contexts/characteristics including neighborhood, workplace, place of learning, and ethnic identity (Elraz 2018; Gonzales et al. 2018; Miconi et al. 2021). Stigma has also been found to be related to another problem, lack of knowledge about identifying mental health issues and where and when to seek appropriate care for them or what is sometimes called mental health literacy (Kutcher, Wei, and Coniglio 2016).
Another important consideration is that the process of stigmatization depends upon social, economic, and political power (Link and Phelan 2001). Even though both powerful and powerless groups can stigmatize each other, the former group’s views are likely to prevail in many settings because they often control the latter’s access to resources.
The extent and impact of stigma can also vary for different mental illnesses, such as schizophrenia and depression, because of different perceptions about the illnesses which may not always be related to the illness itself (Rössler 2016; Struch et al. 2008). For example, there may be a greater willingness to have a connection with someone diagnosed with depression compared to a schizophrenic patient (Struch et al. 2008).
COVID-19 and Mental Health Stigma
While there has been great attention given internationally to the dangers of getting infected by COVID-19 and to the associated risks to physical health of morbidity and mortality (Chang et al. 2022), there has been growing awareness of the risks to mental health and well-being. The impact of COVID-19 on mental health was exceptional, with an increase in threats to mental health because of the increase in mental health stressors, both new and existing ones (Alimoradi et al. 2022; Hossain et al. 2020). As in other countries, there has been great stress, anxiety, and risk of depression found among Israelis during COVID-19, with variations observed by demographic groups (Shapiro et al. 2020; Shapiro, Levine, and Kay 2021; Shechory Bitton and Laufer 2021). Mental health distress seems to have worsened among Israelis who previously had mental health issues (Kimhi et al. 2021).
At the same time that there has been a greater need for mental health care during COVID-19, there has often been lowered access to mental healthcare services as a result of restrictions on travel and people’s fears of exposure to the virus (Hoyer et al. 2021; Li et al. 2022). However, there has been little attention to stigma as a factor. Most of the research about stigma during the period of COVID-19 seems to be focused on stigma toward physical health, especially those who have been infected with the coronavirus (Gronholm et al. 2021; Wahyuhadi et al. 2022).
Mental Health Care in Israel
Israel has universal health insurance, and Israeli citizens are entitled to a comprehensive “basket” of healthcare services provided by one of four health plans (called kupot in Israel, which are similar to health maintenance organizations), with citizens receiving a basic package of mental health services (Rosen, Waitzberg, and Merkur 2015). In 2015, Israel implemented a mental health reform that transferred the responsibility for providing mental health services from the State (Ministry of Health) to the health plans. The expectation was that this would normalize mental health services and could reduce stigma. However, many issues remained unresolved after the reform and it did not appear to reduce stigma (Aviram and Azary-Viesel 2018; Ben Natan, Drori, and Hochman 2017).
In terms of healthcare needs, almost one in five Israelis surveyed in a nationally representative sample reported feeling mental health distress within the prior 12 months that was difficult for them to deal with on their own (Elroy et al. 2017). The survey found that only 36 percent of those reporting feeling mental health distress within the past 12 months sought treatment from a mental health professional, 47 percent turned to other sources for help, and 23 percent did not seek treatment at all (Elroy et al. 2017). A more recent study found decreased rates of using any mental health service; rates decreased with age, with a decrease of 25 percent in the oldest age group (Blasbalg et al. 2023).
Mental health distress has been disproportionately found among vulnerable populations in Israel (Refaeli and Krumer-Nevo 2021). Furthermore, a lack of appropriate utilization of mental health services in Israel has especially been found among minority groups (Dovromilcin 2015; Elroy et al. 2017). Arabs, Haredi (ultra-Orthodox) Jews, and Ethiopians in Israel may face special barriers and/or be less likely to use mental health services when there is a need (Elroy et al. 2017; Fahoum and Al-Krenawi 2021; Greenberg and Witztum 2013; Shapiro, Mekonent, and Tanami 2023).
Mental health stigma, including public stigma, is widespread internationally but there are important variations by country (Seeman et al. 2016). Israel has distinctive culture and social structures which can influence both mental health distress and public mental health stigma there. While often considered a Westernized country, Israel is also a very traditional and religious country with one poll ranking it number one in terms of religiosity (Anon 2022b). Religious Jews and Muslims may not necessarily trust the healthcare system to be sensitive to their distinctive needs or to fully understand their religious outlook; studies have revealed that both Orthodox Jews, particularly Haredi (ultra-Orthodox) Jews, and religious Muslims are less likely to seek mental health services (Al-Krenawi 2002; Fahoum and Al-Krenawi 2021; Greenberg and Witztum 2013).
There are also issues of the cultural adaptation of the healthcare system to different populations in Israel (Ben-Yehuda 2015). Israel is a diverse country ethnically, with almost 20 percent of its population having immigrated from a diversity of countries (Anon 2022a), many with different attitudes that can potentially affect mental health and willingness to use mental health services (Shapiro et al. 2020, 2023) Mental health stigma can also be related to a number of aspects of people’s lives, including those especially prominent in Israeli society, such as the military or studying in religious institutions (Gibbons et al. 2014; Greenberg and Witztum 2013; Schneider et al. 2023).
There is extensive socioeconomic inequality in Israel which is connected with disparities across a range of health outcomes including mental health (Averbach et al. 2021). There are also divisions and tensions between dominant and minority groups which result in social divides. These may cause Arabs and other minority groups to mistrust the mental healthcare system and reduce utilization (Fahoum and Al-Krenawi 2021; Pinchas-Mizrachi, Zalcman, and Daoud 2020).
While there has been speculation, especially in the popular press, that mental health stigma may have been reduced during COVID-19, there have been few academic studies on the topic (Beckford 2022; Gold 2020). This lack is even more problematic because as noted there is some evidence of an increased need for mental healthcare services yet decreased availability of such services since the start of COVID-19. Furthermore, to our knowledge there has been no research about mental health stigma since the COVID-19 pandemic in Israel, a country with distinctive cultural characteristics that could affect mental health and mental healthcare utilization of both Jews and Arabs (Elroy et al. 2017; Hadar-Shoval et al. 2021; Khatib and Abo-Rass 2022).
Research Questions
What is the extent of mental health-related public stigma among Israelis within the sociodemographic context of Israel (ethnic sector, religiosity, gender, etc.)?
How does it vary by context of the stigma (romance, education, neighborhood, etc.)?
Has the level of mental health-related public stigma changed during the COVID-19 outbreak?
Data and Methods
Data for this study come from a custom-designed survey on attitudes toward mental health stigma. A survey of Israelis was conducted to identify mental health stressors and barriers to the appropriate use of mental health services, in particular stigma and lack of mental health-related knowledge. A 49-question survey ethnicity instrument was developed in Hebrew by the research team and implemented using Qualtrics XM software. Where questions were based on an English language tool, validated Hebrew translations were used when possible or, when not, translated professionally for this survey. The final survey was professionally translated into Arabic. The digital questionnaire used for this study was answered and commented on by a diverse pilot group of 25 Israelis which included some Arabic speakers. The survey was modified based on pilot results, to improve survey clarity and reduce the survey length and to try to increase survey quality and the number of responses.
The study sample consisted of 1,099 Israelis between ages 18 and 55. Data were collected from August 2020 to January 2021. During this period, several government regulations were in place, including masking and social distancing requirements. This date range also included two strict lockdown periods in Israel where people were only allowed to go out only under very limited circumstances. Vaccination had not yet started.
Questionnaires were administered to a sample based on a representative national list of telephone numbers of 4,000 Israeli adults between the ages of 18 and 55, as per the study’s inclusion criteria. While the list used to recruit survey respondents was representative, to the extent that the response rates differed by demographic variables, the actual sample was not necessarily fully representative. In addition, the minority groups of Arabs and Haredi (ultra-Orthodox) Jews were oversampled, with the list containing 30 percent Arab and 20 percent Haredi names, each being about 50 percent larger than their actual proportion in the population.
Efforts were made to maximize response rates. Up to five attempts were made to contact each person. When phone attempts were not successful or if the interviewee requested it, a link to an online version of the questionnaire was sent when possible. There was a team of eight interviewers, including those from the target minority groups, who all received training and oversight from the Primary Investigator. Study endorsements were obtained in advance from several Haredi rabbis to encourage people in religious Jewish populations, especially Haredi Jews, to agree to participate as is recommended (Rier, Schwartzbaum, and Heller 2008).
Of the names on the list, not all had working phone numbers or were eligible for the study. Of those eligible and who answered the phone or responded to the message, 41 percent participated in the survey.
Measures
Dependent variable
The questionnaire focused on mental health status, mental health stressors related to COVID-19, barriers to mental health service utilization, as well as demographic characteristics. There was an extensive group of questions about stigma and lack of mental health knowledge. Previously validated questions were used to the extent possible. The Community Attitudes To Mental Illness (CAMI) scale was used to help measure external stigma (stigma toward others, sometimes also called public stigma). The standard CAMI is a widely used tool containing 40 items on a 5-point Likert-type scale (1 = disagree strongly, 2 = disagree slightly, 3 = neither agree nor disagree, 4 = agree slightly, 5 = agree strongly) designed to assess community attitudes toward the mentally ill through four different dimensions, namely social exclusion, authoritarianism, benevolence, and community mental health ideology (Taylor and Dear 1981), and which is often used to measure stigma, including since COVID-19 (Benassi et al. 2020; Sanabria-Mazo et al. 2023). The CAMI’s properties were evaluated using a number of studies (Sanabria-Mazo et al. 2023). Internal consistency has generally been found to be good, and test-retest results were more mixed, with some but not all studies showing acceptable scores. Correlations between the CAMI and other potentially related constructs were statistically significant and in the expected directions. We also chose to use the CAMI both because it widely used in general to measure social exclusion and because it had previously been used and validated with Israeli populations (Ben Natan et al. 2017; Sanabria-Mazo et al. 2023).
A five-question version of the social exclusion portion of the CAMI was used (Cronbach’s alpha = .80; Taylor and Dear 1981); social exclusion has been strongly associated with poorer mental health outcomes (Boardman 2011; Morgan et al. 2007). The scale was adapted for Israeli society by adding two questions, one about military and national service and another about studying in religious institutions. The revised scale was still found to be acceptably reliable (Cronbach’s alpha = .74). Many of the individual questions about mental health status and utilization were taken from an earlier validated survey on the topic performed by the Myers-JDC-Brookdale Institute (Elroy et al. 2017).
Key explanatory variables
The survey questions concerning mental health status and stressors were taken from validated questionnaires such as the Patient Health Questionnaire-2 depression screening tool (Mitchell et al. 2016) and the General Anxiety Disorder-2 anxiety risk screening tool (Plummer et al. 2016). Responses were coded as 0 = not at all, 1= several days, 2= more than half the days, and 3 = nearly every day. The survey also asked about mental health distress, a mental health measure of nonspecific symptoms often connected with anxiety and depression, commonly used in Israel and elsewhere (1 = Yes, 2 = No; Elroy et al. 2017; Viertiö et al. 2021).
The full six-question knowledge portion of the Mental Health Knowledge Scale (MAKS) was used to measure knowledge about mental health (Evans-Lacko et al. 2010). The MAKS is a widely used tool used to better understand how improvements in mental health-related knowledge might lead to changes in attitudes or behaviors and has previously been used for studies of a diversity of demographic groups, including Jews and Arabs (Abi Doumit et al. 2019; Shapiro et al. 2023). Responses were coded on a 5-point scale (1 = disagree strongly, 2 = disagree slightly, 3 = neither agree nor disagree, 4 = agree slightly, and 5 = agree strongly). A study tested internal consistency for the MAKS and found a Cronbach’s alpha of .65.
The pilot revealed that many people said their answers to the CAMI questions depended on specific illness, but the original questions refer to mental health illness in general. Therefore, respondents were also asked to what extent their answers to the CAMI questions would generally have changed if a more common/less severe mental health illness (depression) and a less common/more severe mental health illness (schizophrenia) were specifically asked about. Responses were coded as 1 = more likely to agree, 2 = no change, 3 = less likely to agree, and 4 = not sure.
Respondent characteristics
A variety of demographic questions were asked of respondents. These included: age (1 = 18–29 years, 2 = 30–39 years, 3 = 40–55 years), gender (1 = male, 2 = female), ethnic sector (1 = Jew, 2 = Arab), religion (1 = Jew, 2 = Muslim, 3 = other), religiosity level (1 = secular, 2 = traditional, 3 = religious, 4 = very religious/Haredi), education level (1 = did not graduate from high school, 2 = high school graduate), marital status (1 = never married, 2 = married, 3 = formerly married), and country of birth (1 = Israel, 2 = another country).
Analytic approach
Descriptive analyses were performed for all variables relevant to the research questions as well as demographics. To determine what factors affected external stigma, a linear regression analysis was then performed in three phases. The dependent variable was a scale based on the seven questions, scored using the CAMI scale as is commonly done with the CAMI (Taylor and Dear 1981), with each question receiving 1 to 5 points based on response (1 being the least stigma and 5 the most). One question was reverse coded because agreement with the question indicated less stigma. Therefore, scores could range from 7 to 35.
In the first phase, independent variables were demographics as well as how type of mental health illness affected responses. In the second phase, variables related to the COVID-19 time period were added. These were month number of the study period when the interview was conducted (coded as 1 through 5) and whether the interview occurred during one of the two lockdown periods that coincided with the study period (coded as 1 = lockdown period and 0 = no lockdown). As there was no systematic reason for someone to be interviewed in a particular month and as key sample variables related to stigma that may have varied each month were controlled for in analyses, any population-level differences in stigma levels between months could be identified. In the third phase, variables related to the relationship of the COVID-19 period and stigma were added. In analyses, responses to questions were collapsed into three categories or dichotomized when appropriate to increase analytical power. Analyses were performed using SPSS version 23.
Ethics
The study was approved by the ethics committee of the university. All respondents consented to participate verbally or in writing.
Results
Sample Description
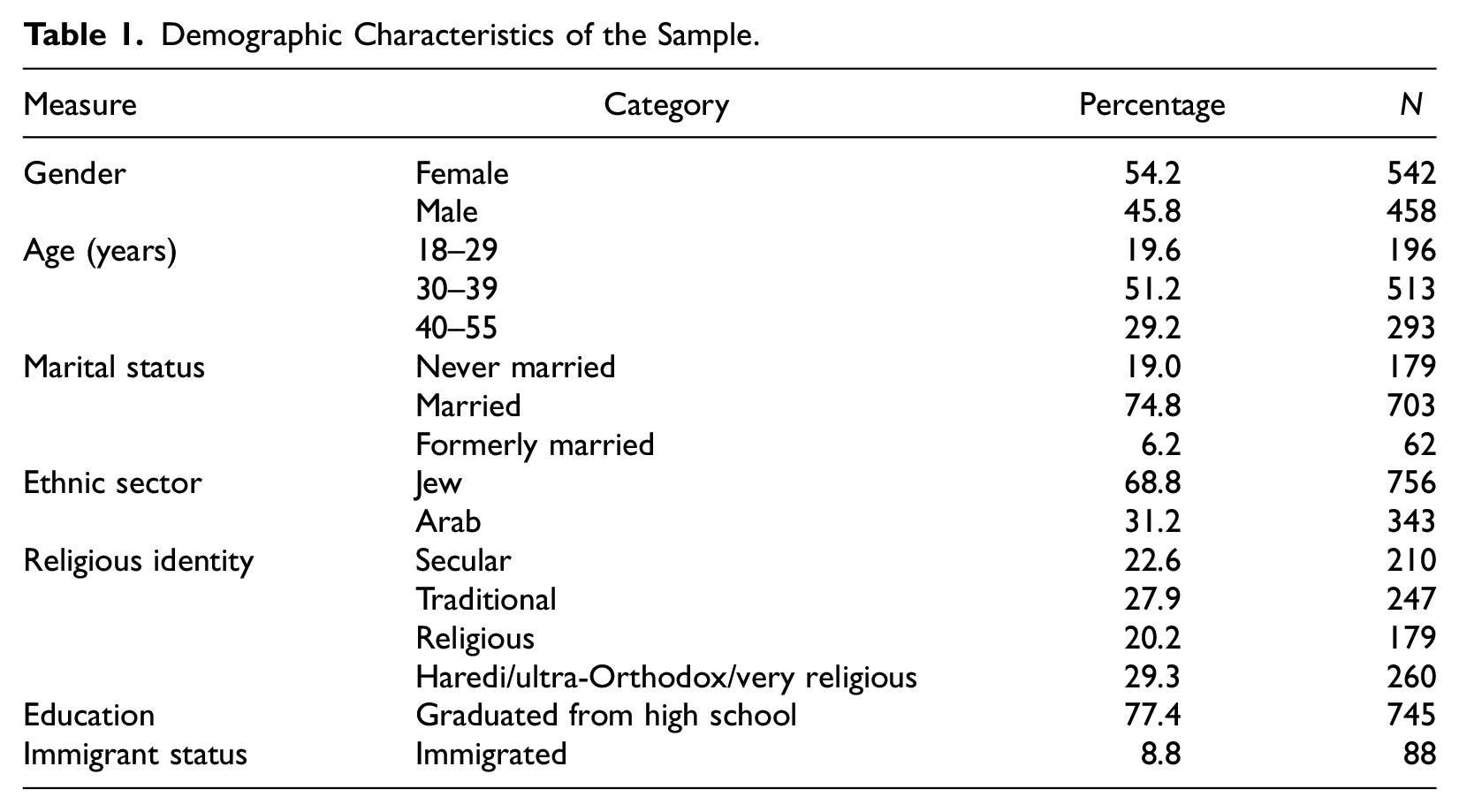
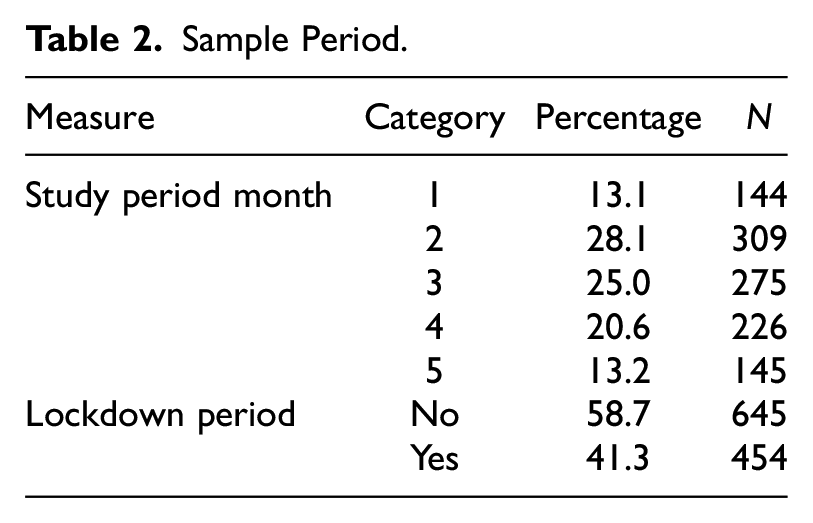
Table 1 presents statistics for sample demographics. The sample represented a diversity of demographic characteristics: the range of ages was 18–55, with slightly over half the sample being between the ages of 30 and 39. Over 54 percent of the sample were female and almost 75 percent of the sample were married. Almost 69 percent of respondents were Jewish and 31 percent were Arab. In terms of religious identity, 28 percent defined themselves as secular, 23 percent as traditional, 20 percent as religious, and 29 percent as very religious (among Israeli Jews, called Haredi). Sample sizes for study respondents each month and during lockdown periods can be found in Table 2. Respondents were interviewed over a five-month period, with about 41 percent of the interviews also occurring during a lockdown.
Demographic Characteristics of the Sample.
Sample Period.
Mental Health Status
Table 3 presents findings for mental health status. Overall, respondents generally reported good health and wellness but also experienced important levels of mental health distress both during their lifetimes and during the period since the COVID-19 outbreak. Respondents were asked to rate their happiness on a scale from 1 to 7 and the average score was 5.95. Almost 64 percent reported that their health was at least very good and only 7.2 percent reported health of fair or below. Slightly over a third of respondents (35 percent) reported having experienced mental distress such as anxiety, depression, stress, and so on, while 53.1 percent said they did not, and an additional 6.9 percent were unsure.
Measures of Well-being and Mental Health Status.

Note. Depression risk based on Patient Health Questionnaire-2 score of 3 or more. Anxiety risk based on General Anxiety Disorder-2 score of 3 or more.
Mental health status and stressors have worsened since the start of COVID-19. About 35 percent of respondents said they had experienced greater mental health distress since the outbreak in March 2020, while only about 3.4 percent felt less distress. Slightly more than 75 percent experienced increased concern about their and their family’s health but only 2.3 percent felt less distress.
Mental Health Stigma
Table 4 presents findings about different types of external mental health stigma. We examined seven types of stigma toward others, based on the CAMI tool questions, including the two questions adapted for an Israeli population. Respondents were read statements expressing stigma and asked to what extent they agreed with them: strongly agree, agree, neutral, disagree, and strongly disagree. Responses were categorized as disagree, agree, or neutral. Percentages of respondents agreeing with a statement indicating stigma and disagreeing or neutral can be found in Table 4.
Extent of Mental Healthcare Stigma toward Others.

The greatest amount of stigma was exhibited in connection to marriage, with 21.1 percent of the sample agreeing that “A woman would be foolish to marry a man who has suffered from mental illness, even though he seems fully recovered.” Furthermore, 19.2 percent of respondents agreed that “The mentally ill should not be given responsibility over anything.” The least stigma was shown in response to the statement that “the mentally ill should be isolated,” with only 5.1 percent agreeing with this idea. When the sample was asked if they would live next door to someone who had a mental illness, 12 percent said they would not want to live near such a person. In addition, 11.3 percent of respondents were unwilling to serve in the military or perform national service with someone mentally ill and 11.5 percent of the sample agreed with the idea that someone with mental illness should not learn in a yeshiva/religious seminary. One CAMI question was asked in a positive direction, with 11.3 percent disagreeing that the mentally ill are far less of a danger than most people think.
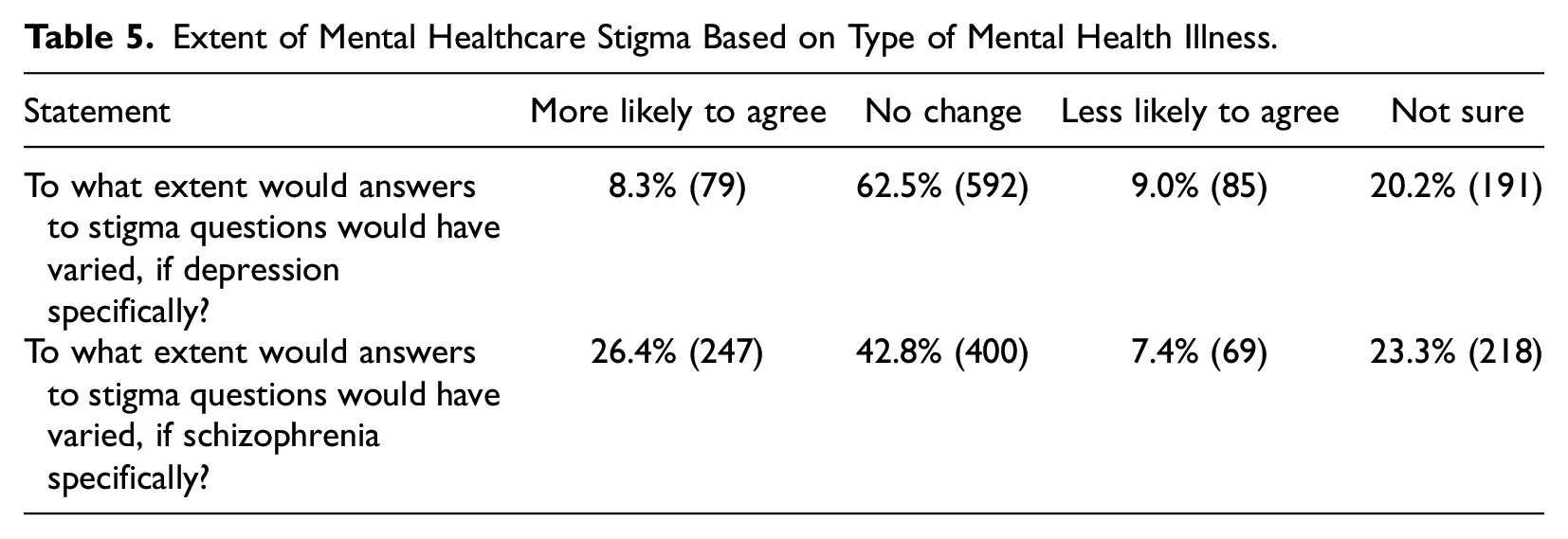
Respondents were also asked to what extent their answers to the CAMI questions would generally have changed if a specific mental health illness, schizophrenia or depression, was mentioned. Findings are presented in Table 5. If the questions had specifically mentioned schizophrenia rather than just a generic “mental illness,” 26.4 percent said they would have generally been more likely to agree with questions, thereby indicating greater stigma. If the questions had specifically mentioned depression, a smaller percentage than schizophrenia (8.3 percent) would have been more likely to agree.
Extent of Mental Healthcare Stigma Based on Type of Mental Health Illness.
Mental Healthcare Attitudes and Knowledge
Table 6 describes findings for mental healthcare utilization and related knowledge and attitudes about the healthcare system, using the questions from the relevant portion of the MAKS described above. In general, while most respondents knew the correct answers to questions about mental health care, large minorities did not. Only 60 percent said they would know what advice to give a friend with a mental health problem to get them professional help, while 22 percent did not, with the remainder being neutral. About 78 percent of respondents thought psychotherapy could be an effective treatment for mental health problems, while only 4 percent did not. Over 68 percent thought medications could be an effective treatment but 11 percent did not. However, only 48 percent thought people with severe mental health problems can fully recover, while 24 percent did not. Almost 39 percent of respondents did not agree that most people with mental health problems go to a healthcare professional to get help, while 34 percent agreed.
Mental Healthcare Attitudes and knowledge (MAKS).
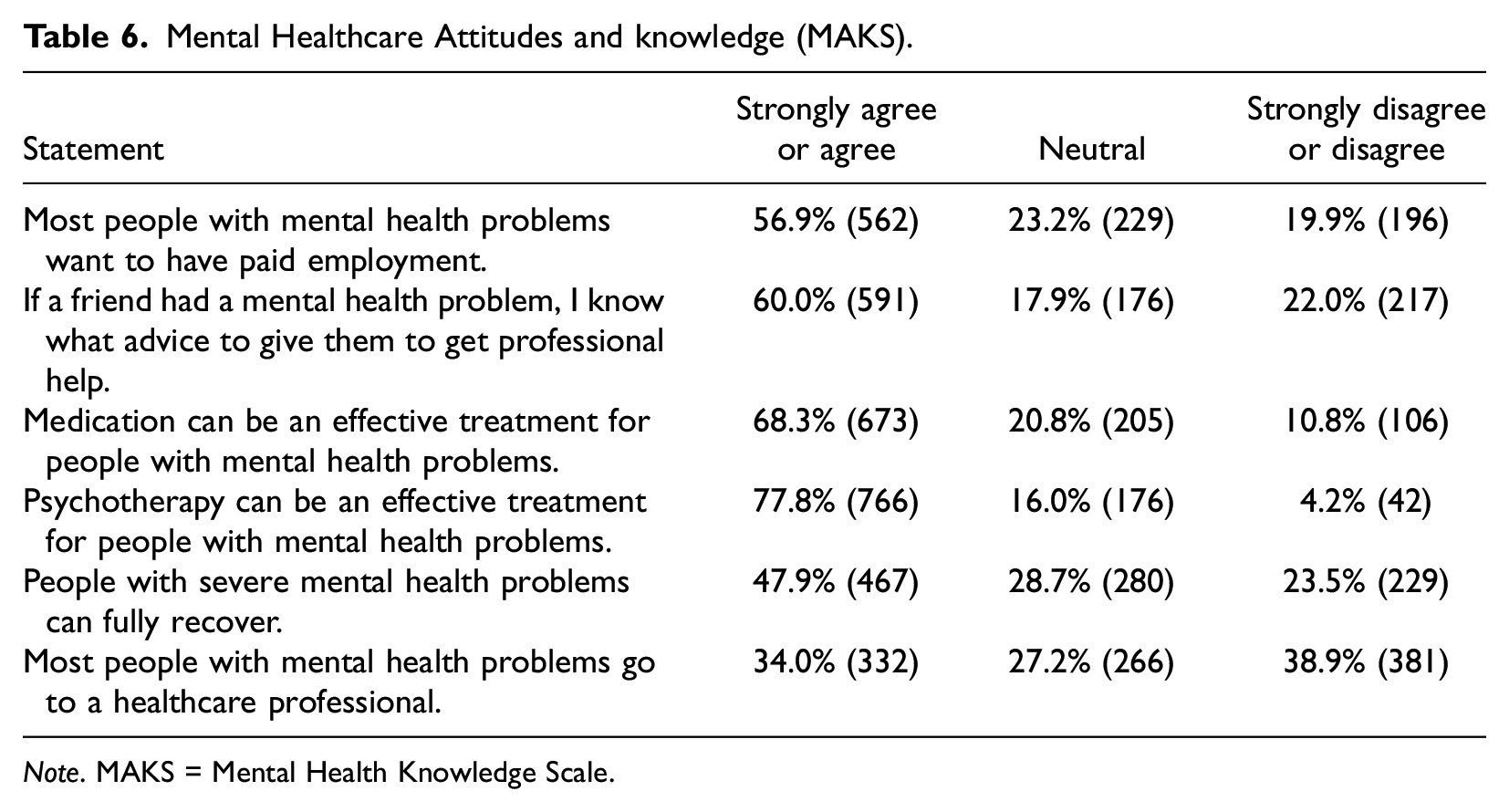
Note. MAKS = Mental Health Knowledge Scale.
Multivariate analyses
To determine what factors were associated with public stigma, linear regression analyses were performed. The dependent variable was a scale based on the seven external stigma questions, scored using the CAMI scale, with each question receiving 1 to 5 points based on response (1 being the least stigma and 5 the most), thus scores ranged from 7 to 35. Standardized and unstandardized beta coefficients as well as standard errors were produced for all variables. Regression diagnostics did not indicate any problems. Multicollinearity between study independent variables was very low (for all, variance inflation factor ≤2). A plot of regression standardized residuals and a regression standardized predicted value scatterplot were produced and indicated that the sample had the desired homoscedasticity.
In the first model, independent variables were demographic variables as well as how type of mental health illness affected responses. Results are found in Table 7. Among demographic variables, ethnic sector and religiosity were strongly associated with greater external stigma (p < .001), with being Arab and being more religious associated with greater stigma, with adjusted betas of .470 and .183, respectively. Not being married and being in an older age category were also associated with greater stigma (p < .01). Being an immigrant and having greater education were associated with greater stigma but only at a marginally significant level (p < .10). Gender was not associated with stigma at even this level. Having the stigma questions refer specifically to schizophrenia was associated with greater stigma (p < .001), with an adjusted beta of .245, while having the stigma questions refer specifically to depression was associated with less stigma but with a smaller effect size of −.082 and only at a marginally significant level (p < .10). The adjusted R2 of the model was .304.
Results of Ordinary Least Squares Regression Models for Stigma Level Based on CAMI Score.

Note. N = 778. Positive beta means more stigma. CAMI = Community Attitudes Toward Mental Health; HS = high school.
p < .1. *p < .05. **p < .01. ***p < .001.
p values are for one-tailed tests.
It should be noted that the question about military/national service is less relevant to populations such as Arabs and Haredi Jews where a much smaller proportion serve and the question about religious seminaries may also be less relevant to the Arab population as well as to Haredi women. To address this issue, a sensitivity analysis was performed, and analyses rerun without these two questions. Major findings remained and, although effect size decreased, the ethnic sector and religiosity variables were still the two demographic variables most associated with stigma.
To test whether the extent of stigma was associated with the COVID-19 period, including lockdowns, two additional variables were added to the second model, study month number and whether the interview took place during a lockdown. Each additional month of the study period was associated with less stigma (p < .01), with an unadjusted beta of −.356, indicating a decreasing amount of stigma during the COVID-19 period being studied. There was also an additional impact of a lockdown period, with less stigma during these periods (p < .05), with an unadjusted beta of −.679. Results for the other variables generally did not change in substantial ways, although the statistical significance levels for education and marital status both increased. Adjusted R2 of the model increased to .327.
In the third phase of the regression, potential factors associated with changes in stigma during the period of COVID-19 and lockdowns were examined. Based on literature as well as key informant interviews, potential reasons for the lowered stigma were greater knowledge about mental health as well as greater personal sensitivity to mental health issues because of the stresses of the period. To test this, mental health knowledge and mental health distress variables were added to the third model. To measure knowledge, we used the six-question MAKS coded from 5 to 30. It was found to be associated with less stigma (p < .001), with an unadjusted beta of −.270. To test mental health distress, we initially used change in mental health distress since COVID-19 to measure mental health status. When this was not found to be significant, we instead added a variable for whether they had ever experienced a mental health issue. This variable was associated with less stigma (p < .01). Those who had never had a mental health issue had an unadjusted beta of .808. After the addition of these two variables to the model, there was a modest decrease in the effect size of the study month and lockdown periods, indicating there was likely at least partial moderation. Among other variables in the model, the main changes that were noteworthy were that education and immigrant status were no longer statistically significant. The adjusted R2 of the model increased to .356.
Discussion
This study adds to the body of knowledge about stigma toward mental health during the period of COVID-19, a topic that has been, perhaps surprisingly, understudied. COVID-19 is not just a threat to physical health but also to mental health, an issue that has received growing attention since the outbreak (Byrne, Barber, and Lim 2021; Shapiro et al. 2020; Venkatesh and Edirappuli 2020).
This study analyzed a national survey of Israelis during the second half of COVID-19’s first year. It found that large numbers of Israelis have had mental health issues, are currently at risk for depression and anxiety, and are not at the highest levels of well-being. Furthermore, mental health distress for many people has increased since COVID-19’s start. The current study’s results are also consistent with other research finding a general decrease in mental health status and an increase in stressors in Israel since the start of COVID-19 (Konstantinov et al. 2021; Shapiro et al. 2020).
At the same time, while a minority, many Israelis exhibit public/external mental health stigma. The extent of this stigma can vary based on context, ethnic subgroup, and mental health issue. However, interestingly, our analyses also found that the stigma appears to have decreased since the start of COVID-19, especially during lockdowns.
Because of the Israel-Hamas war that began in October 2023, the topic of this research has likely become even more relevant since it was conducted. In general, wars create stresses on mental health and a need for appropriate care (Rozanov et al. 2019). This is especially likely to be true in Israel where there are longstanding divides and inequalities related to health among different sectors of society (Averbach et al. 2021). There are initial indications that the war has resulted in a record-high prevalence of mental health problems in both adults and children; in one survey, 60 percent of Israelis who weren’t directly affected by the war developed severe acute stress disorder (Gil-Ad and Trabelsi-Hadad 2023). The traumatic events related to the war will also likely lead to the need to cope with Post-traumatic stress disorder (PTSD) (Zukerman et al. 2016).
The decrease in mental health-related stigma may be a “silver lining” to the COVID-19 outbreak (Beckford 2022). This study points to several potential reasons why public stigma may have decreased during the period of COVID-19. Greater knowledge about mental health care based on the MAKS was associated with less stigma, consistent with other research (Abi Doumit et al. 2019). The increased attention in academic articles, popular media, social media, and in everyday conversations because of COVID-19-related mental health stressors likely has increased people’s awareness of the importance of mental health (Byrne et al. 2021; Gold 2020). It is less clear why lockdown periods would have been associated with less stigma. A qualitative study did find that mental health literacy increased during lockdowns (Jansli et al. 2022). However, the reasons for this are unclear and warrant further research.
The study also found that having experienced a mental health problem was associated with less public stigma. This may lead to greater empathy toward others and also to a greater understanding of the importance of getting appropriate care during the period of COVID-19 or other crises when there are threats to mental health (Fleary et al. 2022; Kimhi et al. 2021). However, it is unclear why having increased mental health distress since the COVID-19 outbreak would not be associated with stigma.
This is not to say, however, that we should not be concerned about stigma. The issue of mental health stigma is not a new one in Israel (Elroy et al. 2017; Struch et al. 2008) and mental health stigma also exists in other countries in the region (Abi Doumit et al. 2019; Gearing et al. 2015). This study may have implications for these other countries too. Even after the reduction in stigma, an important proportion of respondents in our sample still expressed some degree of stigma. And while it is not yet known if and to what degree the trend has continued, it seems likely there is still much stigma toward those with mental health issues. Indeed, an Israeli government poll taken the year after the study found continued high levels of stigma (Jeffay 2022). Stigma has potentially deleterious consequences in causing stress and discouraging those with mental health issues from seeking appropriate care and thus negatively impacting their mental health (Jeffay 2022; Shidhaye and Kermode 2013; Sickel et al. 2019).
It is also noteworthy that the results varied somewhat when specific illnesses were mentioned. It is not surprising that respondents indicated greater stigma when the illness is schizophrenia rather than depression as it is a more severe illness. However, it is interesting that most respondents had depression in mind when they responded to the stigma questions, evidence against those who may claim that stigma is primarily prevalent just for more severe diseases. Questions like the ones we developed for this survey that reference specific diseases should be considered for inclusion in future studies, when possible, not just those about stigma in general as is typically done when the CAMI scale is used.
People with severe mental illness (SMI) may have especially been affected by COVID-19 for several reasons, including stigma (Kassam et al. 2023). Those with SMIs need to be especially targeted by initiatives and to the extent that initiatives are directed to the less stigmatized groups, the problems of those with SMI could be exacerbated. This issue needs to be studied more, especially in Israel.
Our multivariate analyses also found that ethnic sector and religiosity were the demographic factors most strongly associated with greater stigma, with being Arab and being more religious associated with greater stigma. This is not necessarily surprising based on prior research (Al-Krenawi 2002; Fahoum and Al-Krenawi 2021; Greenberg and Witztum 2013; Lavie 2022). More traditional societies such as Arabs and those most religious may view mental health differently and arranged dating/marriages (called “shiduchim” in Hebrew) are more common in these groups, as marriage prospect was the stigma type most prevalent among respondents.
Limitations and Future Research
The study is cross-sectional and self-report, with attendant limitations. For example, to the extent that there is any recall bias about earlier events or changes in level of mental health distress, results could be affected. This study surveyed different people in each month of the study period rather than being longitudinal. While the month number was controlled for in analyses, to the extent that those refusing to participate had different characteristics than those who agreed to respond in different months, that would result in bias that could affect generalizability of results. If there were unmeasured variables potentially related to stigma that may have varied between the samples interviewed in different months or during and between lockdown periods, it could have also affected results related to measurement of changes in stigma between months and by lockdown periods.
Due to the sensitivity of the topic of mental health, there may have been social response bias that affected the veracity of answers. Therefore, the extent of stigma found may be higher than what was reported, although the survey answers were anonymous, to try to keep such bias to a minimum. Additional research, possibly on a qualitative basis, is recommended to probe what neutrality represents and to what degree neutrality may indicate public stigma. A larger sample size would facilitate detecting differences between those neutral and those who agreed or disagreed.
The data collection ended shortly before vaccination for COVID-19 started. It is unclear as to the impact that vaccination or other changes in COVID-19 regulations may have had on results and this warrants further research. Replication and evaluation of the study with later samples would therefore be useful. Reasons for the impact of COVID-19, especially lockdowns, on mental health need to be investigated further.
There were several topics which were beyond the scope of this study but could be useful topics for future research. Analyzing each component question of the CAMI on a multivariate basis may be of potential value in comparing different aspects of stigma. Analyses of the relationships of different aspects of mental health literacy as well as of stigma with demographic variables could help deepen understanding of the findings. Furthermore, the precise impact of stigma on use of healthcare services warrants further study.
Implications
There are several important implications to this study, for both the healthcare system and groups external to it, with potential lessons for reducing stigma and improving mental health even after the threat of COVID-19 has waned. Although there may potentially be greater awareness of mental health issues because of the stresses of COVID-19 that have affected much of society, policies to improve systems and organizations and reduce barriers and improve access to services are needed, especially for religious/racial/ethnic minority groups.
Consistent with other studies, findings generally suggest a need to increase knowledge about mental health issues and the mental healthcare system from a diverse body of information sources and different approaches which may in turn serve to reduce stigma (Abi Doumit et al. 2019; Shapiro et al. 2023). Differing solutions may be called for based on people’s distinctive cultural and contextual characteristics and a need for increased cultural competence in mental health promotion and treatment needed. For example, a community health worker model can be useful when there is a lack of manpower and access to the system, especially among minority groups (Islam et al. 2017).
Stigma reduction can also occur as a result of direct contact of those exhibiting public stigma with members of a stigmatized group. A review of the literature found that contact can often be even more effective than education programs, especially when the contact is in person rather than by video (Corrigan et al. 2012). This type of contact may be especially important in Israel where, as noted, there are divides among different societal sectors, which may be exacerbated by war.
There is a need to increase trust in and appropriate use of the healthcare system. A study examined the Ministry of Health’s success in increasing trust between it and the Haredi community regarding compliance with the guidelines regarding COVID-19 and receiving the vaccine (Schroeder, Numa, and Shapiro 2021). The study suggested that similar initiatives could succeed among other minority groups in Israel and in other health areas, including mental health.
There are also implications of the study related to the theoretical understanding of aspects of stigma. We think this study helps address Link and Phelan’s (2014) call for a more sociologically informed approach to stigma change. This study provides evidence supporting the claim that the societal phenomenon of the COVID-19 pandemic had a potentially positive impact in reducing public mental health stigma of individuals. One possible cause of the reduction may be related to exposure to persons with mental illness, especially those with whom one has a connection. Although we did not measure social networks and interactions directly, the study results are consistent with the growing attention by theoretical models to the importance of elements of our social environment on public mental health stigma, not just individual characteristics. These include social, not necessarily physical, interactions with people we know who may have mental health distress (Felix and Lynn 2022).
This study also adds nuance to the understanding of stigma by highlighting the importance of not only focusing on stigma in general but also of looking at its context. For example, the study found that there is greater stigma related to marrying someone with a mental health issue or to giving people with mental illnesses great responsibility, which has implications for the workplace. This is consistent with the literature about the study’s target populations of both Jews and Arabs (Ciftci, Jones, and Corrigan 2013; Greenberg and Witztum 2013).
Conclusion
Mental health has a very broad meaning, in the functioning of both the individual and the society. Mental health treatment options should be made available and familiar to everyone but the willingness of those in need to avail themselves of such services also needs to be increased. Importantly, there seems to be a positive trend of lower levels of public stigma since the COVID-19 outbreak. However, stigma still exists in Israel, a country with distinctive characteristics including social context that can be related to mental health utilization. Stigma reduction through increased mental health literacy and other means is needed to try to improve the appropriate use of mental health services and thus increase the mental health and wellness of the population and reduce health disparities.
Beyond the specific incidence of mental health problems and public stigma determined by our research, this study can shed light on broader issues. It shows how a crisis such as COVID-19, which began as a physical threat, can have multidimensional impacts on populations and cause society to reconsider how it views something as critical as mental health. This can have important and positive implications in the long term, with potential lessons learned for future crises.
Footnotes
Authors’ Note
Alean Al-Krenawi is also affiliated to Algoma University, Ontario, Canada
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Israel National Institute for Health Policy Research (Grant number 2018/237r).