
Abstract
Prior research has explored the consequences of the sudden transition to remote work during the pandemic. Less is known, however, about how the mental distress of individuals who changed work locations during the pandemic differed from that of those who consistently worked from home or consistently worked on-site, nor to what extent these differences varied across worker characteristics, such as gender and caregiving obligations. This study addresses these gaps using data from the Pew Research Center’s American Trends Panel survey and a Stress Process Model framework. Results show that those who transitioned into working from home during the pandemic reported greater mental distress than those who consistently worked from home or on-site. This association was larger among women with school-aged children. These findings suggest that structural changes in work location during the pandemic were more strongly related to mental distress. Moreover, the finding that this distress was unevenly distributed by gender and caregiving obligations has important implications.
Introduction
The emergence of the COVID-19 pandemic posed serious mental health threats to the life of Americans. Widespread job losses, concerns about contracting COVID-19, enforced lockdowns, and the closures of daycare centers and schools created unprecedented challenges for people in managing their daily lives and their work and family responsibilities (Restubog, Ocampo, and Wang 2020). A brief released by the World Health Organization (2022) concluded that anxiety and depression levels increased by 25 percent around the world during the first year of the pandemic. According to the Kaiser Family Foundation’s analysis of U.S. Census Bureau Household Pulse Survey data (2020–2023), around 36 percent of American adults reported anxiety and depression in April 2020, reaching a peak of almost 40 percent in February 2021, and remaining at 32 percent from February 2022 to present. This indicates that many adults are still struggling with mental health issues almost three years after the onset of the pandemic (Panchal et al. 2023).
Accordingly, the COVID-19 pandemic context provides us with a valuable opportunity to examine how mental health is influenced by rapid, macro-level structural changes, such as those that occurred to the social institution of work (Moen 2022). In particular, the pandemic’s widespread, mandated transition into working from home (hereafter “TWFH”) (Kosteas, Renna, and Scicchitano 2022) challenged our existing knowledge on the work-family interface, offering work-family scholars and policymakers an opportunity to examine how fundamental disruptions to one’s work location (such as a TWFH) relate to mental health (Adisa, Aiyenitaju, and Adekoya 2021; Chambel, Carvalho, and Santos 2022; Fan and Moen 2023; Holingue et al. 2020; Lizana and Vega-Fernadez 2021; Moen 2022; Möhring et al. 2021; Sahni 2020). In the present study, we adopt the perspective of Mirowsky and Ross (1989), where mental health and mental distress constitute a single continuum. We thus conceptualize mental health as the positive state of psychological well-being. Mental distress, in contrast, is conceptualized as the absence (or opposite) of mental health (Payton 2009). Mental distress occurs when an individual experiences unpleasant feelings or emotions (such as sadness, disappointment, anger, worry, or a lack of motivation). With these conceptualizations in mind, we seek to more deeply explore how levels of mental distress varied depending upon whether workers experienced change or stability in their work location (at home or on-site) during COVID-19.
In the pre-pandemic period, working from home (hereafter “WFH”) was less common and mostly voluntarily initiated, while the pandemic’s shift to WFH was enforced and much larger, creating greater disruption to the social institution of the workplace (Kosteas et al. 2022). Pandemic period research on the effects of this TWFH has produced mixed results, with some studies finding negative consequences, such as increased work hours, anxiety and sleep problems, and heightened social isolation (see, e.g., Bolisani et al. 2020; Kim et al. 2023; Lizana and Vega-Fernadez 2021), while others found positive outcomes, such as less time spent commuting and increased family closeness (see, e.g., Adisa et al. 2021; Bolisani et al. 2020). Two recent studies using longitudinal data even found no relationships between a TWFH and work-family balance, burnout, or family/life satisfaction (Chambel et al. 2022; Möhring et al. 2021). To our knowledge, however, no existing studies have used nationally representative data nor a Stress Process Model framework (Pearlin 1989, 2010) to examine mental distress when comparing workers who TWFH versus those who had consistent work locations prior to and during the pandemic. Moreover, research has yet to determine whether the relationship between change versus stability in their pre-pandemic (i.e., prior to March 2020) versus their pandemic (i.e., October 2020) work locations and mental distress varied across social locations (i.e., social identities and biographies within major social structures, Moen 2022), such as gender and caregiving obligations. In other words, scholars have yet to decipher whether mental distress associated with work location during the pandemic was qualitatively different for workers with stable versus shifting work locations, nor whether mental health outcomes associated with stress caused by a disrupted work location are shaped by social-locational markers (like gender and caregiving obligations) (Moen 2022).
Our Contribution
While existing research has explored the negative mental health consequences of WFH during COVID-19 (Bolisani et al. 2020; Chambel et al. 2022; Kim et al. 2023; Lizana and Vega-Fernadez 2021; Möhring et al. 2021; Sahni 2020), research evaluating whether having a change in work locations before versus during the pandemic relates to mental distress is underdeveloped. Accordingly, we adopt a Stress Process Model framework (Pearlin 1989, 2010) to empirically test Moen’s (2022)“Uneven Stress of Social Change” theoretical model on how structural shifts in work contexts are associated with mental distress. Further, we respond to Moen (2022) suggestion that scholars explore inequalities in the stress process by incorporating an intersectional approach and examining whether this relationship varies across individuals’ social-locational markers. Using nationally representative data from the Pew Research Center’s American Trends Panel (ATP) survey, we thus examine the relationship between work location and mental distress (comparing workers who shifted to WFH versus had stable work locations prior to and during the pandemic) and further investigate whether this association differs by two social locations (gender and caregiving obligations).
Literature Review and Conceptual Framework
Change and Stability in Work Location and Mental Health
The “stress process” and “uneven stress of social change” models
According to Pearlin’s (1989, 2010) “Stress Process Model,” macro-level social institutions directly impact individuals’ mental health via a heightened vulnerability and exposure to stressors. That said, as Moen (2022) aptly delineates when she adapts Pearlin’s framework into the “Uneven Stress of Social Change” model, social structures are neither static nor constant. Thus, when these structures (such as the workplace) are subject to widespread shifts, we expect levels of mental distress to be affected. When applying these concepts to Moen’s (2022) conceptual model (p. 86), the pandemic’s enforced TWFH is emblematic of “changing institutional structures” where “external shocks” (such as lockdown-related “public policies”) rapidly disrupted and dislocated the work locations of a substantial proportion of the U.S. labor force. This time of widespread interruption to workplaces likely challenged the adaptive capabilities of individuals (Pearlin 1989, 2010). Moreover, because these shifts were not voluntary, they match Pearlin’s (1989) assertion that “undesired, unscheduled, and uncontrolled” (p. 244) changes are especially harmful to individuals’ mental health. In other words, abrupt transitions in one’s work environment likely led workers to have more stress exposure (via greater role transitions, more role overload, higher levels of work-family conflict, and/or experiencing more strains on resources), and thus, to report greater mental distress.
In the present study, we directly test Moen’s (2022) conceptual model with empirical data to evaluate whether there is a relationship between change in one’s work location during the pandemic and mental distress. Pandemic-era research has shown mixed results related to the impacts of a TWFH. Some studies found negative consequences, such as increases in work demands and hours (Lizana and Vega-Fernadez 2021), greater anxiety symptoms and sleep disturbances (Kim et al. 2023), heightened feelings of social isolation (Bolisani et al. 2020), and struggles associated with frequent interruptions (Sahni 2020). Another line of research revealed that WFH during the pandemic had some benefits, such as saving transportation time (Bolisani et al. 2020), improving productivity (Guler et al. 2021), and increasing family closeness (Adisa et al. 2021). However, like pre-pandemic research, the bulk of these studies conceive of WFH as static, in the sense that they did not account for one’s work location prior to the pandemic to assess whether individuals actually experienced change or stability. The exception is two studies that used longitudinal data, finding that a shift to telework had no relationship with work-family balance, burnout, or family/life satisfaction (Chambel et al. 2022; Möhring et al. 2021). However, due to their small sample sizes and a lack of control groups (e.g., they did not compare the TWFH group to those who did not change their work location during the pandemic), it is difficult to draw a firm link between a TWFH and mental distress based on these two studies alone.
Given these mixed findings and gaps in previous research, we adopt the Stress Process Model, as extended in Moen’s (2022) conceptual framework, to test whether workplace dislocation during the pandemic affected workers’ mental distress by comparing individuals who changed work locations (i.e., TWFH) with those who had more stability in their work locations: workers who consistently WFH or consistently worked on-site (during both the pre-pandemic and the pandemic periods). Specifically, workers who WFH prior to the pandemic were likely more prepared and accustomed to telework, so their mental distress was less likely to be influenced by work location during the pandemic. For these individuals, WFH also likely constituted voluntary workplace flexibility rather than involuntary WFH (Kaduk et al. 2019). Accordingly, existing research that failed to differentiate between these distinctive groups (see, e.g., Adisa et al. 2021; Guler et al. 2021; Kim et al. 2023; Lizana and Vega-Fernadez 2021) may underestimate the association between WFH during COVID-19 and mental distress. Therefore, we propose the following hypothesis:
Intersectional contexts and identities—The role of gender and caregiving
Returning to Moen’s (2022) expansion of Pearlin’s (1989, 2010) model, we also recognize that the link between social structural changes and stress is not uniform, but rather occurs in an uneven fashion. As Moen (2002:88) states, “Social changes interrupt life paths and produce stressful circumstances at particular time points in biographies already defined, shaped, and constrained at the intersections of race, class, nativity, age, and gender.” In other words, when people experience macro-level social changes (such as pandemic-era disruptions to major social institutions like the workplace), their exposures to stressors and their stress responses are not universal. Instead, they vary widely and unequally depending on individuals’“social locations” within social structures (such as their gender and caregiving obligations). Thus, we answer Moen’s (2022) call for scholars to adopt an “intersectional approach” (Choo and Marx-Ferree 2010; P. H. Collins and Bilge 2020; McLeod 2015; Romero 2018; Scheid and Brown 2010) when examining the link between social change and stress outcomes by examining the moderating roles of gender and caregiving obligations. Through this lens, we pay special attention to how pre-existing inequalities (such as differences in men’s and women’s childcare contributions) can intensify mental distress when structural changes intersect with social-locational markers (Moen 2022).
The social location of gender
We examine how change versus stability in work location during the pandemic influences men’s and women’s mental distress separately, as we assume that key factors like roles and resource allocations, as well as socialization processes, are stratified by gender. It is well documented that there were gendered patterns in paid and unpaid labor prior to the pandemic. For example, while U.S. women’s participation in the labor force rose steadily from 1948 to 2000, and has declined slightly since then (Machovec 2023), women have reduced their participation in housework (Bianchi et al. 2012), yet mothers still spend more time with children today than in the past (Bianchi, Robinson, and Milkie 2006). Fathers also complete more housework and childcare, on average, than in the past. Still, a gap between mothers and fathers remains, such that the division of household labor is still gendered, with women taking greater responsibilities for managing domestic and childcare tasks, activities, and events (Bianchi et al. 2006; Bianchi et al. 2012; Daly 2002; Gornick and Meyers 2003; Nomaguchi and Johnson 2009; Sayer 2005). This is often attributed to traditional gender role expectations taught via socialization and reinforced in both the family and work domains through social roles (i.e., the male breadwinner-female homemaker ideology) and resource allocations (e.g., the gender wage gap; public policies on family leave). In terms of gendered patterns in work, literature suggests that women are more likely to value flexible work options like WFH and are more apt to use them to manage family demands (Daly 2002; Gornick and Meyers 2003), while men tend to utilize WFH for work-related reasons, such as to demonstrate commitment (Hill et al. 2008; Hofäcker and König 2013; C. Sullivan and Lewis 2001). Because WFH allows women to increase their involvement in domestic and childcare tasks (Powell and Craig 2015), women who WFH may experience elevated work-family conflict due to blurred work-family boundaries Kim, Henly, Golden, and Lambert 2020. Therefore, TWFH during the pandemic likely perpetuated gender inequality and traditional gender roles.
The temporary closure of in-person schools and businesses following the onset of the pandemic further complicated women’s roles in the work and family domains, which also had a direct effect on their mental health. Increased domestic and childcare demands disproportionately fell on women’s shoulders, resulting in greater job losses, reduced hours of paid labor, more reports of work-family conflict, and worse mental health for women (especially mothers) than for men (Calarco et al. 2020; Carlson, Petts, and Pepin 2022; Carlson and Petts 2022; C. Collins et al. 2020; Zamarro and Prados 2021). Based on both past and current literature, we thus expect that:
The social location of caregiving obligations
In light of Moen’s (2022) intersectional approach, caregiving obligations might also moderate the relationship between change versus stability in work location during the pandemic and mental distress. Several studies have explored how WFH during the pandemic influenced the gendered division of unpaid labor (Carlson and Petts 2022; Chung et al. 2022; Dunatchik et al. 2021; Lyttelton, Zang, and Musick 2022), finding that although men’s engagement in housework and childcare increased marginally during the earliest months of the pandemic, they receded soon after, such that women who WFH still bore a greater share of these responsibilities. When looking at childcare obligations specifically, by Fall 2020, fathers’ contributions to childcare in households were slightly higher than pre-pandemic levels, but the gendered gap in caregiving remained (Carlson and Petts 2022). Still, recent research on how TWFH during the pandemic relates to caregivers’ stress has produced mixed results. Using German survey data, Möhring et al. (2021) found no differences in job or family satisfaction when examining men versus women and mothers versus fathers who TWFH during the pandemic. In contrast, Bernstein et al. (2020) found a reduction in stress among U.S. professional workers who TWFH, except among those with childcare obligations. This is similar to Fan and Moen’s (2023) finding that the benefits of continued remote work during the pandemic were diminished among both men and women with caregiving obligations. Other studies have found distinctly gendered differences among caregivers who TWFH. Qualitative research on Turkish married mothers of children under 18 years of age documented difficulties associated with these women’s TWFH (Çoban 2022). Using 2020 data from the Pew Research Center, Igielnick (2021) also reported that workers with children under 18 years of age at home were more likely to have difficulties getting their work done, with mothers reporting more difficulties than fathers. Thus, increased family demands and an enforced TWFH during the pandemic likely intensified gender inequality in caregiving and caused further damage to women’s mental distress. Therefore, we propose the following hypothesis:
Methods
Data and Sample
We use data from the Pew Research Center’s ATP survey. The ATP is a nationally representative online survey of randomly selected U.S. adults. The current study pools data from two panel waves (wave 64, conducted between March 19 and 24, 2020, and wave 77, conducted between October 13 and 19, 2020). Out of the 8,311 individuals surveyed, 1 we exclude those below the age of 18 years and above the age of 64 years (N = 2,365). We then drop those who are self-employed (N = 397), those who are not working either part- or full-time (N = 1,565), those with more than one job or who consider more than one job to be their main job (N = 104), 2 and those who were not employed prior to COVID-19 (N = 89). This leaves us with a sample of 3,791 adults. We further drop 130 individuals who worked from home before the pandemic and then worked on-site during the pandemic 3 and 344 individuals who were missing values for one or more of the variables we use in the analyses. This leaves us with a final sample of 3,447 adults. All the variables are measured from wave 77, except for the indicator on whether the respondent was diagnosed with any mental health condition prior to the pandemic, which was asked in wave 64.
Dependent Variable
Mental distress is our dependent variable, which we measure using a scale adapted from prior research (Holingue et al. 2020). Two items on loneliness and optimism about life are adapted from the Center for Epidemiologic Studies Depression (CES-D) Scale (Radloff 1977), and one item on stress is adapted from the Generalized Anxiety Disorder-7 (GAD-7) (Spitzer et al. 2006). Respondents are asked the following three questions: “This first question is about how you feel about different aspects of your life these days.”“How often, if ever, do you feel: (1) lonely or isolated from those around you; (2) optimistic about your life; and (3) stressed or anxious.” Each item ranges from 1 (all or most of the time) to 4 (never). The first and the third items are reverse coded. We first sum and then average these three items into a scale to measure mental distress. Higher numbers on the scale indicate higher levels of mental distress. The Cronbach’s alpha for the whole sample is 0.71 (0.70 for men and 0.71 for women), which indicates adequate internal reliability.
Independent Variables
Our main independent variable is change and stability in work location during the pandemic. This item is measured by combining the following two questions: (A) “Are you currently working from home?” (1) = All of the time, (2) = Most of the time, (3) = Some of the time, (4) = Rarely, (5) = Never; and (B) “Before the coronavirus outbreak, did you work from home?” (1) = All of the time, (2) = Most of the time, (3) = Some of the time, (4) = Rarely, (5) = Never. In both cases, WFH is converted to a dummy variable (1 = Yes, 0 = No) where “1” is coded as those who respond with “all of the time, most of the time, or some of the time” and “0” is coded as those who respond with “rarely or never.” 4 To compare the responses pre-pandemic (i.e., prior to March 2020) and during the pandemic (i.e., October 2020), we created a categorical variable to represent change and stability in work location during the pandemic with three categories: (1) TWFH (i.e., worked on-site before the pandemic and WFH during the pandemic) (reference), (2) consistently WFH (i.e., WFH both before the pandemic and during the pandemic), and (3) consistently worked on-site (i.e., worked on-site both before the pandemic and during the pandemic). 5
Moderating Variables
Prior research suggests that men and women use and value flexible work arrangements differently (Kim et al. 2020) and that the effects of flexible work arrangements (such as WFH) differ between men and women (Yucel and Fan 2023). Given these expected gender differences, we first stratify our sample by gender (see Analytical Strategy section). Next, we use two moderators to measure caregiving obligations: the presence of preschool-aged children and the presence of school-aged children. The presence of preschool-aged children is a dummy variable (1 = Yes, 0 = No) for those who are a guardian or parent of any children who are of preschool age or younger and live in the household. The presence of a school-aged child is also a dummy variable (1 = Yes, 0 = No) for those who are a guardian or parent of any children in elementary, middle, or high school and live in the household.
Control Variables
Following prior research (Chambel et al. 2022; Długosz 2021; Holingue et al. 2020; Kim et al. 2023), we control for the following variables that are related to either a TWFH and/or mental distress: age, income, race, education, marital status, partners’ employment status, respondent’s employment status, region, having any childcare responsibilities while WFH, industry, whether an individual changed jobs during the pandemic, and having any diagnosed mental health condition prior to the pandemic. Age is a categorical variable: 18–29 (reference), 30–49, and 50–64. Consistent with prior research (Holingue et al. 2020), we use income as a categorical variable: lower income (income less than $40,000) (reference), middle income (income between $40,000 and less than $100,000), and upper income (income $100,000 and higher). Race is a categorical variable: White (reference), Black, Hispanic, and other. Education level is a categorical variable: 1 = high school graduate or less (reference), 2 = some college, 3 = college graduate or more. Marital status is a dummy variable (1 = married/cohabiting, 0 = no). Partner’s employment status is a dummy variable (1 = having an employed partner in the household, 0 = no). Employment status is a dummy variable: 1 = full-time, 0 = part-time. Region of the country is a categorical variable: Midwest, South, West, and Northeast (reference). Childcare responsibilities while WFH is a dummy variable (1 = those who WFH at least some of the time and have some or a lot of child care responsibilities while WFH, 0 = no). Industry is a categorical variable: primary/secondary, tertiary (reference), and quaternary. This is coded based on prior research (Kenessey 1987), where primary industries extract natural resources (such as forestry, agriculture, etc.), secondary industries are responsible for the manufacturing and production of finished products (such as manufacturing, mining, or construction), tertiary industries include the service industries (such as hospitality, health care industries, and retail), and quaternary industries are based on new technologies and require more education (such as information and technology industries). We add a dummy variable to indicate whether the respondent changed jobs since the COVID-19 outbreak (1 = yes, 0 = no). Finally, we control for any diagnosed mental health condition prior to pandemic to adjust for any pre-existing differences in the mental health conditions of workers. We use a dummy variable to indicate whether any doctor or health care provider ever told the respondent that they have a mental health condition (1 = yes, 0 = no) before March 2020.
Analytical Strategy
Table 1 presents the descriptive findings for all variables used in our analysis. We ran a chi-square test (for categorical variables) and t-test (for continuous variables) to show whether these variables statistically differ between men and women. The outcome variable, mental distress, is a continuous variable. Thus, the results are estimated by running a series of regression analyses. We use Stata 14.0 to estimate these models and use listwise deletion for addressing missing cases. 6 The analytical steps are as follows. First, in Table 2, we estimate the direct associations of change and stability in work location on mental distress for the full sample (Model 1). We then add an interaction term by gender to show whether these direct associations differ between men and women (Model 2). Next, we stratify the sample by gender, where we present models for women (Table 3) and men (Table 4) separately. We show the direct associations in Model 1 (for both Tables 3 and 4). We then add an interaction term by the two measures of caregiving obligations (the presence of preschool-aged children [Model 2] and the presence of school-aged children [Model 3]) to determine whether the association between change and stability in work location and mental distress differs by these variables separately. In all analyses, we report the unstandardized coefficients.
Descriptive Statistics (N = 3,447).
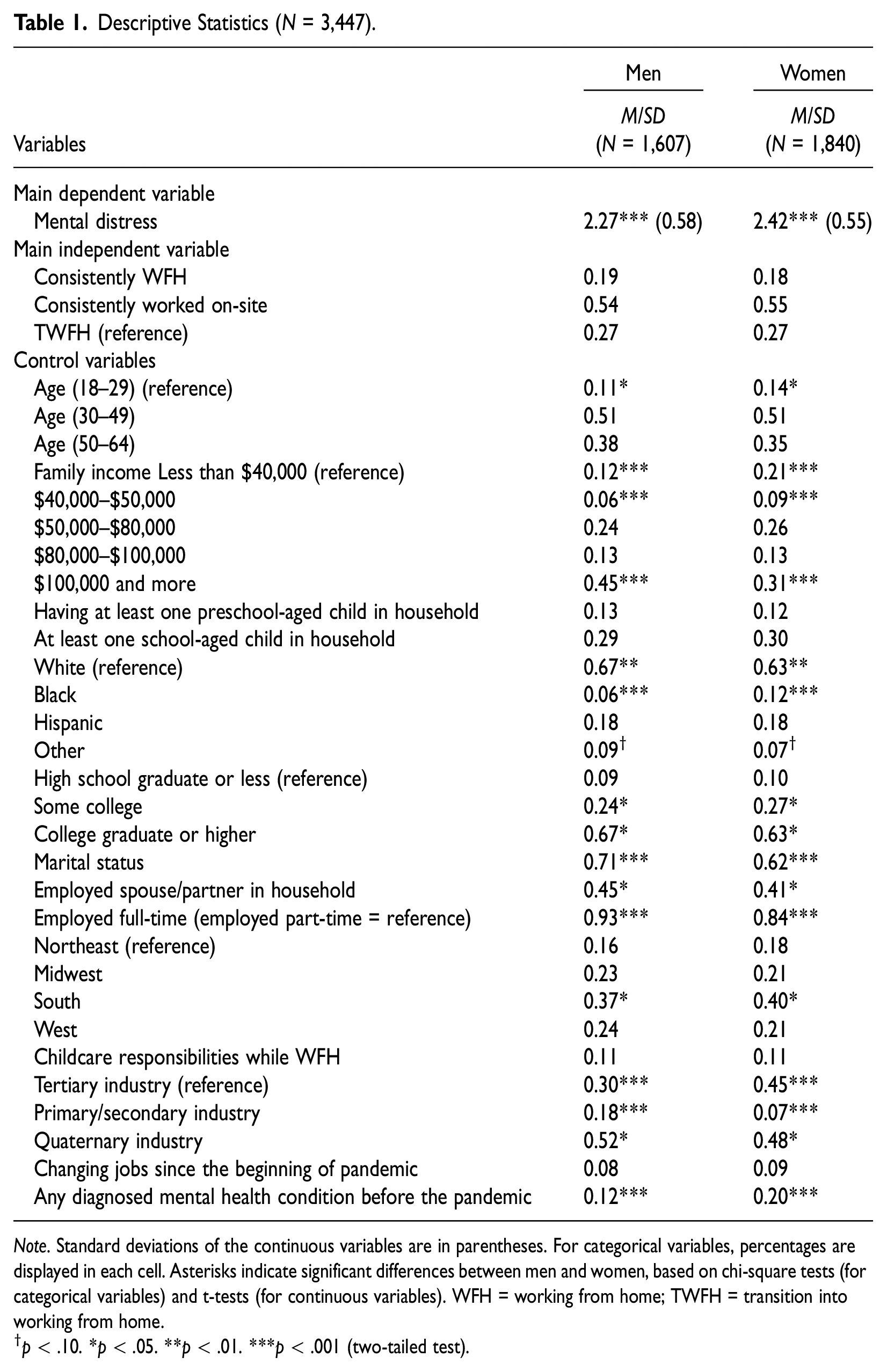
Note. Standard deviations of the continuous variables are in parentheses. For categorical variables, percentages are displayed in each cell. Asterisks indicate significant differences between men and women, based on chi-square tests (for categorical variables) and t-tests (for continuous variables). WFH = working from home; TWFH = transition into working from home.
p < .10. *p < .05. **p < .01. ***p < .001 (two-tailed test).
Predicting Mental Distress for the Full Sample.
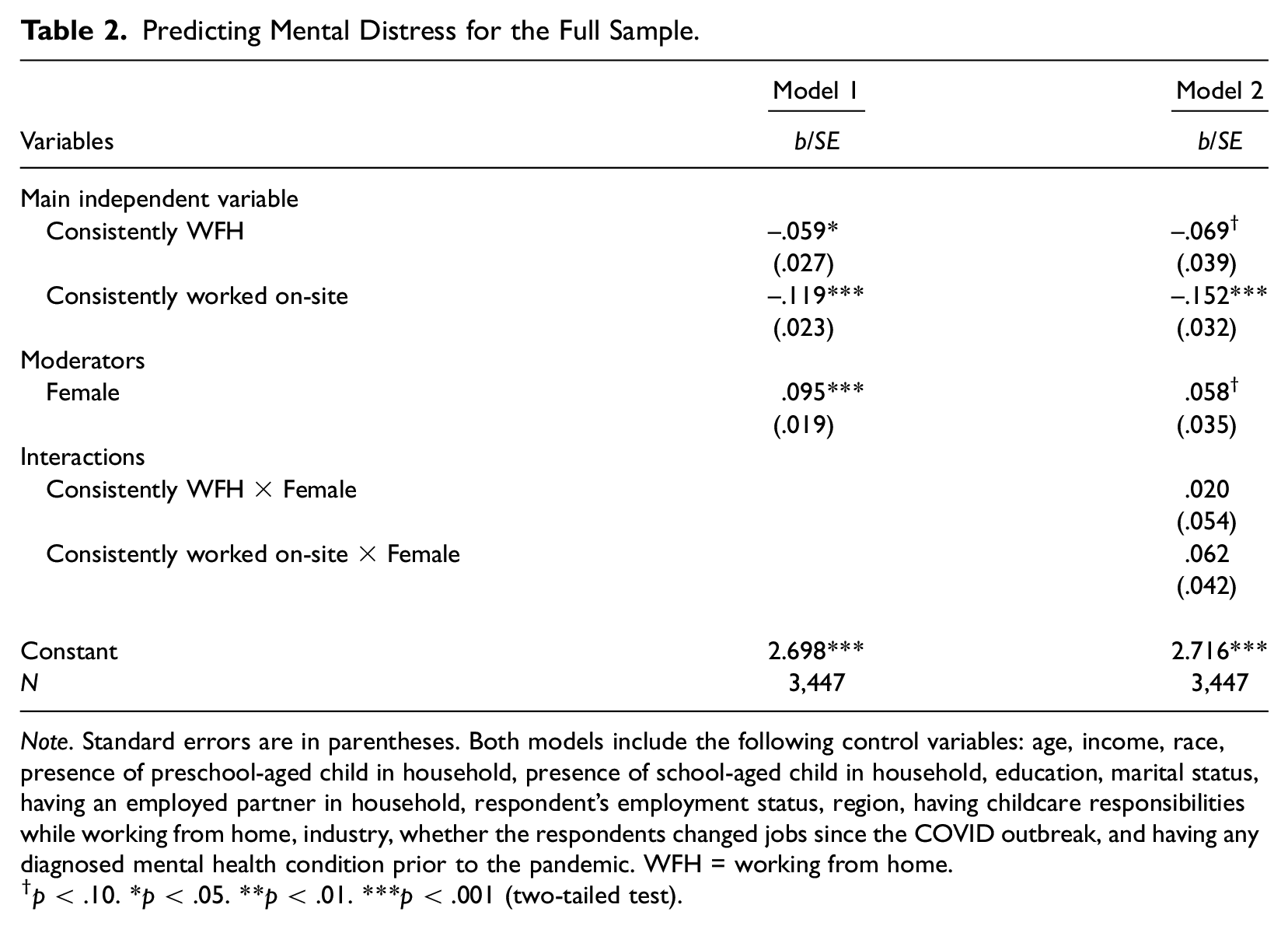
Note. Standard errors are in parentheses. Both models include the following control variables: age, income, race, presence of preschool-aged child in household, presence of school-aged child in household, education, marital status, having an employed partner in household, respondent’s employment status, region, having childcare responsibilities while working from home, industry, whether the respondents changed jobs since the COVID outbreak, and having any diagnosed mental health condition prior to the pandemic. WFH = working from home.
p < .10. *p < .05. **p < .01. ***p < .001 (two-tailed test).
Predicting Mental Distress Among Women.
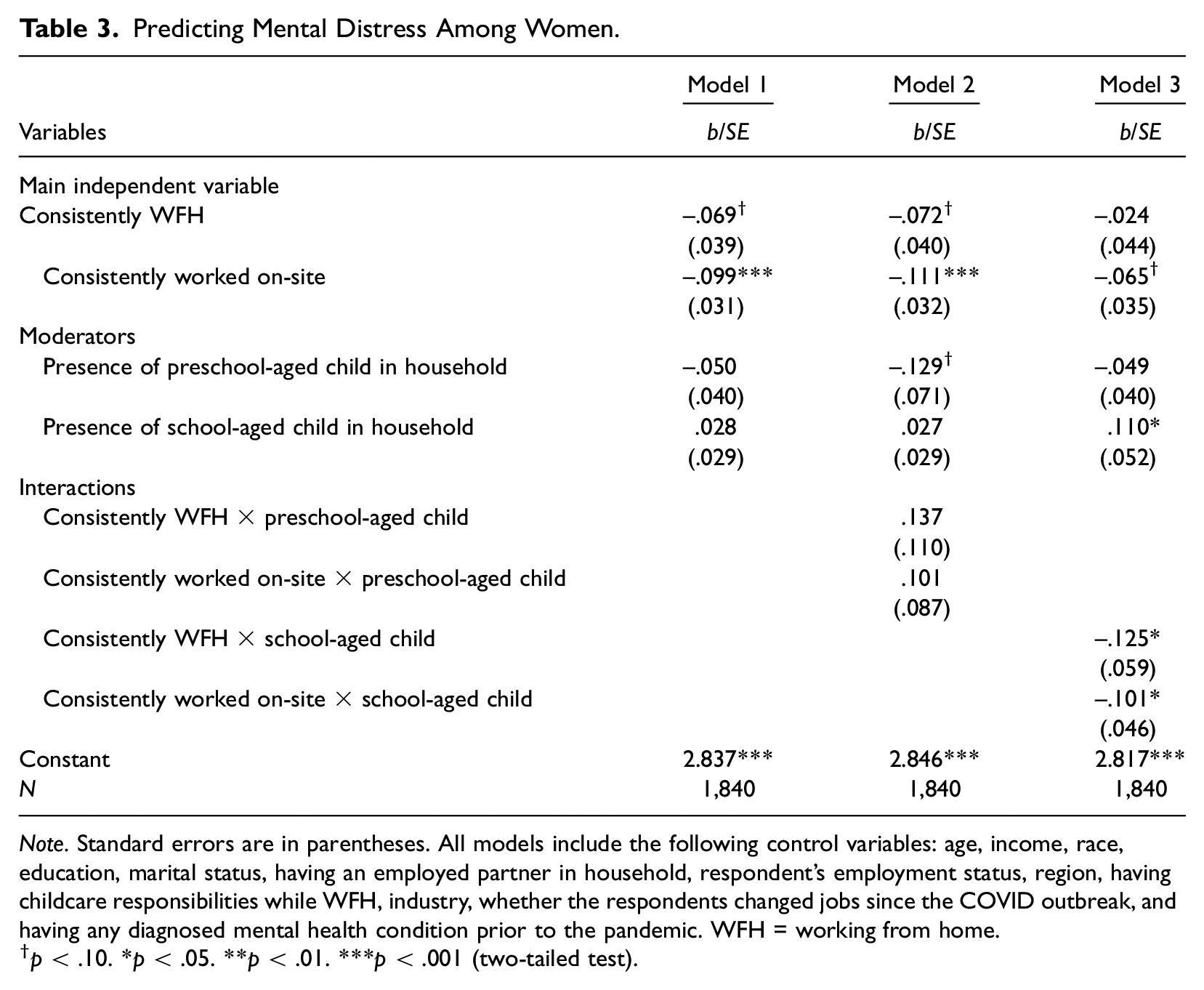
Note. Standard errors are in parentheses. All models include the following control variables: age, income, race, education, marital status, having an employed partner in household, respondent’s employment status, region, having childcare responsibilities while WFH, industry, whether the respondents changed jobs since the COVID outbreak, and having any diagnosed mental health condition prior to the pandemic. WFH = working from home.
p < .10. *p < .05. **p < .01. ***p < .001 (two-tailed test).
Predicting Mental Distress among Men.
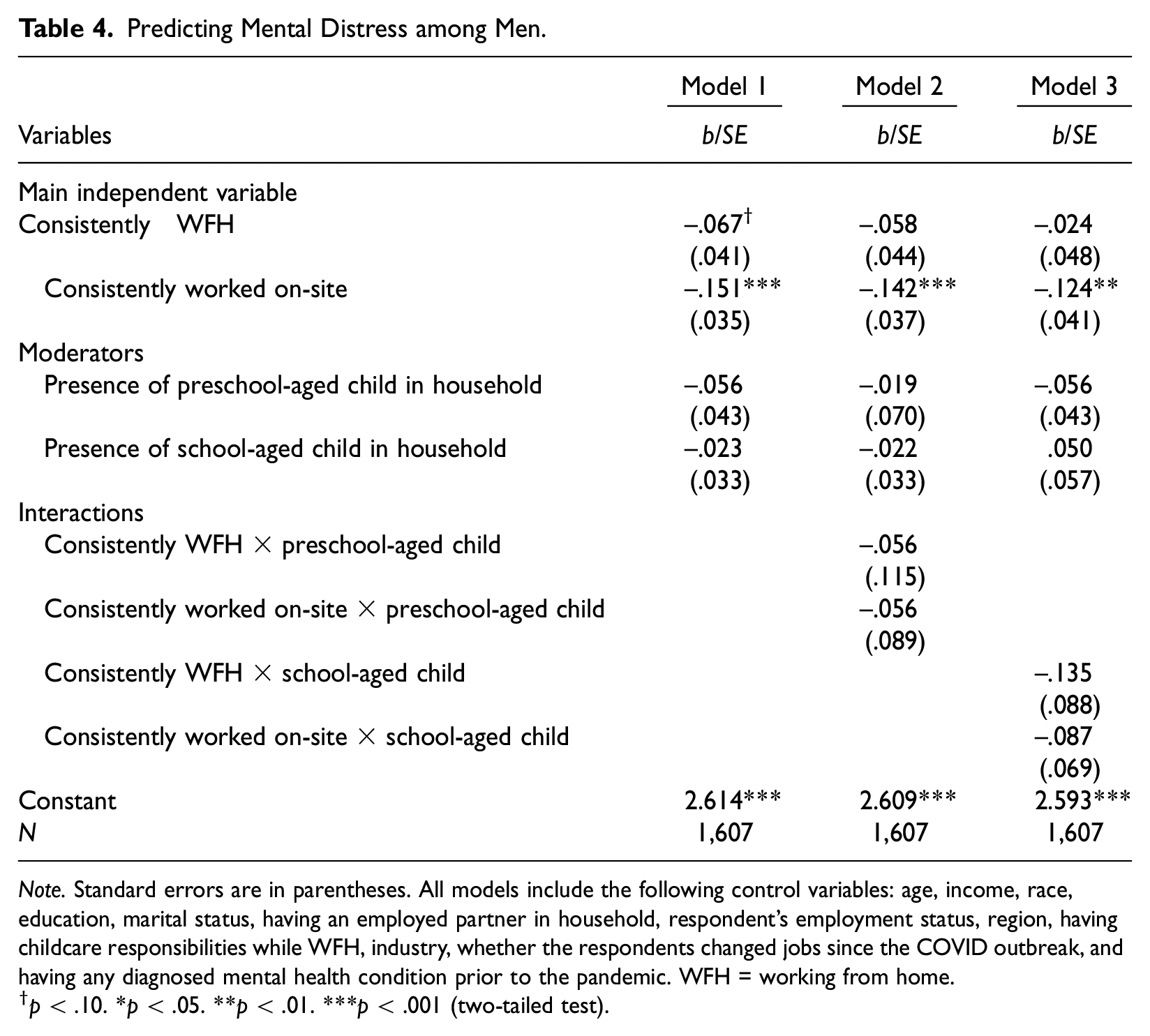
Note. Standard errors are in parentheses. All models include the following control variables: age, income, race, education, marital status, having an employed partner in household, respondent’s employment status, region, having childcare responsibilities while WFH, industry, whether the respondents changed jobs since the COVID outbreak, and having any diagnosed mental health condition prior to the pandemic. WFH = working from home.
p < .10. *p < .05. **p < .01. ***p < .001 (two-tailed test).
Results
Descriptive Findings
On average, women report higher levels of mental distress than men (2.42 for women versus 2.27 for men) (p < .001). There are no gender differences in the categories for change and stability in work location. Women are younger than men (14 percent of women are 18–29 years old versus 11 percent for men) (p < .05). There is a gender gap in income, where more men (45 percent) have a higher income level (i.e., $ 100,000 or more) than women (31 percent) (p < .001). Men are more educated than women (67 percent have a college degree or more versus 63 percent, respectively) (p < .05). More men report either being married or cohabiting than women (71 percent for men versus 62 percent for women) (p < .001). More men have partners who are employed (45 percent for men versus 41 percent for women) (p < .05). More men are employed full-time than are women (93 percent versus 84 percent, respectively) (p < .001). More men are in either the primary/secondary or quaternary industries (18 percent and 52 percent, respectively) than women (7 percent and 48 percent, respectively), whereas more women are in the tertiary industry (45 percent) than men (30 percent). Finally, more women were diagnosed with a mental health condition prior to the pandemic than men (20 percent for women versus 12 percent for men) (p < .001).
In supplemental descriptive statistics (available upon request), we tested whether the variables we use in our analyses differ across the three categories of our main independent variable. Results show that those who TWFH during the pandemic report higher levels of mental distress than those who consistently WFH and those who consistently worked on-site before and during the pandemic. Those who TWFH during the pandemic are also more likely to have a preschool-aged child in the household than those who consistently worked on-site before and during COVID-19. 7
Main Associations and Interaction by Gender
Table 2 shows the direct associations of change and stability in work location on mental distress for the full sample (Model 1) and whether these direct associations vary by gender (Model 2). As shown in Table 2, Model 1, those who consistently WFH before and during the pandemic report lower levels of mental distress than those who TWFH during the pandemic (b = −0.059, SE = 0.027, p < .05). Those who consistently worked on-site before and during the pandemic also report lower levels of mental distress than those who TWFH during the pandemic (b = −0.119, SE = 0.023, p < .001). This finding supports Hypothesis 1. Model 2 shows that the associations between change and stability in work location and mental distress do not vary between men and women, indicating that Hypothesis 2 is not supported. See the Supplemental Appendix, Table A1, for full models with the control variables.
Main Associations and Interaction by Caregiving Obligations and Gender
Tables 3 and 4 show the direct associations, as well as the interaction terms, when predicting mental distress among women and men, respectively (see the Supplemental Appendices, Tables A2 and A3, for full models with the control variables). As shown in Model 1 (Table 3), women who consistently WFH before and during the pandemic report lower levels of mental distress than women who TWFH during the pandemic (b = −0.069, SE = 0.039, p < .10). Women who consistently worked on-site before and during the pandemic also report lower levels of mental distress than women who TWFH during the pandemic (b = −0.099, SE = 0.031, p < .001). Similarly, according to Model 1 (Table 4), men who consistently WFH before and during the pandemic report lower levels of mental distress than men who TWFH during the pandemic (b = −0.067, SE = 0.041, p < .10). Men who consistently worked on-site before and during the pandemic also report lower levels of mental distress than men who TWFH during the pandemic (b = −0.151, SE = 0.035, p < .001).
Turning to the interaction effects by caregiving obligations, Model 2 (in Tables 3 and 4) shows that the presence of a preschool-aged child does not moderate the association between change and stability in work location and mental distress for women or men. Model 3 (in Table 3) shows that women who either consistently WFH or consistently worked on-site before and during the pandemic report lower levels of mental distress than women who TWFH during the pandemic, especially when there is a school-aged child in the household (p < .05 and p < .05, respectively). Thus, Hypothesis 3 is partially supported. On the other hand, Model 3 (in Table 4) shows that presence of a school-aged child does not moderate the main associations among men. Figure 1 displays the bar graph for the significant moderation for women. This figure shows that only among women with school-aged children, those who consistently WFH or consistently worked on-site before and during the pandemic report lower levels of mental distress than women who TWFH during the pandemic. 8
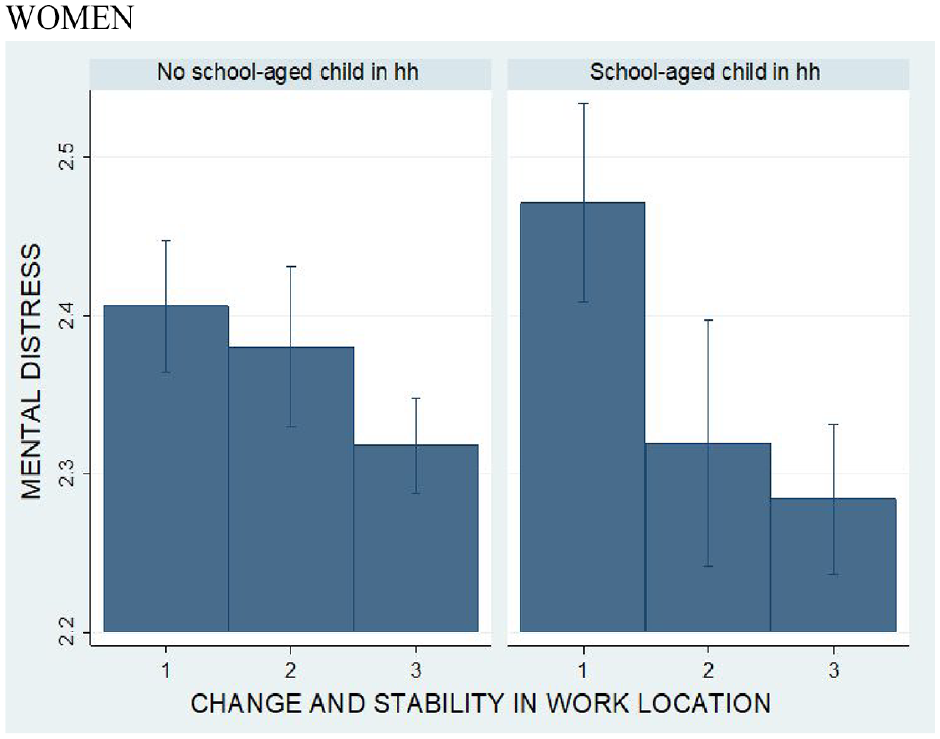
The effect of change and stability in work location on mental distress among women by presence of a school-aged child in the household.
Discussion
Emerging pandemic research has examined how WFH influences work-family balance and well-being (Bolisani et al. 2020; Chambel et al. 2022; Kim et al. 2023; Lizana and Vega-Fernadez 2021; Möhring et al. 2021; Sahni 2020). However, research focusing on change versus stability in work location (comparing the pre-pandemic and pandemic eras) and their association with mental distress is limited. To fill this gap, this article uses Pearlin’s (1989, 2010) Stress Process Model and Moen’s (2022) Uneven Stress of Social Change frameworks to examine whether a structural change in work location (e.g., a TWFH) during the pandemic was associated with mental distress. Furthermore, we answer Moen’s (2022) call to assess inequalities in the stress process by applying an intersectional lens to evaluate whether this association varied across two social-locational markers (e.g., gender and caregiving obligations). Results suggest that for both men and women, those who consistently WFH and those who consistently worked on-site (before and during the pandemic) report lower levels of mental distress than those who TWFH during the pandemic. Moreover, this difference in mental distress by work location is larger among women with a school-aged child.
The finding that TWFH was more strongly related to individuals’ mental distress supports previous literature documenting a decline in mental health among those who WFH during COVID-19 (Kim et al. 2023; Lizana and Vega-Fernadez 2021; Sahni 2020). However, such studies did not account for workers’ pre-pandemic work location. Thus, our study contributes to the literature by empirically testing Moen’s (2022) theoretical model and demonstrating that those who changed work locations (from working on-site before the pandemic to WFH during the pandemic) display more mental distress than those who had stable work locations (even if this meant consistently WFH before and during the pandemic). This main finding also matches the predictions of Pearlin’s (1989, 2010) Stress Process Model, which proposes that the ways in which we experience a stress response appear to be uniquely shaped by historical forces (such as pandemics), our social locations within social structures (such as workplaces), and our unequal access to resources needed to adapt and cope with stressors. In line with this framework, we find evidence that some groups (those who had stability in their work location) appear to fare better than others (those who changed work locations). These findings can also be more deeply interpreted through the lens of Moen’s (2022)“Uneven Stress of Social Change” model (p. 85), which explains that COVID-19 fostered in a number of “rapid change[s]” and “social disruptions and dislocations” (including a compulsory, unanticipated, and abrupt shift in work location) that prompted individuals across diverse social statuses and locations to experience “uneven stresses” that transpired in “disparate ways.” As Moen (2022) notes (p. 91), COVID-19 “accentuated ongoing changes in the nature of work,” and as shown here, the stressors experienced and their shaping of mental health were not universal. Instead, it appears that individuals who had more stable work locations experienced less mental distress than those for whom work locations transitioned.
This positive association between a change in work location during the pandemic and mental distress operated similarly across genders. While unexpected, this could be attributed to a number of factors. First, the lack of significant gender differences in this relationship parallels the findings of several other pandemic-era studies. Using data on Canadian workers, Schieman et al. (2021) found no gender differences in work-life conflict patterns throughout the earliest months of the pandemic. Similarly, Montazer et al.’s (2022) study of U.S. adults in dual-earning partnerships (using data collected at the onset and several months into the pandemic) documented an increase in psychological distress among parents (compared to non-parents), regardless of their gender. This is perhaps indicative of TWFH during COVID-19 being comparably taxing for men and women, even if the mediating mechanisms (e.g., possibly social isolation from coworkers for men versus heightened household demands for women) explaining these links might vary by gender. Prior work has documented several mediating mechanisms that, if accounted for, might reveal important gender differences in mental distress related to the TWFH, such as gendered patterns in levels of work-family interference (Kaltiainen and Hakanen 2023; Kim et al. 2020), job autonomy (Gajendran and Harrison 2007), opportunities for promotion (Bloom et al. 2015), and/or the availability of work space (Buomprisco et al. 2021). 9 Unfortunately, we cannot explore these possibilities given limitations of our data. Second, other scholars have noted that the pandemic fostered some movement toward egalitarianism among dual-earning couples during the first months of the pandemic, as some men did more housework and childcare and some women reduced their work hours (C. Collins et al. 2020; Shockley et al. 2021). While a recent study by Carlson and Petts (2022) finds that by November 2020, fathers’ participation in housework and childcare (on average) had already decreased to near pre-pandemic levels, it also documented that among a subset of the sample (fathers who still worked from home and had older school-aged children receiving remote schooling), men’s childcare contributions remained as high in Fall 2020 as they were in the earliest months of the pandemic. Considering that our data were also collected in Fall 2020, these combined factors could have plausibly canceled out some of the gender differences we expected in mental distress by potentially heightening some men’s mental distress (due to having greater childcare obligations while TWFH) and potentially lowering some women’s mental distress (due to having fewer paid work hours while TWFH). While we are unable to account for these possibilities due to data limitations, we encourage future research to explore them or conduct qualitative research to examine these dynamics with greater nuance.
We do, however, find evidence of Moen’s (2022) theoretical prediction that the relationship between structural changes and stress-related outcomes will vary across intersecting social locations (such as gender and caregiving obligations). While we expected that women with both preschool-aged and school-aged children would show distinctly higher levels of mental distress if they TWFH, this association was only greater among women with school-aged children (than among those without) who TWFH. This finding aligns with recent studies that have shown mixed results when it comes to the role the age of the youngest child in the household played during the pandemic, with some finding a reduced levels of work-family conflict among parents with teenage children (Schieman et al. 2021), and others finding no effect of the age of children on parents’ psychological distress (Montazer et al. 2022). Likewise, Fan and Moen (2023) found fewer benefits of longer-term remote work during the pandemic for both men and women with any caregiving obligations and some benefits (in terms of job and life satisfaction) of a return to work for women with care responsibilities, regardless of the child’s age. That said, at the time of our survey, 48 percent of workers in our sample who TWFH and had a preschool-aged child were using a daycare/preschool regularly, while only 17 percent of workers who TWFH and had a school-aged child had full access to in-person K-12 instruction. This suggests that women in our study with preschool-aged children were potentially relieved of some of their care burden (perhaps explaining the null finding among this group). In contrast, women with school-aged children who TWFH likely took on a greater burden of caring and meeting the educational needs of older, school-aged children while simultaneously shifting their work location, potentially resulting in greater mental distress. Moreover, there are relatively small numbers of workers in our sample who consistently WFH and have a preschool-aged child living in the household (around 2 percent of women and men, respectively), which might also contribute to why we found no significant interaction effects for the presence of a preschool-aged child.
In addition, pandemic literature suggests that the challenges associated with taking care of children during the pandemic may be particularly severe for parents of school-aged offspring. For example, Braga and Parker (2022) found that about six in 10 K-12 parents reported that the pandemic had a negative effect on their children’s education, while about half of parents reported that their school-aged children’s emotional well-being suffered. Other studies have documented a wide-range of additional negative effects of the pandemic on school-aged children/families, including financial hardship, a loss of school meals and services, disrupted routines/schedules, heightened anxiety and loneliness, learning loss, and poorer emotional regulation (see, e.g., Centers for Disease Control and Prevention 2022; Chabaane et al. 2021; Chen, Byrne, and Velez 2022). Verlenden et al. (2021) directly connects the mental health risks experienced by school-aged children and their parents to prolonged amounts of virtual schooling. Given these heightened demands associated with having a school-aged child during the pandemic, as well as the large percentage of school-aged children in our sample still receiving remote schooling when our data were collected in October 2020, women who TWFH might have experienced greater caregiving challenges (while simultaneously managing their dislocated work location) than women without a school-aged child.
Despite these contributions, our study also has some limitations. First, the cross-sectional nature of the data makes it impossible to test causal relationships. Therefore, it is important to note that our results show only correlations between a TWFH and mental distress. Relatedly, the results should be interpreted cautiously because while we include a measure of any prior diagnoses of a mental health condition, we do not have a direct measure of mental distress (using the same items as our dependent variable) prior to the pandemic. It is also possible that, among the consistently worked on-site group, some workers quickly transitioned to WFH and then returned to their original work arrangement, on-site (i.e., between March and October 2020). These workers might dilute differences between groups, such that our findings may overestimate the difference in mental distress between the TWFH and the consistently worked on-site groups. In addition, although these workers had a quick TWFH, they may experience similar levels of mental distress to workers who consistently worked on-site. If this is the case, our findings would be less influenced by these workers. It would be therefore useful for future research to explore the relationship between change and stability in work location and mental distress utilizing consistent measures and longitudinal data. In addition, despite the fact that the three items we used for mental distress were derived from validated and established measures, such as the CES-D (Radloff 1977) and GAD-7 (Spitzer et al. 2006), this scale is limited because it does not capture all the emotional states found in the Kessler 10 scale (Kessler et al. 2003), such as depressed mood, nervousness, and worthlessness. While our scale assesses these dimensions using two items (i.e., pessimism and stress/anxiety) and additionally captures one’s feeling of loneliness (which could be a particularly relevant dimension to examine during the pandemic), it would be useful for future research to explore this question using more comprehensive measures on mental distress. Moreover, each wave from the ATP has a web-based design from thousands of individuals. While this strategy allows us to reach a larger sample on a variety of topics, it restricts any detailed information that can be obtained about the sample (e.g., details on caregiving tasks performed throughout the day) (Holingue et al. 2020). 10 Lastly, it is important to note that our findings are only relevant to changes in work location through October 2020. Workers who TWFH may not experience the same struggles to adapt to a new work environment now that we are in a post-pandemic period, as many workers have already been exposed to and/or adjusted to the telework modality. Therefore, for future research exploring whether our findings still hold using more current, post-pandemic data are necessary.
Overall, we contribute by finding that a transition in work location during the pandemic is more strongly related to mental distress than is stability in work location. By identifying a link between a disruption in work location and mental distress, we respond to Moen’s (2022) call for a “stress of social change research agenda investigating deliberate shifts in the work environment and subsequent effects on human experience” (p. 90). Moreover, our findings might be used to inform workplace policies. For example, it is important that employers and supervisors be aware of these challenges and provide adequate support so workers can manage their new work environments at home. Supervisors might consider holding remote social gatherings to reduce the social isolation of workers or adjusting work hours and work demands so workers (particularly women) who TWFH can better accommodate work and family responsibilities. Given that the experiences of TWFH were associated with more distress among women with a school-aged child, TWFH might contribute to the continuation of gender inequalities in work and family environments. Therefore, employers might provide counseling services or outreach programs for these more vulnerable workers to explore ways to lighten their burdens.
Supplemental Material
sj-docx-1-smh-10.1177_21568693231200037 – Supplemental material for When Change and Stability in Work Location Matter for Psychological Distress: A Study of Workers Before and During the COVID-19 Pandemic
Supplemental material, sj-docx-1-smh-10.1177_21568693231200037 for When Change and Stability in Work Location Matter for Psychological Distress: A Study of Workers Before and During the COVID-19 Pandemic by Deniz Yucel, Beth A. Latshaw and Jaeseung Kim in Society and Mental Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.