
Abstract
Early medical school development in the United States was considerably more robust than is usually appreciated. Most histories include only that portion of medicine known as regular or allopathic medicine. To fully understand developments in the country, it is necessary to include the various medical sects that developed in the country in the early 19th century. It is also important to realize that the impetus for medical school development came not from established academic institutions but from the medical community itself. Medical schools in the United States developed at a time and place that hospitals, as we know them, did not exist. The melding together of the preceptorship (apprenticeship), didactic lectures, demonstrations, and clinical/hospital experience evolved slowly. The move from heroic medicine occurred somewhat reluctantly as in Europe. In the United States, in contrast to the situation in Europe, the majority of medical practitioners were called “doctor.” The development of medicine and medical education is usually discussed as a progression of knowledge. It has been fashionable to ignore the development of the various medical sects. Even within regular medicine, no uniformity of thought existed by this time. The American Medical Association was born of this. Change within a segment of society always reflects, and is reflected by, change in society at large. The rapid increases in geographic area and the huge population growth must be understood. Times changed as the character of the population changed. Perception of gender and freedom were important aspects of this change. A number of prominent African American physicians also emerged.
Part 1
Introduction
Early medical school development in the United States was considerably more robust than is usually appreciated. Most histories include only that portion of medicine known as regular or allopathic medicine. To fully understand developments in the country, it is necessary to include the various medical sects that developed in the country in the early 19th century. It is also important to realize that the impetus for medical school development came not from established academic institutions but from the medical community itself.
Medical Schools in the Pre–Civil War Era
The first physician in the colonies was Dr Laurence Bohune who arrived in Virginia in1610 as physician for the London Company. The first physician in New England was Dr Samuel Fuller who arrived on the Mayflower in 1620. 1 These and other early physicians were practitioners who had received their training in Europe. (It is unlikely that they were medical school graduates but had probably been trained as surgeons.) Early efforts at medical education in the colonies involved a preceptorship, at first very informal but becoming increasingly formal. The student worked with a practicing doctor and saw his patients with him. Formal articles of apprenticeship with all duties delineated were signed and dated by both 2 (see Table 1 ). As might be imagined, this relationship also involved doing various errands, including cleaning the office and chopping wood. The preceptor also usually provided at least some textbooks as well (with the rarity of books at this time, this was an important consideration). A degree was not required to practice and was not obtainable in the colonies, and many simply started practice after 2 to 5 years of apprenticeship. Those who were really interested and could manage the expense ultimately went to Europe to attend schools there. Probably the largest number of these went to England and Scotland because of the language, although increasingly, Paris was a destination.
Addendum: Copy of an Early Preceptor Agreement

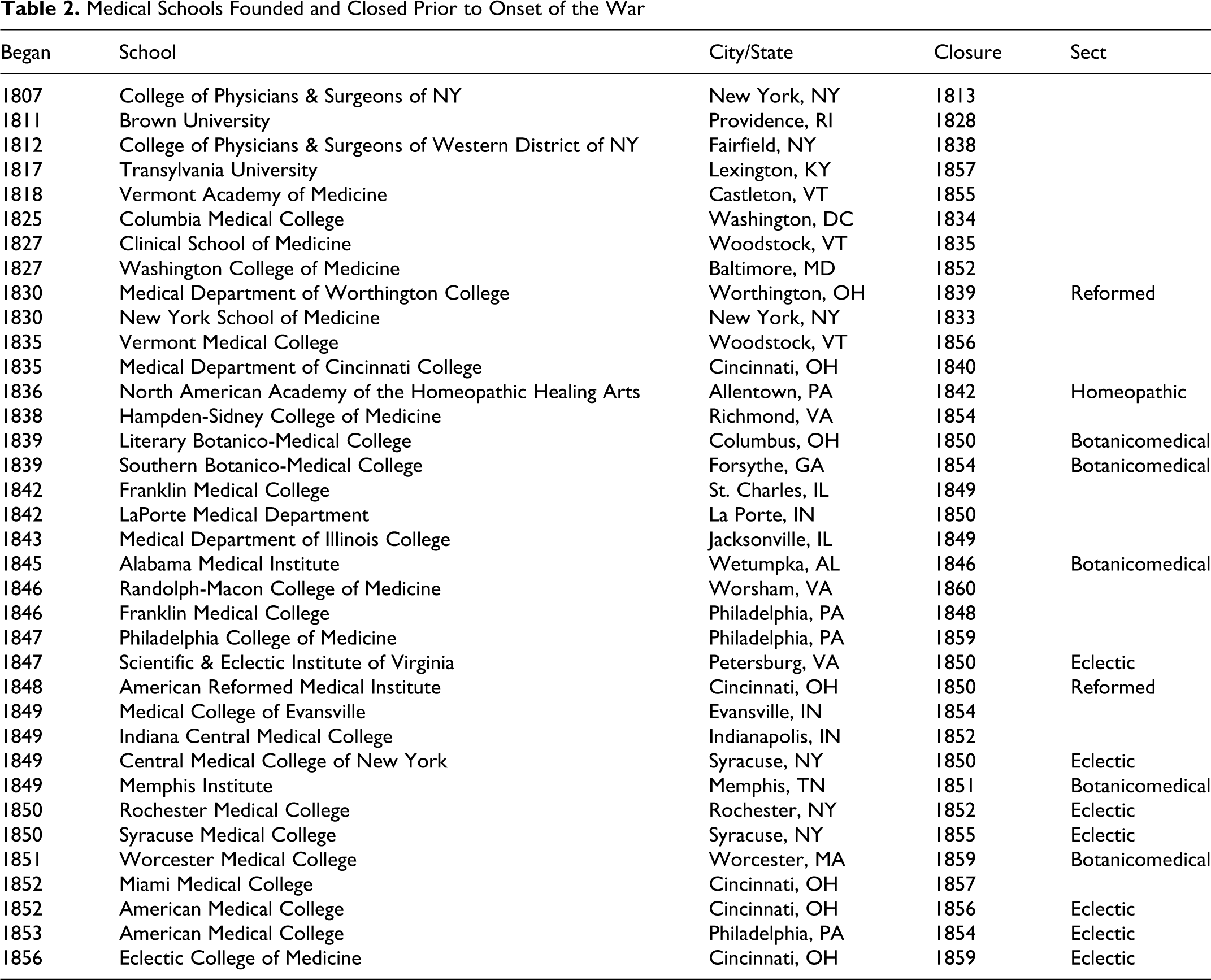
First efforts at formal medical education in the colonies began with preceptors giving lectures on various subjects to multiple students, first just to their own students but then to other students as well. The first medical school in the colonies was founded by John Morgan (Figures 1.1 and 1.2) in Philadelphia in 1765 as the Philadelphia College of Medicine. 2–5 These lectures were conceived initially as supplementary to the preceptorship and were coordinated with it. 2,6 This school ultimately underwent a name change to become the University of Pennsylvania. Kings College in New York City was the next school started in 1767. Only these 2 schools had begun prior to the Revolutionary War. Two more schools, both in New England, were started before 1800: Harvard Medical School in Cambridge, Massachusetts, in 1782 7 and Dartmouth Medical School in 1797 in Hanover, New Hampshire (Table 2 ). 2–4 The College of Physicians and Surgeons of New York was started in New York City in 1807. In 1813, this was merged with Kings College to become Columbia University College of Physicians. Because of the shortage of anatomical subjects and clinical patients, Harvard Medical College moved to Boston in 1810. 7

John Morgan, MD: He was the central figure in starting the Medical College of Philadelphia that became the University of Pennsylvania. He was also the first Surgeon General of the Continental army (courtesy of the National Library of Medicine, Bethesda, MD)

William Shippen, MD: He worked with Morgan in setting up the University of Pennsylvania. He was George Washington’s choice for replacement of Morgan as Surgeon General of the army
Medical Schools Founded and Closed Prior to Onset of the War
In 1807, the first medical school in the South was started in Baltimore, Maryland, when a group of professors obtained a state charter from the Maryland Legislature (Figures 1.3 to 1.5). 5,8,9 This charter was needed because of the strong antivivisection activity in Baltimore. An additional 10 schools had opened by 1820, including 2 west of the mountains in Trans-Appalachia: the Medical Department of Transylvania University in 1817 (the university itself had been started prior to 1800) in Lexington, Kentucky, as the first medical school west of the mountains and the Medical College of Ohio in Cincinnati, Ohio in 1818 (Table 3 ).
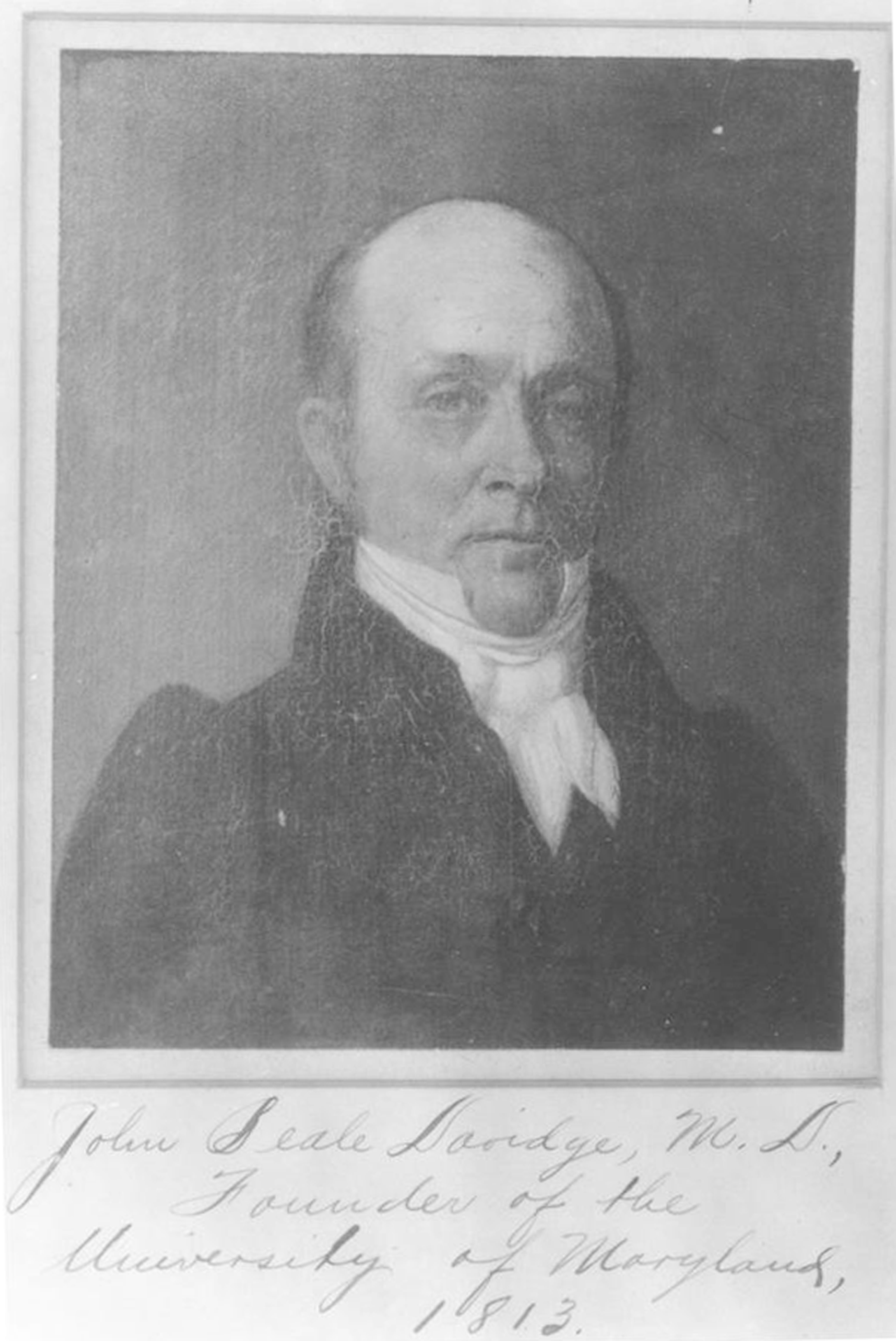
John Beale Davidge: He was founder and first dean of the University of Maryland School of Medicine and responsible for the planning and building of Davidge Hall (courtesy of the Medical Alumni Association of the University of Maryland, Baltimore, MD)

Davidge Hall, opening in 1812, was the first building in America built exclusively for medical education. It has been in continuous use since that time. This picture (circa 1850) is the oldest known photograph of the building (courtesy of the Medical Alumni Association of the University of Maryland, Baltimore, MD)

Davidge Hall in February 2002 (courtesy of the Medical Alumni Association of the University of Maryland, Baltimore, MD)
Medical Schools Open at the Beginning of the War


Then, 11 schools opened from 1821 to 1830, with 14 additional schools by 1840 together with the first of several sectarian schools, the Literary Botanico-Medical School at Columbus, Ohio in 1839. (As discussed later in this series, various dissident groups of practitioners existed at this time. Because such groups were a definite minority, they were called “sects” by the dominant majority of regular, or allopathic, practitioners; Table 3). 2,10 The 1830s also saw the closing of several medical schools (note the appropriate dates of founding and closure in Table 2). Some of these were closed permanently, whereas others were closed by internal strife and reopened almost immediately under a different name or under the auspices of a different college. 2,10
Through 1860, a total of 99 medical schools, including 31 sectarian schools, had opened in the United States. 2,10 This included the Medical College of the Pacific in San Francisco, California, founded in 1858 as the first West Coast medical school. 2 The inclusion of the sectarian schools, usually ignored by traditional medical historians, is important. These schools provided a large number of the medical practitioners for several decades after the war. 10 The superiority of regular medicine still lay, to some extent, in the general education of its leaders rather than in any therapeutic advantage. 11 A total of 36 medical schools had opened and closed prior to 1860 (Table 2), some with very short lives, although Transylvania University was open for 40 years, with large numbers of students for 30 of those years. A very slow period followed the opening of nearby Louisville, Kentucky. Transylvania University finally closed in 1857 as competition from the close neighbors with better clinical resources in Kentucky and Ohio forced the issue. At the onset of the Civil War, there were 63 medical schools open in the United States (Table 3). 2–4,10 This total comprised 47 allopathic, or regular, medical schools and 16 sectarian medical schools. Of these, 23 schools were in 10 different southern states; 16 of these schools were in states that subsequently seceded from the Union. All but one of the schools in the states that seceded closed with the advent of the war. Only the Medical College of Virginia in Richmond, Virginia, remained open after 1861. 2,12
Medical School Ownership
The majority of medical schools were owned by the teaching faculty, who were paid directly by the students. Not until after 1860 did the University of Michigan and one or two other state institutions begin to pay salaries to medical professors in the German manner. 11 It is customary today to castigate proprietary medical schools and the faculty who owned them. As previously stated, the medical needs of the burgeoning population, spread over a large geographic area, could not be met by the existing medical schools. Inevitably some of the new schools were started as a road to financial gain for a few. These schools also advertised shortened courses and decreased time to a degree. Both series of lectures were actually offered in the same year at some schools. It has been stated frequently that such ownership constituted a conflict of interest on the part of the faculty and induced them to accept more students than the facilities could reasonably accommodate. This influenced decisions against improvements in the quality of education, such as longer lecture sessions, more years of training, and graded classes. 13,14 This last charge undoubtedly is true, but it is only part of the issue. It is definitely true that few professors ever became wealthy in the medical schools. In fact, the records show that the faculty, often from their own pockets, provided money for library facilities and for anatomical and pathological specimens and models. 14 The faculty at Maryland had actually started a hospital to provide adequate patient experience for students. 6,8,9 It must also be stated that had a proprietary system not existed, few schools would have emerged until much later. Very little funding was forthcoming from the various colleges whose names and degree-granting capabilities were used. In fact only limited public or privately donated funding was made available, and even when outside funds were found, they were never sufficient to finance a school.
Part 2
Introduction
Medical schools in the United States developed at a time and place in which hospitals, as we know them, did not exist. The melding together of preceptorship (apprenticeship), didactic lectures, demonstrations, and clinical/hospital experience evolved slowly. The move from heroic medicine occurred somewhat reluctantly, as in Europe. In the United States, in contrast to the situation in Europe, the majority of medical practitioners were called “doctor.”
Medical Training
The number of students who actually enrolled at this time is in question because many schools inflated enrollment numbers for promotional purposes. Specific school enrollment varied from only a few to more than 400 students attending lectures. 6 Attempts were made to equate numbers to quality, although the opposite was often true. The country was growing rapidly in both size and population. The total population in the country increased 6-fold from 1800 to 1860, going from 5 300 000 to 31 400 000 people. 1 The established schools, usually in the East, no longer provided the needed numbers of practitioners for this new expansion. The rapid birth of new schools in the West and the South attempted to meet this need. The population in the West (Midwest by current terminology) increased from 51 000 in 1800 to 9 097 000 by 1860. 1 Regional differences mattered, and it is documented that in 1859, more than 300 students left Philadelphia in protest against John Brown’s raid and returned to Southern medical schools. 2
The requirements for the degree of Doctor of Medicine in these early years was somewhat uniform, although there were exceptions. A candidate had to have completed 2 years of classes and 3 years of preceptorship and be 21 years of age. 2,13,15,16 Although initially some preliminary education was required, this was gradually reduced to knowledge of Latin and Greek and evolved to no requirement beyond secondary school. However, many did have some college experience. Waite 16 found that at one New England school, as many as 15% or 20% had some college attendance. Hudson found that 35% of “imminent” physicians had a college degree prior to 1830, and this increased to 50% by 1870. 17 Still, it is clear that this was not true of the majority of students. With very few exceptions, there was no entrance requirement beyond secondary education. The term of classes each year consisted of 16 weeks only, and the second year was a repeat of the first. The classes were totally nongraded—that is, all were given simultaneously without prerequisite. The historian, Waite, 16 describes the process in Ohio in the 1850s, stating that a student spent about 30 weeks in classes and 124 weeks in preceptorship, thereby emphasizing the great importance of the clinical experience (preceptorship) in the education process. Waite stresses this fact because it is commonly stated that the preceptorship had decreased in value in later years and was not essential to the degree process. As the medical school lectures started to supplement the preceptorship, so the regularly scheduled lectures from the medical school came to be supplemented by those knowledgeable in a subject not covered in the formal school lectures. These informal lectures covered a large variety of subjects.
The route to a degree was long and expensive, particularly as a partially trained practitioner could still earn more than a laborer or a teacher. Many started practice with minimal preceptorship and/or minimal attendance at medical school. Only between 25% and 40% of medical school attendees ever graduated. 6,18 In 1830, probably no more than 40% of practitioners had medical degrees. 19 As late as 1850, as many as 25% of physicians had no degree. In fact, in some states, practitioners in homeopathy and the botanicals were exempted from requirements for degrees or licensure by state law. 20
The majority of schools had 6 to 8 professors who gave lectures on the subjects they covered. 2 Table 4 shows the list of subjects at the University of Maryland in 1840. This is typical of the times. 21 Groupings in the table indicate that the lectures were given by the same professor. Not all subjects were covered at all schools.
Subjects Taught at the University of Maryland in 1840 a
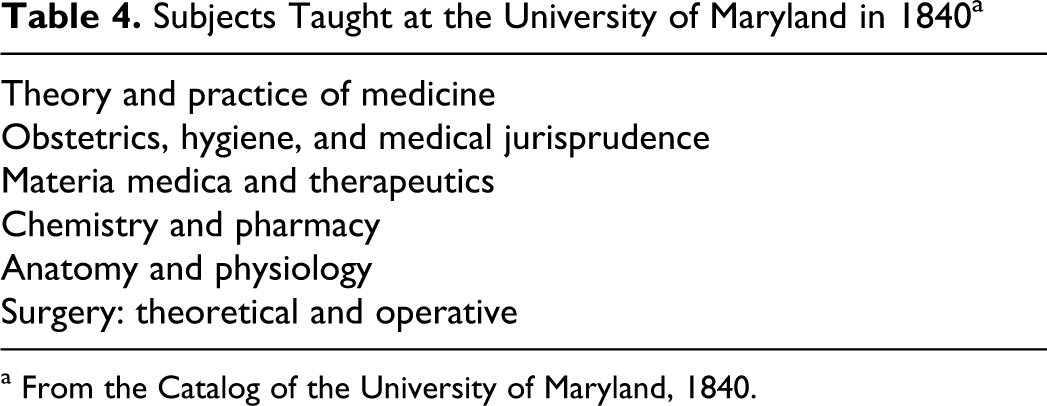
a From the Catalog of the University of Maryland, 1840.
A demonstrator in anatomy (the individual who actually performed the dissection and explained the process to the class) was also soon included, and so anatomy was the first laboratory course introduced into medical education. 2 For a long time, it was the only one included. There were changes in subject matter over the years and lectures were added in pathology, medical jurisprudence, obstetrics and women’s diseases, and diseases of children. Botany was required at most schools until into the 1860s. By the end of the period, many schools also included Ophthalmology. Lectures were given in each subject 5 days a week with exams usually given on Saturdays. Schools with adequate numbers of anatomical specimens such as Maryland also required attendance at anatomy lab with demonstration dissections by the demonstrator and by the students themselves. 21 These dissections were usually done in as short a time as possible because of the decomposition of the cadaver in those days with neither preservatives nor adequate refrigeration being available. The requirement for an anatomical laboratory was not universal, and at least 4 schools did not require this for graduation. Students at schools with hospital facilities also had to spend time in the hospital. 2,6
It has been noted that the average medical student at this time tended to be older than students at liberal arts colleges and law schools, although no actual tabulation of ages has been found. This is thought by some to be a result of the relatively high cost of medical education even then. 2
The quality of education in the various medical schools was extremely variable. 2,6,10,14 The most variable aspects of this were the experience in anatomy and in clinical/hospital experience. The attitude of the medical schools to hospital attendance was also variable. In part, this related to availability. In response to the 1849 survey of the newly formed American Medical Association, a variable answer was received. Of 33 respondents, only 8 reported hospital attendance as mandatory; 12 respondents had no hospital attendance requirement at all. 15 Many students entered private practice with the preceptorship as the only route to bedside instruction. As stated above, some schools did not require a ticket in anatomy for graduation, whereas other schools provided extensive experience, both with a demonstrator and with individual student participation. It is true that dissections were somewhat hurried because of the lack of preservation or refrigeration facilities. Some schools also had dissection with dogs as subjects. The issue of availability of anatomical subjects had been the cause for obtaining a state charter for the University of Maryland. It also became the direct cause of the closure of several small country schools. In several instances, charges of grave robbing were made, and in at least 2 instances, the locals actually raided the school to obtain the body. 2,10,15 In 1 case, the school building was destroyed by fire, and in another, 2 people, a student and a professor, were killed.
One of the largest differentiators of medical schools was the availability of medical school–related clinical experience. Schools in cities with large hospitals usually were able to develop a relationship with the hospital so that students could be with the patients. When multiple schools existed in a city, there was competition for the hospital. Smaller and newer cities usually did not have adequate hospital facilities. In this instance, clinics were developed, although patient contact was often limited to that of the preceptorship. These were known as “country” schools in the competition for students. This difference between the so-called “city” and “country” schools had been the reason for Harvard’s move from Cambridge to Boston in 1810. 7 It was one of the causes of the closure of Transylvania University. Many of the small country schools in New England, New York, Ohio, and the Old Northwest just did not have adequate clinics. The faculty at the University of Maryland actually started a hospital in 1823, so that their students might have an adequate exposure (This hospital was taken over by the medical school in 1830). 8,9 Students at the University of Maryland and the University of Pennsylvania, for example, had a required hospital attendance. 2,3
Although surgery was a major subject in the schools very early, it was not as known today. The subject was taught by means of lectures. Few operations of any sort were ever done by medical students. Operations done by students consisted of bloodletting and cupping. Certainly, less than 1% of physicians had ever done any other operation by the time of graduation from medical school. The schools and the hospitals had large amphitheaters where the operation was done by the attending physician with students gathered around, often in large numbers and without personal participation. Most of the operations done were bloodletting, lancing of boils, blistering, and dressing of injuries. An occasional amputation was done. 2
The student contact with the patients and responsibility for their care was extremely limited in many cases. It needs to be emphasized that hospitals were used largely by the poor, the insane, and elderly relatives of the wealthy. The majority of patients were actually treated at home, with physician or surgeon attendance there. In many hospital settings, the student simply followed the attending physician during his daily rounds. The attending physician talked to the patient, examined the patient, and gave orders for care. When a hospital facility was not available, a stronger reliance on the preceptorship was necessary. 6,16 Additional lectures were given by many to supplement the regular medical school lectures, and these covered a wide range of topics, often with patients present as examples. 2,6 An occasional medical school even arranged for student participation at childbirth. 21 It is clear that in many schools, including Harvard, modern techniques of auscultation and percussion, including use of the stethoscope, were included in the clinical instruction. 2,22 The University of Maryland started a required class in physical diagnosis, including percussion and auscultation in 1845. 23 In 1854, Maryland added a course in microscopic histology; in 1860, students were provided with microscopes, and specimens were provided for study in 1861. 23
There were, of course, exceptions to the general rule. The University of Virginia was established initially with a 9-month program. 12 It stayed this length, although it did not have large numbers of students. In 1849, the University of Michigan began with the requirement of 6 months of lectures for each of 2 years, together with the 3 years of preceptorship. 2 The most impressive exception is New Orleans College of Medicine established in 1856. 2,6 It not only required attendance at 9 months of lectures each year but also required students to interview, examine, diagnose, and present the patient to the attending with treatment recommendations and follow the patient to discharge. This school closed at the beginning of the war. Such clinical clerkships were not reinstituted until the late 1880s.
Cost of Medical Education
It was customary in proprietary schools for the student to buy individual course tickets from the professor involved. These usually cost $15 to $20 a year for a total of $90 to $120 a year for tuition. This money was paid directly to the professors in most cases. Operating expenses for the school were shared. Even at Harvard when it opened, professors' salaries were the amounts paid for the lectures. 7 In addition, there was an initial matriculation of from $10 to $30 and a graduation fee that was usually $20. There was also an anatomy laboratory fee—usually $20—and attendance at the associated clinic or hospital often cost an additional $100 for a year. These fees did not include living costs, and these varied more widely than did the tuition costs. In general, room and board was $1.00 to $1.50 a week, although in some cities it could reach $3.00. 2
It should not be assumed that preceptorship was free. In fact, near the end of this period, it usually cost about $100 a year. It was often possible for the student to provide some additional work to pay for room and board during this time. It is possible that many preceptors worked to keep the preceptorship long because of this monetary advantage to them.
In tabulating the total cost of medical education then, we must add all these factors together (see Table 5 ). When a clinical or hospital rotation charge is added, the total cost then increases to $788. This total could be as high as $1250 at some of the city schools. Either amount was a large sum of money to be accumulated at a time when the annual income for a physician seldom surpassed $600 a year. 24 A factory laborer earned about $360 a year, whereas a farm laborer earned about half of that sum. Unless one’s family had money or the person had a good loan source, it took several years of parsimonious living to save the required amount of money. It must be remembered that there were no guaranteed student loans or tuition grants available. It would also explain why several students attended more than 1 school with time between medical school courses. It also makes it easier to understand why so many people went into practice without obtaining a degree 25 or even without attending medical school, particularly because it was possible to call oneself a doctor with no education at all and because no licensing was done in many states. Most of those states that required licensing in some form in the early years of the 19th century had repealed this requirement by 1850 (Figures 2.1 to 2.5).
Typical Cost of Medical Education (Medical School Attendance for 2 Years)


Oliver Wendell Holmes, MD: He taught the use of the stethoscope and microscope with physical diagnosis. He was dean of Harvard Medical School in 1850 (courtesy of the National Library of Medicine, Bethesda, MD)

Samuel Gross, MD: He was a prominent surgeon at the outset of the war and wrote A Manuel of Military Surgery in 1861 (courtesy of the National Library of Medicine, Bethesda, MD)

Joseph Jones, MD: While a professor at the Medical College of Georgia, he did extensive temperature measurements with the clinical thermometer for various fevers (courtesy of the National Library of Medicine, Bethesda, MD)

Nathan Ryno Smith, MD: While a professor at the University of Maryland, he provided subjects for anatomical dissection to several other medical schools (courtesy of the National Library of Medicine, Bethesda, MD)

William Hammond, MD: During his short time out of the Army Medical Service, he served as a professor at the University of Maryland School of Medicine in 1860 (courtesy of the National Library of Medicine, Bethesda, MD)
Part 3
Introduction
The development of medicine and medical education is usually discussed as a progression of knowledge. It has been fashionable to ignore the development of the various medical sects. Even within regular medicine, no uniformity of thought existed by this time. The American Medical Association was born out of this situation.
Dissent and Division in Medicine
One of the notable elements of the early medical schools and medicine in general was the contentiousness of the practitioners. Few medical schools existed for more than a few years without a major conflict between faculty members. These disagreements were often marked and divisive and very, very public. It became common for articles and letters to appear in medical journals and newspapers filled with pointed acrimonious remarks concerning the opponents of the author. In fact, this very contentiousness was summed up by one editor in 1857 26,27 : “It has become fashionable to speak of the Medical Profession as a body of jealous, quarrelsome men, whose chief delight is in the annoyance and ridicule of each other.”
This public arguing helped undermine public confidence in medicine and physicians. This attitude was responsible for the demise of many medical schools, with the principals often leaving to start a rival school nearby. One well-respected medical educator of the time, Daniel Drake, was instrumental in starting several such schools and, certainly, was known for his “independent” attitude. 10,28,29
In addition to the contentiousness among the traditional medical practitioners, there also appeared on the scene several medical sects and philosophies that seriously challenged the dominance of the traditional medical practitioners. 5,13,24,26,27 These were Thomsonianism, 30,31 botanicomedicalism, homeopathy, and eclecticism. 32 The common denominator in all these sects was a strong opposition to the use of “heroic” medicine. 33–36 This was echoed by rising demands from the public for a kindlier medicine with less harsh treatment of disease by doing away with bloodletting and the use of mercury compounds such as calomel purges. 24,37,38 By the 1840s, Thomsonianism, a basic herbal medicine approach, had faded away, although botanicomedicine was an outgrowth of it. 24 The other 3 sects actually started medical schools and made significant inroads into medical practice. 10 Homeopathy involves the use of minute amounts of drugs to cause symptoms similar to the disease in a healthy person (the opposite of this is allopathy as regular medicine was called by them). The American Medical Association passed a resolution opposing homeopathy in 1855. 39 Eclecticism was the descendant of Thomsonianism and had moved even closer to allopathy than botanicomedicalism. It shared the aversion to “heroic” therapy but had no basic philosophy of its own. 5,13 It was similar to the approach that had been formulated by Louis in Paris after he demonstrated that calomel and bloodletting were not beneficial but actually harmful. 40,41 These last 2 sects comprised about one tenth of the physicians in the United States in 1860. 5,13 After 1840, it became increasingly difficult to differentiate between the different medical sects. This was both because of the rising pretensions of the sects and the falling pretensions of the regulars. This corresponded to the decline of premedical education in medicine in both the United States and England.
Movement for Change and the American Medical Association
Efforts to improve the system and quality of education were ongoing. The non-degree-granting schools of supplementary medical lectures that emerged were an improvement. 6,12 This increased the knowledge base in subjects not included in the formal medical curriculum. Some schools developed requirements for hospital attendance, but this was true in only a small number of cases. Subjects were added and changed in the degree schools. By 1840, most schools included medical jurisprudence. Obstetrics was added and expanded to include women’s diseases. Diseases of children was also added, as was ophthalmology. 2
Efforts were made to incorporate the newer clinical advances and approaches from European schools, particularly Paris. The thermometer, the stethoscope, the microscope, and hygiene were added to some curricula. Calls were made to increase the number of subjects and the material covered in lectures. This meant extending the lecture year to 6 or 9 months or increasing the number of years. Demands were made for better clinical and bedside teaching as a formal part of medical school.
Oliver Wendell Holmes, the poet, physician, and medical educator, complained bitterly that American medical literature was simply a rewrite of European literature with little American contribution to the literature. 42 Gross reiterated this criticism in 1856 and admonished physicians to use their own patients as case material for articles. 39 In truth, research had little role in American medical education, and few faculty members were engaged in research at this time. Joseph Jones from Georgia is an exception to this, although he was slow to publish the results of his work defining different diseases, including detailed temperature measurements. 43 This lack of research involvement may well have been a result of the proprietary nature of the schools and faculty as charged. It may also simply have been a consequence of the times in America.
As early as 1835, Paul Eve and the faculty of the Medical College of Georgia called for a medical convention to consider improvements in medical education. 2,39 There was no response from the Northern schools. A convention was held in Columbus in 1838, but no practical changes followed. Nathan Davis from New York did organize a meeting in 1846 with designated delegates from 16 states who then organized a meeting in 1847 with 250 delegates. This was the beginning of the American Medical Association. 14,39
This first meeting proposed setting entrance requirements, including the demonstration of an education beyond the usual public school, certifying preceptorship, and instituting the requirement of 3 years of lectures of at least 6 months a year. It also gave a list of required subjects, requiring clinical instruction and required attendance by students. Although today these appear sound, there was much resistance at the time and not always for monetary reasons. 44 The medical faculty from Harvard (including Holmes) was opposed to this and published a statement in 1849. 45,46 They stated that what was needed was more study by the student and more private instruction including patients. They felt that there was no need for more didactic lectures. Similar arguments were made by the faculty of the University of Pennsylvania. 5 Others objected that adoption of the recommended medical school entrance requirements would severely limit the number of eligible students because only the elite secondary schools and private academies provided the courses required. 13 The majority of schools would have to close because of lack of students. The few remaining schools would not provide anywhere near the number of physicians needed by the country. Change needed to start in the lower schools, and this was not practical at that time. Parenthetically, none of the colleges in the country required the level of secondary schooling that the American Medical Association was suggesting. 13
One can certainly ask what the role of this preliminary education was to be. The sole issue seems to be the raising of the prestige of the medical profession, as in Europe. Little science other than mathematics was taught in the liberal arts colleges of the time. Most of the science of the day was actually taught in and around the medical schools. 2 Liberal arts colleges in the United States still emphasized a classical education with philosophy, Latin, and Greek. 2,47 Early technical schools, even when sponsored by a college, were not considered part of the college, and technical faculty did not have the status of college professor.
Very little change in medical education was made prior to the beginning of the war. One exception was that already mentioned with New Orleans School of Medicine, and this school closed at the beginning of the war. Several schools, including the Medical College of South Carolina and the University of Buffalo, experimented with extended terms but rejected them. 5 Penn Medical University (an eclectic school) announced progressive (graded) courses in 1854. Then, 5 years later, Lind University (the future Northwestern Medical School) introduced a 3-year graded curriculum with 6 months of lectures and annual tests in each subject. 11 In 1858, Harvard introduced a 3-year graded program (but only as an option) and the requirement of a multiple-member oral final exam for all graduates (Figures 3.1 to 3.5). 48

William Cullen, MD: He was a professor of medicine at the University of Edinburgh in Scotland in the 1700s and was responsible for bringing back the Greek concept of “heroic medicine” (courtesy of the National Library of Medicine, Bethesda, MD)

Benjamin Rush, MD: Thought by many to be the father of medicine in the American Colonies, he was a pupil of Cullen at Edinburgh, a strong proponent of “heroic medicine,” and believed that all diseases had only 1 cause (courtesy of the National Library of Medicine, Bethesda, MD)
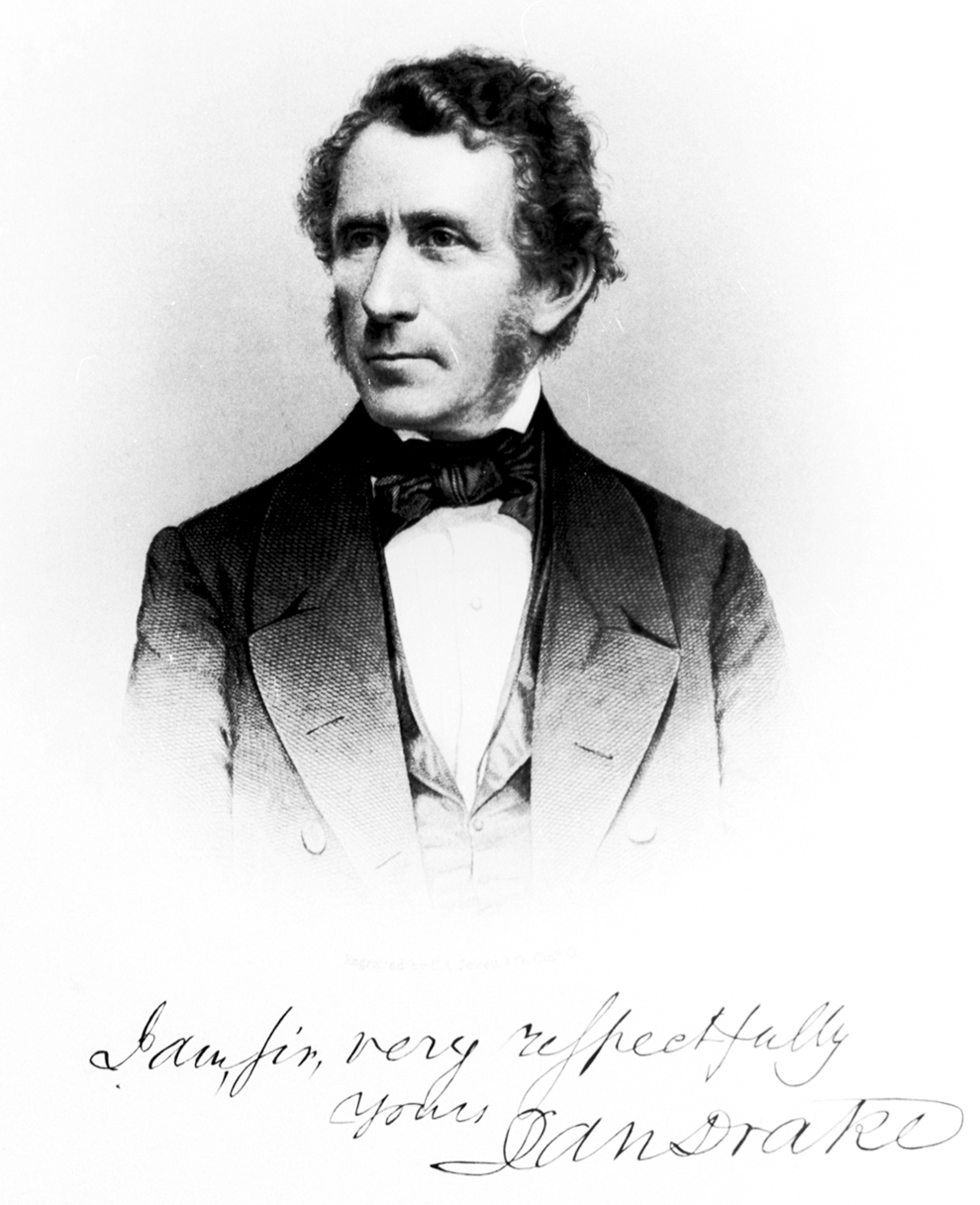
Daniel Drake, MD: This man was an early educator who was responsible for the founding of several medical schools in the West. He was also known for his contentious nature (courtesy of the National Library of Medicine, Bethesda, MD)

Paul Fitzsimmons Eve, MD: This professor from the Medical College of Georgia was an early advocate of an organization to improve the quality of medical education and the status of the profession (courtesy of the National Library of Medicine, Bethesda, MD)

Nathan Davis, MD: He organized the 1847 meeting that culminated in the formation of the American Medical Association (courtesy of the National Library of Medicine, Bethesda, MD)
Part 4
Introduction
Change within a segment of society always reflects, and is reflected by, change in society at large. The rapid increases in geographic area and the huge population growth must be taken into account in our analysis. Times changed as the character of the population changed. Perception of gender and freedom were important aspects of this change. A number of prominent African American physicians also emerged.
Advent of Women in Medicine
The 1840s saw another change within the medical profession. This was the unexpected movement of women into medicine. The origin for this was the feminist movement that was particularly active in the United States—another sign of the feelings and desires for equality. 49 The chief argument for this was that of abstract justice, but both sides also appealed to Victorian sentiment, each in a different way. 47 Advocates insisted that women should have the services of their own sex in matters of delicacy, particularly obstetrics and gynecology, and women were not satisfied professionally with the role of midwife. This argument was actually put forth by men as well, and Samuel Gregory 5 was active in this regard. Most men, and probably most women, were still opposed publicly to feminism. 49 Women as such were held to be unqualified, mentally and physically, for the tasks of medicine (although they were the principal givers of medical care at home). The woman’s sphere was the home and to remove her from this was both indelicate and dangerous. 5,47,49
A few women persisted, however, and in 1849, Elizabeth Blackwell became the first female medical graduate in the United States when she graduated from Geneva Medical College. 2,5,49,50 The number of female medical graduates grew, although few women were admitted to regular medical schools. The sectarian schools (eclectic and homeopathic) encouraged the matriculation of women. The Female Medical College of Philadelphia opened in 1850, and the New England Female Medical College opened in Boston in 1852 (both were initially eclectic schools) as the first women’s medical colleges. 2,10 By 1861, at least 200 women had obtained medical degrees in this country.
Medical practice for women was primarily, but not restricted to, women, although there was a wider acceptance among immigrant groups. Within the professional community at large, acceptance remained a problem. This advent of women was adamantly opposed by organized medicine, including the newly formed American Medical Association. 47,49 Membership in the various professional medical societies was withheld for several decades.
African American Physicians
Although traditional medical histories do not mention it, a number of African Americans rose to prominence in medicine in the United States prior to the Civil War. Detailed precise information is not available about many of these men. There were no newspapers or journals dedicated to these groups. 51 About 1800, a slave known only as Caesar 52 became known for his treatments for poison and snakebite. In fact, as a reward, the South Carolina Legislature bought his freedom. The earliest known African American graduate of a medical school was James McCune Smith, who received a medical diploma from the University of Glasgow, Scotland, in 1837. 51–54 The first such graduate of an American school was David J. Peck, who graduated from Rush Medical School in Chicago in 1847. 52,53,55 In all, 12 different medical schools granted degrees to more than 20 African Americans. Several others have been identified, born slave or free, who practiced by apprenticeship or received degrees from American or Canadian schools.
The Country and the Time, 1830 to 1860
It must always be remembered that this was a very dynamic time in the United States. Rapid change was the rule. The geographic boundaries of the settled areas were changing rapidly as wilderness became organized territory and territories became States. There was at the same time a gigantic influx of people into the country as a whole. 1 Huge numbers of people immigrated to the United States from Ireland because of the potato famines and political unrest. Similar numbers arrived from Germany because of famine, and political unrest and civil war there. Although lesser in number, there continued to be significant immigration from England as well. These groups swelled the populations in the cities, particularly the slums. They filled the cities to overflowing point and then followed the native populations west.
Politically, the country itself was unsettled. The issue of slavery, that “peculiar institution” of the South, was becoming more central in national controversy (the issue of secession had already been raised by South Carolina in the 1830s). 56 Many factions were developing from all sectors of the country. A growing segment of “native Americans” resented the waves of immigrants. The settlers in the Far West (the Midwest of today) resented the control of the country by the more populated East. Cities were developing problems that were very different from those in rural areas. Resentment was also building in the South toward the more industrialized North. At the same time, the rate of increase of the white population in the South was substantially behind that in the rest of the country. 1
The most nearly universal demand was the demand to be “free.” To most, this meant freedom to do as they pleased without governmental control. The government was only required to provide police protection and a stable economy. The people wanted no protection except for the freedom of inquiry and freedom of action. This antagonism to control had caused the revocation or lack of enforcement of medical licensing laws in the majority of states in the 1830s and 1840s. 3,57 Most of the laws regulating legal practice had also been repealed during this same period. 11,57 This is certainly a marked contrast from how medicine is practiced today.
Education and/or freedom from it were part of this freedom. The spirit of the time moved the West away from established schools. Few saw either the need for or benefit in higher education. It has frequently been noted that the education level of physicians had gone down in this period as shown by the decrease in entrance requirements and liberal arts education among them. In the 1840s and 1850s, the status of physicians in society changed. 5,57 The Northern professionals became victims of the industrial revolution. This included physicians. Medicine became increasingly commercial in keeping with the society of the time. The education level of physicians has been viewed as part of this commercialism, possibly more in retrospect than at the time. It should also be noted that the general level of education among state and national legislators was down, 14 probably as part of the reaction of equalitarianism and antiegalitarianism that developed. It should be emphasized that this lower education status applied at all levels. In 1800, 75% of lawyers in practice had attended law school, but by 1860, this number had fallen to 25%. 57 Prior to 1860, 6 presidents of the United States did not have college degrees. 56 In fact, the next 2 presidents (Abraham Lincoln and Andrew Johnson) had neither a formal education nor a college degree. This does not necessarily imply that these men were uneducated but only that they were not formally trained (Figures 4.1 to 4.4).

Elizabeth Blackwell, MD: In 1848, she become the first woman to receive a medical degree, not only in the United States but in the world (courtesy of the National Library of Medicine, Bethesda, MD)

James McCune Smith, MD: He was the first African American to receive a medical degree. He received a baccalaureate degree, then a master’s degree, and finally a medical degree from the University of Glasgow, Glasgow, Scotland, in 1837 (used with permission of the Moorland-Spingarn Research Center, Howard University, Washington, DC)
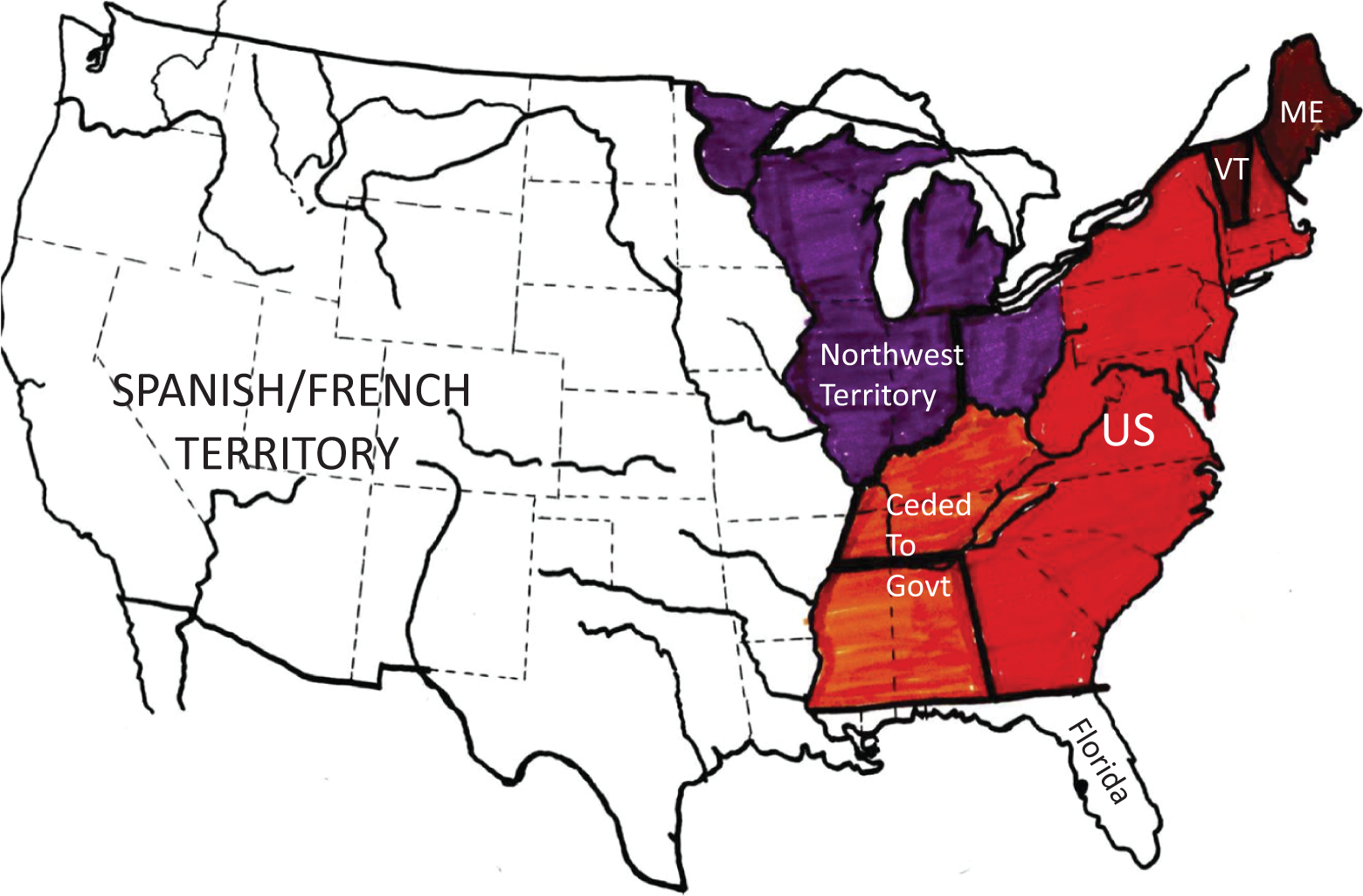
The United States in 1802: This map shows the small size of the country at this time. Although several states had been added since the revolution, a vast amount of territory was still unsettled. Only in the northwest did the country’s claimed territory reach the Mississippi River

The United States in November 1860: This map shows the westward growth of the country as the result of the Louisiana Purchase, a treaty with England, and the war with Mexico. This was the continental United States as it exists today, although vast areas were as yet unorganized. The organized states were polarized into “free” and “slave.” It should be noted that California and Oregon had chosen admission as “free” states. Also note that Maryland and Delaware were in the “slave” state block
Summary
Physicians as a group have always been considered conservative people. These physicians, as a group, were no different. Old attitudes and old ways change slowly in all people. The predominant approach to general education in this period was still the classics, philosophy, logic, and mathematics as it had been for generations. The approach to medical education was theoretical as it had been for generations. There was as yet little of the inductive approach of the new science. Observation in Europe had yielded new insights and facilitated diagnosis. But it had produced little improvement in cure.
It is certainly true that the disaster that occurred with the coming of the war was little helped by medicine as it was taught and practiced in the United States prior to 1861. This disaster was not primarily a result of a lack in the educational system. It was a result of the lack of knowledge in medicine in the world at that time.
The impact of disease in some cases might have been lessened with proper application of contemporary knowledge, but it is doubtful whether any major effect could have been obtained. Certainly the much-vaunted European system of education and medicine had done no better in Crimea in the mid-1850s or in northern Italy in 1859 (in fact the disease to injury ratio was substantially higher in those wars than in the Civil War in the United States).
The medical problems in the Civil War were not a result of the lack of medical education as such but the result of a lack of medical knowledge available in the world. It would take several decades for this required knowledge to be gained, developed, disseminated, and incorporated in medical practice for mankind to benefit.
Footnotes
Acknowledgment
This article was presented at the National Museum of Civil War Medicine Annual Medical Conference, August 2, 2002, in Shepherdstown, West Virginia.
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author received no financial support for the research, authorship, and/or publication of this article.