
Abstract
This study evaluated a self-report survey assessing school professionals’ perceptions of school and community mental health supports and services. Based on responses from 560 school professionals, findings provide support for the measure’s internal structure and ability to distinguish low-poverty and high-poverty schools. Practitioners and researchers may consider using this survey to understand perceptions of the quality and availability of mental health services, informing the selection and adaptation of school-based mental health supports and services.
Of the 42 million children and adolescents in the United States, approximately 7.7 million are estimated to suffer some form of mental health disorder (Whitney & Peterson, 2019). Data from the 2016 National Survey of Children’s Health indicate that among children ages 3–7, 7.1% had anxiety problems, 7.4% had behavioral or conduct problems, and 3.1% had problems with depression (Centers for Disease Control and Prevention, 2016). For anxiety and depression, rates are considerably higher among children between the ages of 12 and 17, estimated to be 10.5% and 6.1%, respectively. Mental health challenges in childhood can interfere with healthy development; influence quality of life, well-being, and academic outcomes in childhood; and lead to difficulties in adulthood, including poor health outcomes, unemployment, and frequent contact with law enforcement agencies (Scott et al., 2016).
Despite the prevalence and implications of mental health difficulties in youth, children and adolescents with mental health disorders are unlikely to receive appropriate treatment and services (Merikangas et al., 2011). When children and adolescents do receive treatment, they are most likely to receive it in school settings (Costello et al., 2014). Thus, the demand on schools to monitor and address child and adolescent mental health problems is not surprising (Fazel et al., 2014). The National Alliance on Mental Illness (2020) advocates for public policy that prioritizes schools to serve as gatekeepers for mental health screenings and services, and calls for the delivery of school-based mental health services. Indeed, emerging research supports the cost-effectiveness of school-based emotional health screenings and the benefits of specific early childhood interventions (Hawkins et al., 2007; Kuo et al., 2009).
Within schools, school counselors are particularly well positioned to provide interventions that address student mental health needs and thereby meet the needs of youth unlikely to receive mental health care in other settings (Collins, 2014). School counselors are involved in supporting the academic and social/emotional needs of the student body through activities such as the provision of mental health screenings, short-term mental health counseling, universal prevention programming, and advocacy (American School Counselor Association [ASCA], n.d.). School counselors may also serve as liaisons between families, schools, and community agencies while supporting the mental health needs of students (ASCA, n.d.; Messina et al., 2015). Because school counselors may face hefty caseloads, as well as conflicts in their roles related to counseling duties and administrative tasks (Bardhoshi et al., 2014; Villarreal & Castro-Villarreal, 2016), collaborations between school counselors and outside mental health providers are critical for addressing the vast mental health concerns of students (Villareal & Castro Villareal, 2016).
Given the potential of schools to reach a diversity of students with mental health needs, coupled with the potential for school counselors to effectively deliver mental health interventions, researchers have also begun to emphasize the development and evaluation of school counselor-led mental health programming (Whiston et al., 2011). To date, school counselor-led programming that targets student mental health has been demonstrated to support positive academic and behavioral outcomes, including improvements in externalizing behaviors, test anxiety, school attendance, well-being, and feelings of school connectedness or belonging (Amatea et al., 2010; Dimmitt & Wilkerson, 2012; Webb et al., 2019). These promising outcomes underscore the potential for counselor-led, school-based interventions to address child and adolescent mental health.
The growth in research supporting the development and evaluation of school-based and counselor-led mental health interventions is encouraging. However, as researchers, administrators, and school-based practitioners such as school counselors select mental health screenings and applied interventions, it is critical that they recognize the variation in quality, availability, and support of both community and school mental health services. For example, low-income, rural communities are often limited by a lack of community behavioral and emotional service providers and school resources (Hodgkinson et al., 2017; Lavalley, 2018). Only an estimated 63% of U.S. counties have one or more mental health facilities providing outpatient treatment for youth, and less than half of rural counties have such facilities (Cummings et al., 2013). Factors such as economic diversity, ethnic and racial minoritization, and proximity to high-quality medical services play a significant role in the availability of mental health care (Alegria et al., 2010; Howell & McFeeters, 2008).
An understanding of the availability of mental health services and supports in schools and their surrounding communities is an important consideration for individuals across multiple roles. Such information could support researchers evaluating interventions; school leadership selecting mental health programming goals and initiatives; and school counselors developing mental health programming, providing individual and group interventions, and coordinating community services. Because school counselors are involved in both the provision of mental health care in school and the coordination of community referrals, their perspectives are particularly important for understanding the scope and range of services provided across settings. In this manner, school counselors bridge the mental health gap between schools and communities, developing an intricate understanding of both school- and community-level services. Therefore, the purpose of this study was to establish the psychometric properties of a new self-report survey, the School and Community Mental Health Services Questionnaire (SCMHSQ), designed to measure school counselors’ and other school support professionals’ perceptions of the quality and availability of school and community mental health services.
Theory and Research Guiding Instrument Development
A holistic understanding of the quality and availability of mental health services can be framed by an ecological systems framework. The SCMHSQ was designed according to ecological systems theory, which posits that multiple systems or levels of environmental influences transact to influence child development (Bronfenbrenner, 1996). Ecological systems theory centralizes the student ontosystem, or internal system, and spans out to include: the microsystem, or the most proximal environment to the student (e.g., family, community provider, and school); the mesosystem, or paths connecting the student’s microsystems (e.g., family and school interactions); the exosystem, or the larger systems such as government or media; the macrosystem, or cultural values, expectations, and laws; and the chronosystem, or dimensions of time.
Although all aspects of a student’s ecology are important for understanding student development, school counselors are well positioned to provide insights into the quality and availability of mental health supports and services within both the microsystem (e.g., in-school mental health supports, professional support for mental health in schools, community supports and services) and mesosystem (e.g., school relationships with families, hospitals, and mental health providers). Salient components of the school microsystem include school-based mental health services, which have been shown to have positive effects on child mental health problems, such as decreases in childhood internalizing and externalizing difficulties, substance abuse, and attention concerns (Sanchez et al., 2018), and increased access to mental health care (Bains & Diallo, 2016). Administrative support, which can be demonstrated through provision of professional development activities addressing mental health needs and support for the selection and implementation of mental health services, is another important facilitator of school-based mental health service success that is embedded in the school microsystem (Langley et al., 2010). A final important microsystem to consider involves mental health services located in the community (outside of school), which can support student well-being and academic success (Atkins et al., 2015).
Communication between families and schools, and networks between community providers and schools, are potential mesosystem facilitators for successful implementation of school-based mental health services (Langley et al., 2010; Orlando et al., 2018). Partnerships between schools and community health care providers are considered integral to effective school-based mental health programs (Bains et al., 2017) and school–family partnerships can support access to quality behavioral services in schools (Smith et al., 2020). Moreover, interventions designed to foster school–family relationships have shown positive impacts on student mental health and functioning (Sheridan et al., 2017; Smith et al., 2020). Collectively, salient indicators of school and community mental health supports and services must account for quality and access that are considered across a student’s ecology.
The Present Study
The overarching aim of the present study was to determine whether the SCMHSQ is suitable for addressing perceptions on the part of school professionals (school counselors and those in similar student support roles) of the quality and availability of school and community mental health supports and services. By accounting for key ecological factors, the SCMHSQ was designed to provide a holistic measure of perceptions of mental health supports and services, informing the appropriate selection of targeted mental health initiatives and interventions.
The following specific research questions guided this exploratory investigation. 1. Does the underlying dimensionality of the SCMHSQ align to the theoretically informed dimensions of the measure, which address microsystem indicators (in-school mental health supports and services, in-school leadership support of mental health, and community-based mental health services) and mesosystem indicators (school–community and school–family relationships)? We expected that the underlying dimensionality, assessed with exploratory factor analysis, would be relatively consistent to the theoretically derived dimensions that were based on the student’s microsystem and mesosystem. 2. Are the latent components derived from these models consistent when replicated in a split-half sample? We expected consistent and adequate factor loadings assessed with confirmatory factor analysis. 3. Are the latent components derived from these models internally reliable? We expected that each of the factors would demonstrate adequate internal reliability. 4. Can the SCMHSQ distinguish between school professionals’ perceptions of the quality and availability of school and community mental health supports and services in low-poverty communities compared to those with mid-poverty and high-poverty levels (establishing known-groups validity)? We expected that professionals working in schools serving students with higher economic needs (i.e., higher poverty) to report significantly worse quality and availability of mental health supports and services compared to professionals serving with more well-resourced areas (i.e., lower poverty).
Method
The present study used an exploratory descriptive study design to examine the psychometric properties and known-groups validity of the SCMHSQ. A convenience sampling method was employed to survey school professional perceptions of quality and availability of school and community mental health supports and services.
Participants
Participants were drawn from a larger study that aimed to investigate the psychometric properties of multiple measures addressing school experiences. Following Institutional Review Board approval, we invited members of a school counselor directory to participate by sending an email with a link to an anonymous, online survey available on Qualtrics. We targeted school counselors (and those working in similar roles to school counselors) for the study considering their prominent role in communication between health agencies and schools, and because of their role in providing school-based counseling and mental health services to and advocating for students with a variety of needs (Dekker et al., 2016; Marraccini et al., 2019).
Considering the low response rates associated with school professional completion of online surveys (Yetter & Capaccioli, 2010), we invited the complete directory of 34,571 school counselors with the aim to recruit between 600 and 800 participants. To minimize participant burden, we sent the email invitation only once. A total of 994 individuals opened the link, and 864 completed consent procedures. The final statistical sample included a total of 560 school professionals who completed the measures pertaining to the aims of this study.
The majority of participants reported working as a school counselor (95.9%) and a small number (3.8%) reported working in a related role (e.g., supervisor of school counselors, career development coordinator). Participants reported their race to be White (86.1%), Black or African American (9.1%), other (3.0%), American Indian or Alaskan Native (2.0%), Asian (1.4%), or Native Hawaiian/other Pacific Islander (0.9%). Ethnicity was asked as a separate question, with 4.7% of the sample indicating they were Hispanic or Latinx. The majority of participants (85.9%) reported their gender as female. Participants described working in their position for 0–5 years (36.6%), 5–10 years (23.5%), 10–15 years (21.7%), 16–20 years (14.9%), or 20 or more years (3.2%).
Participants reported working in elementary schools (23.9%), elementary and/or upper elementary schools (5.7%), middle schools (21.3%), high schools (35.9%), and schools with grades pre-K–12 (6.8%). Racial and ethnic compositions included schools that were predominantly non-Hispanic/Latinx and White (approximately 73% reported their student body as having 0%–30% Latinx students and 57.3% reported 50%–100% White students).
Measures
Demographic Questions
Demographic questions about participants included age, gender, ethnicity, profession, years spent working in the current position, and years spent working in the current school. Participants also reported on the demographics of their schools, describing the age range, racial/ethnic composition, and socioeconomic demographics of the student bodies.
The School and Community Mental Health Services Questionnaire
The SCMHSQ was initially developed as part of a larger questionnaire focused on school mental and community mental health services, and hospital-to-school reintegration services (Marraccini et al., 2019). Based on previous research and following an ecological systems theory, the items comprising the SCMHSQ were designed with the idea that schools can serve as a primary microsystem and facilitate supports across a student’s mesosystem. Thus, as described in the introduction, the survey aims to capture issues related to the microsystem (in-school mental health supports and services, leadership support of mental health services) and mesosystem (school relationship with the families, hospitals, and mental health providers).
Although the survey was intended for use by school support professionals more broadly (e.g., school psychologists, school counselors, school social workers, school nurses), the initial study in which this measure was piloted focused on school psychologist perceptions. Therefore, the survey was initially developed and iteratively modified based on feedback from five school psychologists working in five different states. School psychologists made recommendations for removing, adding, and revising specific items to address study aims (focused on school-based mental health practices) and to improve their accuracy and clarity. The survey was disseminated to school psychologists across the United States in an exploratory study examining existing processes and protocols for supporting school re-entry following psychiatric hospitalization (Marraccini et al., 2019). Findings from this preliminary study, based on data collected from school psychologists, identified school counselors as a primary provider of school-based mental health supports and services, meriting additional research focused on the perceptions of those working in a school counselor role (Marraccini et al., 2019).
Following this initial exploratory study, the survey was again refined based on feedback from an expert in survey design prior to dissemination. The disseminated survey that is the focus of the present study included a total of 17 items addressing the availability and quality of indicators at the student’s: (a) microsystem: school mental health supports and services, professional development and administrative support related to school mental health services, and community mental health services; and (b) mesosystem: relationship between school and community mental health and hospital providers, and relationship between school and family about mental health issues. Response options ranged from very poor (1) to excellent (5).
Analytic Plan
Prior to conducting psychometric analyses, we explored the sampling adequacy for our approach by calculating a Kaiser–Meyer–Olkin (KMO) and by conducting Bartlett’s test of sphericity with data from the full sample. KMO indicates the strength of the partial correlation between variables, with estimates at least 0.80 considered adequate for factor analysis (Kaiser & Rice, 1974). Bartlett’s test of sphericity tests the null hypothesis that the correlation matrix is an identity matrix (indicating that variables are unrelated), which suggests that data is not appropriate for factor analysis (Bartlett, 1951).
We next used a split-half, cross-validation approach to investigate the psychometric properties of the SCMHSQ (Redding et al., 2006), which involves randomly splitting the sample into halves for exploratory and confirmatory psychometric analyses. To address our first research question, “Does the underlying dimensionality of the SCMHSQ align to the theoretically informed dimensions of the measure?”, we conducted a series of exploratory factor analyses (EFA) with geomin rotations, considered appropriate when the true loading structure of the measure is unknown (Asparouhov & Muthén, 2009), using the first half of the sample. The number of components was selected using a combination of visual analysis of scree plots, Kaiser’s method of identifying eigenvalues above 1.0, theory alignment, and Horn’s parallel analysis. We interpreted factor loadings based on recommendations indicating >.71 as excellent, .63–.71 as very good, .55–.62 as good, .45–.54 as fair, and .32 or lower as poor (Tabachnick et al., 2007).
To address our second research question, “Are the latent components derived from the models internally consistent when replicated in a split-half sample?”, we employed cross-validation analysis using confirmatory factor analysis (CFA) on the second half of the data. Using the final set of items, we explored alternative models that were informed by findings from the EFA. We evaluated CFA models based on confirmatory fit index (CFI) and root mean square error of approximation (RMSEA) to examine model fit, with a CFI greater than .9 and RMSEA less than .05 indicating satisfactory fit (Awang, 2012).
Our third research question, “Are the latent components derived from these models internally reliable?”, was explored by calculating McDonald’s omega (ω). Omega is considered a more appropriate index of internal consistency reliability than Cronbach’s alpha (
Our fourth research question, “Can the SCMHSQ distinguish between school professionals’ perceptions of the quality and availability of school mental health supports and services in low-poverty communities compared to those with mid-poverty and high-poverty levels (establishing known-groups validity)?”, addressed known-groups validity. We examined differences in the final factor scores on the SCMHSQ between schools coded as low-poverty, mid-poverty, and high-poverty, controlling for report of racial and ethnic demographics (percent White and percent Hispanic/Latinx), using multivariate analysis of covariance (MANCOVA). We coded school professional-reported estimates of free and reduced priced lunch (FRPL) as a proxy for poverty using similar ranges to those employed by National Center for Education Statistics (Kena et al., 2015). More specifically, 35.8% of schools were categorized as low-poverty (in which 0%–30% of students were eligible for FRPL), 36.4% as mid-poverty (in which more than 30% and up to 75% of students were eligible for FRPL), and 27.7% as high-poverty (in which more than 75% of students were eligible for FRPL).We considered known-groups validity adequate when significant effects demonstrated at least a small effect (Cohen’s d ≥ 0.20).
We used SPSS version 26 (IBM Corp, 2019) to conduct descriptive analyses and data cleaning, and Mplus version 8 (Muthén & Muthén, 2017) to conduct the item analyses, EFAs, cross-validation, and final CFAs. Missing data for EFAs and CFAs were handled in Mplus with full information maximum likelihood (FIML) estimation.
Results
Prior to conducting psychometric analyses, we first tested assumptions of the sampling adequacy for our approach. We calculated a KMO value of .900 and found that Bartlett’s Test of Sphericity was significant,
Research Question 1: Exploratory Analyses
The initial EFA was conducted on the randomly selected first half of the sample (n = 274). Although Horn’s parallel analysis indicated retainment of only two factors, the Kaiser rule indicated retainment of four factors (with eigenvalues greater than 1.0 for four factors). Factor loadings calculated in the four-factor model also aligned well with ecological systems theory. More specifically, three factors represented separate aspects of a student’s microsystem (community and institution mental health services and supports, school-based mental health supports and services, and administrator support and professional development for mental health needs) and one factor represented an aspect of a student’s mesosystem (quality of relationships and communication between schools and families or institution/community mental health providers). Although the four-factor model was tentatively selected as the most appropriate fit to the data, we retained the two-factor model to evaluate fit in comparison to the four-factor model during the cross-validation procedure.
Factor Loadings from Exploratory Factor Analysis for Four-Factor Model of SCMHSQ.
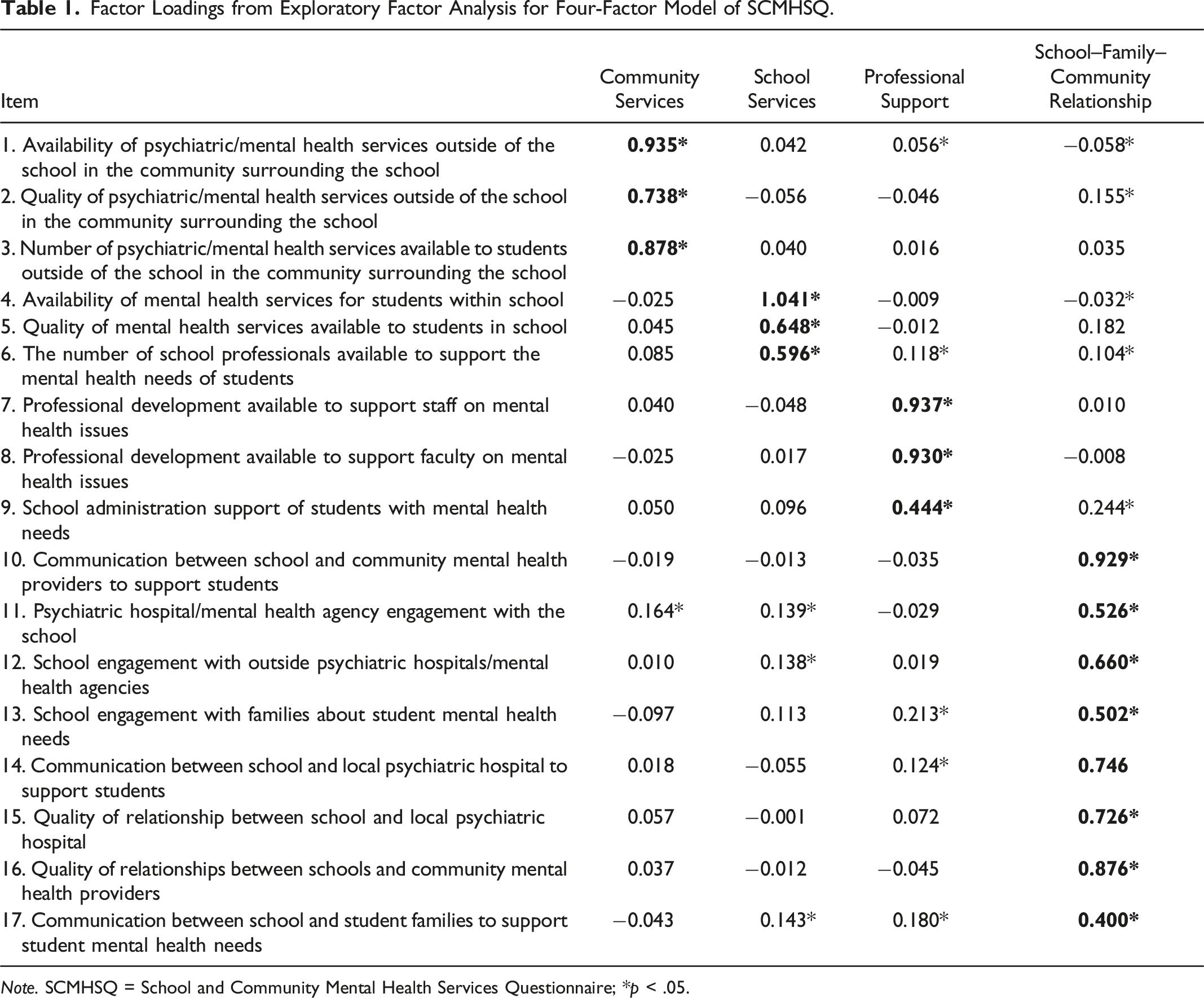
Note. SCMHSQ = School and Community Mental Health Services Questionnaire; *p < .05.
Research Question 2: Confirmatory Analyses
Summary of Fit Indices for Alternative SCMHSQ Models.

Note. CFI = confirmatory fit index; CI = confidence interval; df = degrees of freedom; RMSEA = root mean square error of approximation; SCMHSQ = School and Community Mental Health Services Questionnaire.

Standardized estimates for correlated model of SCMHSQ. Note. SCMHSQ = School and Community Mental Health Services Questionnaire; *p < .001.
Research Question 3: Internal Reliability
We assessed internal reliability using data collected from the entire sample by calculating McDonald’s omega (ω). Adequate reliability estimates were found for all four factors: Community Services, ω = 0.919, 95% CI: 0.904, 0.933; School Services, ω = 0.890, 95% CI: 0.871, 0.906; Professional Support, ω = 0.860, 95% CI: 0.834, 0.881; and School–Family–Community Relationships, ω = 0.902, 95% CI: 0.919, 0.940.
Research Question 4: Known-Groups Validity
We expected schools serving children and adolescents with higher economic needs to report having lower school and community mental health supports and services. To explore this hypothesis, we employed a MANCOVA with reported rates of FRPL serving as a proxy for school poverty level as the independent variable (low-poverty, mid-poverty, or high-poverty) and four dependent variables (Community Services, School Services, Professional Support, and School–Community–Family Relationship), controlling for race and ethnicity (percent White and percent Hispanic/Latinx). A final CFA was conducted on data from the entire sample to generate factor scores for each dependent variable used in this analysis (CFI = .879, RMSEA = 0.118; 90% CI: 0.111, 0.125). The results of the MANCOVA revealed a significant main effect of school poverty level (λ = .926, F(8) = 4.954, p < .001, partial η2 (ηp2) = .038). Neither of the covariates, percent White (λ = .985, F(4)=1.909, p = .108, ηp2 = .015) or percent Latinx (λ = .995, F(4) = 0.589, p = .671, ηp2 = .005), were significant.
Tests of between-subjects for school poverty level were significant for all four variables: Community Services, F(2) = 12.163, p < .001; ηp2 = .046; School Services, F(2) = 4.265, p = .015; ηp2 = .017; Professional Support, F(2) = 9.366, p < .001; ηp2 = .036), and School–Community–Family Relationships, F(2) = 9.686, p < .001; ηp2 = .037. No significant between-subjects differences were found for percent White or percent Latinx among any of the dependent variables.
Pairwise Comparisons for Univariate Tests of School Level and SCMHSQ Factor Scores.

Note. LB = lower bound; SE = standard error; SCMHSQ = School and Community Mental Health Services Questionnaire; UB = upper bound; *p < .05, **p < .01, ***p < .001.
Discussion
As schools increase school counselor-led mental health programming (Erford, 2019; Whiston et al., 2011) and counselors increase their delivery of systematic screenings, social/emotional interventions, and community-based services (Counts & Gionfriddo, 2016), attention to the range and quality of existing school and community services is needed. Therefore, the purpose of this study was to evaluate the psychometric properties of a new self-report measure (the SCMHSQ) identifying perceptions of the quality and availability of mental health supports in schools and communities, including quality of communication and relationships between schools, families, and communities. Findings suggest adequate model fit for a four-factor model composed of Community Services, School Services, Professional Support, and School–Community–Family Relationships. Furthermore, the measure’s ability to distinguish between low- and high-poverty districts provides preliminary support for the measure’s known-groups validity. In the following sections, we describe how each of the domains captured by the SCMHSQ relates to the literature and discuss how findings may inform research and practice.
Community Services
To prevent and ameliorate mental health difficulties among students, interventions need to be tailored to the specific makeup of individual schools. For example, schools in rural areas are less likely to have access to adequate numbers of mental health clinicians serving as outside providers and resources to support in-school programs, particularly those in poor or isolated areas (Hodgkinson et al., 2017). Although all subscales comprising the SCMHSQ could be distinguished by the school student body’s poverty level, the subscale Community Services may be particularly useful for capturing the quality and availability of these services. Schools that do not readily have access to such community supports may benefit from telehealth delivered from facilities in more distant regions; this has shown preliminary support for addressing several mental health disorders (Holland et al., 2021). Data collected from the SCMHSQ may help practicing counselors and lead counselors at the district or state-level advocate for such services.
School Services
School counselor-led mental health supports and services may be effective for promoting positive academic and behavioral outcomes (Amatea et al., 2010; Dimmitt & Wilkerson, 2012; Webb et al., 2019). The revised ASCA position statement on the School Counselor and Student Mental Health (ASCA, 2015) charges school counselors with advocating for student mental health needs by way of mental health-based instruction; academic, career, and social/emotional development advising; short-term counseling and interventions; and referrals to community resources in cases where students may need more intensive or longer term supports. Accordingly, school counselors represent a key stakeholder in informing the quality and availability of these services to support student mental health needs. Therefore, the School Services subscale may be used by practicing school counselors and district- and state-level counselor leads to identify gaps in quality and availability of school-based mental health supports and services, informing the need for additional resources and professionals to support such activity.
Professional Support
Schools within the same district may deviate in administrative support of mental health activities, and in professional development opportunities to enhance mental health care, implicating the potential value to using the Professional Support subscale to understand differences between schools. Successful implementation of school-based mental health programs may depend on buy-in by a majority of school personnel (Kutash et al., 2006) and on administrative support for the program (Langley et al., 2010). Previous research also suggests that school counselors may feel confident in their skills for counseling general education students, but they may feel less confident when supporting youth with more intensive mental health needs and benefit from targeted training opportunities (Carlson & Kees, 2013). Therefore, school counselors and associated professionals may leverage findings from the Professional Support subscale to advocate for training activities to bolster knowledge and skills for supporting student mental health.
School–Community–Family Relationships
Finally, the School–Community–Family Relationships subscale can assess the efficacy of communication bridging outside providers, families, and the school system. Relationships between the school and the community, and the school and the family, are critical for delivering culturally grounded mental health interventions (Marraccini et al., 2021). Moreover, limited communication between these entities can serve as a barrier to school reintegration and mental health support (Savina et al., 2014). Effective school counseling is considered a “collaborative process involving school counselors, students, families, teachers, administrators, other school staff, and education stakeholders” (ASCA, 2019a; p. 2). The School–Community–Family Relationships subscale can be used to inform needs assessments regarding networks between schools and communities, given the need for school counselors to connect youth with mental health concerns to care providers (ASCA, 2019a), and to inform partnerships with families.
Implications
Findings from this study suggest that practicing school counselors, and those in a similar role, were able to distinguish between types of mental health supports for low- and high-poverty schools. Because students of color are overrepresented in economically disadvantaged schools across the United States (Anderson & Ritter, 2017; Marrast et al., 2016), this survey may support school counselors in addressing the needs of economically and racially diverse student bodies. Indeed, the ASCA National Model requires school counselors to become proficient in addressing the complex needs for school, families, and community mental health supports and services among students who may experience environments that are culturally different and less resourced from those of the counselors (ASCA, 2019a, 2022; Butler & Constantine, 2005).
School counselors are well positioned to advocate for economically and racially diverse students (ASCA, 2019a, 2019c), including advocacy efforts that target adequate community and school-based mental health supports (Adelman & Taylor, 2015; Atkins et al., 2010). While lack of resources and support contributes to the importance of school counselors’ involvement in school–community–family relationships (i.e., non-counseling duties), it also fits well within ASCA’s description of the roles of school counselors as advocates, consultants, and collaborators. As educational leaders, school counselors advocate for students’ needs related to their academic, career, and social/emotional development (ASCA, 2019a). As consultants and collaborators, school counselors share strategies, serve as advocates, and work with other members of the community “to support student achievement and advocate for equity and access for all students” (ASCA, 2019a, p. 81).
The ASCA School Counselor Professional Standards & Competencies (2019b) also calls on school counselors to identify gaps in resources in schools by collecting and analyzing student data, including the need for appropriate resources to support action plans. Therefore, the SCMHSQ may support school counselors in improvement efforts and decision making for mental health interventions. Specifically, school counselors can use the SCMHSQ as a tool to guide school–community–family relationship building and actions in support of student mental health care.
First, acting in their role as consultants and advocates, school counselors can meet with school and community members to help support the mental health needs of economically disadvantaged schools. The school counselor should first become familiar with the cultural groups served by the school and within the community (Panigua, 2013). By examining their own cultural assumptions, school counselors can seek to identify and explore how the values and experiences of families—who may be hesitant in seeking mental health services—may differ from their own in relation to mental health.
Second, school counselors can assess the needs and strengths of their students’ ecology (Erickson & Abel, 2013). This involves identifying student-level needs and strengths, and also identifying the needs and strengths of the student’s school and community with an assessment such as the SCMHSQ, which can be enhanced with additional inquiries into school experiences. For example, school counselors may interview students, teachers, parents/families, and community members in subscales of the SCMHSQ that were particularly high or low.
A third and final step involves analysis of data, which can be enhanced through collaborations with school, community, and family in the form of a partnership leadership team (PLT). The PLT could be made up of the school counselor, administration, student services personnel (psychologist, social workers), teachers, students, family members, and community members. Members can begin by reviewing each SCMHSQ subscale or item that is most pressing to determine goals and strategies to improve relationships and enhance care. Ultimately, these actions can serve as a roadmap for increasing access to quality mental health care and enhancing partnerships with families and communities.
Limitations
The present study included a national sample of school counselors and professionals in similar student support roles, representing key professionals who interface with students in the context of mental health crises (Marraccini et al., 2019); however, because the sample was a convenience sample from a school counselor directory, findings may not generalize to all counselors. Although this instrument was designed to address multiple school-based support professionals, including school counselors, its development was originally informed and piloted with school psychologists and could benefit from feedback provided by school counselors specifically. Moreover, perspectives of other support personnel, and those of students, families, and community members, may be important to consider for informing a more holistic understanding of school and community mental health supports and services.
Although designed to examine a self-report measure, all study variables may be limited by self-report bias and may not accurately reflect school and community characteristics. Moreover, because we did not collect the specific location of professionals, we were unable to explore similarities and differences based on regional location. Finally, the study did not examine the relationship between school professionals’ perceptions of school and community mental health and student outcomes, which would provide important information regarding the validity of this measure.
Conclusion
As school systems and school counselors tackle student mental health issues, there is a need for brief, reliable, and valid measurement tools designed to assess quality of mental health services. The SCMHSQ serves as one possible starting point for schools to address their students’ mental health service needs. Results indicated that the SCMHSQ demonstrated adequate internal reliability and known-groups validity, revealing a four-factor model that describes the availability of school and community mental health services and the quality of the relationships between schools, families, and community mental health providers. This new measure has potential as an informative tool for practicing school counselors seeking to better understand availability and quality of mental health supports for their students; for school administrative teams seeking baseline information to understand and improve services; and for researchers controlling for heterogeneity in school-based mental health service quality and availability. Further validation of this measure could help create a meaningful tool that can support practitioners and school-based professionals in developing a better understanding of the availability and quality of mental health services in schools and in the community.
Footnotes
Acknowledgments
The researchers thank the professionals who contributed their time in support of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.