
Abstract
Background:
Produce Prescription Interventions (PRx) are designed to improve food insecurity and diet quality by offering greater access to healthy fruits and vegetables (FV) and nutrition and culinary education. This study evaluated the relationship between participation in a family-based PRx and child FV intake.
Methods:
Between November 2022 and December 2024, children (0–18 years) and caregiver dyads were recruited to participate in a 6-month PRx that provided 16 pounds of FV per month and virtual nutrition and culinary education sessions monthly. Adult-reported child FV intake data were collected at baseline and post-intervention. The effect of the intervention on child FV intake was evaluated by multiple mixed model regression analyses.
Results:
A total of 176 dyads completed an FV intake evaluation. Participation in the intervention was associated with a significant increase in fruit (R = 0.21, p = 0.004) and vegetable (R = 0.30, p < 0.0001) consumption. When adjusting for demographic and programmatic variables, the effect of time remained significant.
Conclusions:
These data support the hypothesis that PRx participation is associated with a modest improvement in FV intake, but barriers to FV intake remain. Further work is needed to understand the optimal PRx design to achieve healthy FV intake in children.
Keywords
Introduction
The rate of obesity in children and adolescents has steadily increased since 1980. 1 In 2020, the rate was 26.2% and 24.8% for Hispanic and non-Hispanic Blacks, respectively. 2 Healthy eating patterns, including fruits and vegetables (FV), whole grains, lean protein, and healthy fats, and minimal intake of ultra-processed foods are recommended by health experts to prevent the risk of developing obesity and comorbidities in the average population. 3 There is strong evidence that adherence to a healthy eating pattern in children is associated with lower risks of obesity 4 and metabolic disease 5 and better school performance and educational attainment. 6 However, many children in the United States do not meet these healthy eating recommendations, especially falling short on FV intake.7,8 In children and adults, household food insecurity (FI), defined as a lack of access to adequate food, 9 is associated with a lower intake of FV10,11 and poor weight and health outcomes, 12 suggesting that low-income and racial/ethnic minority populations need more effective and targeted interventions to improve healthy eating habits and prevent obesity. Early prevention efforts designed to improve access to healthy foods and diet quality in children may help reduce childhood and adult obesity and should be a public health priority. 13
Many factors contribute to child FV consumption. Barriers to FV intake include accessibility, cost, personal preferences, and perceived quality and availability, especially in low-income areas where there tends to be greater access to fast food than to fresh produce.14,15 Parental factors such as household income and purchasing habits, 16 modeling and palate development, 17 and the home food environment 18 also play a significant role and may extend into the child’s adult eating behaviors and health. 19 The facilitators of FV intake include healthy home food routines, meal preparation, and frequency of eating at home and with the family. 20 To help address healthy eating patterns, Food as Medicine (FAM) emphasizes the roles that food and nutrition play in both the prevention and treatment of diseases. FAM refers to interventions that seek to improve health and nutrition security through the provision of healthy food in a way that is integrated within health care settings. 21 Produce Prescription Interventions (PRx) are FAM interventions that allow health care providers to “prescribe” FV to eligible patients with a chronic disease diagnosis or lacking access to nutritious foods. These programs are often paired with educational interventions that use a culinary medicine (CM) curriculum. CM offers learners a foundation of culinary and food preparation techniques that are consistent with real-world budgets, time constraints, taste, and cultural preferences. 22
Qualitative studies of PRx in households with children have reported positive associations with FI and FV intake,23–25 but there are very few longitudinal quantitative PRx studies focused on households with children. 25 Some quantitative studies have reported an association with improvements in household FI26–28 and child FV consumption,28–30 while others have shown no association.31,32 There is evidence in an adult population that providing comprehensive nutrition and culinary education in a PRx may facilitate a change in healthy eating behaviors. 33 Additionally, our previous qualitative work exploring the impact of the current ongoing intervention on perceived produce consumption patterns and nutrition- and cooking-related knowledge and behaviors suggested that participants made changes to their behaviors that were motivated by the educational content of the current intervention. 26
To understand the impact of a PRx with nutrition education on quantitative child FV intake, we analyzed adult-reported child FV intake. We hypothesized that participation in the intervention would increase child FV intake.
Methods
Intervention Setting
The Family Lifestyle Program’s PRx (FLiPRx) is an ongoing intervention offered by Children’s National Hospital (CNH) with community partners. 34 The goal is to address diet-related chronic disease risk by increasing healthy food access and nutrition and culinary literacy in households with children living in historically and economically marginalized35,36 neighborhoods.
Inclusion, Exclusion, and Disenrollment
Between November 2022 and December 2024, pediatric patients (0–18 years old) and their adult caregivers who screened positive for FI via the Hunger Vital Sign™ 37 were recruited from two CNH primary care clinics. Only a single child and parent dyad from a home were eligible, and families were not allowed to repeat participation. The detailed inclusion criteria have previously been described26,31 and were maintained and included the presence of diet-related disease risk factors in any member of the household, expressed FI or food hardship, English fluency, and a delivery address within the delivery zone. If a family asked to end their participation in the program or moved outside the delivery zone, they were considered disenrolled from the intervention. There were no disenrollment criteria based on survey completion or class attendance. This work was approved by the Institutional Review Board of CNH (Pro00014391). It was granted a waiver of written documentation of informed consent, and caregivers provided their verbal consent.
Food and Nutrition Intervention
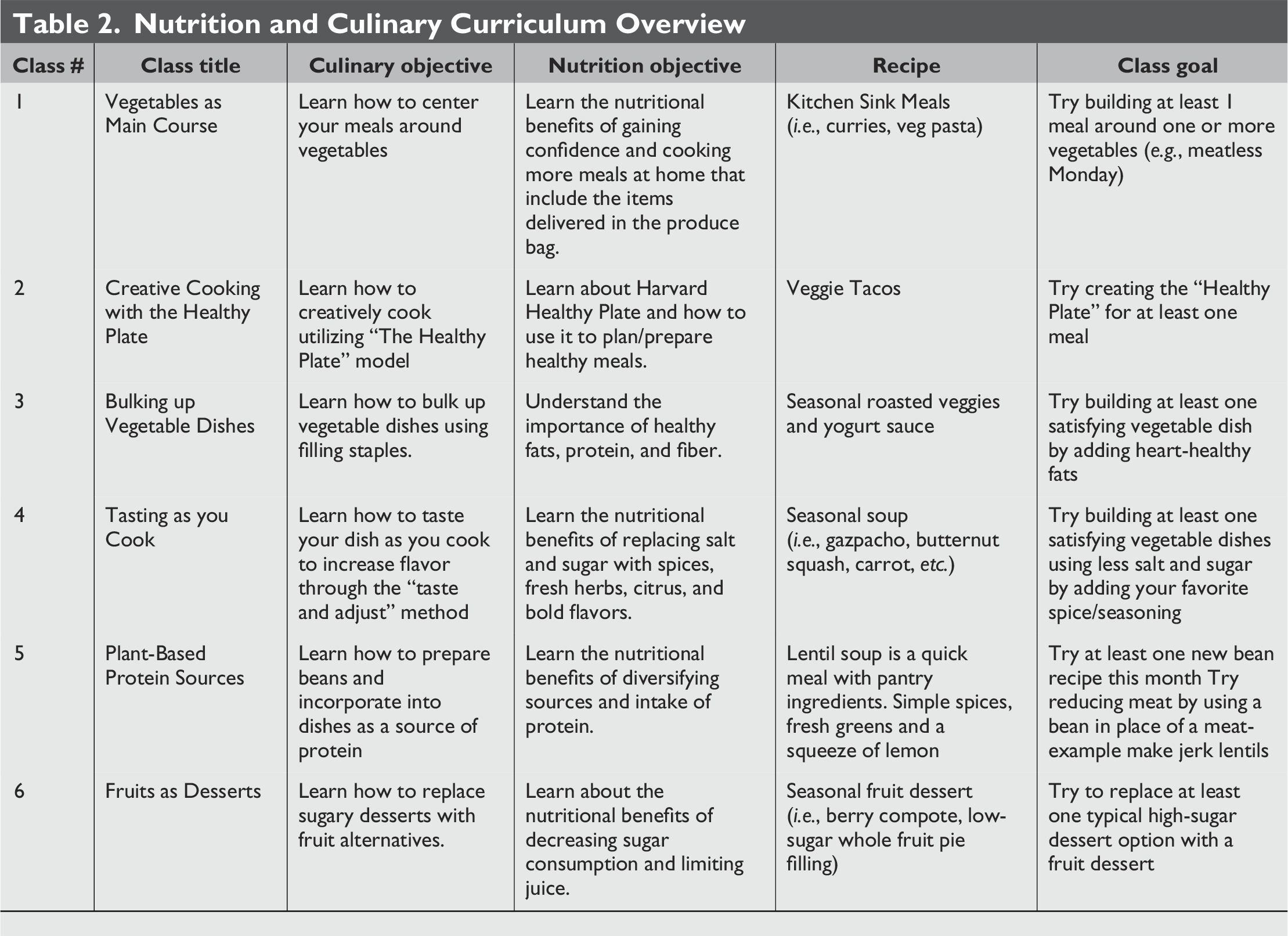
All enrolled families received 8 pounds of fresh locally grown FV delivered to their homes every other week for 6 months at a cost of $30 + $6 delivery fee per delivery. Items were preselected based on local availability and seasonality and were approximately half fruit and half vegetables. Based on standard serving size guidelines, 16 pounds of fruit and vegetables can provide between 64 and 106 servings. Delivery logistics and issues, such as missed delivery, theft, or spoilage, were monitored and handled on a case-by-case basis. Substitutions were allowed in the case of food allergies. Enrolled families also received a one-time delivery of staple ingredients (e.g., lentils and grains) and cooking supplies (e.g., spices and oil) to help utilize the delivered produce and engage in cooking demonstrations. Enrolled families also received culturally relevant, evidence-based nutrition and culinary education in various forms: (1) printed guidebook, (2) library of prerecorded videos, and (3) monthly classes. The printed guidebook contained recipes and instructions, which was meant to help families become familiar with the delivered items and facilitate their use in home cooking and eating (Fig. 1). The videos offered healthy eating tips, including limiting processed foods and eating healthy fats (Table 1). The monthly live, virtual nutrition and cooking classes were co-taught by a culinary expert, a medical provider, and a registered dietitian (Table 2). The class information was directed toward the parent/adult caregivers, and the structure was ∼5 minutes introduction, 20–30 minutes recipe demonstration, 10–15 minutes of nutrition education, and the remaining time for question and answer and group sharing. Recipe demonstrations were based on the delivered items and the cultural food norms and traditions of the target population, which were co-developed with input from previous program participants. Example recipes were “Mushroom Burgers,” “Zucchini Boats,” and “Spaghetti Squash Bowls.” Cooking along with the class instructor was highly encouraged. For additional context, please see a description of the lived-experiences of participants in this class, as detailed in a previous article. 26 The educational content was guided by the Social Cognitive Theory (SCT) and the Transtheoretical Model38,39 and aimed to address the common barriers to FV consumption, such as picky eating, culinary and nutrition self-efficacy and literacy, and food resource management. In our previous iteration, participants’ self-reported attendance and staff perception of attendance were low; thus, we recognized that the educational component and participants’ barriers to education attendance were significant areas of improvement. 31
Example pages from the printed produce guidebook. All participants received a printed guidebook with information about healthy heating, participation in FLiPRx, and suggestions for using the produce delivered during the intervention. Seen here are the title page, table of contents, and two example produce pages (Arugula and Asparagus). We attempted to represent a variety of items that might be delivered during the intervention. Each produce page offered tips on storing and cooking the delivered produce items and a link to our online produce directory with links to recipe ideas, using a QR code. FLiPRx, Family Lifestyle Program’s PRx.
FLiPRx Educational Video Topics
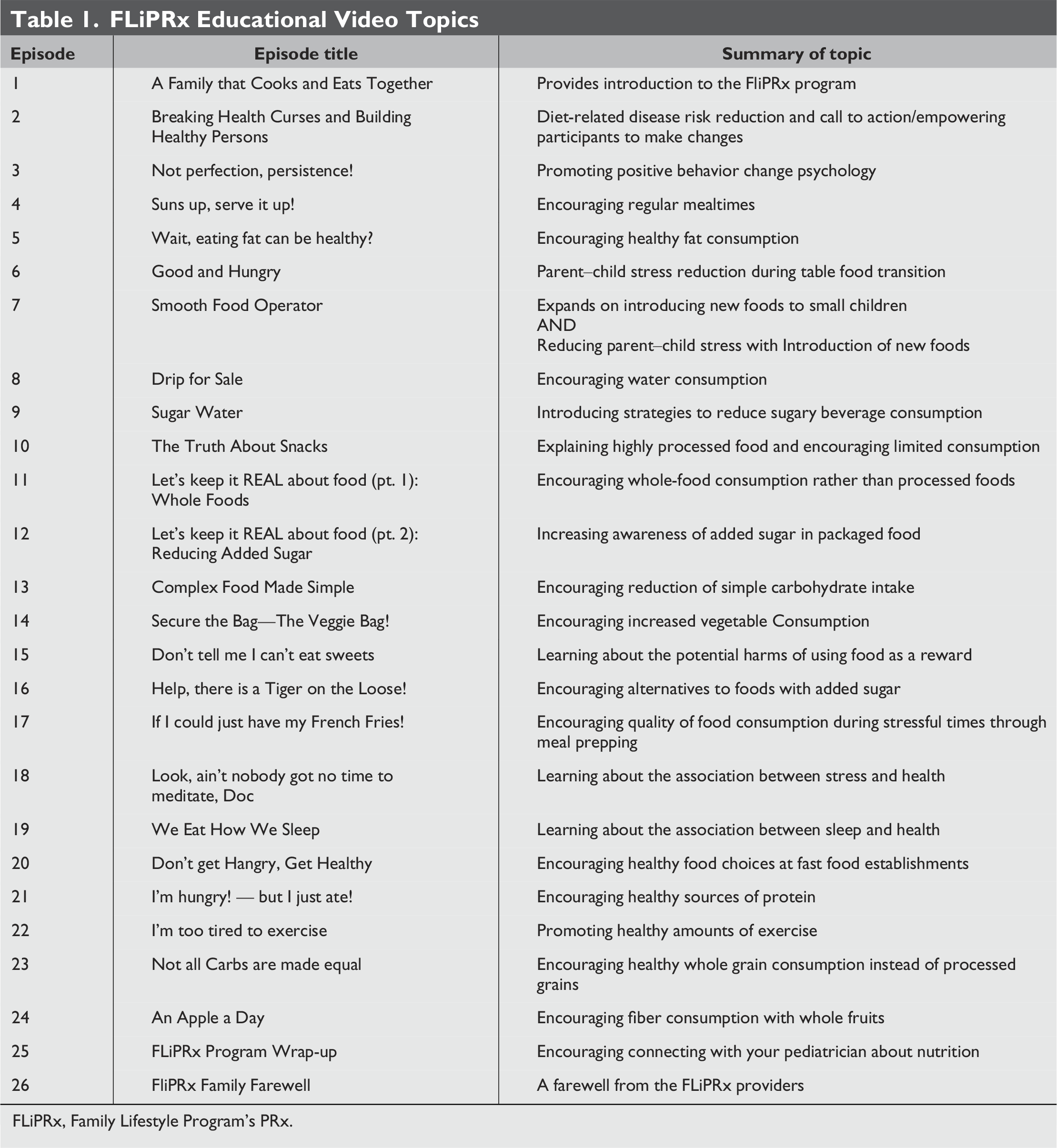
FLiPRx, Family Lifestyle Program’s PRx.
Nutrition and Culinary Curriculum Overview
Study Design
This was a nonrandomized longitudinal interventional cohort study with no control group. A quantitative method approach was utilized through pre–post adult self-report surveys to assess the change in parent-reported child FV consumption. Additionally, baseline demographics and programmatic outcomes data were collected. There were no study disenrollment criteria.
Data Collection
Programmatic data
Retention was the number of enrolled families post-intervention divided by the number of enrolled families at baseline. The response rate was the number of families who completed post-intervention surveys divided by the number of enrolled participants who completed the 6-month intervention at the time of the analysis. The program staff observed and recorded individual class attendance at each monthly class, and attendance was defined as ≥50% or <50% of the classes attended. Produce utilization was self-reported by monthly surveys (on a scale of 0%–100%) and averaged across surveys for each individual. Program satisfaction was evaluated through a self-report post-intervention survey question with a 5-point Likert-type scale response options (5 = Completely Satisfied, 4 = Very Satisfied, 3 = Neutral, 2 = Somewhat Satisfied, 1 = Not at All Satisfied). We asked participants for qualitative feedback about their delivery on delivery days via text message and on monthly surveys. This information was used to troubleshoot logistical issues on a case-by-case basis.
Demographics
Adult caregivers reported household, self, and child demographic factors at baseline, including household size, FI using the USDA 6-item Food Security Survey with a 30-day reference period (scale score of 0–6 to evaluate baseline FI severity), 40 marital status, income, employment, education, use of public benefits, age, race, ethnicity, and gender.
Child FV intake
Adult caregivers answered selected questions from the National Cancer Institute’s (NCI) Eating at America’s Table Study Quick Food Scan All Day Screener 41 to report their enrolled child’s fresh fruit and fresh or cooked vegetable intake frequency and portion size in the previous week for children over the age of 1 year. To obtain the daily cup equivalents of FV, the weekly frequency of intake was averaged to the daily intake and then multiplied by the portion size using the 2005 MyPyramid definitions of fruit and vegetable cup equivalents, as per the NCI’s scoring algorithm. 42 Cases were excluded if frequency or portion size responses were missing. Adults also self-reported their FV intake, and these data will be reported at a later date.
Participants received monetary compensation for their time spent completing surveys. Study data were collected and managed using Research Electronic Data Capture (REDCap) tools hosted at CNH. 43
Data Analysis
Descriptive statistics
The data were tested for normality by observing the distribution of residuals of each continuous variable. The data were not normally distributed; therefore, nonparametric tests were used. Univariate analyses were used to describe programmatic outcomes, baseline demographics, and cross-sectional FV intake. The median and interquartile range for continuous variables and the number and percentage for categorical variables are reported. We conducted a sensitivity analysis by evaluating the distribution of missing responses with respect to demographic factors.
Regression analyses
Raw FV data were not normally distributed and were log-transformed to meet the assumptions of the regression. Log-transformed data were approximately normally distributed. Multiple mixed-effects regression models were used to test the main effect of time (baseline and post-intervention) on log-transformed FV intake variables (fruit and vegetable). Models tested the independent main effects of time on the dependent FV intake variables (fruit and vegetable) with and without controlling for baseline demographic and programmatic variables that were suspected to potentially impact FV intake (class attendance, produce use, FI score, adult age, child age, number of adults and children in the home, marital status, education level, income level, employment status, and Supplemental Nutrition Assistance Program and/or Supplemental Nutrition for Women use). We report the unadjusted and adjusted regression coefficients for the main effect of time (R) and the corresponding p-value.
The significance level of all analyses was 5%. Statistical analysis was conducted with SAS software version 9.4. 44
Results
Demographics and Programmatic Outcomes
During the stated time frame, 307 child/adult pairs were enrolled in the intervention, and 5 were disenrolled (302/307 = 98% retention); 197 participants completed the post-intervention survey (197/302 = 65% response rate), and 176 participants provided complete pre–post food frequency data (176/197, 89%, Fig. 2). The analysis was conducted on the 176 who provided complete data. The distribution of missing data was independent of any demographic variable. The majority of adult participants were female (92.1%) and African American (92.5%) with >1 child in the home (66.5%). At baseline, the median FI score was 3.0 (interquartile range [IQR]: 4) out of 6, which corresponds to a status of “low food security,” characterized by some degree of difficulty accessing enough food and associated with coping strategies, such as reducing the quantity or quality of food consumed. 9 Average produce utilization was 79% (IQR: 30%), over half of the participants attended over half of the classes (59.1%), and 94.5% of the participants were “Very” or “Completely” satisfied with the program (Table 3).
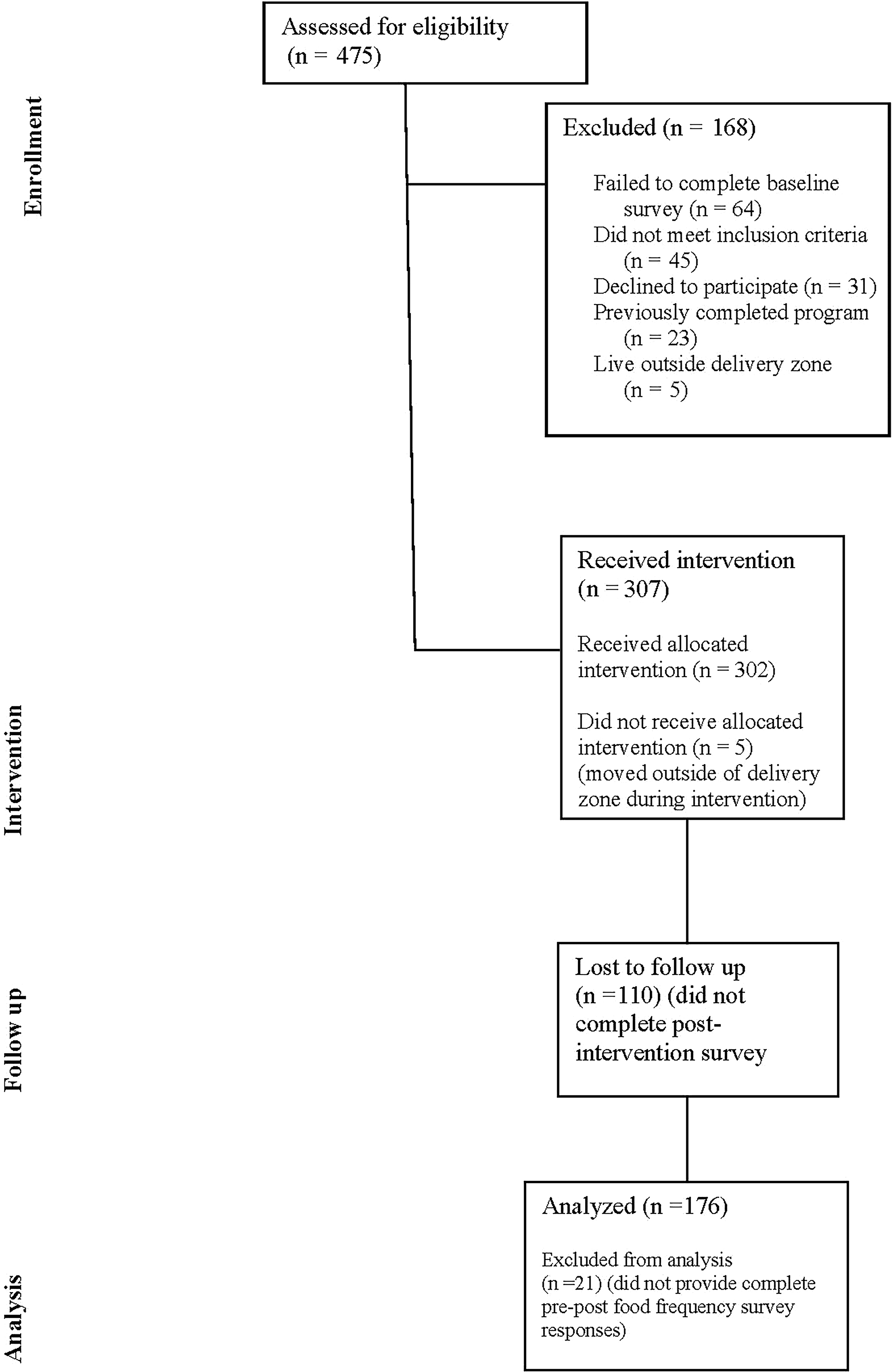
Consort diagram. The diagram describes the flow of participants through enrollment, intervention, follow-up, and analysis. During the stated time frame, 475 families were referred to FLiPRx and were assessed for eligibility for FLiPRx participation, 168 were excluded due to not completing baseline assessments, not meeting the inclusion criteria, declining to participate, already enrolled, or living outside the delivery zone. There were 302 families that received the FLiPRx intervention as intended. Among those, 110 did not complete the post-intervention survey, 21 did not provide complete pre–post data, and the final analytical sample was n = 176.
Demographics and Programmatic Data (n = 176)
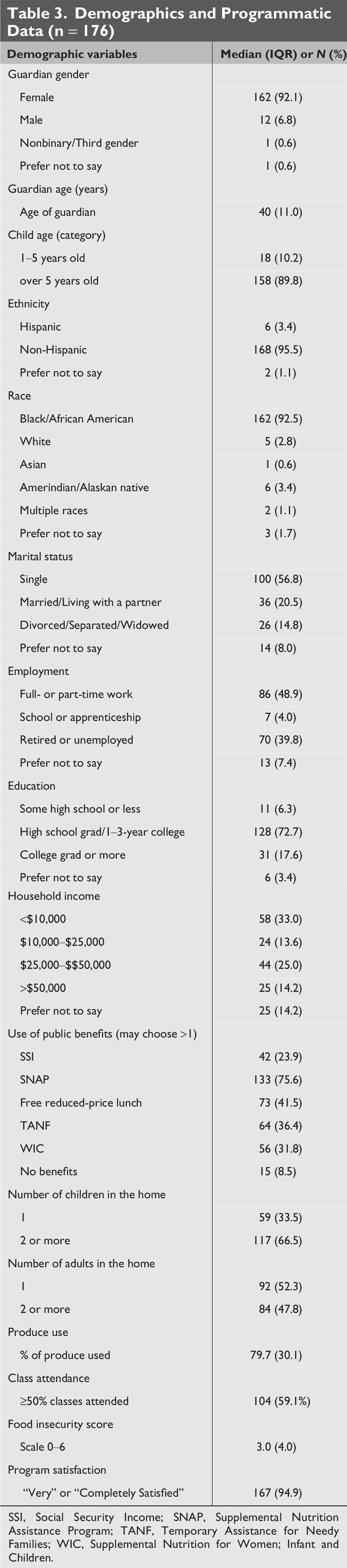
SSI, Social Security Income; SNAP, Supplemental Nutrition Assistance Program; TANF, Temporary Assistance for Needy Families; WIC, Supplemental Nutrition for Women; Infant and Children.
Child Fruit and Vegetable Intake
Median cup equivalents
The median daily cup equivalent intake of vegetables and fruits increased from baseline to post-intervention. Baseline and post-intervention vegetable intake levels were 0.13 (0.20) and 0.25 (0.39), and fruit intake levels were 0.19 (0.45) and 0.25 (0.39), respectively (Table 4).
Pre–Post-Intervention Change in Fruit and Vegetable Consumption and the Mixed-Model Regression Coefficient for the Main Effect of Time
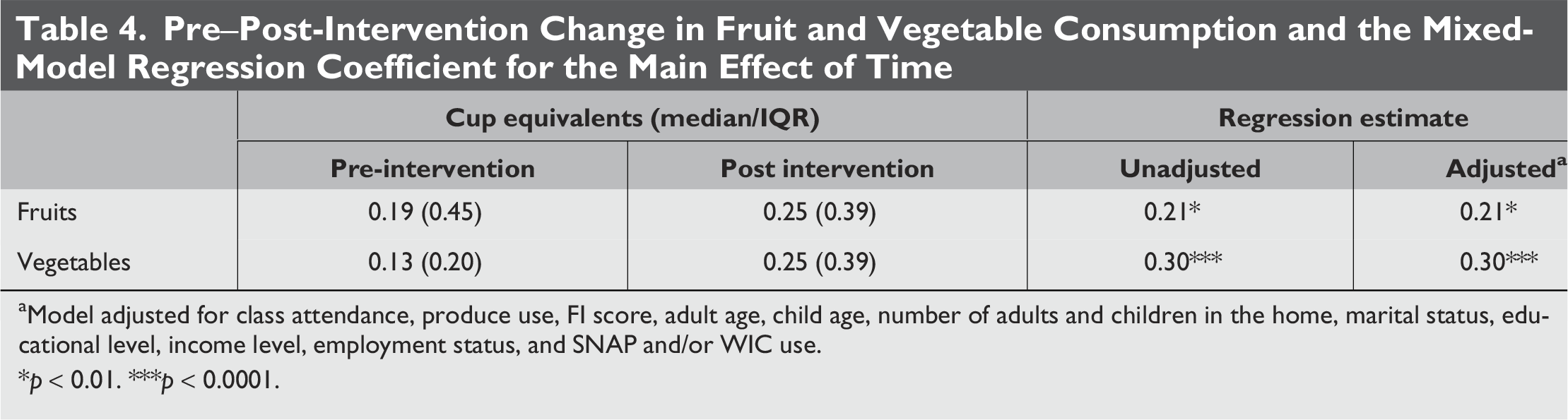
Model adjusted for class attendance, produce use, FI score, adult age, child age, number of adults and children in the home, marital status, educational level, income level, employment status, and SNAP and/or WIC use.
*p < 0.01. ***p < 0.0001.
Regression models
There was a significant effect of time on fruit (R= 0.21, p = 0.004) and vegetable (R = 0.30, p < 0.0001) consumption, indicating the pre–post increase in FV consumption was statistically significant. In adjusted models, the effect of time on fruit and vegetable consumption remained significant and was not attenuated, (R = 0.21, p = 0.004 and R = 0.30, p < 0.0001, respectively). There were no other statistically significant main effects of any demographic or programmatic variable on FV consumption.
Discussion
The goal of this study was to evaluate the impact of a PRx on child FV intake. Caregivers reported higher child FV consumption versus baseline consumption. This supports our hypothesis that PRx participation is associated with increased child FV intake. Additionally, despite post-intervention improvements, child FV intake was still notably low, falling well below the recommended guidelines for children, indicating that further improvements in the intervention are necessary to achieve the optimal FV intakes.
These data are consistent with the findings of other studies that have reported increased child fruit intake in participants of PRx29,30,45,46 and provide a counterpoint to other PRx reports of no association with child FV intake.31,32 One possible reason for the lack of a consensus is the variable use of an education component. 47 Some evidence suggests that nutrition education combined with culinary interventions have a significant effect on dietary habits.48–50 In our study population, the observed increase in child FV intake may potentially be attributed to several factors related to the content of the evidence-based education. The classes provided caregivers with practical skills and knowledge on how to prepare, store, and cook different types of produce, many of which were delivered directly to their home through the intervention. The class also provided encouragement and motivation for caregivers to offer FV at more meals and snacks and provided instructions for making produce more “kid-friendly” by preparing it in more palatable ways and making it more appealing to children. The curriculum also focused on getting the children involved in all aspects of home cooking. Another potential route of the impact on child FV intake could be through a behavior modeling mechanism. For example, if the caregivers themselves began eating more FV during the program, it may have influenced the child to eat more FV because kids’ eating habits are modeled after the adults in their home.17,18
Another potential driver of the impact of this intervention on child FV intake is the use of home delivery. Greater access to fresh produce in the home may have addressed financial 16 and geographical constraints that may have limited the FV options in the home. Study participants reside in an area classified as a food desert, where fast food options are more readily accessible than sources of fresh produce, making the pursuit of healthy eating a difficult endeavor. Participants in this study population have previously described the challenges they face when making food purchases for themselves and their families related to the lack of access to healthy, affordable, high-quality food and barriers related to limitations in finances, transportation, knowledge, and time.15,24,26 The FLiPRx intervention was designed to help mitigate some of these barriers. The increased availability of fresh FV via home delivery may help address structural barriers, such as the lack of public transportation infrastructure and the lack of access to affordable, high-quality FV options. Other interventions that utilize produce vouchers have reported low redemption rates and barriers to redemption, many of which cited limitations around access to locations where redemption is offered.15,51,52 Home delivery may be an ideal implementation strategy to overcome this common barrier.
Despite post-intervention improvements, FV intake levels remained well below the recommended amounts (∼2 cups per day), indicating that further efforts are necessary to achieve optimal FV consumption in child participants of PRx. Our findings are consistent with the existing literature, showing that typical child FV intake is well below the recommended amounts, particularly in low-income populations.7,8 This highlights the need for more targeted and effective PRx interventions. A potential area for improvement is in the quantity or duration of the delivery. All families received the same amount of produce regardless of the family size, which might have made it difficult to meet the FV needs of families with more people, resulting in fewer potential FV servings per family member. The choice to offer 8 pounds every other week (approximately 16 pounds of produce per month) was based on our available funding and the standard delivery size of our produce delivery partners, 4P Foods. We recognize that this amount might not be enough to appreciably increase child FV intake, especially if a household has multiple children and adults. Because this is a family-based intervention, we recognize that some of the produce may have been consumed by other family members, who were not the reference child under observation. Additionally, our intervention offered virtual education that was primarily targeting adult caregivers. A curriculum that directly targets child PRx participants and which is offered in-person may be helpful in achieving greater increases in child FV intake. We will explore these factors in future iterations of the program by offering child-directed education and by scaling the amount of produce delivered by the family size.
This study was not without limitations. This study was not randomized, did not include a control group, and participants were self-selected into the intervention. Another limitation is that the data were collected via adult-report. Adult caregivers may not be entirely aware of the eating habits of their children and may inaccurately report FV intake. Also, adult caregivers might overestimate child FV intake. Additionally, we cannot rule out the possibility that some unmeasured factor played a role in the relationship between PRx participation and increasing child FV intake; thus, future research should use randomized controlled designs. In addition to adult-reported child outcomes, in the future, it would be valuable to collect child-reported outcomes. Another limitation is that we did not collect quantitative or qualitative data regarding delivery issues, such as spoilage or theft. Although we did not collect the data, the quality of the deliveries can be inferred from the level of satisfaction with the overall program. Quantitative and qualitative data related to delivery issues will be included in future iterations.
Conclusion
These data support the hypothesis that participation in PRx is associated with improvements in child FV consumption and might extend to other PRx that serve similar populations. While this outcome is encouraging, FV intakes were still well below the US dietary guidelines recommendations; thus, further work to increase PRx efficacy is needed. Future PRx interventions should consider the size and frequency of the produce offered and explore additional educational and behavioral supports, such as education for the child and nutrition counseling from a registered dietitian. It is possible that a more tailored or intensive intervention could have greater improvements on child FV intake.
Impact Statement
These data support the hypothesis that Prescription Interventions (PRx) are associated with improved child fruit and vegetable intake. This study offers new insight for the implementers of Produce PRx and health care providers looking for effective resources to prevent and manage childhood obesity.
Authors’ Contributions
E.M.P.: Methodology (supporting), formal analysis (equal), data curation (equal), writing—original draft (equal). K.E.: Project administration (equal), conceptualization (equal), writing—review and editing (supporting), funding acquisition (equal), resources (supporting). A.T.: Investigation (supporting), resources (supporting), writing—review and editing (supporting). Q.A.: Project administration (equal), investigation (supporting), resources (supporting), conceptualization (equal), funding acquisition (equal), writing—review and editing (supporting). L.F.: Project administration (equal), supervision (lead), investigation (lead), conceptualization (equal), formal analysis (equal), methodology (lead), data curation (equal), writing—original draft (equal), writing—review and editing (lead), funding acquisition (equal), resources (lead).
Footnotes
Acknowledgments
The authors would like to acknowledge the families who participated in this study, clinicians and staff from CNH who referred participants, 4P Foods for their partnership in food delivery, and the YMCA of Washington DC for education support. The authors would also like to thank Barbara Welsch for her administrative support and Beth Tarini for her mentorship and guidance. Lastly, the authors would like to thank the FLiP Community Advisory Board for their continual partnership, guidance, feedback, and support.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work is supported in part by the National Institute of Food and Agriculture, U.S. Department of Agriculture [AWD 2022-70424-38477]; No Kid Hungry [AWD00003121]; Children’s Health Board [na]; Capital One [AWD00003715]; Morningstar [AWD00004246]; and the Vitamix Foundation [AWD00003856].