
Abstract
This randomized controlled trial aimed to investigate the distinctness after treatment among hot herbal compress, hot compress, and topical diclofenac. The registrants were equally divided into groups and received the different treatments including hot herbal compress, hot compress, and topical diclofenac group, which served as the control group. After treatment courses, Visual Analog Scale and 36-Item Short Form Health survey were, respectively, used to establish the level of pain intensity and quality of life. In addition, cervical range of motion and pressure pain threshold were also examined to identify the motional effects. All treatments showed significantly decreased level of pain intensity and increased cervical range of motion, while the intervention groups exhibited extraordinary capability compared with the topical diclofenac group in pressure pain threshold and quality of life. In summary, hot herbal compress holds promise to be an efficacious treatment parallel to hot compress and topical diclofenac.
Myofascial pain syndrome is one of the most common illnesses in the working-age population attributable to tasks that require remaining in a sitting posture for an extended period of time, such as using a computer. Myofascial pain syndrome leads to muscle and joint pain, particularly in the upper trapezius, which, in turn, adversely affects occupational efficiency and quality of life. 1 –5 A widely used treatment is the administration of conventional medicine, especially nonsteroidal anti-inflammatory drugs. However, despite their efficacy in relieving pain and inflammation, nonsteroidal anti-inflammatory drugs have been found to cause undesirable side effects. One best alternative treatment for myofascial pain syndrome that can empirically relax muscles and alleviate pain and, at the same time, reduce the undesirable side effects of pain relief medication is the application of a hot compress. 6
A review of the literature indicates that very little research on the use of a hot compress has employed a scientific instrument in following up its posttreatment efficacy. The present study, therefore, aimed to examine the efficacy of a hot compress in the treatment of myofascial pain syndrome in the upper trapezius in comparison with that of nonsteroidal anti-inflammatory drugs. Ultimately, it is hoped that the research will play a part in preserving Thai folk wisdom and advancing guidelines for developing Thai traditional medicine into scientific treatment recognized for its efficacy in alleviating chronic diseases and improving quality of life.
Methodology
Study Designs
The present study was a single-blind randomized controlled trial using a simple random sampling method and a pregenerated random assignment scheme enclosed in an envelope.
Study Settings
The research was conducted at the Faculty of Medicine of Thammasat University at the time of the study.
Participants
Ninety patients volunteered to participate in the study. Having been diagnosed with myofascial pain syndrome in the upper trapezius by clinicians, the patients were assigned into the hot herbal compress group (n = 30), the hot compress group (n = 30), or the topical diclofenac group (n = 30).
Inclusion Criteria
Patients with myofascial pain syndrome in the upper trapezius aged between 25 and 65 years Over 3 months of the symptoms Being diagnosed with myofascial pain syndrome and trigger points in upper trapezius muscles including local tenderness, taut bands, hyperirritable spots, jump signs, and referred pain
3,4
Willingness to participate throughout the study period
Exclusion Criteria
History of allergy to diclofenac (Difelene) Pregnancy for female patients Injuries to or fractures in the neck, back, and/or shoulders Referred numbness to the arms caused by entrapment neuropathy Consumption or application of steroid medication 2 weeks prior to participation in the study Being administered acupuncture treatment or physiotherapy at the time of the study
Study Intervention
The randomization process involved the allocation of a pregenerated random number enclosed in an envelope to each of the participants, making it impossible for the physicians or the assessor to be aware of their group prior to the treatment (see Figure 1).

Study flowchart.
Hot Herbal Compress Group
The participants in this group received a 20-minute treatment at a temperature not exceeding 45°C once a week for 2 weeks that was done by the same therapist throughout the study period. 7 The hot herbal compress (930 g) containing Zingiber cassumunar Roxb., Curcuma longa L., Cymbopogon citratus (DC.) Stapf, Citrus hystrix DC., Tamarindus indica L., Acacia concinna (Willd.) DC., camphor, and sea salt was administered once every 3 days at D1, D4, D7, D10, D13, and D16, before the final treatment and follow-up, totaling 7 times of treatment.
Hot Compress Group
Similarly to those in the hot herbal compress group, the participants in this group received a 20-minute treatment at a temperature not exceeding 45°C once a week for 2 weeks that was done by the same therapist throughout the study period. 7 The hot compress was administered once every 3 days, that is, D1, D4, D7, D10, D13, and D16, before the final treatment and follow-up, totaling 7 times of treatment.
Topical Diclofenac Group
The participants in this group were prescribed 2 mg of diclofenac gel, a nonsteroidal anti-inflammatory drug, according to medical standards for self-application on the affected areas 3 times a day in the morning, at noon, and in the evening for 2 weeks before the final follow-up.
Analytical Tools
Pain Assessment
Commonly used to measure a characteristic or an attitude that cannot be directly measured easily, a Visual Analogue Scale (VAS) is a 10-cm scale instrument on a continuum of values ranging from “0” (no pain) to “10” (worst imaginable pain). 8 –10
Cervical Range of Motion (CROM)
A magnetic device was placed on the participants’ nose bridge and ears and fastened on the back of their head with a Velcro strap to measure their CROM. 8,9 This procedure ensured accurate measurement and remeasurement, rotational movement in an upright position, and prevention of the chance of human errors.
Pressure Pain Threshold (PPT)
A pressure algometry technique was used to measure the participants’ PPT. A handheld electronic pressure algometry device with a surface area at the round tip of 1 kg/cm2 was used to gradually increase compression pressure at the rate of approximately 1 kg/s perpendicularly onto the muscle tissue to be tested. The participants had been instructed to state immediately when the pressure turned into a sensation of pain, at which time compression was stopped with the pressure being released. After a 30-second pause, the next measurement was taken. Each threshold pressure was measured 3 times and the average value was used for analysis. 8 –10
Short-Form Health Survey
The Short-Form Health Survey (SF-36) used in the present research was a 36-item questionnaire measuring the quality of life across 8 physical and emotional domains, namely, physical functioning, role limitations due to physical health, role limitations due to emotional problems, energy/fatigue, emotional well-being, social functioning, pain, and general health. 10 –14
Statistical Analysis
Descriptive statistics such as mean, standard deviation, and percentage were used for the analysis. In addition, a paired t test was used to compare changes in the scores before and after the treatment and between the 3 groups. Also, repeated-measures ANOVA was run to compare the scores on the VAS, CROM, and PPT.
Results
The demographic characteristics of the participants are shown in Table 1. In terms of age, those in the topical diclofenac group were the oldest, followed by those in the hot compress group and the hot herbal compress group. With regard to gender, the participants in all the 3 groups were mainly female. Regarding job fields, all the participants were working in a profession that required the use of a computer. As for pain periods, those in the hot herbal compress group had been suffering from myofascial pain syndrome in the upper trapezius for the longest period of time, followed by those in the hot compress group and the topical diclofenac group.
Demographic Characteristics of the Participants.

aMean ± standard deviation.
bNumber (percentage).
Figure 2 shows the adjusted estimated means of pain intensity measured with VAS scores among the 3 groups using the GLM. The participants in all the 3 groups did not experience any statistically different levels of pain at baseline, on day 16, or during the follow-up (P < .05). In addition, the participants in all the 3 groups similarly felt a statistically lower level of pain during the follow-up (P < .05) although those in the hot herbal compress group suffered the lowest level of pain, followed by those in the hot compress group and the topical diclofenac group.
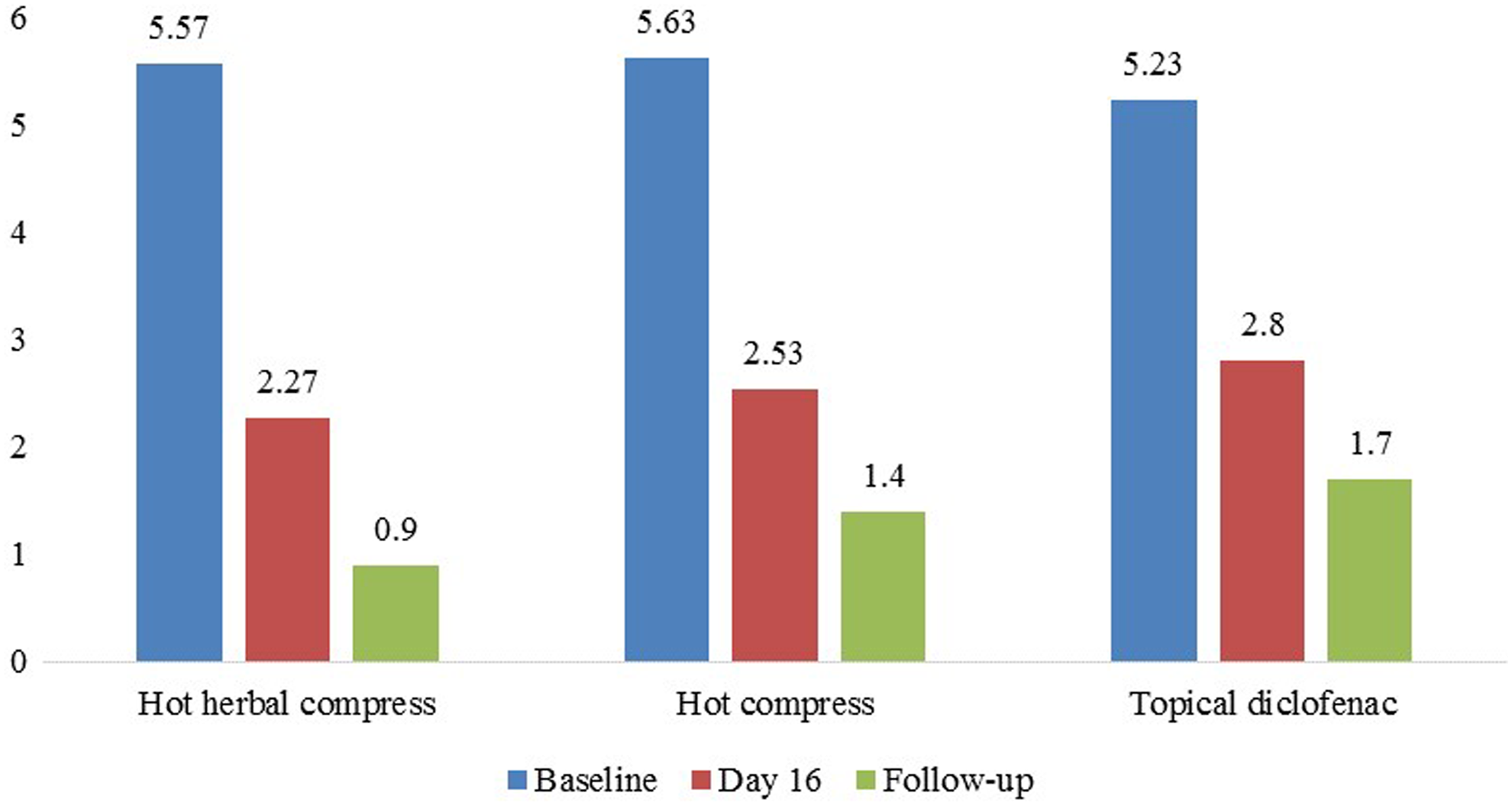
Estimated means of pain intensity measured with Visual Analogue Scale (VAS) scores.
Figure 3 shows the adjusted estimated means of CROM scores among the 3 groups using the GLM. The participants in all the 3 groups did not experience any statistically different levels of CROM flexion, CROM extension, lateral flexion RT, or lateral flexion LT at baseline, on day 16, or during the follow-up (P < .05). In addition, the participants in all the 3 groups similarly illustrated a statistically higher level of CROM flexion, CROM extension, lateral flexion RT, and lateral flexion LT during the follow-up (P < .05), although those in the hot herbal compress group enjoyed the highest level of CROM flexion, CROM extension, lateral flexion RT, and lateral flexion LT, followed by those in the hot compress group and the topical diclofenac group.
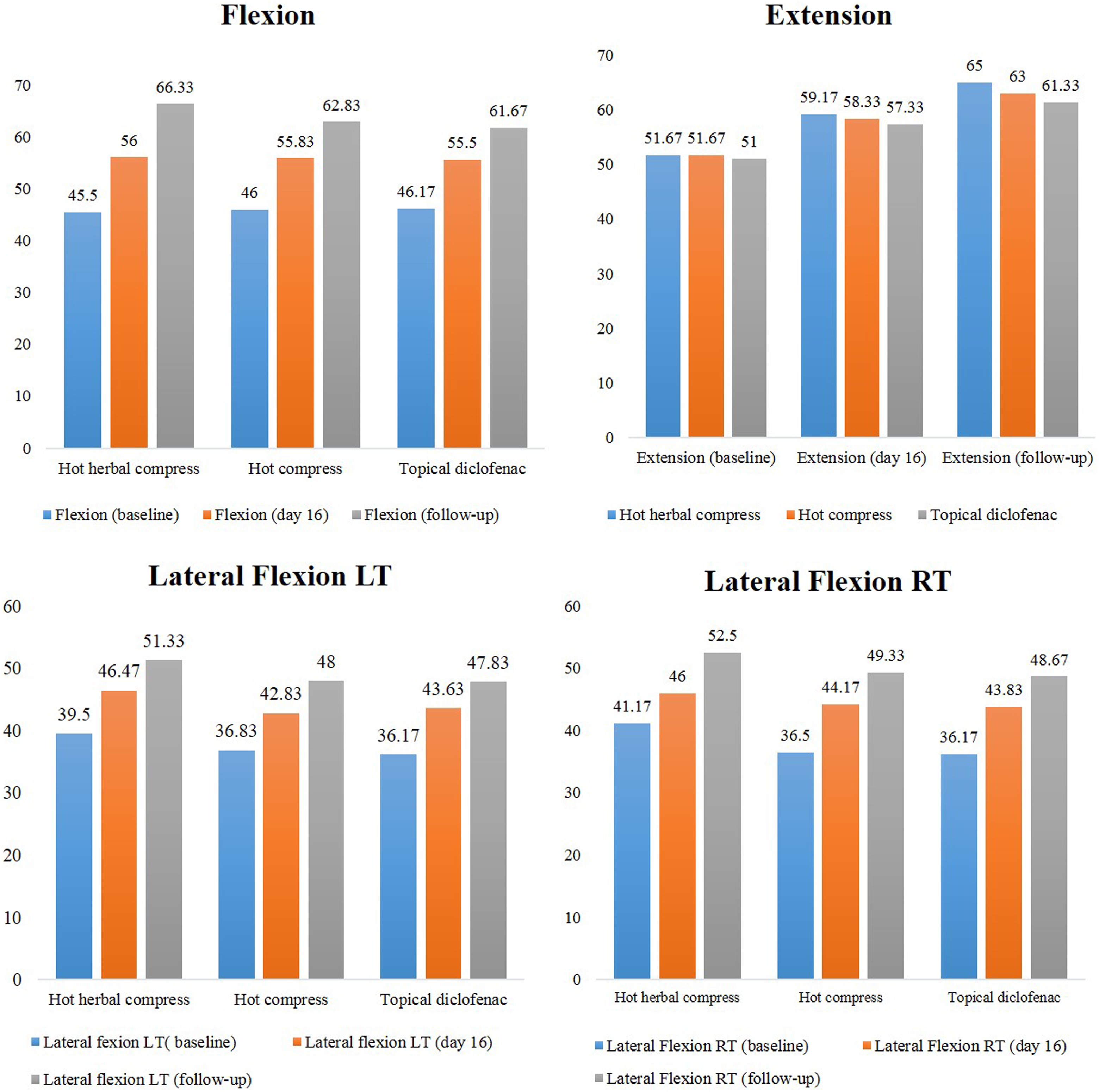
Adjusted estimated means of cervical range of motion (CROM) scores among the 3 groups.
Figure 4 shows the adjusted estimated means of PPT scores among the 3 groups using the GLM. The participants in all the 3 groups did not experience any statistically different levels of PPT LT or PPT RT at baseline, on day 16, or during the follow-up (P < .05). In addition, the participants in all the 3 groups similarly exhibited a statistically higher level of PPT LT and PPT RT during the follow-up (P < .05), although those in the hot herbal compress group enjoyed the highest level of PPT LT and PPT RT, followed by those in the hot compress group and the topical diclofenac group.

Adjusted estimated means of pressure pain threshold (PPT) scores.
Table 2 compares the SF-36 domain means divided into Physical Component Summary scores and Mental Component Summary scores before and after treatment as well as across groups. The participants in all the 3 groups experienced statistically significant improvements in both the physical components and the mental components of their quality of quality after the treatment (P < .05). As for differences across groups, the participants in the hot compress group enjoyed the highest level of improvement in the physical components of their quality of life, followed by the hot herbal compress group and the topical diclofenac group. Similarly, the participants in the hot compress group exhibited the highest level of improvement in the mental components of their quality of life, followed by the topical diclofenac group and the hot herbal compress group. However, it should be noted that such differences were not statistically significant.
Comparison of SF-36 Domain Means Divided Into Physical Component Summary Scores and Mental Component Summary Scores Before and After Treatment Across Groups.

Abbreviations: CI, confidence interval; PCS, Physical Component Summary; MCS, Mental Component Summary.
Discussion
The objective of this experimental study is to determine whether a hot herbal compress is as efficacious as a hot compress or a nonsteroidal anti-inflammatory drug, specifically a topical diclofenac gel, in treating patients with myofascial pain syndrome in the upper trapezius. To recapitulate, it was found that the pain levels experienced by the 3 groups of participants reduced statistically significantly during the follow-up (P < .05). In addition, the PPT levels tolerated by the 3 groups of participants increased statistically significantly during the follow-up (P < .05). Additionally, improvements in the physical components and the mental components of quality of life across the 3 groups were statistically significant after the treatment (P < .05).
Such findings bear a resemblance to those in the literature. 15,16 One randomized controlled trial assigned 60 participants to a Thai massage group, a Thai herbal compress group, and an oral ibuprofen group in order to examine the efficacy of the 3 options in treating osteoarthritis and alleviating pain and stiffness, discovering statistically significant improvements on all assessment indices that were comparable across the 3 experimental groups. 16 Similarly, in a meta-analysis of the clinical effects of Thai herbal compress, it was found that all the 13 studies analyzed indicated that Thai herbal compress treatment resulted in statistically significant improvements in the alleviation of osteoarthritis and muscle pain and that such a treatment alternative was as efficacious as nonsteroidal anti-inflammatory drugs, knee exercise, and hot compress therapy. 16 Similar results have also been reported elsewhere in studies examining the efficacy of similar therapeutic approaches focusing on relieving pain and increasing flexibility, such as massage, yoga, and stretching. 17 –20
When explored further, the 3 treatment options applied in this study led to different outcome levels. That is, hot herbal compress treatment seemed to be generally superior to treatment with a hot compress and a topical diclofenac gel, albeit not statistically significantly, at least in terms of reducing pain intensity, enhancing CROM, and increasing PPT. This finding came as a surprise at first, but a review of the literature points to a similar likelihood. 15,16 For instance, hot herbal compress therapy was reported to be more efficacious than not only its alternative, nonmedical counterparts, such as a hot compress, massage, and muscle exercise, but also medical options administered to relieve pain, such as nonsteroidal anti-inflammatory drugs. 15,16
Although definite reasons for the superiority of a hot herbal compress are not yet known, it may be hypothesized that the combination of heat and herbal ingredients including Z cassumunar, C longa, C citratus, C hystrix, T indica, A concinna, camphor, and sea salt gives this treatment option an advantage over others relying on only one therapeutic component, such as a hot compress and massage. Z cassumunar is used as an essential oil and is believed to ease pain and inflammation in traditional medicine. The rhizome oils of Z cassumunar have been previously investigated for its chemical composition. Terpinen-4-ol, α- and β-pinene, sabinene, myrcene, α- and γ-terpinene, limonene, terpinolene, sabmene, and monoterpenes have been reported as its major constituents. 21,22 In addition, compound D, (E)-4-(3′,4′-dimethoxyphenyl)but-3-en-2-ol, is another compound that can be found in the hexane extract of Z cassumunar. In many studies, compound D showed successive effectiveness on anti-inflammatory activity and anti-analgesic activity. Compound D also has been documented as a mediated prominently on the acute phase of inflammation as well as inhibition of prostaglandin biosynthesis in animal models. 23 Apart from Z cassumunar, C longa also was added to the herbal ball. The methanolic extract from rhizomes was investigated to identify the chemical constituents. Previous research reported that the major compounds consisted of curcumin, ar-turmerone, β-sesquiphellandrene, and curcumenol. 24 In animal models, C longa rhizome extracts were also examined for analgesic and antipyretic activities, and the rhizome extracts showed effective potency on analgesic effect. 25 C citratus is another widely used herb in folklore and traditional medicine. The chemical constituents of essential oil have been examined and it was found that geranial, neral, and myrcene were 3 main active constituents. 26 Furthermore, C citratus was investigated for its analgesic and antipyretic properties, and previous research has suggested that the essential oil from C citratus displayed strong analgesic and antipyretic properties both in central and peripheral analgesic activities. 26,27 C hystrix is another ingredient whose chemical composition in essential oil was reported, which dominantly contained citronella (citronellal, citronellol, and geraniol). 28 Citronella, which is commonly used as an effective insect repellent, also exhibited analgesic and anti-inflammatory properties. 29 T indica, a leguminous tree in the family Fabaceae indigenous to tropical regions, was added into the herbal ball as another ingredient. Some scientific evidences reported its active constituents from leaves. Their results confirmed that its leaves contained essential oils, free and conjugated fatty acids, flavonoids, and other compounds such as linonene and benzyl benzoate. 30 T indica was evaluated and its anti-inflammatory activity by the methanol extract showed significant reduction in paw thickness in carrageenan-induced acute inflammation and cotton pellet–induced chronic inflammation models and also produced significant central analgesic activity. 31,32 A concinna, which has been commonly used in both the Ayurvedic and Thai traditional medicine, was also added. The chemical constituents of volatile compounds have already reported: A concinna contained common fatty acids such as palmitic and linoleic acid. 33 Even though analgesic activity has not been documented, A concinna played an important role in immunological adjuvant activities by the saponin extracts, which lead to enhance IgG, IgG1 IgG2a, and IgG2b antibody levels in serum. 34 Despite its advantage over a hot compress or a topical diclofenac gel, however, a hot herbal compress was found in the present study to be less satisfactory than a hot compress in terms of the physical components of quality of life and both a hot compress and a topical diclofenac gel in terms of the mental components of quality of life. This result does not seem to have any logical premises considering the fact that a hot herbal compress fared better than a hot compress and a topical diclofenac gel in terms of pain intensity, CROM, and PPT. One interpretation of the participants’ more favorable reaction to a topical diclofenac gel on the SF-36 is perhaps that their response might not be an accurate manifestation of their actual physical improvements. Alternatively, possible explanations may lie in different interactions between the 3 types of treatment and the self-rated physical and mental components scores of quality of life in contrast to such objectively measurable outcome variables such as pain intensity, CROM, and PPT.
Although this study has made it clear that a hot herbal compress is an alternative for patients with myofascial pain syndrome in the upper trapezius that is as efficacious as, if not more so than, comparable nonmedical choices, such as a hot compress, or even pain-relief medications, such as nonsteroidal anti-inflammatory drugs, it remains to be seen to what physical mechanisms the efficacy of a hot herbal compress can be attributable, why actual physical improvements do not coincide with self-rated improvements in the physical and mental components of quality of life, and whether a hot herbal compress may have any undesirable side effects on this group of patients and under what conditions, to name but a few. Research answering these questions will not only preserve but also advance the application of Thai folk wisdom and alternative treatment, especially in alleviating muscle and joint pain caused by myofascial pain syndrome in the upper trapezius.
Conclusion
The present study aimed to examine the efficacy of a hot herbal compress compared to that of a hot compress and a topical diclofenac gel in the treatment of patients with myofascial pain syndrome in the upper trapezius. The findings indicated that all the 3 treatment options were efficacious in reducing pain levels, increasing CROM, increasing PPT, and improving quality of life. However, hot herbal compress treatment contributed to lower pain levels and higher CROM and PPT. It can be concluded, therefore, that treatment with a hot herbal compress is likely to be a better option than that with a hot compress or a topical diclofenac gel.
Footnotes
Acknowledgments
The authors gratefully acknowledge the Thammasat University Fund under TU Scholar Contract No. 2/40/2560 and the Faculty of Medicine of Thammasat University for sponsoring this study.
Author Contributions
Study conception and design: Boonruab and Nimpitakpong
Acquisition of data: Boonruab, Damjuti, and Nimpitakpong
Analysis and interpretation of data: Boonruab and Damjuti
Drafting of manuscript: Boonruab and Damjuti
Critical revision: Damjuti
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded Thammasat University Fund under TU Scholar Contract No. 2/40/2560.
Ethical Approval
The study was approved by the Ethics Committee for Research Involving Human Subjects of the Faculty of Medicine, Thammasat University (No. 224/2559).