
Abstract
Literature indicates that subjective social status (SSS) is a robust predictor of health outcomes net of objective social status (OSS). However, research that has considered gender in the relationship between SSS and health is limited. Using 2016–2018 data from the Wave V biomarker sample of the National Longitudinal Study of Adolescent to Adult Health, we investigate the relationship between SSS and two health outcomes—allostatic load and depressive symptoms—and the moderating role of gender in these relationships among a nationally representative sample of U.S. adults (ages 33–44 years) (n = 5,269). We find that SSS is inversely associated with both allostatic load and depressive symptoms, net of OSS. Moreover, we find that gender significantly moderates the SSS-allostatic load relationship but not the SSS-depressive symptoms relationship. Specifically, SSS has a greater impact on allostatic load among women than men. Future research should explore the underlying psychosocial mechanisms that contribute to these gender differences.
Introduction
Decades of research provide evidence for a robust and persistent relationship between objective social status (OSS) and health in the United States (Marmot et al. 1997; Phelan, Link, and Tehranifar 2010). A distinct gradient in health exists across the OSS hierarchy wherein higher income, educational attainment, wealth, and occupational prestige afford individuals favorable physical and mental health profiles and lower risk of mortality, and vice versa (Glymour, Avendano, and Kawachi 2014; Hayward, Hummer, and Sasson 2015).
More recently, a nascent body of literature has interrogated the relationship between subjective social status (SSS) and health, providing evidence that SSS is a powerful predictor of both physical and mental health outcomes, net of OSS (i.e., Cundiff and Matthews 2017; Demakakos et al. 2008; Freeman et al. 2016; O’Leary et al. 2021; Sakurai et al. 2010; Seeman et al. 2014; Subramanyam et al. 2012; Wolff et al. 2010). SSS measures an individual’s perceived position relative to others in a social hierarchy (Freeman et al. 2016; O’Leary et al. 2021; Subramanyam et al. 2012). It takes into account facets of OSS (i.e., educational attainment, occupational prestige, and income), but also captures multidimensional psychosocial aspects of social status not directly measured by OSS (Subramanyam et al. 2012). This includes cognitive comparative appraisals of power and control, access to privileges and resources, and opportunities for advancement, among others (Freeman et al. 2016; Langlois et al. 2020). Moreover, it is not simply a proxy measure for OSS as demonstrated by the fact that an individual’s belief of their SSS standing does not necessarily align with their position on the OSS hierarchy (Hoebel et al. 2017; McLeod 2014; Richards, Maharani, and Prag 2023).
Scholars have proposed that SSS has health consequences independent of OSS because the emotions associated with these comparative status evaluations influence psychological and physiological processes (Richards et al. 2023). For example, lower SSS may induce negative affectivity (McLeod 2014; Singh- et al. 2005) and/or stress-related physiological dysregulation (McLeod 2014; Seeman et al. 2014). Moreover, from a psychosocial standpoint, it has been theorized that the emotive reactions associated with perceived status may have greater psychosocial-related health impacts than objective measures of social rank themselves (Bartley 2004; Sakurai et al. 2010; Shaked et al. 2016; Weiss and Kunzmann 2020). This has also been empirically demonstrated in regard to self-rated health (Singh-Manoux et al. 2005) and psychological distress (Sakurai et al. 2010).
Despite the growing attention given to the role SSS plays in its unique effect on health, less scholarship has been devoted to investigating the differential SSS-health association across various sociodemographic groups. Gender is one important factor to consider for several reasons. First, disparities exist between men and women’s health, contingent on the health outcome in question. For example, while women have a greater average life expectancy than men, they also have higher rates of certain mental and physical morbidities such as depression and non-life-threatening chronic conditions (i.e., arthritis) (Denton, Prus, and Walters 2004; Read and Gorman 2010). This warrants the need to better understand the social factors that may differentially contribute to men and women’s health. Second, despite U.S. women surpassing men in college degree attainment (United States Census Bureau 2022), women still earn 83 cents to men’s dollar (Shrider et al. 2021) and are less likely to hold occupational positions of power (i.e., boss or manager) (Aragão 2023). This is a consequence of living in a highly gendered society in which gender is indivisible from social hierarchies, status beliefs, social roles, and performance expectations irrespective of OSS (Ridgeway 2001).
The limited research that has considered gender in the association between SSS and health in the United States thus far has been inconsistent in findings. For example, some research indicates the relationship between various physical health outcomes is stronger among men than women (Freeman et al. 2016), whereas other research suggests the opposite (McClain, Gallo, and Mattei 2022; Subramanyam et al. 2012), or finds no gender differences in regard to physical (Seeman et al. 2014) or mental (Subramanyam et al. 2012) health outcomes.
It is noteworthy that some of the inconsistencies in research findings could be attributable to variation in the age group considered among the aforementioned studies. Several of them focused on young adults (ages 24–32 years) only (Freeman et al. 2016; McClain et al. 2022), whereas others used data from samples of adults in young to old age (Seeman et al. 2014; Subramanyam et al. 2012). In our study, we narrow our focus to the early midlife (roughly 30s and 40s) period of the life course, which has been largely overlooked in extant scholarship. We argue that this distinct life course stage is particularly important to consider when studying the SSS-health association for two main reasons. First, OSS hierarchies are largely settled through completed education and established long-term employment or careers (Arnett 2012) leading to stark gender OSS disparities (i.e., earnings) (Dowell 2022). Second, the years from 30 to 45 are often considered the most intense and demanding out of the adult life course because adults in this age range are generally juggling taking on greater responsibilities and moving up in organizational hierarchies while starting and maintaining families (Mehta et al. 2020). This can especially disadvantage women’s ability to climb the social status ladder because women are still expected to be the primary family caretakers, diminishing their ability to advance in their careers and earnings potential (Mehta et al. 2020). As such, these gendered status differentials have implications for the role gender may play in the SSS-health relationship.
Using 2016–2018 data from the Wave V biomarker sample of the National Longitudinal Study of Adolescent to Adult Health (Add Health), our study extends the scholarship on SSS and health by considering the role of gender in the association between SSS and indicators of physical and mental health—allostatic load and depressive symptoms—among a nationally representative sample of U.S. adults aged 33–44 years. We consider these two health outcomes because each is heavily influenced by psychosocial factors, including perceived position in social hierarchies or SSS (Demakakos et al. 2008; Diaz, Guendelman, and Kuppermann 2014; Guardino and Schetter 2022; Hoebel et al. 2017; Seeman et al. 2014). Our research findings (1) provide further evidence of the role that SSS plays in explaining variation in physical and mental health, and (2) help to clarify whether these relationships are contingent on gender during early midlife, a life course period the SSS and health literature has largely overlooked.
Background
The Association between SSS and Health
The long-standing observed pattern of a robust relationship between OSS and health has led social scientists to theorize as to why SSS may be a salient predictor of health above and beyond OSS. Social-psychological explanations for the link between SSS and health are often conceptualized in social comparison and/or relative deprivation theories (Hoebel and Lampert 2020; McLeod 2014). The seminal social comparison theory (Festinger 1954) broadly argues that individuals evaluate their abilities by comparing them with similar others due to a fundamental “drive” for self-validation (Goethals and Darley 1987). Grounded in the notion of social comparisons, the core tenet of relative deprivation theory underscores that through comparisons to others, individuals perceive either themselves or their ingroup to be at a relative and unfair disadvantage (Smith et al. 2012). In other words, juxtaposing absolute deprivation, or the lack of tangible resources needed for the standard of living, relative deprivation embodies perceived lack of access to education, wealth, and social prestige relative to others an individual compares themselves with (Hoebel and Lampert 2020).
While divergent in ways, these theories converge in their emphasis on individual-level social comparison processes that are linked to emotional responses. Notably, perceiving oneself as being of lower social standing compared with others can generate feelings of subordination, inferiority, shame, resentment, inadequacy, and frustration, which in turn manifest in adverse psychological and physiological outcomes (Bartley 2004; Richards et al. 2023). Explicitly, these negative comparative evaluations and ensuing feelings activate stress responses (i.e., Bartley 2004; O’Leary et al. 2021; Seeman et al. 2014). Protracted stress has consequences for mental health through maladaptive psychological (i.e., depressive symptoms) and behavioral responses and downstream effects on physical health through “wear and tear” on bodily systems (Goosby, Cheadle, and Mitchell 2018).
Conversely, perceiving oneself as high status relative to others can increase perception of control or mastery (Mayor 2015)—the extent to which an individual believes they have the ability to control their life circumstances and/or environment (Pearlin and Schooler 1978)—which is associated with better mental and physical health (i.e., Infurna and Mayer 2015; Pudrovska et al. 2005). Specifically, control or mastery is a psychosocial resource that aids individuals in persevering in the face of challenges, actively anticipating and avoiding problems, and seeking social support—all of which buffers against stress and benefits health (Louie 2020).
As detailed, the psychosocial ramifications of social status comparisons have substantial inferences for variations in both mental and physical health across the SSS hierarchy. Motivated by this, the first aim of our study is to consider the relationships between SSS and indicators of physical (allostatic load) and mental (depressive symptoms) health among early midlife adults.
Allostatic load, first introduced by Bruce S. McEwen and Eliot Stellar (1993), is an established measure of the cumulative burden of exposure to chronic stress on the dysregulation of multiple physiological systems (i.e., metabolic and cardiovascular) (Goosby et al. 2018; Guidi et al. 2021), including exposure to psychosocial stress (Miller et al. 2021). Although the relationship between SSS and allostatic load has only been considered in a few studies, an inverse association net of OSS has been observed among a sample of U.S. women one-year after birth (Guardino and Schetter 2022), a nationally representative sample of older English adults (Richards et al. 2023), and a nationally representative sample of U.S. adults within a wide range of ages (34–84 years) (Seeman et al. 2014).
Furthermore, extant research on the relationship between SSS and depressive symptoms has provided strong evidence for an inverse association, independent of OSS, among various populations globally (Demakakos et al. 2008; Diaz et al. 2014; Ekl and Gallati 2024; Hoebel et al. 2017; Kwong et al. 2020; Mutyambizi et al. 2019; Zvolensky et al. 2015). This includes one recent study using data from a nationally representative sample of U.S. adults (Ekl and Gallati 2024).
Given the theoretical grounding for the psychosocial implications associated with social status comparisons and existing research findings, we expect to find the following:
The Role of Gender in the SSS-health Relationship
As previously noted, prior research has considered the role of gender in the relationship between SSS and various physical and mental health outcomes, but findings have varied. For example, evidence indicates the relationship between SSS and C-reactive protein (CRP; a marker of inflammation) is stronger among men than among women (Freeman et al. 2016), whereas other research suggests the relationships between SSS and cardiometabolic risk markers (waist circumference, body mass index [BMI], and high-density lipoprotein [HDL]) (McClain et al. 2022) and SSS and insulin resistance (a metabolic risk factor) (Subramanyam et al. 2012) is stronger among women than among men. Furthermore, a couple of studies have found no gender differences in the relationships between SSS and allostatic load (Seeman et al. 2014) or depressive symptoms (Subramanyam et al. 2012).
Motivated by this, the second aim of our study is to consider the moderating role of gender in the association between SSS and health in the context of early midlife, a life course stage in which gender differences in this association may be particularly pronounced. Specifically, early midlife is a unique life course stage typified by what Jeffrey J. Arnett (2012) describes as “role immersion.” Relative to the 20s, adults within the age range of 30–45 years have primarily completed their education, are working in long-term or permanent jobs with increasing demands and requirements, including moving up the occupational ladder, and/or parenting and maintaining households (Arnett 2012). Given the high demands in work and family domains, these years are often described as the most intense and arduous out of the entire adult life course (Mehta et al. 2020). However, gender inequalities preside in the division of labor in the household and the ability to climb the social status ladder. Despite gender roles becoming less distinct in the last several decades, women still spend more time caring for children and/or doing housework, even when they earn more money than their male partners (Mehta et al. 2020). Moreover, women often experience a “motherhood wage penalty” in which women with children make less money than their female peers without children, whereas male parents do not experience such a penalty (Mehta et al. 2020). This is in large part a consequence of interrupted employment (i.e., taking leaves or reducing hours to care for children) which diminishes women’s wages and ability to advance in their careers (England et al. 2016).
Of course, we are aware that not all early midlife adults are partnered, in heterosexual partnerships, and/or parents. Regardless of their partnership or parenthood status, however, women still face disadvantages relative to men in their ability to obtain a higher social status. As an institutionalized system, gender embodies status beliefs, or evaluative rankings of individuals socialized as men and women (Ridgeway 2001). Explicitly, belief systems of intrinsic social and biological differences between men and women (Ellemers 2018; Glick and Fiske 1996), as well as the binary categorization of gender (Ellemers 2018), lend to persistent gender stereotypes that women are more communion oriented than men (i.e., warm, sociable, caring, and interdependent), whereas men are more agentic (i.e., competent, assertive, independent, and achievement oriented) (Ellemers 2018; Jost and Kay 2005). These stereotypes have ramifications for gender divisions in occupational positions of power (Ellemers 2018) and the ability to acquire power and authority in other domains (Ridgeway 2001), conferring advantages for men and disadvantaging women. For example, women with similar skill levels and qualifications as their male peers are less likely to be perceived as competent, chosen for promotions and prestigious positions, and receive favorable job performance evaluations—all of which diminishes women’s income levels and career advancement relative to men (Ellemers 2018).
We argue that these gender social status differentials have implications for the moderating role of gender in the relationship between SSS and health during early midlife. Aligned with Scott Schieman (2002), we consider this possibility within the “disadvantaged status” thesis which suggests that individuals from disadvantaged groups, including women, may procure greater beneficial returns from “social-structural” resources than individuals from more advantaged groups (Mirowsky, Ross, and Reynolds 2000). More explicitly, as Schieman (2002) contends, for historically disadvantaged groups that have experienced barriers to status acquisition and mobility in domains such as employment, gains in these domains may provide them enhanced “personal and social rewards.” These may comprise both physical and mental health-benefiting psychosocial resources such as perceived control and autonomy (Schieman 2002), which help ameliorate the effects of psychological and physiological stress, including reducing physiologic stress reactivity (Wiley et al. 2017).
Regarding gender, due to gender structural inequality, men generally hold greater power and control in most realms of life than women, subsequently affording them more psychosocial coping resources such as mastery or control and self-esteem than women (Denton et al. 2004; Elliott 2013). Thus, because of their general status disadvantage relative to men, perceived status comparisons, particularly status advantage, may provide women greater positive psychosocial returns (Schieman 2002); this could in turn amplify the beneficial health effects from higher SSS more so for women than for men. In support of this argument, Schieman (2002) found that the positive effect of job autonomy on both global health and depressive symptoms was greater for women than for men, and these findings were explained by mastery and self-esteem.
Data and Methods
Data
Data for our study were drawn from the National Longitudinal Study of Adolescent to Adult Health (Add Health), a longitudinal study of adolescents in 7th–12th grade in 1994–1995. To date, five waves of data have been collected between 1994–1995 and 2016–2018. The first wave of data (Wave I) included an original sample of 90,118 students from 145 middle, junior, and high schools, and 20,745 of these students were selected to complete the 1994–1995 in-home interview. A parent or guardian of the Wave I in-home survey participants also completed a survey. Subsequent waves of data were collected from the original Wave I sample of the in-home survey participants in 1996 (Wave II), 2001–2002 (Wave III), and 2008 (Wave IV). 1 The most recent wave of data (Wave V) was collected between 2016 and 2018 when respondents were early midlife adults aged 33–44 years and included 12,300 individuals from the Wave I cohort. In addition, biomarker data were collected from 5,381 respondents in the Wave V sample. The biomarker data collected include anthropometric, cardiovascular, glucose homeostasis, lipid, renal function, and inflammation and immune function measures, as well as medication use information.
Given our target population is early midlife adults, we use data from Wave V, as well as data from the Wave I parent/guardian survey. We restrict our sample to respondents in the Wave V biomarker subsample (n = 5,381) to construct our allostatic load measure. 2 We use the Wave V biomarker survey weights to account for Add Health’s complex survey design (Chen and Harris 2020), and subsequently 112 respondents are excluded in our weighted analyses due to their missing information necessary for applying survey weights. To retain the largest number of participants and maximize statistical power, we use multiple imputation to address cases with missing values on any of our dependent and independent variables and therefore do not exclude those cases in our analyses. 3 Imputed values were randomly drawn from a posterior predictive distribution conditioned on the observed values and subsequently replaced any missing values (von Hippel 2020). Using the mi function in Stata version 18.0 (StataCorp, College Station, Texas), imputations were executed using “chained” equations (MICE) over 20 iterations. Thus, our final weighted analytic sample size is 5,269.
Measures
Outcomes
Our outcomes of interest are allostatic load (range 0–10) and depressive symptoms (range 0–15) at Wave V. We constructed our allostatic load measure following one of the most commonly employed measurements (Kezios et al. 2022). This allostatic load measure is a cumulative score based on values for 10 biomarkers of stress, use of biomarker-regulating medications, and self-reported diagnoses of a health condition related to the biomarkers (Richardson, Goodwin, and Hummer 2021). First, a point is assigned for a respondent having values of diastolic blood pressure (DBP), systolic blood pressure (SBP), pulse rate, BMI, waist circumference, hemoglobin A1c (HbA1c), triglyceride, total cholesterol, and/or CRP at or above the 75th percentile of all values in the Wave V biomarker sample. In addition, a point is assigned for a respondent having HDL cholesterol levels at or below the 25th percentile. Next, if a respondent was not assigned a point for being at or above/below any of the biomarker thresholds listed, they were assigned a point if they used a biomarker-regulating medication or self-reported being diagnosed with a condition related to the biomarker. Specifically, individuals who self-reported taking medication for hypertension, diabetes, hyperlipidemia, or inflammation were assigned a point for DBP and SBP; HbA1c; triglycerides, total cholesterol, and HDL cholesterol; and CRP, respectively. Finally, if an individual self-reported having been diagnosed with hypertension, diabetes, or hyperlipidemia, they were assigned a point for SBP and DBP; HbA1c; and triglycerides, total cholesterol, and HDL cholesterol, respectively. The total allostatic load score is a summation of the points assigned for biomarker levels, medication use, and self-reported diagnoses related to each biomarker and results in an allostatic load score for each individual within a range of 0–10. 4
We constructed our depressive symptoms measure based on a modified five-item Center for Epidemiological Studies (CES-D) instrument which asked respondents questions such as the following: about how often in the past week they could not shake the blues, felt depressed, or felt sad. We coded response options as 0 “never or rarely,” 1 “sometimes,” 2 “a lot of the time,” and 3 “most of the time or all of the time.” We summed the five questions for a depressive symptom score with a range of 0–15 (Cronbach’s alpha = .84). Other studies have provided support for the reliability and validity of the five-item subset of the CES-D (Bohannon, Maljanian, and Goethe 2003; Lewinsohn et al. 1997).
Primary predictor
Our primary predictor is Wave V SSS (range 1–10) as measured by the MacArthur Scale of Subjective Social Status (MacArthur SSS Scale). The MacArthur SSS Scale measures a person’s perceived rank or status relative to others in a group, community, or society by asking respondents to place themselves on a 10-rung “status” ladder (higher scores indicate higher social standing) (Cundiff et al. 2013). It is one of the most widely used measures in the SSS and health literature (Cundiff and Matthews 2017).
5
The question in the Wave V Add Health questionnaire asks respondents the following: Think of this ladder as representing where people stand in the United States. At the top of the ladder (Step 10) are the people who have the most money and education, and the most respected jobs. At the bottom of the ladder (Step 1) are the people who have the least money and education, and the least respected jobs or no job. Where would you place yourself on this ladder? Pick the number for the step that shows where you think you stand at this time in your life relative to other people in the United States.
Respondents select their perceived “rung” on the ladder which results in each individual having an SSS score between 1 and 10.
Modifier variable
For the second aim of our study, we examine gender as a moderator for the relationship between SSS and each health outcome. While we acknowledge gender is not a binary construct, the Wave V surveys did not have options to select a sex or gender identity outside of “male” or “female.” For this study, we thus code gender as 0 = male and 1 = female.
Control variables
We control for Wave V adjusted household income and educational attainment as our OSS indicators in accordance with other studies examining SSS and health (i.e., Diaz et al. 2014; Sakurai et al. 2010; Seeman et al. 2014; Subramanyam et al. 2012). Household income levels are reported in discrete categories ranging from $5,000 or less to $200,000 or more in Wave V, and, in accordance with Assini-Meytin et al. (2022), we calculated the midpoint of each category, adjusted for household size by dividing the midpoint by the square root of the respondents’ household size, and then transformed the adjusted income measure by using the natural log to reduce positive skew. We create a categorical measure of highest level of educational attainment which includes “less than high school” (reference), “high school degree or GED,”“some college,” and “bachelor’s degree or more.”
We exploit Add Health’s longitudinal design by additionally controlling for Wave I (adolescent) family OSS using information from the Wave I parent/guardian survey. Accordingly, we control for adolescent household income (continuous measure) and parent educational attainment (“less than high school” [reference], “high school degree or GED,”“some college,” and “bachelor’s degree or more”). These indicators of family socioeconomic background have long-lasting OSS attainment (Suglia et al. 2022) and health impacts into adulthood (Cohen et al. 2010).
We account for a variety of sociodemographic indicators including whether a respondent was employed (1 = yes), married (1 = yes), and/or had children living in the household (1 = yes) (i.e., Seeman et al. 2014; Shaked et al. 2016; Wolff et al. 2010; Zvolensky et al. 2015), and behavioral health indicators including whether a respondent was a current smoker (1 = yes) and/or a current alcohol drinker (1 = yes) (i.e., Kwong et al. 2020; Richardson et al. 2021). Finally, we control for demographic indicators including race/ethnicity, “Non-Hispanic, White” (reference), “Hispanic,”“Non-Hispanic, Black,”“Non-Hispanic, Asian/Pacific Islander,” and “Non-Hispanic, Other,”age (range 33–44 years), and whether a respondent was foreign-born (1 = yes).
Analytic Strategy
We ran a series of negative binomial regression models to estimate the associations between SSS and two health indicators—allostatic load and depressive symptoms. We use negative binomial regression models to account for overdispersion in each of the outcome variables. 6 We first estimated bivariate models to determine whether a preliminary association exists between SSS and each of our outcomes (Model 1). We then added all control variables to the models (Model 2), including OSS, which provides evidence of whether SSS is associated with our outcomes net of covariates, with particular interest in whether SSS is associated with physical and mental health independent of OSS. Next, we included an interaction term between gender and SSS in each of our fully adjusted models (Model 3).
In alignment with current methodological recommendations that suggest that the coefficients from interaction terms in nonlinear models should not be used to draw conclusions about the significance of the interaction (Mize 2019; Mustillo, Lizardo, and McVeigh 2018), for each outcome, from Model 3, we estimated the average marginal effects (AMEs) of SSS on the outcome by gender and then the difference between these AMEs (test of interaction) (Mize 2019) to determine if gender moderates each of the associations. Finally, to examine potential gender differences across the SSS ladder, we estimated the predicted margins (counts) of each outcome for men and women at every level of the SSS ladder (also estimated from Model 3), as well as the gender AMEs, and plotted these predicted margins for graphical interpretation. We used Stata version 18.0 (StataCorp) for all of our analyses.
Results
Descriptive Statistics
Table 1 provides weighted descriptive statistics for our overall sample and for men and women separately, as well as tests for significant differences in the proportions and means between men and women. As shown, the mean allostatic load score for men (3.8) is significantly higher than for women (3.2), but the mean number of depressive symptoms is slightly higher for women (2.5) than for men (2.4), although this difference is not significant. The mean rating on the SSS ladder is not significantly different between men (5.5) and women (5.4). A significantly larger proportion of women have a highest educational attainment level of a bachelor’s degree or more (44.3 percent) than men (38.1 percent), but the adjusted household income (natural log transformed) is significantly higher for men (10.5) than for women (10.4). A significantly larger proportion of men (85.5 percent) than women (77.1 percent) are employed. While there is not a significant difference in the proportion married between men and women (55.7 vs 57.3 percent), a significantly larger proportion of women (74.1 percent) have children than men (61 percent). In terms of demographic indicators, the majority of both men and women are non-Hispanic, White, approximately 38 years of age on average, and born in the United States. 7
Weighted Descriptive Statistics for Total Sample and by Gender.
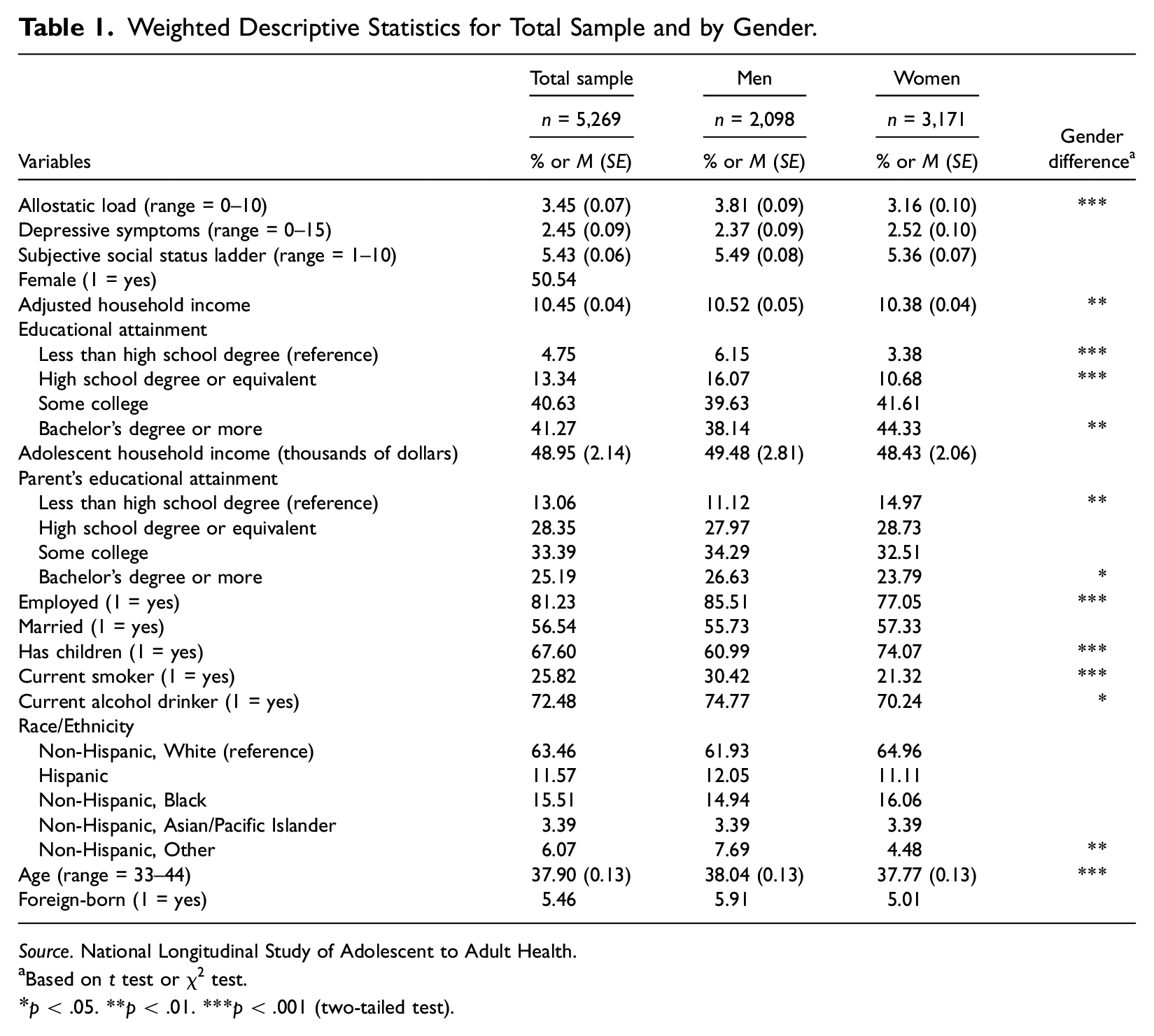
Source. National Longitudinal Study of Adolescent to Adult Health.
Based on t test or χ2 test.
p < .05. **p < .01. ***p < .001 (two-tailed test).
Multivariate Regression Results for Allostatic Load
Table 2 displays the results from a series of negative binomial regression models of the association between SSS and allostatic load presented in incident rate ratios (IRRs). As shown in Model 1, there is a statistically significant negative association between SSS and allostatic load in the bivariate model (IRR = 0.93, 95% confidence interval [CI]: 0.92, 0.95). When fully accounting for control variables in Model 2, the association between SSS and allostatic load remains significant. Specifically, for each unit increase in SSS, the rate for allostatic load decreases, on average, by a factor of 0.97 or 3 percent.
Weighted Estimates (IRRs) from Negative Binomial Models Predicting Allostatic Load (n = 5,269).
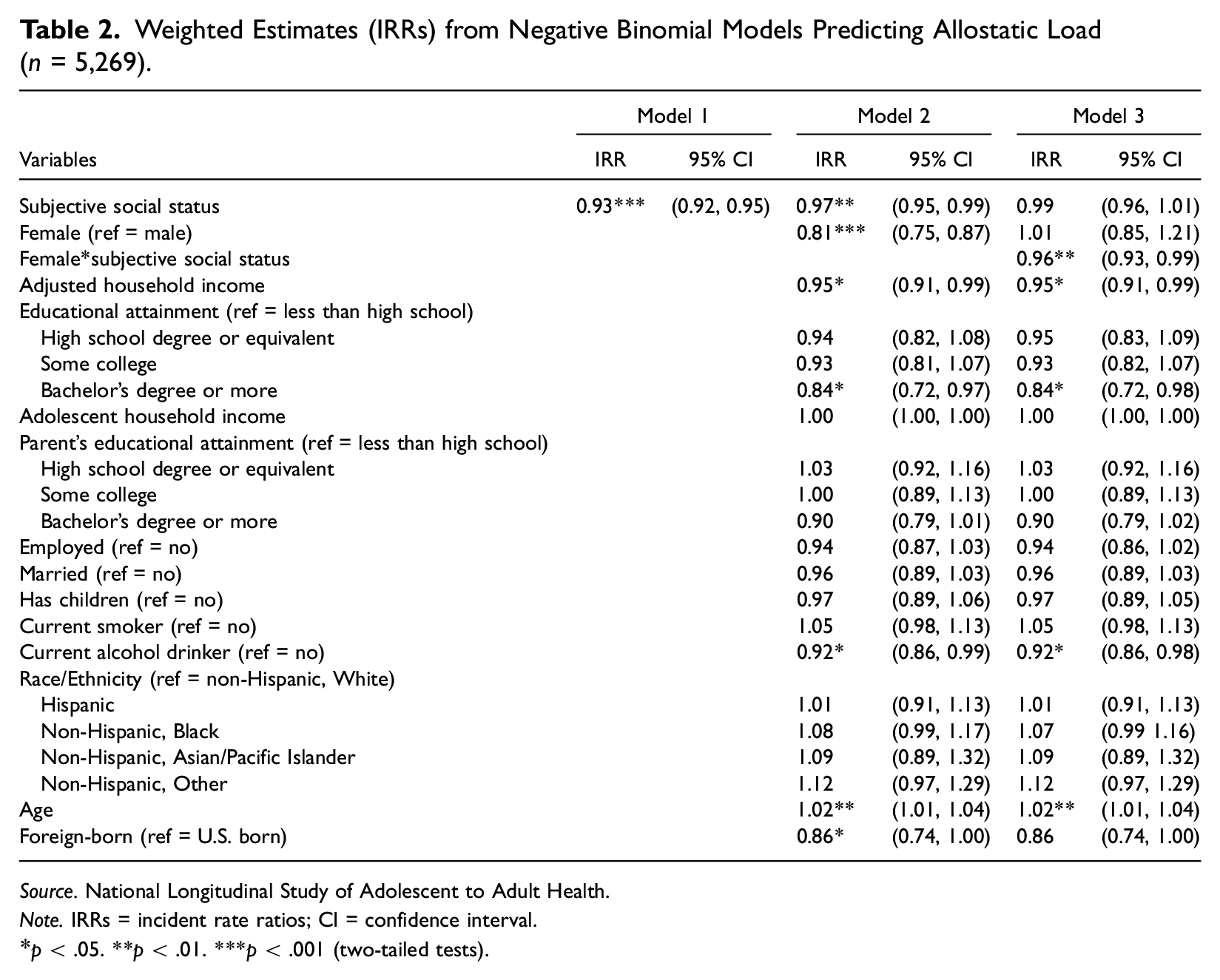
Source. National Longitudinal Study of Adolescent to Adult Health.
Note. IRRs = incident rate ratios; CI = confidence interval.
p < .05. **p < .01. ***p < .001 (two-tailed tests).
Table 3 shows the AMEs of SSS on the predicted count of allostatic load by gender, as well as the difference in these AMEs. As shown, the AME of SSS (−0.05) for men is not statistically significant, whereas the AME of SSS (−0.17) for women is (p < .001). The difference in the AMEs between men and women is 0.12 and significant at the p < .05 level. In other words, each unit increase in SSS is associated with an average decrease in the predicted count of allostatic load that is 0.12 points significantly greater among women than among men. Overall, these results suggest that gender moderates the SSS-allostatic load relationship, and specifically, SSS has a stronger negative association with allostatic load among women than among men.
AMEs of SSS on the Predicted Count of Allostatic Load by Gender (n = 5,269).
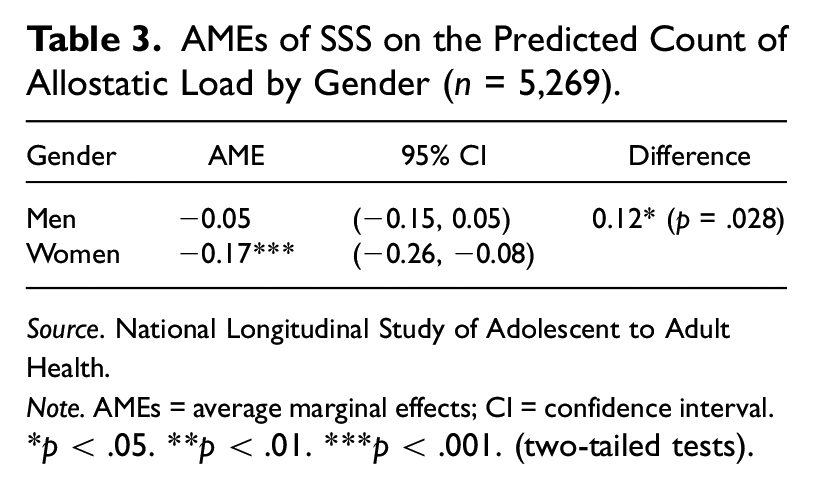
Source. National Longitudinal Study of Adolescent to Adult Health.
Note. AMEs = average marginal effects; CI = confidence interval.
p < .05. **p < .01. ***p < .001. (two-tailed tests).
Figure 1 displays the predicted allostatic load scores across the SSS ladder by gender. Corresponding to Figure 1, Table 4 shows the gender differences in the predicted allostatic load score (AMEs) at each rung of the ladder. There are several noteworthy takeaways. First, the differences (or AMEs) in allostatic load scores between men and women are negligible and not statistically significant among those who rate themselves as lower on the SSS ladder (Rungs 1–2) but become increasingly pronounced and statistically significant as ladder rankings increase (Rungs 3–10). For example, whereas the difference in the average allostatic load score between men and women at the lowest rung of the ladder (Rung 1) is 0.11 and not statistically significant, this difference increases to 1.21 at the highest rung of the ladder (Rung 10) and becomes statistically significant (p < .001). This suggests that all else equal, women who rate themselves as “10” on the SSS ladder have an average predicted allostatic load score that is 1.21 units lower than men who rate themselves as “10” on the SSS ladder. Moreover, all of the contrasts, or second differences, between the gender AMEs at each rung of the ladder are statistically significant at the p < .05 level (i.e., AME of Rung 1 is 1.10 units significantly lower than AME of Rung 10) (detailed contrast results available upon request).
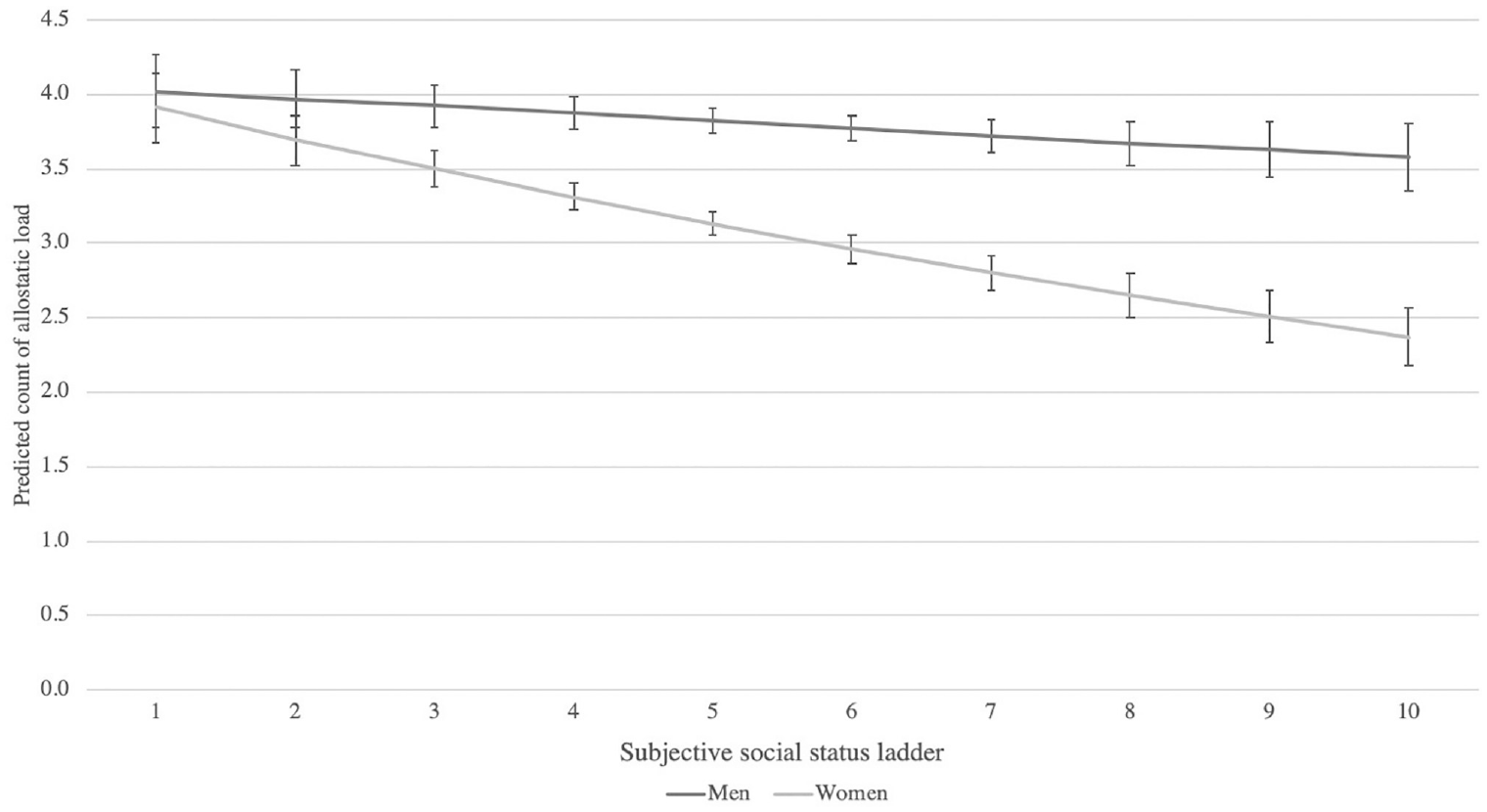
Predicted count of allostatic load (SE) across the SSS ladder by gender (n = 5,269).
AMEs of the Predicted Count of Allostatic Load between Men and Women across the SSS Ladder (n = 5,269).
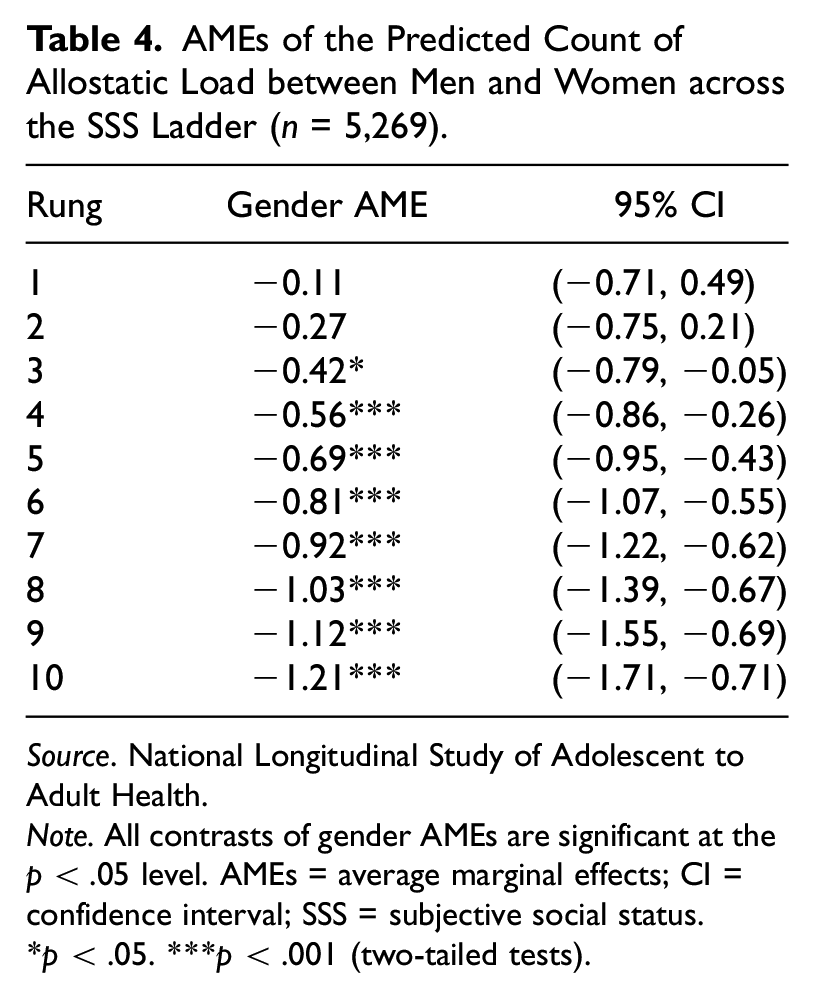
Source. National Longitudinal Study of Adolescent to Adult Health.
Note. All contrasts of gender AMEs are significant at the p < .05 level. AMEs = average marginal effects; CI = confidence interval; SSS = subjective social status.
p < .05. ***p < .001 (two-tailed tests).
Second, whereas the average allostatic load score marginally decreases among men across the SSS ladder (and there are no statistically significant differences in allostatic load scores between any of the rungs of the ladder), the average allostatic load score decreases appreciably and significantly among women across the SSS ladder. For example, the average allostatic load score difference between women who rank themselves as 1 on the SSS ladder and women who rank themselves as 10 is 1.54 (p < .001). Overall, these results further demonstrate that SSS has a larger impact on allostatic load for women than for men, and, specifically, higher SSS is more beneficial for physical health for women than for men.
Multivariate Regression Results for Depressive Symptoms
Table 5 displays results from a series of negative binomial regression models of the relationship between SSS and depressive symptoms. Similar to allostatic load, results from Model 1 demonstrate a statistically significant negative association between SSS and depressive symptoms without accounting for control variables (IRR = 0.88, 95% CI: 0.86, 0.91). After fully adjusting for all controls (Model 2), this association remains significant. Specifically, for each unit increase in SSS, the rate of depressive symptoms decreases (on average) by a factor of 0.93 or 7 percent.
Weighted Estimates (IRRs) from Negative Binomial Models Predicting Depressive Symptoms (n = 5,269).
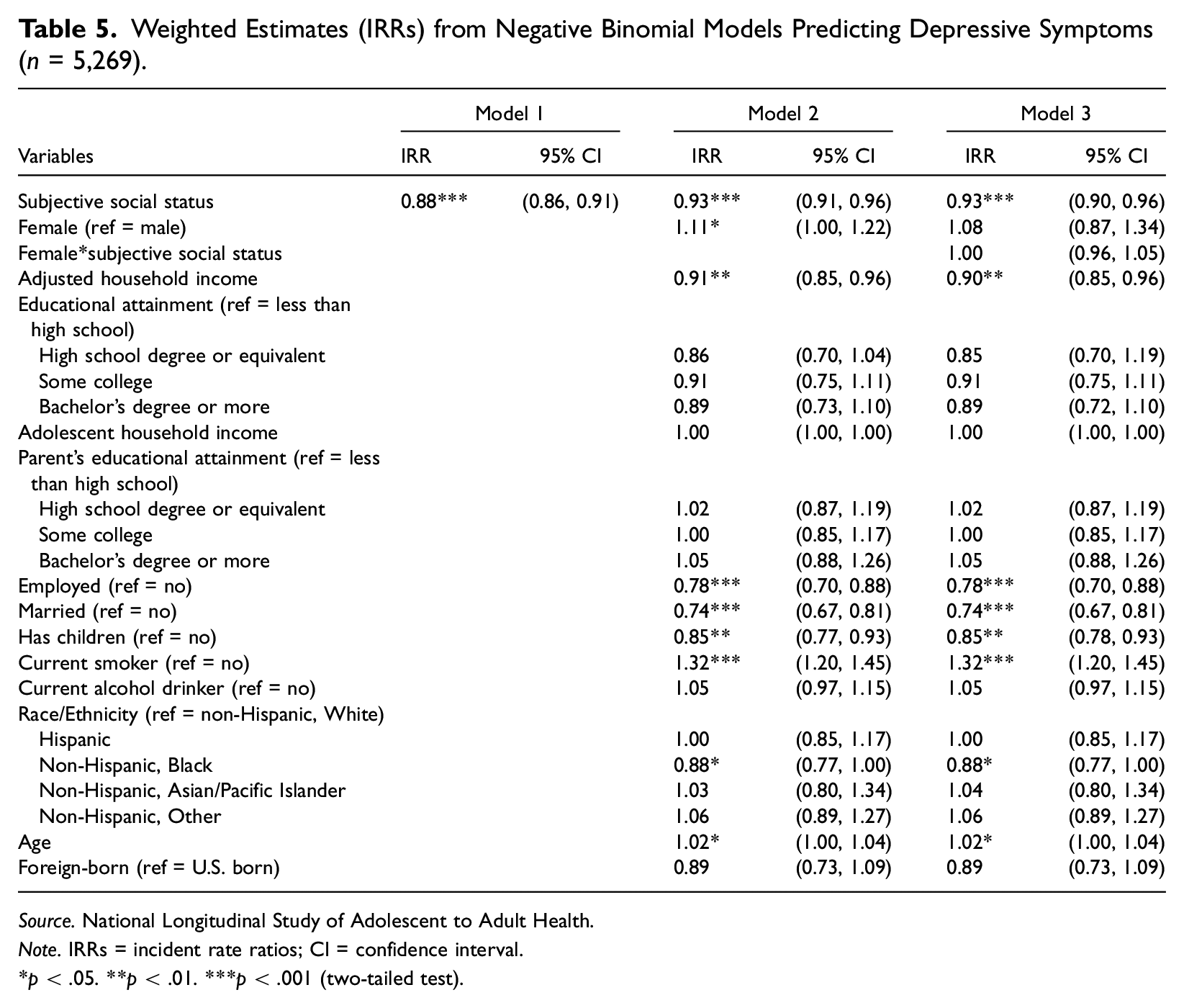
Source. National Longitudinal Study of Adolescent to Adult Health.
Note. IRRs = incident rate ratios; CI = confidence interval.
p < .05. **p < .01. ***p < .001 (two-tailed test).
Contrary to allostatic load, however, there are negligible differences in the AMEs of SSS on the predicted count of depressive symptoms by gender as shown in Table 6. Moreover, as depicted in Figure 2, across the SSS ladder, there are no significant differences in the average number of depressive symptoms between men and women. These results lead us to conclude that gender does not moderate the SSS-depressive symptoms association.
AMEs of SSS on the Predicted Count of Depressive Symptoms by Gender (n = 5,269).
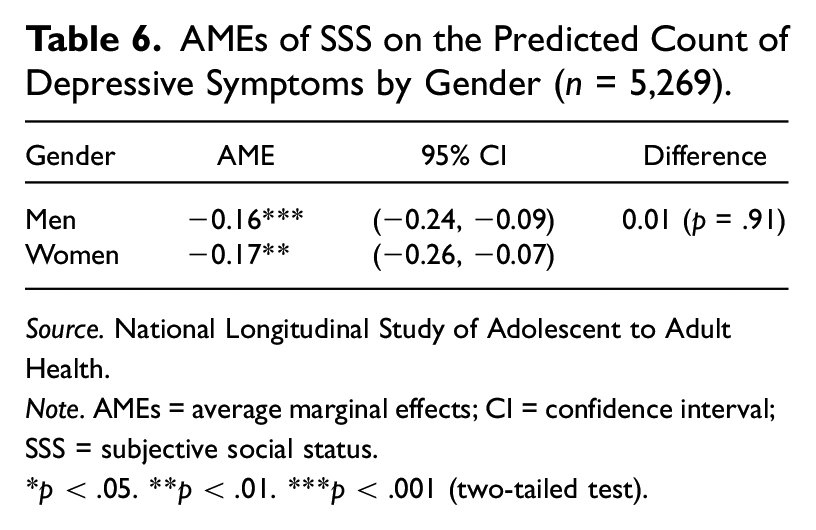
Source. National Longitudinal Study of Adolescent to Adult Health.
Note. AMEs = average marginal effects; CI = confidence interval; SSS = subjective social status.
p < .05. **p < .01. ***p < .001 (two-tailed test).
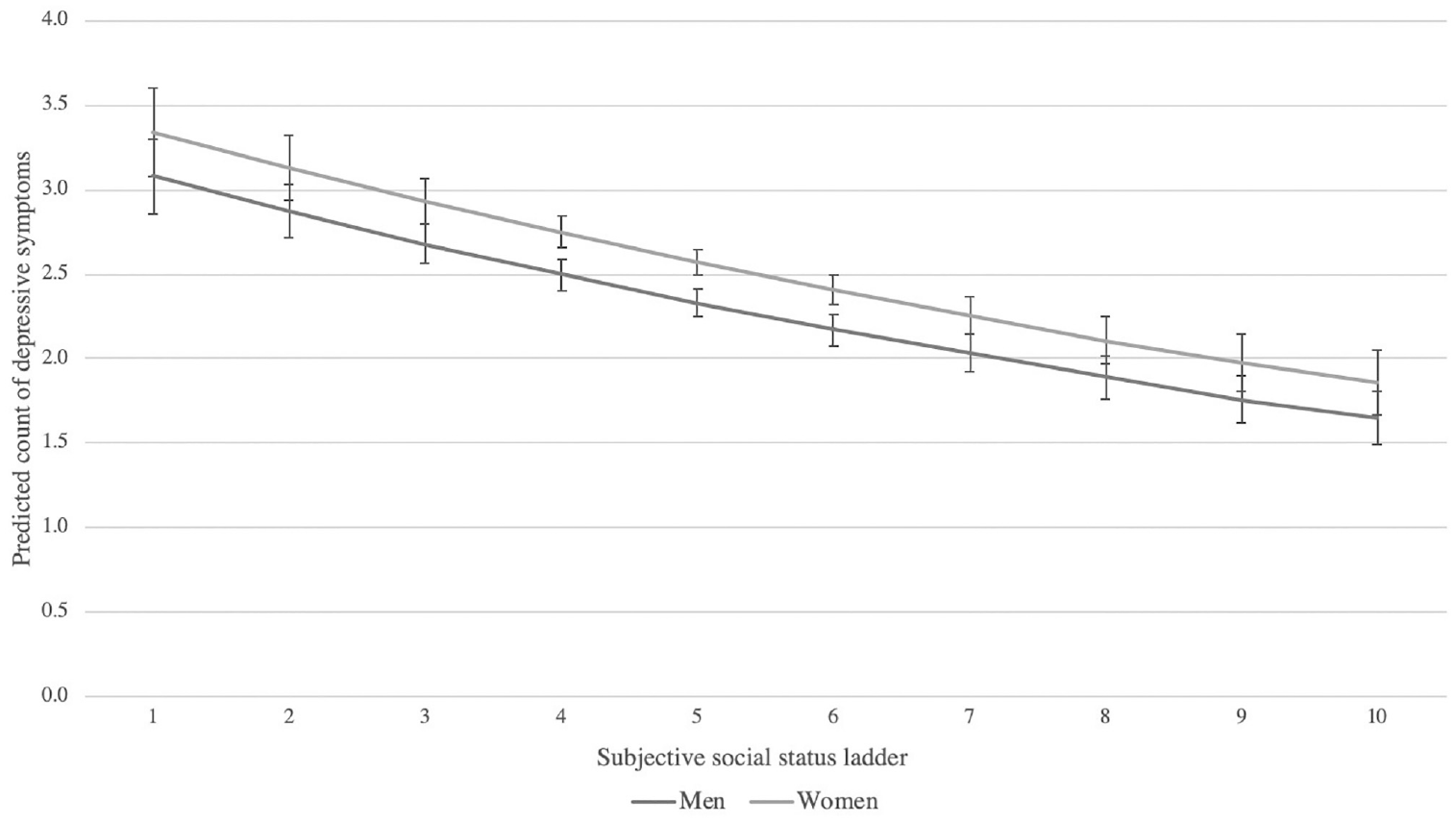
Predicted count of depressive symptoms (SE) across the SSS ladder by gender (n = 5,269).
Discussion
A burgeoning body of literature has examined the relationship between SSS and various mental and physical health indicators as motivated by the psychosocial implications of social comparison processes (Hoebel and Lampert 2020; McLeod 2014). However, differential SSS-health associations across different sociodemographic groups, particularly gender, have received less consideration. As such, the purpose of this study was to build upon the existing literature through investigation of the relationships between SSS and two health outcomes—allostatic load and depressive symptoms—as well as consider the moderating role of gender in these relationships, during early midlife, an important overlooked life course stage in the SSS-health literature.
Our analyses revealed several key findings. First, confirming our first two hypotheses and corroborating prior research findings, we found that SSS was significantly and inversely associated with both allostatic load and depressive symptoms, net of indicators of OSS. These findings provide further confirmation of the importance of considering an individual’s perceived social status location compared with others, in addition to their objective position, as it relates to both physical and mental health. From a psychosocial standpoint, they support the notion that the emotional processes linked to comparative evaluations likely play a robust role in determining variations in health independent of OSS (Bartley 2004; Richards et al. 2023). In other words, relative or comparative measures of social status inequalities unequivocally tap into psychosocial processes that objective measures do not (O’Leary et al. 2021).
Our second key finding was that gender moderated the relationship between SSS and allostatic load, confirming our third hypothesis. Notably, whereas we did not find significant differences in allostatic load between men and women at the lowest echelons of the SSS ladder, we found gender differences became significant and increasingly pronounced as perceived societal rank increased, favoring women.
Our gender findings regarding allostatic load provide support for the “disadvantaged status” thesis (Mirowsky et al. 2000; Schieman 2002), such that women, as a historically marginalized group, benefited more from the health-protective effects of higher perceived social status relative to their generally better-resourced male counterparts. As a reminder, this thesis suggests that due to gender structural inequality, men largely have more power and control in most domains of life than women, potentially affording women more positive psychosocial returns from perceived status advantages (Schieman 2002). These psychosocial returns could include greater perceived control and autonomy which may inadvertently reduce stress and promote better health (Mayor 2015).
This is an important contribution to the sociology of mental health scholarship because our study is the first, to our knowledge, to offer a theoretically informed analysis asking if and under what circumstances gender may matter for the SSS—health association. Our focus on adults in early midlife also advances the SSS—health research as we were able to show that women may benefit from higher perceived status in terms of lower physiological imprint during a stage in life when gender disparities in OSS are particularly pronounced (Dowell 2022), and work and family demands may be particularly intense (Mehta et al. 2020). While we are unable to test whether psychosocial resources such as mastery operate as mediators due to data limitations, it is our hope that scholars in the future will investigate this research question further by testing explicit pathways through which perceived social status may offer health benefits to socially marginalized groups.
Our finding that gender did not moderate the relationship between SSS and depressive symptoms is unexpected and warrants further examination as well. We can only speculate about the lack of significance for this conditional effect. First, it is possible that women “truly” derive greater stress-related physiological rather than psychological health benefits from higher SSS relative to men. For example, women and men may be similarly reactive to the stress associated with lower SSS, as supported by men and women’s equivalent allostatic load scores at the lowest levels of SSS but receive more physiological stress reduction returns to higher SSS than men. This could be due to other factors not captured in our analyses such as women’s diminished household and caretaking duties at higher levels of SSS due to the ability to outsource this labor (i.e., affording childcare).
Second, it is possible that our gender results are an artifact of the objective versus subjective nature of these two measures. Specifically, if the disadvantaged status thesis holds, women may derive greater mental health returns to higher SSS than men, but men’s underreporting of depressive symptoms could mask this effect. It has long been theorized and empirically supported that men often underreport depressive symptoms, otherwise known as the “response bias hypothesis,” because depressive symptoms are perceived as less masculine or “weak,” diminishing men’s willingness to report them (Sigmon et al. 2005). This may be especially salient among men who perceive themselves as high on the SSS ladder because denial of depression (or depressive symptoms) is used as a way for men to avoid assignment to a low-status position (Courtenay 2000). Moreover, the CES-D (among other traditional diagnostic tools for depression) may not be capturing symptoms that are typically associated with depression among men such as irritability, anger, substance abuse, and risk-taking (Cavanagh et al. 2017). Taken together, these factors indicate that future research could benefit from further exploring gender differences in the SSS-mental health relationship using alternative measures of depression and/or other mental health outcomes such as substance abuse.
There are limitations to our study that must be acknowledged. First, we use cross-sectional data, which means we cannot speak to causality. It is possible there is a bidirectional association in which physical and mental health influences one’s perception of societal rank. However, randomized and experimental studies have provided evidence that lower SSS is causally related to depressive symptoms (Hoebel and Lampert 2020) and biological markers help address issues of reverse causality (Goosby et al. 2018). While we cannot be certain there are not bidirectional associations, we have a foundation to believe our findings are not due to reverse causality. Second, given sample size and power limitations, we were unable to examine racial/ethnic or other demographic differences in conjunction with gender. It is certainly feasible there could be gender heterogeneity both between and within racial/ethnic or other demographic groups. Third, Add Health only has a societal and not community SSS measure. Evidence suggests that community and societal SSS have differential associations with OSS as well as impacts on health, and it is plausible that the moderating role of gender in the relationship between SSS and health may differ based on the referent group. For example, research has indicated that societal SSS is more closely related to OSS indicators, such as income and education, than community SSS (Cundiff et al. 2013; Diaz et al. 2014), and that community SSS is a more robust predictor of mental health, whereas societal SSS is a more robust predictor of physical health and health behaviors (Diaz et al. 2014; Ghaed and Gallo 2007; Wolff et al. 2010). Given the availability of data, future research could replicate our analyses with both community and societal SSS ladders to better understand if the referent group matters.
Limitations notwithstanding, our study provides a novel contribution to the literature on SSS and health by examining the moderating role of gender in the association between SSS and two psychosocial-related health outcomes among a nationally representative sample of early midlife adults. Our results provide further evidence that SSS has a significant impact on both allostatic load and depressive symptoms, net of OSS, and demonstrates that gender moderates the relationship between SSS and allostatic load. More explicitly, we found that higher perceived societal rank is more beneficial for women’s physical health than men’s. Given the literature on gender differences in the social determinants of health is far from straightforward, we encourage researchers to continue to untangle this puzzle to help promote greater gender health parity in a highly gendered society such as the United Status.
Supplemental Material
sj-docx-1-smh-10.1177_21568693231213094 – Supplemental material for Subjective Social Status as a Predictor of Physical and Mental Health among Early Midlife Adults in the United States: Appraising the Role of Gender
Supplemental material, sj-docx-1-smh-10.1177_21568693231213094 for Subjective Social Status as a Predictor of Physical and Mental Health among Early Midlife Adults in the United States: Appraising the Role of Gender by Carlyn Graham and Gabriele Ciciurkaite in Society and Mental Health
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors of the study acknowledge assistance provided by the Population Research Institute at Penn State University, which is supported by an infrastructure grant by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD; P2CHD041025). This study uses data from Add Health, which is directed by Robert A. Hummer and funded by the National Institute on Aging cooperative agreements U01 AG071448 (Hummer) and U01AG071450 (Aiello and Hummer) at the University of North Carolina at Chapel Hill. Waves I–V data are from the Add Health Program Project, grant P01 HD31921 (Harris) from the Eunice Kennedy Shriver NICHD, with cooperative funding from 23 other federal agencies and foundations. Add Health was designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.