
Abstract
Since Kai Erikson’s landmark study of the devastation of five communities in West Virginia, sociology has leveraged the concept of trauma to describe certain social phenomena. Collective trauma came to refer to the destruction of social infrastructure and the ensuing negative mental health outcomes, while cultural trauma has come to describe the imposition of historical and ongoing attacks by a dominant group on the culture (broadly defined) of a group of people sharing a collective identity. The following article sketches out a theory of social trauma designed to bring these two types of sociological trauma together, highlight their similarities and differences, and unite them by grounding them in the neuroscience of (social) pain. The term trauma, borrowed from medical and psychological study, implies pain, but the sociological version of trauma is best understood as the collectivization and enculturation of social pain, or the evolved negative affective response to separation, rejection, exclusion, and isolation from cherished social objects including statuses. The article concludes by modeling the process by which an event transforms individual social pain into collective social trauma as well as the pathways through which social trauma becomes enculturated in a collective identity. Implications for the sociology of mental health follow.
Ever since Kai Erikson’s (1976) landmark study on the Buffalo Creek coalmine flood and the devastation of five West Virginian small towns, the conceptual language of trauma has circulated in the sociological lexicon. Sociologists have engaged the concept in relationship to the negative physical and mental health outcomes stemming from human-made and environmental disasters (Erikson 1994; Tierney 2019), long-standing or recent onslaughts on the cultural reality of groups (Alexander et al. 2004; Subica and Link 2021), and as a primary and secondary source of stress (Aneshensel and Avison 2015; Pearlin 1999). Indeed, as environmental risks of disasters and crises grow alongside increasing intergroup conflicts along political, economic, racial, and other lines, trauma and its effects on human well-being will only increase.
Several lingering questions remain largely open. For instance, what are the differences and similarities between Erikson’s collective trauma and the constellation of studies on cultural trauma (Alexander et al. 2004; Eyerman and Sciortino 2019)? Can we draw clear distinctions between psychological and sociological trauma rarely made in practice (Wheaton et al. 2013)? In short, there is a pressing need for theorizing what makes social trauma unique from its psychological counterpart and, in turn, for making sense of the relationship(s) between collective and cultural trauma, two seemingly distinct types of social trauma.
Considering the fact that pain always undergirds trauma presents one possible way to begin this distinguishing process. Pain, in sociology, is often ignored (Bendelow and Williams 1995; Zajacova, Grol-Prokopczyk, and Zimmer 2021), or it is conceptualized as a mediating force—a stressor (Pearlin 1999; Thoits 2010). Yet, pain is at the heart of trauma. Erikson (1976) chose the term because it underscored an allusion: to him, the Buffalo Creek flood was akin to medical trauma, in that each represented an acute rift in connective tissue (the former of the body social, the latter to the body physical). The term also made sense with regard to posttraumatic stress disorder, here extended to the lingering symptoms of collective trauma endured across a swath of West Virginia for years following the flood. Erikson theorized that as the flood exacted individual, psychological, and medical trauma on the people, there also arose a collective trauma in which “a blow to the basic tissues of social life that damages bonds [leads to] a general realization that the community no longer exists as an effective source of support and an important part of the self has disappeared” (p. 154). Collective trauma, for Erikson, is distinct from other types of trauma because it wipes away the very thing “that cushions pain, provides the context for intimacy, represents morality and serves as a repository of old traditions” (p.193–4): the community, or more specifically, communality. Cultural trauma scholars, who instead treat sociological trauma as metaphorical and not, in fact, ontologically real, also evoke the imagery of pain and victimization (e.g., Alexander et al. 2004:13ff.; also Brown 2016). The difference between collective and cultural trauma for sociologists is then whether the trauma is conceptualized as “real” and whether it is a real community or a class of people (e.g., Black or Indigenous Americans) who experience it (allowing that some cases crosscut both types of trauma (Brave Heart et al. 2011)).
Returning to the idea that pain underpins both types of trauma suggests the promise and potential for constructing a theory of social trauma that adds clarity, precision, and ontological distinction to the sociological study of trauma and of pain. A theory such as this has clear implications for bringing a set of social scientific subfields into closer dialogue, promising to supplement them with theoretical and methodological innovations. The study of disasters invariably overlaps with a theory of social trauma (Arcaya, Raker, and Waters 2020), as do various strands of the sociology of mental health, including stigma theory (Link and Phelan 2013), stress processes and negative mental health outcomes (Aneshensel and Avison 2015; Pearlin 1999), and, more broadly, the social determinants of mental and physical health (DeAngelis 2020; 2021).
To that end, this article posits a theory of social trauma in three steps. First, I detail both types of trauma, drawing out their linkages and highlighting the central structural difference between them: Collective trauma emerges and persists within collectives of all sized via recurring interaction that makes use of shared social infrastructure, while cultural trauma is rooted in a collective identity shared by those belonging to a category or class of people, who do not necessarily interact or live with each other. Second, I close the ontological gap predicated on this structural difference by asking whether trauma is real and answering in the affirmative by drawing on the science of social pain. Physical pain is an evolved, affective alarm signal designed to keep the organism alive by protecting against noxious stimuli in the present and by avoiding them in the future. Social pain is a human, and perhaps primate, adaptation in which separation, rejection, exclusion, and isolation trigger the same affective neural circuits as physical pain (Eisenberger 2015; Rotge et al. 2015), thereby motivating humans to defend their cherished social relationships, repair those under threat, and seek new social objects when significant ones are lost. Although social pain is ubiquitous, it varies in important ways based on structural and cultural factors unevenly distributed in a community or society. It follows that the two types of trauma are two different conceptual processes by which social pain is collectivized into social trauma. Third, I lay out the process of social trauma, highlighting the basic mechanisms increasing the likelihood of social trauma as well as its expected duration.
In so doing, this article contributes to sociological inquiry in several important ways. First, as noted, it integrates two seemingly distinct literatures and processes (collective/cultural traumas). Second, it extends a promising interest in social pain and its direct link to negative physiological and mental health outcomes (DeAngelis 2021; DeAngelis, Hargrove, and Hummer 2022; Gunn 2017; Inagaki et al. 2018), in addition to some research that shows both types of trauma (and the attendant pain) may be a fundamental cause of health disparities (Subica and Link 2021). Third, it supplements myriad sociological traditions, most notably stress process theory (Pearlin 1999). In part, it abstracts both the idea of pain and trauma from the stress process, allowing for an isolation of the mechanisms, direct effects, and unique dynamics of each vis-à-vis human health and well-being. Finally, by bridging the biopsychological process of social pain with a sociological process (social trauma), suggestive links between other sociological concepts that draw allusions to pain (without the biopsycho science undergirding pain) can be discerned—for example, stigma (Link and Phelan 2013) or anomie (Durkheim [1897] 1951:246–48, 258, 284ff.).
A Tale of Two Traumas?
Collective Trauma
On February 26, 1972, in Logan County West Virginia, a coal slurry impoundment dam burst, unleashing 132 million gallons of coal wastewater. Peaking at 30 ft, the flood devastated 15 coal towns and 5,000 people nestled in the hollow below. One hundred twenty-five people died; 1,121 were injured; and more than 4,000 lost their homes. People watched in horror as the flood demolished bridges, community symbols like schools, and, of course, the personal possessions that were extensions of self; death was visible amidst the chaos. Erikson (1976) spent approximately three years off and on at the fieldsite. Initially, he observed classic “disaster syndrome” symptoms (Wallace 2003): numbness, apathy, a state of dazedness, the sense of death closing in, survivor’s guilt, grief and panic over lost things, and the loss of confidence in social and moral order. But, over time, as the communities endured a state of suspended animation, awash in the litigation process and the clean-up, Erikson’s (1976) respondents began showing symptoms of something very different; the resolution of disaster syndrome—“the sudden and logically inexplicable wave of good feeling that comes over survivors shortly after disaster”—never came (p. 200). In its place, Erikson detailed another type of shared phenomenon, too ubiquitous for psychological categorization, that he labeled collective trauma, denoting “traumatized communities as something distinct from assemblies of traumatized persons” (Erikson 1994:230). For my purposes, collective trauma refers to the sudden, acute destruction of social infrastructure. This destruction separates individual members from the social objects that connect their personal identity to the collective identity. This is crucial, because, as sociology teaches us, it is the connective tissue of social relationships that provides the practical and the moral wellsprings of mental, physical, emotional, and social well-being. We become as attached to real others as we do to things like possessions, landmarks, and other external representations charged with the emotional residue of mundane and spectacular rituals that have made and remade “community,” a sense of “belongingness,” and our social selves (McDonnell et al. 2017).
In Erikson’s estimation, the flood was the equivalent of a knife wound to the body, a medical trauma. The blow mattered, but so did the enduring reality of scattered communities, disintegrated social geography, and the incapacity to do community and self. People were separated from moral and social anchors, and the sense of social isolation accrued despite the clustering of survivors in government-provided trailer camps. The collective trauma was so vivid and palpable that even those fortunate to not be home during the flood “caught” their neighbors’ symptoms upon return. How could they not? The rituals of community life had been replaced with new rituals of a very different emotional tone and moral content. The tragedy became a new anchor, the overarching focal point drawing mutual focus and arousal. Rituals of life were replaced with piacular, or mourning, rituals (Durkheim [1912] 1995:389–414). No less efficacious in building social solidarity, these new rituals left members in a state of suspended shared trauma that quickly enveloped returning denizens.
Central to Erikson’s assertion is the idea that personal identities, particularly in smaller, tight-knit social units, are inextricably tied to the collective identity. In Durkheim’s ([1912] 1995) model, the “center” of the community—as externalized in symbols that pockmark the physical space and internalized as an “idioculture,” or a shared sense of history, destiny, and identity (Fine 1979)—draws mutual attention and arousal. The community’s center has a gravitational pull which allows members of a small group, neighborhood, or small town to feel meaningfully grounded and anchored. Erikson notes that just as the internal organs are protected by muscle, tissue, and fat, community members “are surrounded by layers of trust, radiating out in concentric circles like ripples in a pond” and disruptions “mean not only a loss of confidence in the self but a loss of confidence in the scaffolding of family and community, in the structures of human government, and in the larger logics by which humankind lives” (Erikson 1994:242).
For the most part, collective traumas have been synonymous with disasters which threaten physical and social landscapes (Erikson 1994): some human-made, like the Buffalo Creek flood caused by greedy mine owners, and some natural, like a massive hurricane or earthquake that destroys a part or an all of a community. For this reason, collective trauma studies have largely been bracketed from cultural trauma studies (Alexander et al. 2004). And yet, place-based destruction or displacement due to civil wars (O’Neill and Spybey 2003) or ethnic/racial oppression and segregation (Adams, Hattum, and English 2009; Fullilove 2016) can also shred the connective tissue and separate a collective or parts of it from the cherished moral and social anchorages to external sources of collective identity. For instance, Indigenous peoples’ stories are rooted in the recurring historical narrative of displacement and relocation (Brave Heart et al. 2011). The tendency to forcibly comingle different groups with different cultural modes of living, while also subjecting these populations to purposive, coercive cultural assimilation, further stripped these peoples of their attachments to a moral anchor, severing the link between the individual member and the collective. This sort of trauma is not simply historical, as many Indigenous communities struggle to reclaim the lost cultural center, while being geographically, socially, and culturally “isolated” from other communities because of lingering prejudice and discrimination.
Communities that have suffered collective trauma are always at risk of a newly devastating blow, like a boxer whose cut was temporarily sealed between rounds. In 2014, for instance, the murder of Michael Brown was an acute blow to the Ferguson, Missouri Black community, triggering a protest response that, as it was met by police, produced a second source of collective trauma. What distinguishes this from the trauma of Erikson’s flood is that, on one hand, the definition of collective trauma applies neatly to Ferguson as a self-contained minoritized community, while on the other hand, Black Americans are diffuse throughout the U.S. population and, through traditional and social media, were exposed to the same trauma stimuli. But, this distinction between corporate units, like groups, organizations, or geographically bound communities, and categoric units, like Black, Asian American, or any social identity, underscores the scholarly distinction between collective and cultural trauma and exposes blurring at the borders.
For Black Americans, like Indigenous peoples, the collective identity to which their personal identities are anchored is rooted in separation from cherished social objects, isolation and exclusion, and rejection. Black Americans’ story is rife with displacement from place (Fullilove 2016). Thus, a sort of priming for subsequent acute blows comes with the territory, which in turn accounts for the sorts of daily affectual, cognitive, and behavioral strategies employed by many Black Americans to shield themselves from small and large traumas (DeAngelis 2020) and their negative physical health consequences. However, a significant amount of the negative mental and physical health outcomes Black Americans, or any number of other minoritized groups, face in the United States or elsewhere is predicated on cultural trauma, or the real, imagined, or anticipated attacks on the collective identity from which they draw a sense of belongingness within a diffuse class of others with shared history and destiny.
Cultural Trauma
Cultural trauma, as distinct from collective trauma, moves from the separation of members from social infrastructure to the construction, adoption, and maintenance of a collective identity rooted in past and ongoing “physical and psychological assault or stressor perpetuated by an oppressive dominant group on the culture of a group of people sharing a specific shared identity” (Subica and Link 2021:1). The assault is less on a physical place and tangible objects than on the cognitive and symbolic center of a class of people, often mediated via the interpretation and framing of the trauma and its meaning for the collective identity by entrepreneurs or various forms of media (Alexander 2004). The identity often is tied to a collective trauma event or set of events as “represented in the collective memory of the group” (Hirschberger 2018:1), but these events are usually animated by ongoing acute blows that range from minor—the sort of systematic discrimination found in a racialized organization (Ray 2019)—to major—Brown’s or George Floyd’s murder. Contemporary Black or Jewish Americans, for instance, did not directly experience slavery or the Holocaust, and yet have been subjected to ongoing assaults at different times since. For Black Americans, slavery was followed by Jim Crow laws, the perpetuation of segregation—and its expansion via red lining, highway construction, and other political and economic tools (Fullilove 2016)—and, today, recurring everyday assaultive policing and high-profile police violence. Thus, the direct experience is replaced or superseded by the internalization of this social identity by a significant proportion of members belonging to the class (e.g., Black Americans) such that members are acutely primed for both daily and spectacular assaults, endure negative physical and mental health outcomes because of the threat and experience of these assaults (Monk 2015; 2020), and often adopt defensive strategies designed to mitigate the mental and emotional costs of these assaults.
Groups defined by collective trauma, then, are dealing with constant threats to their ability to build meaningful attachments to social objects that generate purpose and imbue their personal identities with confidence. Cultural trauma, however, is predicated on exclusion from access to privilege, status, and power while attaching oneself to an identity whose history and destiny is rooted in trauma narratives. It is also about isolation, in varying degrees, manifest in residential, marital, occupational, educational, and other segregations. Finally, it involves rejection, situationally through status expectations about competence, performance, and reward (Ridgeway 2019) and, at worst, through stigmatization that severely reduces economic chances, social ties, and the like (Link and Phelan 2013).
Cultural trauma affects mental health in several ways. Groups integrate and regulate their members based on some form of shared culture (Subica and Link 2021), and cultural trauma involves the degradation of this culture, constraints on its perpetuation, and even its appropriation. Racialized organizations (Ray 2019) further affect health, as members do not simply experience their lower status in everyday interactions. Rather, dominant institutional systems like polity, economy, law, medicine, and education often trigger the social identity and the trauma associated with it, and research shows that institutional disprivilege leads to stress and poorer health outcomes (Adler 2009). Furthermore, the separation from or intense regulation and restriction of a people’s physical and geographic space can have the twin effects of delimiting the enactment of their cultural ways of living, strip institutional control away, and effect the practical needs of the group as material resources like housing or food are constrained or made scarce.
The deleterious effects of cultural trauma are becoming better understood. Research on Indigenous people has found widespread negative health outcomes stemming from the group-level trauma they have endured (Brave Heart et al. 2011). The stress Black Americans experience trying to manage day-to-day racist microaggressions (Monk 2020) leads to concerted affectual, cognitive, and behavioral strategies associated with a slew of poorer physical health outcomes (DeAngelis 2021; DeAngelis et al. 2022). Second- and third-generation American Jews appear to have greater rates than expected of various mental illnesses attributable, in part, to the intergenerational transmission of the cultural trauma rooted in the Holocaust (Scharf 2007). Indeed, recent reviews of the literature show that cultural trauma may be a fundamental cause of health disparities, as it has a direct relationship to a panoply of mental health challenges (Subica and Link 2021).
If cultural trauma is a fundamental cause, the question is whether it remains tenable to treat it as a sociological abstraction or metaphor for some otherwise “black boxed” processes as Alexander et al. (2004) intend or whether there is something ontologically real that can be identify. This criticism is not necessarily reserved for this form of trauma only, as collective trauma suffers from a lack of empirical realism because it too relies on Durkheim’s homo duplex, or the ontological position that the social is truly discrete from the individual, an untenable position, to be sure (Lizardo 2009).
To overcome this issue, I would argue that what unites the two types of trauma most clearly and thus serves as a potentially good starting point for their integration is the concept of trauma and its allusion to pain. A lot of sociological concepts evoke pain (Abrutyn 2023), though usually metaphorically, because sociologists tacitly conceptualize pain as something biological and psychological (Zajacova et al. 2021). Rather than risk reductionism, actual pain is substituted conceptually by terms like anomie or, in the present case, trauma. In both collective trauma and cultural trauma, pain matters. Erikson observed the widespread complaint of psychosomatic pain, as though Buffalo Creek denizens had lost a limb or had suffered painful, slow-to-heal wounds. Cultural trauma, too, evokes pain. Not the physical kind that victims of police violence experience, but pain nonetheless.
To avoid metaphors, I next consult the science of social pain, which may help ground these social phenomena in the actual neurophysiological experience of pain and, therefore, the same sorts of preconscious responses (collectivized, of course) that any organism employs to mitigate and avoid the cause of their pain.
Social Neuroscience And Social Pain
In its simplest form, physical pain is an evolved, protective alarm designed to prevent an organism’s death. The neural circuitry of pain consists of two apparently dissociable process (Rotge et al. 2015): the sensation of pain and the affective response to said sensation. The sensation of pain is triggered by noxious stimuli, like the acute sting of a rose’s thorn or the tonic throb of a stubbed toe, and it is processed in the primary and secondary somatosensory cortices and posterior insula of the brain. The affective dimension of pain is the innate reaction to the sensation that triggers emotional, cognitive, and behavioral responses to mitigate or avoid the noxious stimuli. The affective aspect of pain is also intimately tied to learning (whether reinforcing, updating, or creating) new schema about objects in our environment (LeDoux 2012). The affective pain circuitry is found primarily in the dorsal anterior cingulate cortex (dACC) and the anterior insula (AI). The dACC, notably, plays a unique role in linking the brain’s limbic (affective) systems and the prefontal (cognitive) cortex. Hence, it serves as an alarm for signaling pain and distress (Spunt et al. 2012) as well as the preconscious/unconscious and conscious effort to respond to said pain while also serving as a recorder, storing in our memory the success or failure of our response as well as details about the original triggering stimuli (Reeve and Lee 2019). Importantly, functional imaging shows that the dACC is activated only during the affective response to pain, which squares with research on patients with damage to or loss off the dACC who can identify where the pain sensation occurs while simultaneously not being bothered by the pain (Eisenberger 2015). The dissociability of the two neural pain circuits is key to understanding social pain, which tracks along the affective system and not the sensorimotor system.
The study of social pain began when affective neuroscientist Jaak Panksepp (1998) hypothesized that the brain’s opioid centers, responsible for pleasure and pain relief, had been “exapted” during mammalian evolution for promoting social bonding. Mammals experience intense distress, panic, and, over time, grief when separated from their primary caretakers, an evolved response that most of us have experienced as children when we have lost sight of a parent in a crowded place and some of us have experienced as parents who have lost sight of our own child. Subsequently, cognitive scientists MacDonald and Leary (2005) found that the lexical references to severe types of rejection or exclusion, like experiencing unrequited love, cross-culturally used synonyms of hurt, injury, or pain. Over time, these findings were supported by a diverse array of neuroimaging, self-report, and behavioral studies (Eisenberger 2015; Rotge et al. 2015). As such, social pain is defined as the affective response to real, imagined, or anticipated separation, rejection, exclusion, or isolation from cherished social objects. Although social pain runs along one of the same neural circuits as physical pain, it is distinguishable as a mixture of demoralization, dysregulation (in the Durkheimian sense), and emotional distress. While it may be tempting to measure social pain using popular cognitive appraisals like “loneliness,” the affective signature of pain should register around panic and grief (Panksepp 1998), processed through any number of emotions, including intense fear or rage, shame, or, in many cases, a cocktail of undifferentiated emotions that demands our immediate attention.
Cognitively, social pain, like any affective response (LeDoux and Brown 2017), coordinates decision making, interpretation, perception, and learning, as we try to figure out what is causing the pain and how best to respond; in some cases, the social pain can command or even control our cognitive functions. Finally, like physical pain, social pain is an alarm that motivates behavioral responses designed to mitigate or avoid the stimulus. Unlike avoiding a cactus or removing a splinter from our finger, however, social pain is rooted in social environments in which we have less control. Thus, one might expect that defensive strategies will have higher costs (Summers-Effler 2004). Avoiding whole groups of people or places may be impossible or impractical, for instance, meaning that a Black American must enter White spaces regardless of the potential for harm (Anderson 2015). Ultimately, behavioral responses may be prosocial (e.g., finding social support) or risky, like the abuse of opioids that counteract the neurobiological effects social pain has on our pleasure centers in the brain (Inagaki 2018). All of this is to say that social pain exacts a cost on our mental health, particularly when it is chronic (MacDonald and Leary 2005).
If social neuroscience has a central limitation, it is its lack of understanding of sociological theory and the fact that people can become attached to just about any object as an extension of self—including abstract groups, places, objects, and even rules, values, norms, and so forth. That is, we can feel panic and grief when we are separated, rejected, excluded, or isolated from the things to which we have come to feel strong affective attachment, especially if we blame ourselves or widespread beliefs and narratives blame us for this rejection.
To recap, when differentiating the two forms of trauma, we can say that collective trauma is the acute separation from social infrastructure, 1 whereas cultural trauma is usually about exclusion, rejection, and isolation from access to various social objects. In both cases, social pain is the fundamental biopsycho experience, and, as such, it helps us explain the urge to respond affectually, cognitively, and behaviorally. However, both forms of trauma are unique from the social neuroscience literature on social pain precisely because the pain process (the cause, experience, response) is collectivized. It is not an individual-level phenomenon. This is especially important with regard to the response to this pain. Responses may be culturally sanctioned, they may emerge within the group and become a part of the collective identity, and so forth.
If these assertions are on the right track, then the two forms of trauma are actually not distinguished by their shared biopsycho etiology. Instead, they belong to a more general social phenomenon we might call social trauma. Social trauma is the collectivized separation, rejection, isolation, and exclusion of a corporate and/or categoric unit that motivates affectual, cognitive, and behavioral responses externalized and enculturated in a collective or social identity. The concept of social trauma brings sociological ideas into social neuroscience, distinguishing individual-level social pain from a phenomenon in which a group or class of people becomes defined by its past and ongoing experiences of social pain. It is not simply an internal or intrapersonal feeling, but one that emerges in external representations, is corporeally experienced in mundane and spectacular rituals, and is internalized within personal identities produced and reproduced by these representations and rituals. Social trauma, thus, scales up and down. When a significant proportion of people experience a tragedy, it amplifies the experience for those within the community and, through mediating mechanisms, those identifying with the community. A key advantage to this conceptualization of social trauma is its ability to distinguish itself from other concepts, yet remain broad enough to encompass a panoply of cases like disasters (Tierney 2019), intensely marginalized categories of people, refugees forcibly or willingly fleeing violence, and, also, the communities subjected to outbreaks of violence (e.g., high schools, prisons) like suicide clusters (Abrutyn and Mueller 2016) and rampage shootings (Newman et al. 2005). It also makes sense of vicarious experiences of social trauma—for example, when members of the LGBTQ community or Asian Americans identify with a victim of a high-profile hate crime (Bell and Perry 2015; Lim 2009).
Ultimately, the grounding of social trauma in social pain suggests a neurobiological reaction and set of preconscious responses, collectivized to be sure, to precipitating environmental stimuli. It is ontologically real. And, if physical pain can lead to negative mental health outcomes and an assortment of pathological behavioral responses, there is plenty of evidence to suggest social pain does as well (Inagaki 2018; Panksepp 1998). But the inverse must be considered as well: if social trauma connects sociology to social neuroscience, then what can sociology offer social neuroscience while also providing a well-articulated theory from which sociologists can draw.
Theorizing Social Trauma
Collective and cultural traumas differ in their direct exposure to social pain stimuli, yet the event itself matters for both. Thus, understanding how different trauma-inducing events vary allows for the systematic study of the trauma process. Four dimensions of trauma events can be identified, leading the following theoretical outline to be guided by two basic propositions. The first states the following:
P1: Social trauma is a positive function of the real, imagined, or manufactured (1) intensity or magnitude, (2) extent, and (3) temporality of one or more precipitating event(s), and (4) the success of the ensuing recovery effort.
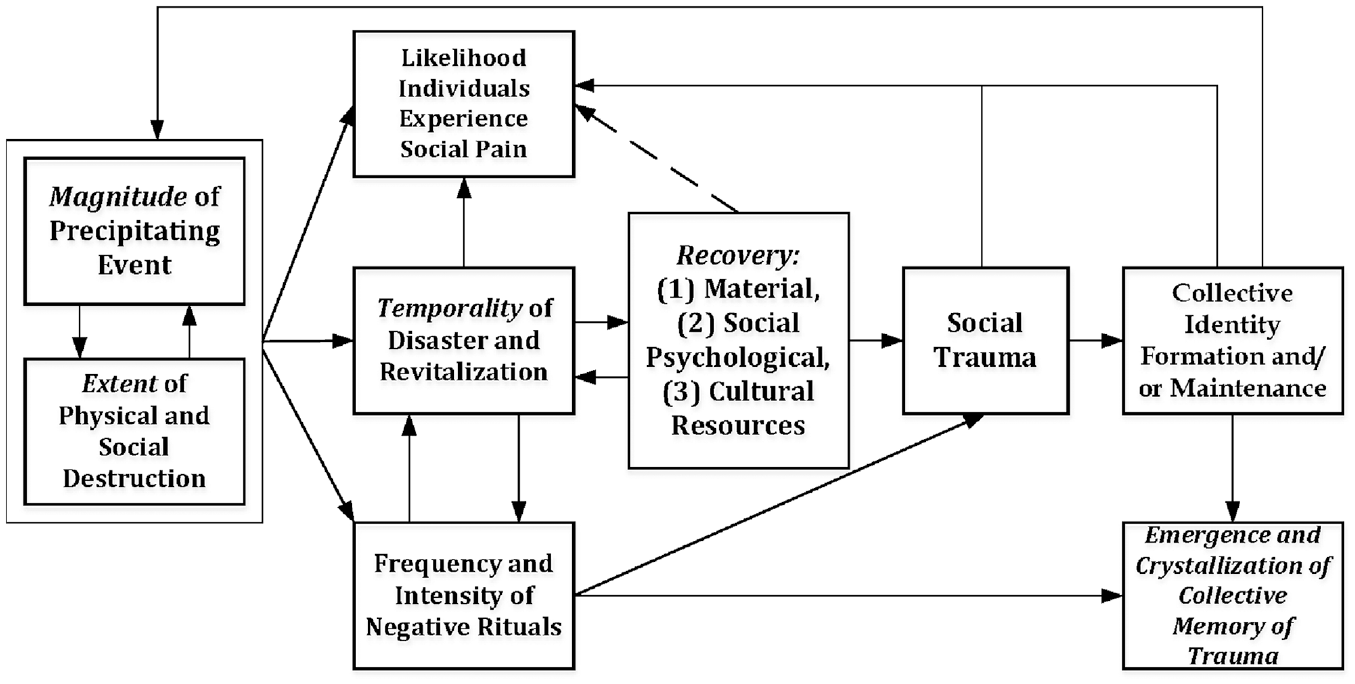
These first three dimensions are ordered in terms of causal preeminence, though they are often iterative (see Figure 1 below). While this approach does increase the complexity of the model, no theory worth its salt will oversimplify a causal process for the sake of simplification. In that vein, the fourth dimension, recovery, emphasizes three conditions that can facilitate or buffer the emergence of social trauma, or collectivized social pain: material, social psychological, and cultural resources. Ultimately, the discussion of the first proposition leads to an explanation for how and why social trauma becomes crystallized in a collective identity, which, though beyond the scope of this article, may be mobilized for collective action:
P2: The greater is the degree of social trauma, the greater is the shared experience of social pain, and the greater are the pressures for creating, reinforcing, or updating a collective identity predicated on the trauma narrative.
The making of a social trauma.
Magnitude
When it comes to collective trauma, a trauma event’s magnitude may be defined as its intensity. Intensity, in turn, is given by (1) the sheer number of people displaced, injured, and/or killed, (2) the visibility and spectacle of ruin, and (3) the sudden, unexpectedness of the event. Magnitude is a function of the cost of human life, as well as the amount and “density” of horror survivors must deal with immediately and over time. However, magnitude cannot only be measured in the cost of life. A suicide bombing, for instance, produces carnage, but is dwarfed in comparison to the flying of two planes into two tall, visible towers in the largest city in the United States or the leveling of a city with an atomic bomb. In this comparative example, the death toll matters but so does the spectacle. A war, nuclear meltdown, or hurricane leaves in its wake infrastructural damage that serves as a painful reminder of what once was, while also tearing the arteries or conduits along which the most routine interaction rituals occur. The physical representations of collective identity are shredded alongside the social occasions, gatherings, and routines that continually renew the otherwise abstract notion of community and belonging. In Anthony Wallace’s (2003:153–54, emphasis added) words,
The sight of a ruined community with houses, churches, tress, stores, and everything wrecked, is apparently often consciously or unconsciously interpreted as a destruction of the whole world. .. The objects with which he has an identification, and to which his behavior is normally turned, have been removed. He has been suddenly shorn of much of the support and assistance of a culture and a society upon which he depends and from which he draws sustenance; he has been deprived of the instrumentalities by which he manipulated his environments; he has been, in effect, castrated, rendered impotent, separated from all sources of support, and left naked and alone, without a sense of his own identity, in a terrifying wilderness of ruins.
Thus, we can posit two propositions related to magnitude as a causal force:
P3: The greater is the magnitude of a disaster, the greater is the pressure to make sense of the loss of physical and social anchorage to others and/or the center and reconstruct the collective’s identity. P3a: The greater is the magnitude of disaster, the greater is the urge to memorialize the trauma event in ritual and representational space.
While P3 speaks for itself, P3a points to a core insight from cultural trauma studies that can be usefully imported for social trauma (Simko 2020): memorialization is one key pathway toward transforming collective into cultural trauma. The memorial, in true Durkheimian ([1912] 1995) fashion, creates an external representation that can become a formal or informal pilgrimage site acting a center of gravity for collective identity formation and reproduction (Turner 1973). Furthermore, memorialization serves as a mechanism by which social trauma more broadly can be transmitted horizontally (across populations who come into contact with the memorial) and temporally (intergenerationally) (Gómez-Barris 2010).
Memorials, incidentally, need not be statues or elaborate constructs. Negative space, as in ruins or missing physical infrastructure, can become a real or symbolic pilgrimage center that orients people sharing a collective identity. For instance, in its absence, a formerly vibrant Black neighborhood—for example, the Black Wall Street destroyed in Tulsa—can serve as a reminder of past collective traumas brought about by racist violence that reverberate decades or centuries later just as Auschwitz has become an actual museum. Magnitude, then, not only strikes the acute blunt blow but also endures in material reality.
Extent
The extension of an event’s effects in physical and social space refers to the trauma event’s extent, or (1) the geographic scope of a disaster and ensuing trauma and/or (2) the demographic scope—that is, the sheer number of people affected by the trauma, not only in terms of direct experience, but through direct and indirect means of diffusing social emotions (like empathy), interpretations, and social pain. As noted earlier, even those Buffalo Groveans absent from the flood came to experience collective trauma, having “caught” it vicariously upon return. Or, consider a more recent example, 9/11, with severe consequences for New Yorkers, both those who were in Manhattan or across the river watching, as well as those who would later survey the wreckage of Ground Zero. But, for most Americans and anyone else watching the 24/7 coverage, seeing planes fly into a recognizable symbol of America, watching it smolder and smoke and collapse, seeing people jumping out of one of the towers, and listening to the endless dissection of what happened, what was happening, and what it meant spread the trauma quite efficaciously. Thus, extent is about how widely the acute blow’s effects become known.
Two propositions summarize extent:
P4: The greater is the extent of a trauma event, the more likely it is to diffuse social pain across a wider and more diverse population. P4a: Generally speaking, magnitude varies positively with extent, but, in cases of cultural trauma, extent may manufacture perceptions of greater magnitude.
What corollary P4a suggests is that the causal relationship between magnitude and extent may flip from collective to cultural trauma. The former suggests magnitude drives extent, for obvious reasons, but the latter, predicated on reinterpretation and narrative-making, allows entrepreneurs to manufacture social pain, outrage, and other emotions that shape how intense an event in the past or, especially, in the present is supposed to have been. Thus, while systematic research is necessary, some research suggests LGBTQ hate crimes reverberate beyond the victims, triggering the sorts of self-reports we would expect when social pain becomes collectivized and enculturated into social trauma—for example, LGBTQ folks who learn about the crime felt “anger, pain, worry, sadness, isolation, anxiety, depression, bewilderment, and disgust” (Bell and Perry 2015:106). What this suggests, ultimately, is that communication matters.
This implies a second corollary of great importance to the mechanics of extent:
P4b: Extent is constrained by the degree to which (1) transportation and communication technologies are delimiting and (2) geographic, social, and cultural barriers remain intact.
On one hand, as the flow of people and information in time and space accelerates, so too does the diffusion of collective trauma. For instance, displaced survivors become refugees (O’Neill and Spybey 2003), bringing their pain with them or potentially overwhelming host sites. Likewise, as Randall Collins (2004:55ff.) has argued, TV/online video is superior to radio as a medium of collective arousal-making because it blends sights and sounds in ways that uniquely affect our neurophysiology. Not only do we see survivors or refugees but also the media can refract their situation in ways that can make us more or less aware of and more or less sympathetic or resentful toward their pain and trauma. On the other hand, geographic, social, and cultural barriers may also constrain or facilitate the flow of information and people. Some privileged communities may be able to weather a crisis because their members can leave temporarily, have the means to rebuild, or are better equipped to leverage political and economic resources for reconstruction (Picou, Marshall, and Gill 2004). In other cases, geographic, social, and cultural barriers may block affectual responses such that trauma remains place-based. General Americans’ negative attitudes toward Indigenous people combine with the fact that many Indigenous communities are residentially segregated from white communities such that sympathy is difficult to generate.
Temporality
Trauma events may also extend in time. First, the actual length of time that the trauma event lasts matters similarly to the dynamics of extent. Second, recurring shocks matter to both healing and recovery processes. The number, frequency, and spacing of shocks can prolong the trauma event or introduce new acute blows. Hence,
P5: The likelihood a trauma event will require identity work is a positive and additive function of (1) the duration of the event and (2) the number, frequency, and spacing of aftershocks.
Each of these dimensions of temporality is independent, but additive, generating some useful observations. For instance, the duration of an event, like an atomic bomb, is rendered unimportant because of the magnitude, extent, and duration of the ensuing recovery. Collective trauma, as a rule, tends to be triggered by shorter sharper blows, like a massive hurricane or flood; cultural trauma is far more complex. Whereas Michael Brown or George Floyd’s deaths represent the sort of acute blows that radiate outward throughout the broader American Black population, racialized organizations may trigger less intense feelings of social pain more frequently (Ray 2019). Similarly, a school shooting may be devastating to a high school population, but the recurring shooter and lockdown drills combined with the frequent news reports of gun violence throughout the United States may produce low-level cultural trauma for a far broader set of high school students. Indeed, many collective identities forged, in part, through social trauma have these sorts of vacillating types of trigger events. LGBTQ communities will feel the pain of a high-profile hate crime just as Black communities feel the pain of another victim of police brutality, while daily interactions are laced with the actual effects of discrimination and the ever-present threat of stigma (Link and Phelan 2013).
Recovery
Recovery is related to temporality, but is a distinct dimension (as reflected in the literature on disasters), in part because it fits neatly into the causal chain shaped by the magnitude, extent, and temporality of a trauma event. This is to say, massive destruction is more costly and time-consuming to rebuild, extensive damage produces greater challenges as restorative resources are stretched thin and conflict between parties grows more likely, and some types of crises invite new precipitating events before the old ones have been repaired. For victims of social trauma, recovery can also be complicated. Holocaust survivors did not simply move on with their lives, but, in their striving to do so, crafted a trauma-based identity that they passed down to their children and grandchildren (Scharf 2007). School shooting survivors sometimes become political activists (e.g., David Hogg), while Black and Indigenous Americans navigate recurring events that trigger the trauma narrative of their respective collective identities. Recovery, thus, is not linear.
Recovery, however, offers an entry point to thinking about the sorts of contingencies that help explain variation across cases of social trauma. Although any number of “variables” might be selected for shaping recovery, I posit,
P6: The degree to which recovery conditions or sustains social trauma is a positive function of (1) extant material resources, (2) the distribution of social psychological resources, and (3) the content and availability of cultural resources.
Material resources
That recovery is dependent on political economy is not surprising, in so far as the availability and distribution of material resources follows broader and local social stratification systems and has both practical and symbolic consequences. Inequitable distribution of resources, for instance, leads to better and worse preparedness for disasters (Adams et al. 2009) and recoveries on the other (Picou et al. 2004). Wealthier communities or neighborhoods, however, can mitigate the intensity and extent of a disaster, leveraging their wealth to reduce deaths (Arcaya et al. 2020), facilitate recovery, and, in the case of cultural trauma, provide individuals with wider safety nets and greater access to diverse, quality mental health care (Subica and Link 2021). Theoretically, of course, lack of adequate resources is not a zero-sum game. Communities or groups that fit into superordinate categoric units (Ridgeway 2019), like poor whites in the United States, might be more likely to receive assistance in the form of direct and indirect material resources, volunteer human labor, and, importantly, sympathy from beyond the community, but they may also be acutely vulnerable to social trauma (DeAngelis et al. 2022).
Social psychological resources
A second contingency speaks to the psychological, emotional, and social psychological resources any given individual exposed to a traumatizing event can access. Clearly, medical and mental health disparities are not randomly distributed (Link and Phelan 1996). When lots of people with histories of trauma aggregate, the possibility of serious social trauma increases because those folks are lacking the necessary individual resources to weather a storm. That said, some communities also suffer from long-standing cultural trauma that is not simply internalized when new members are exposed to the collective identity, but becomes inscribed in the physical and social landscape; these inscriptions, in turn, serve as Durkheimian external representations that collectivize memory. Social disorganization theory argues that disrupted social milieus attract or produce, depending on one’s position on causality, pathological outcomes like crime, mental illness, and violence (Sampson and Groves 1989). Where social psychological resources are stretched thin, precipitating events are more likely to translate into social trauma or reinforce collective identities steeped in trauma narratives.
Cultural resources
Recent work by Subica and Link (2021:3) points us to two types of cultural resources that may mitigate the effects of social trauma: cultural modes of being and cultural lands. By cultural modes of being, they mean that groups are able to maintain the sort of elements of culture that undergird the social infrastructure necessary for well-being and health which are often more resilient. In most cases, Indigenous groups have been severely restricted from or stripped of many aspects of their cultural modes of being, which reduces their ability to cope individually and collectively (Brave Heart et al. 2011). By cultural lands, Subica and Link refer to the material and symbolic location of the community. Social infrastructure need not be rooted in place, but our social self is built up, in part, on geographical location, and thus place becomes entwined with collective identity. We have seen this dynamic earlier in the discussion of memorialization as well as in thinking about one aspect of the social pain experienced by refugees or others displaced (like Black Americans who have seen neighborhoods laid to waste or split in half by highways; Fullilove 2016). Where the dominant group actively works to control space and the flow of information and movement, resilience may be weakened.
Subica and Link mention a third cultural resource, institutions, arguing that these can buffer against trauma. In a community, then, that is oppressed politically and economically from without having strong kinship and religious institutions may provide some source of support and well-being. But, it is an open empirical question how much. Consider how the historically low Black American rate of suicide has long been explained via cultural explanations (Spates and Slatton 2017), particularly the idea that the Black Church and extensive kin networks are protective. Yet, while Black Americans tend to have lower rates of suicide as well as mental illness—notably, this has been changing over the last decade or so (Cureton et al. 2023)—they disproportionately suffer from physical maladies related to chronic stress (DeAngelis 2020). Is it possible that what is protective against one form of trauma might amplify others? Today, cultural resources are one of the most exciting frontiers for new research on social trauma.
Implications
The theoretical model is visualized in an analytic form in Figure 1. The model begins with the two key forces driving the emergence of social trauma, magnitude, and extent. Notably, neither is primary; often, they are locked in a feedback loop. This loop determines the various elements of temporality, the likelihood that any given person subjected to the event will experience social pain, and how often “normal” interaction rituals are replaced with rituals reflecting and reinforcing the erosion of social and physical infrastructure. As the crisis unfolds and recovery begins, the role of resources comes into play. As noted previously, recovery and temporality are intimately related, but, in drawing on the stress process literature (Aneshensel and Avison 2015; Wheaton et al. 2013), recovery is related to the experience of social pain with greater resources predicted to buffer the intensity and duration of any given members’ experience. In turn, the outcome of high magnitude, extensive, enduring events is social trauma, which increases the likelihood that members will experience social pain directly or vicariously. As rituals intensify the social trauma, the search for a new collective identity (or the reinforcement and updating of an existing identity) grows as does the likelihood of memorialization and, thereby, the external representation of said identity. And, once this identity enculturates trauma, it increases the likelihood that members will feel social pain and it increases the magnitude and extent of future precipitating events, given that those possessing the identity are more likely to perceive additional events as salient and painful.
A Sociology of Pain and Affect
The most important set of implications rests on incorporating pain—or, more accurately, social pain—into the sociological lexicon (see, for instance, Abrutyn 2023). To that end, this theory first grounds sociological trauma—collective and cultural—in the social neuroscience of social pain, allowing us to distinguish social trauma from its psychological counterparts. Importantly, the mechanisms by which key cognitive processes associated with identity formation and maintenance, like memory, are activated and sustained are revealed: intense negative affect is one of the most powerful motivators of action and sources of learning and memory (LeDoux 2012). And, these neurobiological responses are tied to the construction of a social self (LeDoux and Brown 2017). Sociology, of course, teaches us that our social self is always anchored to one or more collective identities, which helps us make sense of why the same processes that might happen inside a person can collectively occur within a group of people. The personal becomes collective, saturating and priming the individual’s self for the experience of social trauma, or collectivized social pain. Put differently, social trauma becomes a social phenomenon that can affect a specific corporate unit—for example, a small community that has suffered a series of suicide clusters (Mueller and Abrutyn 2016)—or a broader class of people, like Black Americans (Fullilove 2016; Monk 2020).
Secondarily, social trauma and social pain highlight the causal impact of affect on cognition and behavior, well-being, and health. While affect and emotion have become important factors in sociology, they remain relegated to dependent variables (e.g., emotions are constructed by structure and culture) or mediating variables (cognition causes negative affect which causes interpretation and action). Yet, social pain is an evolved, affective response that requires no learning (Panksepp 1998). In fact, it is a learning mechanism in so far as any object can come to be considered noxious through experience or vicarious modeling; people respond to separation, rejection, exclusion, and isolation with panic and grief. Social trauma points toward not only the collectivization of this pain but also the collectivization of responses. In some communities, this might mean a rise in alcohol and drug abuse, such as what we might find in poorer white places (Case and Deaton 2020), while in others, it might generate the search for a fundamentalist religious community that can provide the sense of belongingness from which individuals feel detached. Why one response or another emerges is, ultimately, an empirical question worth pursuing in future research, but beyond the scope of this article.
A third implication of this schema is the way treating social pain and trauma in this way supplements other traditions in behavioral social science like the stress process model (Pearlin 1999), which also highlights the causal importance of pain and trauma, but tends to focus on physical pain and does not distinguish between psychological trauma (e.g., that experienced by sexual and physical abuse victims) and the sociological trauma considered here. Besides the neurobiological distinction we can draw, some stressors or stress-related phenomena are different from others. The sudden destruction of social infrastructure is qualitatively distinct, and it has direct causal links to poor mental health outcomes (Raker et al. 2019), as do historical and ongoing attacks on a group or class of people’s cultural reality (Subica and Link 2021). Likewise, social pain appears to have direct routes toward physical (Inagaki et al. 2018) and mental illness (DeAngelis 2020; DeAngelis et al. 2022), while serving as primary and secondary stressors that subsequently have indirect pathways toward negative health outcomes. To be sure, this refinement does not negate the insights of stress process theory, but expands them while borrowing ideas from the model such as the import of resources as buffers (Aneshensel and Avison 2015).
Finally, by treating pain more systematically, a theory of social trauma contributes to a gap in sociology with regard to a sustained focus on pain (Bendelow and Williams 1995; Zajacova et al. 2021). This includes the observation that while physical pain is a serious problem worthy of sociological attention, our capacity to affectively attach ourselves to specific, general, and imagined others as well as physical objects (like places or things) and abstract objects (like external representations, institutions, or values/norms) makes social pain as important as physical pain, if not more so. Sociology lends so much theoretical power to future research on the dynamics of social trauma. Social trauma can be built up from the destruction of a place, from the systematic exclusion of people and their separation from cherished objects, or other forms of isolation. If social pain due to separation, rejection, exclusion, or isolation is collectivized (e.g., experienced by a community of people simultaneously) or enculturated (e.g., the experience of social pain is indelibly tied to collective identity), then social trauma can be said to be real.
Expanding Our Explanatory Lens
Much of the analysis above draws from myriad marginalized communities, like Indigenous, Black, or LGBTQ communities, and their experiences of imposed traumas; it may also provide sociological explanations for the plight experienced by other communities not historically discriminated against or oppressed. As Case and Deaton’s (2020)“deaths of despair” research argues, white communities evince a significantly high rate of opioid overdose, alcohol liver disease, and suicide rates because of growing rates of “despair” predicated on the erosion of their way of life. Indeed, the abuse of opioids, of all possible drugs, points directly toward the ubiquity of social pain and social trauma: opioids dull the pain of rejection and exclusion (Inagaki 2018; Pansksepp and Watt 2011). Hence, the social pain and social trauma perspective provides greater context and more precise mechanisms for making sense of the widespread abuse of painkillers.
In this case, there are, arguably, three levels of social pain operating simultaneously.
At the macro level, Merton’s (1938) strain theory makes sense (DeAngelis 2020). White working-class Americans, especially men, have been socialized into a system that purports to favor them, imparting a set of values and goals that they should achieve because of their high valuation and status. And yet, their success has been eroded, gradually and imperceptibly at first, but rapidly and noticeably in the last decade or so (Cherlin 2018); thus, while separation, in neuroscience and even sociology, is often thought of in terms of real social relationships, it can also mean separation from the abstract objects (ideals, institutions, beliefs, values) that invigorate social reality (Rambotti 2022). Moreover, for several decades, Fox News and now the wider Conservative media ecosystem has been eliciting anger and fear by repeatedly presenting the white working class as excluded from political, educational, and cultural spheres (Rotolo 2022). At the meso/community level, towns where white working-class Americans predominate have been declining for decades. Social infrastructure has, in fact, been dissolving. Putnam’s reference to “bowling alone” cataloged this in his famous book, but other sociologists of small town life have shown this to be the case as well (Wuthnow 2018). Social pain has collectivized into social trauma as echoed in Hochschild’s (2016)Strangers in the Own Land, where white folk in a small southern town felt the anonymous, distant threats from Washington D.C. and an amorphous economy as causing the “frightening loss. . . of their cultural home, their place in the world, and their honor” (p. 54). Intergenerational linkages have broken down as young people left for opportunities, unions and other associations had disappeared a fog of “golden ageism,” and the sense of sharing a destiny had been under siege from progressivism and the swapping out of folks like themselves for “foreign” workers and refugees seeking the American Dream. Finally, at the micro or individual level, rising rates of morbidity and mortality have winnowed people’s actual social networks through tragic and suspicious circumstances. Social pain intensified as it became clear that everyone within these communities had their own stories of family and friends who had succumbed to alcohol, drugs, suicide, or some other self-destructive behavior.
A second example that has been mentioned in passing throughout this article is the exposure to intense violence that some socially, culturally, and geographically bounded spaces experience and the possibility that a social trauma frame may help make sense of the outcomes. High schools, for example, are vulnerable to suicide clustering and rampage shootings. High school students spend inordinate amounts of time in their schools and, thus, a student suicide cluster—which is not just defined as two or more deaths, but also the prevalence of attempts, ideation, and nonsuicidal self-injury (Abrutyn and Mueller 2016)—can serve as an acute blow to an entire high school community, with ensuing deaths and tragedies retarding recovery. 2
Conclusion
A theory of social trauma and social pain reimagines a classic sociological problem related to integration, connectivity, and belongingness. In a sense, Emile Durkheim’s ([1897] 1951) most important contribution—that social solidarity is positively related to social (and individual) health—is once again validated. Mental, emotional, and physical health depends on being connected, not just for the sake of social capital but as a matter of feeling like you matter (Elliot et al. 2004), feeling self-assured, and feeling a sense of purpose and meaning. To be sure, not all connections are healthy, positive connections (Mueller and Abrutyn 2016), but this empirical fact does not detract from the existential danger people face when separated, rejected, excluded, and isolated from the social objects external to us which draw the internal biopsycho essence of self into a web of social relations. As such, social pain may undergird other sociological concepts that describe specific types of separation or rejection, like stigma, anomie, or alienation. Although it is beyond the scope of this article to dig deeper into the conceptual and empirical implications social pain and social trauma have for these concepts, it is enough to suggest that any sociological question focused on attachments to mutually constitutive objects and concepts has the potential to examine social pain when these ties are threatened or lost.