
Abstract
Objective:
Frozen shoulder is a common disorder in general orthopedic practice, characterized by spontaneous onset of pain in the shoulder and accompanied by limitation of glenohumeral movement. Treatments for frozen shoulder include shoulder exercise, manual therapy, corticosteroid injection, manipulation under anesthesia, and arthroscopic capsular release. Several patients suffer from some degree of pain and range of motion limitation for up to 10 years even when these treatments are applied. Kampo, a traditional Japanese herbal medicine based on traditional Chinese herbal medicine, has been used for the treatment of pain in Japan. Nijutsuto has been a Kampo formula used to effectively treat frozen shoulder.
Methods:
Thirteen patients suffering from long-term frozen shoulder refractory to Western medical treatment were administered Nijututo.
Results:
Almost all patients experienced sound pain relief after Nijutsuto admnistration. There were no severe side effects reported.
Conclusion:
Nijutsuto combined with an exercise program improved pain intensity in 13 patients with long-term frozen shoulder.
Keywords
Frozen shoulder, or adhesive capsulitis, is a common disorder in general orthopedic practice, 1 –3 characterized by spontaneous onset of pain in the shoulder and accompanied by limitation of active and passive glenohumeral movement. 1,3 Although the exact cause is unknown, 1,4 the pain is always severe enough to disturb the patient’s sleep. 4,5 Treatments for frozen shoulder include shoulder exercise, manual therapy, corticosteroid injection, manipulation under anesthesia, and arthroscopic capsular release. 1,4 –6 Some studies described that frozen shoulder was resolved in a few years, while others showed that several patients suffered from some degree of pain and range of motion limitation for up to 10 years even when these treatments were applied. 2,5,6
Kampo, a traditional Japanese herbal medicine based on traditional Chinese herbal medicine, has been used for the treatment of not only pain but also many diseases in Japan. 7,8 Nijutsuto (ingredients: white and blue atractylodes, hoelen, citrus, arisaema, cyperus, scute, clematis, chianghuo, pinellia, liquorice, ginger) has been a Kampo formula used to effectively treat frozen shoulder. 8 –10 We report here that Nijutsuto combined with a 20-minute exercise program improved pain intensity and shoulder function in 13 patients with frozen shoulder refractory to Western medical treatment.
Methods
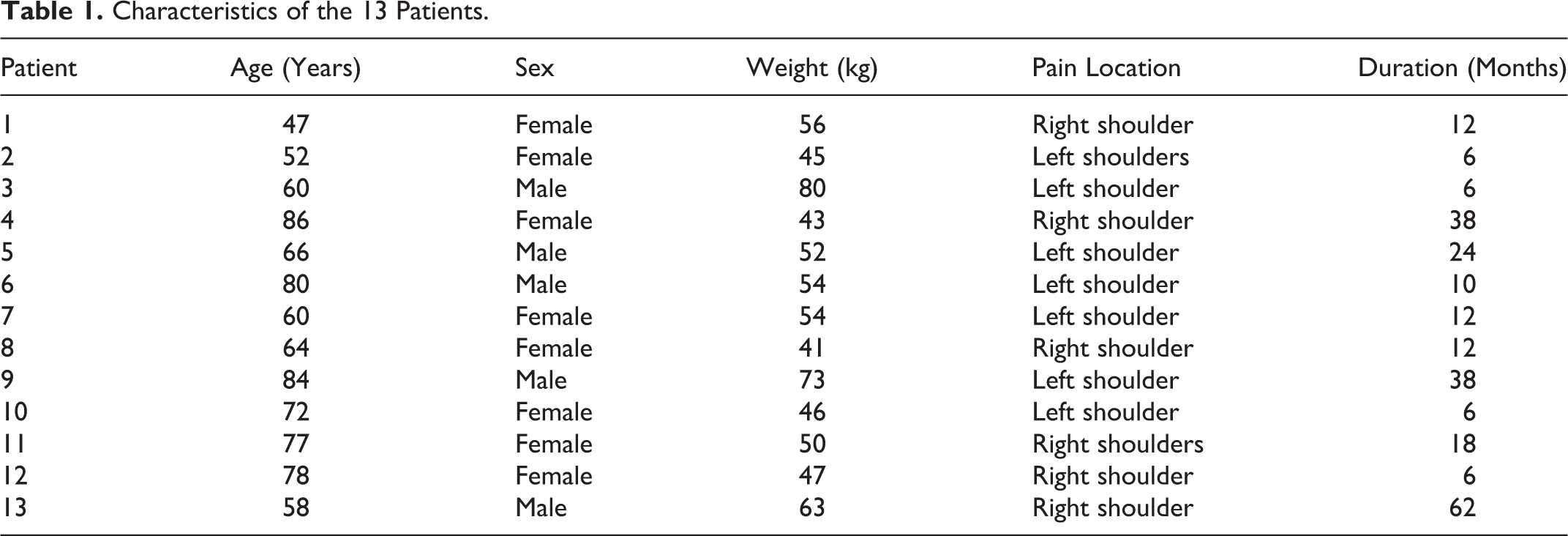
Retrospective analysis from January 2012 to October 2013 was performed on 13 patients who visited the Multidisciplinary Pain Center (Pain Center) of Aichi Medical University. All patients were referred from other hospitals to the Pain Center because of frozen shoulder refractory to shoulder exercise, manual therapy, and corticosteroid injection. Treatment protocols used in the present report were based on institutional policy and clinical guidelines approved by the institutional review board of Aichi Medical University. After obtaining approval from the institutional review board of Aichi Medical University, we routinely explain to all patients that we record and store demographics, symptoms, course of pain and medical records of all patients for possible future use in our research after which we obtain written informed consent on their initial visit to the Pain Center. The characteristics of the patients are described in Table 1. Eight patients were female and 5 were male, and their ages ranged from 41 to 80 years.
Characteristics of the 13 Patients.
The diagnosis was made based on the presence of shoulder pain with limitation of active and passive movements of the glenohumeral joint of ≥25% in at least 2 directions (flexion, abduction, external rotation, internal rotation). The intensity of pain was rated by the patients using a numerical rating scale where 0 indicated no pain and 10 the greatest pain possible in a lying position, at rest, and on active shoulder elevation. The shoulder flexion, abduction, and internal and external rotation active range of motion were measured before treatment and on completion of treatment.
After obtaining approval from the Ethics Committee of Aichi Medical University (reference number: 13-097), we explained to the patients that we had recorded and stored their demographics, symptoms, course of pain, and medical records for future use in our review after which we obtained written informed consent. The patients were taught a 20-minute exercise program to be performed at home twice a day by physiotherapists. It consisted of stretching exercises and active range of motion exercises in the planes of flexion, abduction, external rotation, and internal rotation. Follow-up physical assessments and advice about intensity, frequency, and progression of the exercises were also conducted by the physiotherapists once a month. All patients visited our Pain Center every month. They were administered 2.5 g of Nijututo (TJ-88, Tsumura & Co., Tokyo, Japan) 3 times a day, while continuing the exercise program. A numerical rating scale at rest and while moving in the patients ranging from 0 to 10 (0 = no pain, 10 = worst pain imaginable) was evaluated and recorded each month. Changes of shoulder active range of motion were evaluated before and at the completion of the treatment.
Results
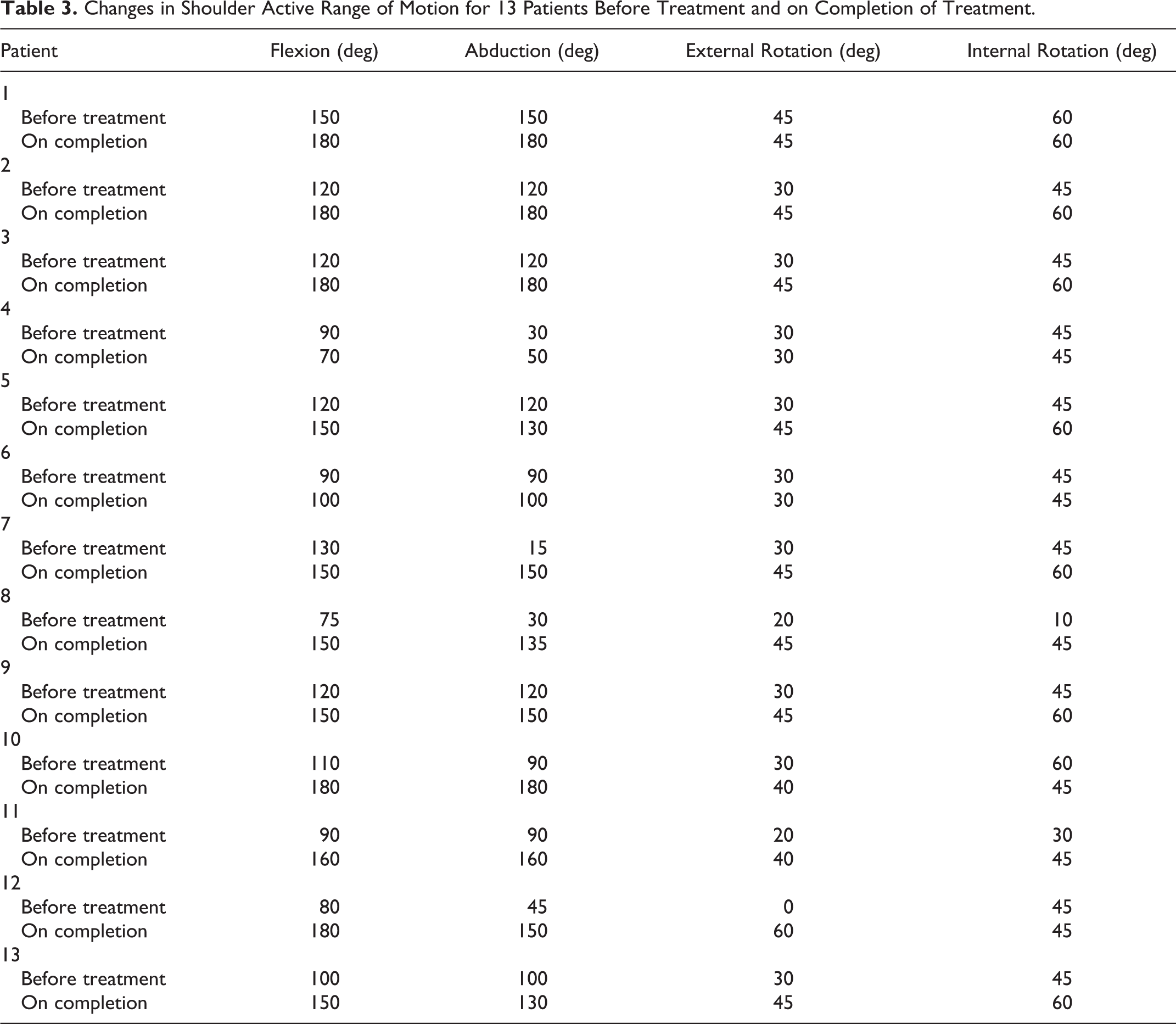
Almost all patients experienced sound pain relief after the treatment (Table 2). The scores on the numerical rating scale in a lying position significantly decreased in 3 months (median [range] of baseline, 5 [0-9]; median [range] of month 1, 4 [0-9]; median [range] of month 2, 2 [0-8]; median [range] of month 3, 1 [0-7]; Friedman test, P < .0001). The numerical rating scale scores at rest significantly decreased in 3 months (median [range] of baseline, 3 [0-7]; median [range] of month 1, 1 [0-3]; median [range] of month 2, 0 [0-3]; median [range] of month 3, 0 [0-3]; Friedman test, P = .001). Also, the scores on active shoulder elevation significantly decreased in 3 months (median [range] of baseline, 7 [3-10]; median [range] of month 1, 4 [0-10]; median [range] of month 2, 3 [0-8]; median [range] of month 3, 1 [0-4]; Friedman test, P < .0001). Moreover, the shoulder flexion active range of motion significantly improved (median [range] of baseline, 110 [75-150]; median [range] at completion, 150 [70-180]; Wilcoxon matched pairs test, P = .0029) (Table 3). The shoulder abduction active range of motion significantly improved (median [range] of baseline, 90 [15-150]; median [range] at completion, 150 [50-180]; Wilcoxon matched pairs test, P = .0016) (Table 3). And the shoulder internal rotation active range of motion significantly improved (median [range] of baseline, 30 [0-45]; median [range] at completion, 45 [30-60]; Wilcoxon matched pairs test, P = .0049) (Table 3). Also, the shoulder external rotation active range of motion significantly improved (median [range] of baseline, 45 [10-60]; median [range] at completion, 60 [45-60]; Wilcoxon matched pairs test, P = .0248) (Table 3). There were no severe side effects reported.
The Changes of Individual Pain Scores (Numerical Rating Scale) in a Lying Position (L), at Rest (R), and on Active Shoulder Elevation (A) for 13 Patients.

Changes in Shoulder Active Range of Motion for 13 Patients Before Treatment and on Completion of Treatment.
Discussion
Frozen shoulder is one of the most common musculoskeletal problems experienced in orthopedics. 1 –3 It is characterized by spontaneous onset of shoulder pain and by progressive limitation of both active and passive glenohumeral movement. 1,3 Although the exact cause has yet to be identified, the pain is always severe enough to disturb patient’s sleep. 4,5 Treatments for frozen shoulder include shoulder exercise, manual therapy, corticosteroid injection, manipulation under anesthesia, and arthroscopic capsular release. 1,4 –6 Some studies described that frozen shoulder was resolved in 1 to 3 years, while others showed that 20% to 50% of patients suffered from some degree of pain and range of motion limitation for up to 1 decade even when Western medical treatment was applied. 2,5,6 In fact, this case series shows that the patients had been suffering from shoulder pain for a long time even while receiving Western medical treatment such as shoulder exercise, manual therapy, and corticosteroid injection.
Kampo, a traditional Japanese herbal medicine based on traditional Chinese herbal medicine, has been used for the treatment of not only pain but also many diseases in Japan. 7,8 Nijutsuto is a Kampo formula used to effectively treat frozen shoulder. 8 –10 We have prescribed Nijutsuto for almost all patients with frozen shoulder refractory to Western medical treatment in our clinical daily practice.
We briefly reported the effect of Nijutsuto on pain intensity of frozen shoulder in our previous survey report, 10 so we thought that we should elaborate on the effect of Nijutsuto not only on pain intensity of frozen shoulder at rest and while moving but also on shoulder active range of motion in a case report of more patients because not a few patients suffer from refractory frozen shoulder. However, we understand that there are several limitations to this study; the present report is a retrospective and still small case series and a nonrandomized control analysis of Kampo treatment. We need a prospective and comparative study that might be more appropriate to support predictive, preventive, and personalized value of Kampo treatment. However, Nijutsuto combined with a 20-minute exercise program improved pain intensity in 13 patients with frozen shoulder refractory to Western medical treatment for a long time. Thus, we postulate that Nijutsuto should be tried for refractory frozen shoulder.
In conclusion, Nijutsuto combined with a 20-minute exercise program improved pain intensity and shoulder function in 13 patients with frozen shoulder refractory to western medical treatment.
Footnotes
Acknowledgments
The authors would like to express their gratitude to Matthew McLaughlin for assistance as language editor.
Author Contributions
Y-CA conceived of the study, participated in its study, and conducted all experiments. Y-CA, MI, HS, YO, TM, KS, MCN, TK, TI, and SI conducted the acquisition of data. Y-CA helped draft the manuscripts. All authors read and approved the final article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
We obtained approval from the Ethics Committee of Aichi Medical University (reference number: 13-097).