
Abstract
Background
Surgery is often avoided in the setting of pediatric orbital complications from acute sinusitis unless necessitated by alarming ophthalmological signs. Criteria for surgical intervention are not well-defined.
Objective
We aim to review our experiences, management practices and patient outcomes over a ten-year period for Chandler III patients.
Methods
A retrospective review was performed from January 1, 2007 through December 31, 2016 of patients treated for orbital symptoms secondary to acute sinusitis at a free-standing tertiary-care pediatric hospital.
Results
Of the 186 patients reviewed, 42 Chandler III patients were included. Average age was 82.6 months (SD 50.6) with a slight male predominance (M to F, 1.8 to 1). 27 patients (64.3%) underwent intervention including endoscopic sinus surgery (ESS) with or without orbitotomy. Late surgical intervention (>48hrs from admission) demonstrated significant increase in overall length of stay (LOS) when compared with early surgical intervention and/or medical management (median, 6.9 vs 3.6 vs 3.7 days; p < 0.01). Postoperative LOS was also higher in the late surgery group compared with patients who had surgery within 48 hours of admission, but this did not reach statistical significance [median, 3.8 vs 2.8 days, p= 0.12]. There was no significant difference in overall abscess volume between patients who underwent intervention and those who did not (1019 mm3 vs 805 mm3, p = 0.5), but abscess width ≥ 1.2 cm was associated with higher rates of intervention. An alarming extraocular exam was the most common factor associated with surgical intervention.
Conclusion
Pediatric subperiosteal orbital abscess may prompt surgical intervention by ESS. An alarming ophthalmologic exam should prompt consideration of early intervention, which may lead to decreased overall and post-operative length of hospital stay.
Level of Evidence
4
Meeting Information
American Rhinologic Society, Fall National Meeting. Chicago, IL, USA. September 8–9, 2017.
Introduction
Orbital complications from acute sinusitis are a relatively common occurrence, particularly in the pediatric population. The orbital septum is a key anatomic landmark used to differentiate pre-septal and post-septal cellulitis. Infections anterior to the orbital septum are consistent with pre-septal cellulitis, while infections of the soft tissue surrounding the eye, posterior to the orbital septum, are referred to as orbital (post-septal) cellulitis. 1 Orbital cellulitis is important to recognize, as retrograde spread of the infection can lead to alarming consequences including subperiosteal abscess, intracranial abscess, cavernous sinus thrombosis, meningitis, and vision loss.2–5 Chandler developed a widely-used classification system that describes the extent and severity of orbital infection. 6
Acute rhinosinusitis is the most common cause of orbital complications in children, accounting for 60–80% of pediatric cases, with acute ipsilateral ethmoiditis being the most common cause.1,7–9 These infections can rapidly spread and lead to devastating consequences, even with aggressive IV antibiotic therapy.1,10 Thus rapid diagnosis, treatment, and close monitoring of patients is warranted. Patients who present with mild symptoms, without ophthalmoplegia or proptosis, are often managed medically with IV antibiotics and close observation.1,2,9,10 Conversely, patients who present with ophthalmoplegia and proptosis, or those who fail to respond to conservative measures, are more likely to require surgical intervention to drain a fluid collection.1,10,11 The timing of surgery and the precise indications for surgery are not well-defined, particularly for Chandler III patients who by definition have a subperiosteal abscess of the orbit (SPAO).1,10,12 Many authors advocate for early surgical intervention in patients who are unlikely to benefit from medical therapy due to the extent of their disease and the risk for severe complications.1,10,12
We aimed to review our experiences, management practices, and patient outcomes over a ten-year period for patients treated for SPAO at an academic pediatric tertiary-care center, with the hope of adding to the criteria which delineate ideal surgical candidates and timing for surgical intervention.
Materials and Methods
Patient Selection
IRB approval for this study was obtained from Indiana University (IRB # 1704110118). A retrospective chart review was performed from January 2007 through December 2016 of patients evaluated and managed at Riley Children's Hospital, a freestanding tertiary pediatric hospital. Patients less than 18 years old who were admitted for orbital complications related to sinusitis were included in this study (those with the given diagnosis codes in their record: ICD-9 376.0x and ICD-10 H05.0x). Patients with lack of evidence of sinus disease on radiographic imaging and those with intracranial disease were excluded from this study.
Data Extraction
Charts were reviewed for demographic information including age, sex, clinical and radiographic findings, presence of sinusitis, blood work, microbiology, length of and types of antibiotics administered, placement of peripherally inserted central catheters (PICC), physical examination (as described in ‘ophthalmologic evaluation’ below), patient-reported symptoms, length of overall and post-operative hospital stay, and interventions provided.
Outcome Measurements
Measured outcomes included: ophthalmologic exam improvement following intervention, ophthalmologic complications prior to and after interventions, length of hospital stay, length of antibiotics, readmission for recurrent/recalcitrant symptoms, and need for further surgical intervention after the initial procedure.
Institutional Standard Management Algorithm
A standardized management algorithm was utilized for all Chandler III patients during the study period. Patients were typically admitted to the infectious disease (ID) service, with prompt ophthalmology and otolaryngology consults and complete physical exams. If ophthalmologic and otolaryngologic exam was not alarming (as quantified in the results), patients were started on IV antibiotics (selection per ID), along with a nasal regimen (saline spray/irrigation, nasal decongestants for 3 days, and nasal corticosteroids indefinitely), and monitored clinically by all involved teams for 24–48 hours. If a patient clinically worsened, failed to improve after 48 hours, or demonstrated radiographic progression on serial imaging, surgery was typically pursued after a multi-disciplinary discussion, but the ultimate decision to go to the operating room was decided by the Otolaryngology attending. Repeat imaging was not routinely obtained but was sometimes pursued after multidisciplinary discussion in the patient with a worsening or unreliable exam. If the event of clinical improvement (defined as decreasing peri-orbital erythema/edema, improving EOM, lack of fever, improving labs, and improvement on imaging), observation was continued and the patient was transitioned to a home antibiotic regimen and discharged home when meeting typical criteria, per the ID team.
Ophthalmologic Evaluation
The ophthalmology team evaluated every patient and documented visual acuity, intraocular pressure, afferent pupillary defect, proptosis, and extraocular motion (EOM) restriction. EOM was graded from 0–3, such that 0 represented no restriction, 1 represented mild restriction on extremities of gaze, 2 represented moderate restriction, and 3 represented severe restriction (fixed globe).
Lund-Mackay Score Determination
Lund-Mackay scores were determined through retrospective review of the imaging by one of the senior resident authors (C.R.), in standard fashion after review of several scans with a rhinology attending, with a maximum score of 24 for each patient. 13
Measurement of Orbital Abscess Size
Measurements of SPAO size were performed for Chandler III patients. The extent of orbital disease on initial radiographic imaging was utilized to classify patients based on the Chandler system. This classification was assigned by the clinician at the time of hospitalization, as demonstrated through the admission and progress notes, and confirmed during our retrospective review. We developed a novel method to consistently measure SPAO volume by treating the abscess as a half-ellipsoid, adjacent to the ethmoid air cells. The volume of the full ellipsoid was calculated using the formula: V = [4/3 × π × a/2 × b × c/2], where a, b, and c represented anterior posterior (AP) length, width, and height, respectively (

Orbital abscess volume calculation. Axial and coronal views of a child with a left-sided subperiosteal abscess are shown. Orbital Abscess Volume was calculated by treating the abscess as a half-ellipsoid, using the final formula [V = 1/6 x π × a × b × c], where a, b, and c represented anterior posterior (AP) length, width, and height, respectively.
Group Comparisons
To compare patient outcomes, two subgroups were created and analyzed. First, medical and surgical patients were compared regarding the variables noted above. Next, the surgical group was divided into an early intervention group (surgery ≤48 hours after admission), and a late group (surgery >48 hours after admission). These criteria were chosen based on previously published data which has provided variable recommendations regarding timing of intervention.1,10,12
Statistical Analysis
Data was aggregated utilizing Excel 2013 software (Microsoft Corp). Student two-sample T-tests were used for parametric continuous variables, Mann-Whitney U tests were used for non-parametric continuous variables, and Fisher's Exact statistical analysis was performed on categorical variables, using IBM SPSS Statistics (version 24, IBM Corp.). For all test, p values <0.05, and their corresponding confidence intervals, were considered statistically significant.
Results
Of the 186 patients initially identified through chart review, 108 patients met criteria for further analysis. Altogether, patients mostly presented in the winter and spring seasons, specifically between December and April. Patients were classified according to the Chandler system (Table 1); forty-two Chandler III cases met criteria for final inclusion. The demographic and clinical features of these patients are listed in Table 2, along with comparisons of medically-treated and surgically-treated patients. Twenty-seven patients underwent intervention including endoscopic sinus surgery (ESS) (n = 14) or ESS with open orbitotomy (n = 13). No Chandler III patients underwent orbitotomy alone. In patients who underwent ESS without orbitotomy, the procedure entailed endoscopic medial orbital wall decompression, endoscopic anterior ethmoidectomy, and in some instances maxillary antrostomy and/or sphenoidotomy. In those who underwent concurrent orbitotomy, the orbitotomy incision was typically utilized to decompress the medial orbital wall, while ESS in these patients included anterior ethmoidectomy and sometimes maxillary antrostomy and/or sphenoidotomy.
Chandler Classification at Presentation and Intervention Rates.

Demographic and Clinical Data for all Patients, with Surgical vs Medical Comparisons a .

Values presented are mean (SD) unless otherwise specified.
Surgical = Patients treated with endoscopic sinus surgery +/- orbitotomy.
Medical = Patients treated with antibiotics (IV and PO), nasal decongestants, nasal saline spray, and nasal steroid sprays.
Student t test: 2-tailed.
“N-1” Chi squared test.
“N-1” Chi squared test, comparing the 14/17 patients with lateral length > 1.2 cm who underwent intervention, vs the 13/25 with lateral length <1.2 cm who underwent intervention.
Mann-Whitney U test.
*An Alarming Ophthalmologic exam consisted of one or more of the following: decreased visual acuity from baseline, unreliable ophthalmologic exam, afferent pupillary defect (APD), and/or grade 1-3 extraocular motion restriction (all evaluated by the ophthalmology team at our institution).
Abbreviations: N, number of patients; m, months; CI, Confidence Interval; SD, Standard Deviation; mm, millimeters; d, days; WBC, White blood count; EOM, Extra-ocular motility; APD, Afferent Pupillary Defect; PICC, Peripherally Inserted Central Catheter.
There was no significant difference in LOS between those who underwent ESS alone and those who underwent ESS and orbitotomy [mean (SD); 5.4 (4.4) vs 5.8 (3.3) days; p = 0.80]. 5/42 patients received parenteral or oral steroids; four received 24 hours of IV dexamethasone upon presentation, and one presented to the hospital having received a five-day outpatient course of oral prednisolone; steroids were not associated with any change in evaluated outcomes.
The abscess locations in the medically-treated group included 1 inferior and 14 medial. Locations in the surgical group included 1 inferior, 18 medial, 3 inferomedial, 1 superior, 1 superolateral, and 3 superomedial. Notably, all 5 patients with superior involvement underwent surgery; 4/5 underwent ESS and orbitotomy concurrently, and 1 underwent ESS alone. There were no other factors associated with concurrent orbitotomy; surgeon variability and preference likely played a role.
Frontal sinus disease did not correlate with higher rates of surgical intervention (P = 0.9): 16 of 21 patients with obstructive frontal sinus disease on presentation underwent surgery, while 11 of 21 patients without significant frontal sinus disease underwent surgery.
Retrospective analysis revealed that the decision to proceed with surgery was based on the following overlapping factors: a poor response to IV antibiotics (n = 12), large size of SPAO on initial imaging (no specific cutoff was cited) (n = 8), alarming/unreliable ophthalmologic exam (n = 6), progression of SPAO on serial imaging (n = 3), and concurrent large burden of sinus disease (n = 2).
Although data was variable, patients were typically empirically treated with Unasyn or Ceftriaxone plus clindamycin or vancomycin. There was no correlation between antibiotic choice and avoidance of surgery. Antibiotic resistance was not found to be a factor associated with higher rates of surgery. There was no significant difference in age, gender distribution, prevalence of asthma and allergies, WBC count, length of stay (LOS), length of antibiotics, PICC line placement, or Lund-Mackay score between those who underwent surgery and those who did not (
SPAO volume was not correlated with intervention rates, but a sub-measurement, width, was correlated with a higher rate of intervention (
Of patients ultimately undergoing ESS, late surgical intervention (>48hrs from admission) demonstrated significant increase in overall LOS when compared with early surgical intervention and/or medical management (median (IQR); 6.9 (9.1) vs 3.6 (1.8) vs 3.7 (2.8) days; p < 0.001 on Mann-Whitney U) (Tables 2 and 3, Figure 2). Postoperative LOS was higher in the late surgery group compared with patients who had surgery within 48 hours of admission, but this did not reach statistical significance [median; 3.8 vs 2.8 days; CI 0.6–5.5 days, p = 0.12 on Mann-Whitney U] (
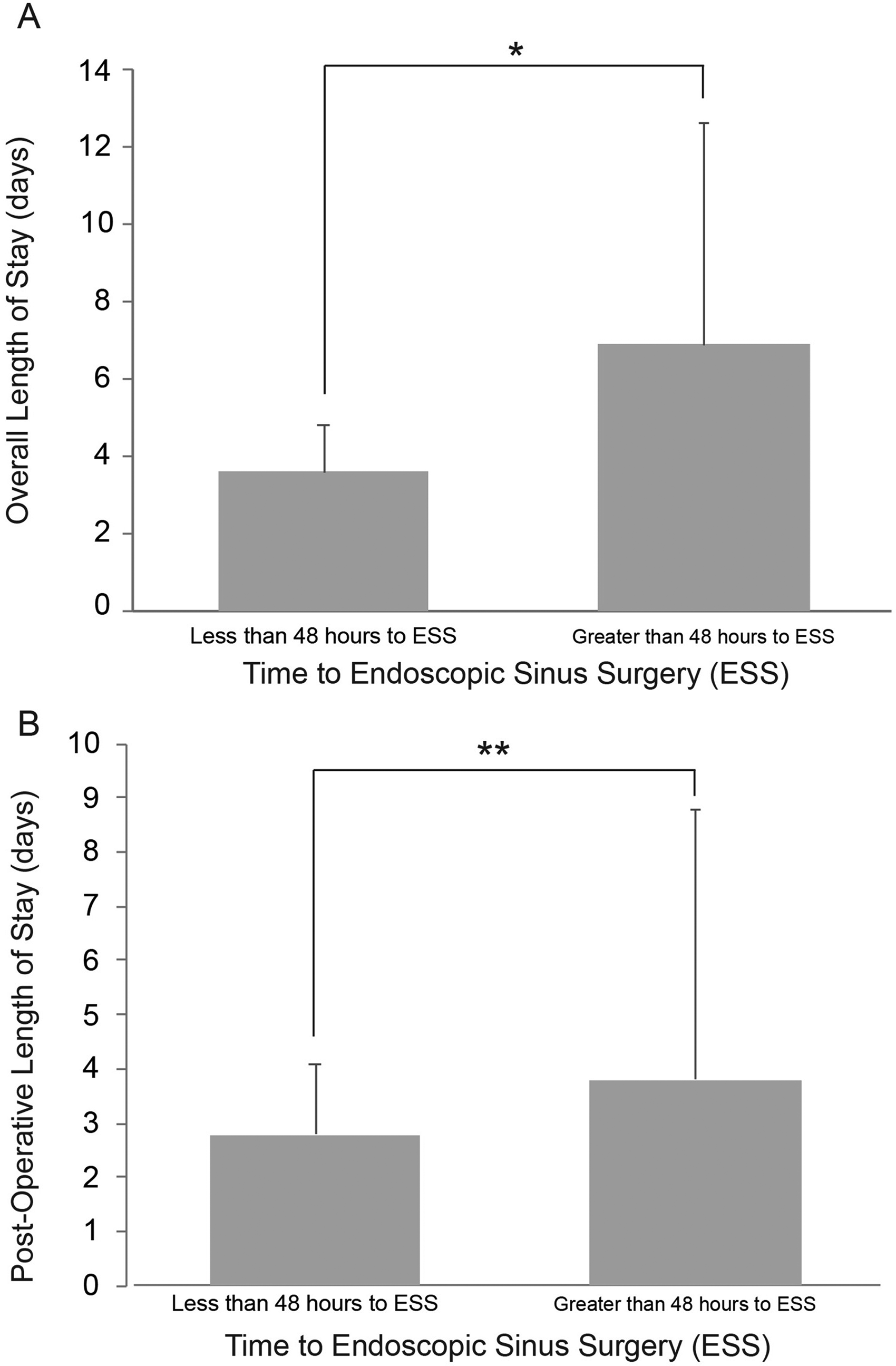
Relationship between length of stay (LOS) and time to intervention. Among patients with a subperiosteal abscess, those who underwent surgical intervention (ESS) within 48 hours of admission were compared with those who underwent surgery after 48 hours from admission. Earlier intervention was associated with a significantly shorter overall LOS (A) and (B) possible decreased postoperative length of stay (although this did not meet statistical significance). *p < 0.001; **p = 0.12 on Mann-Whitney U. mm = millimeters. ESS = Endoscopic Sinus Surgery.
Demographic and Clinical Data for Early vs Late Surgical Patients a .
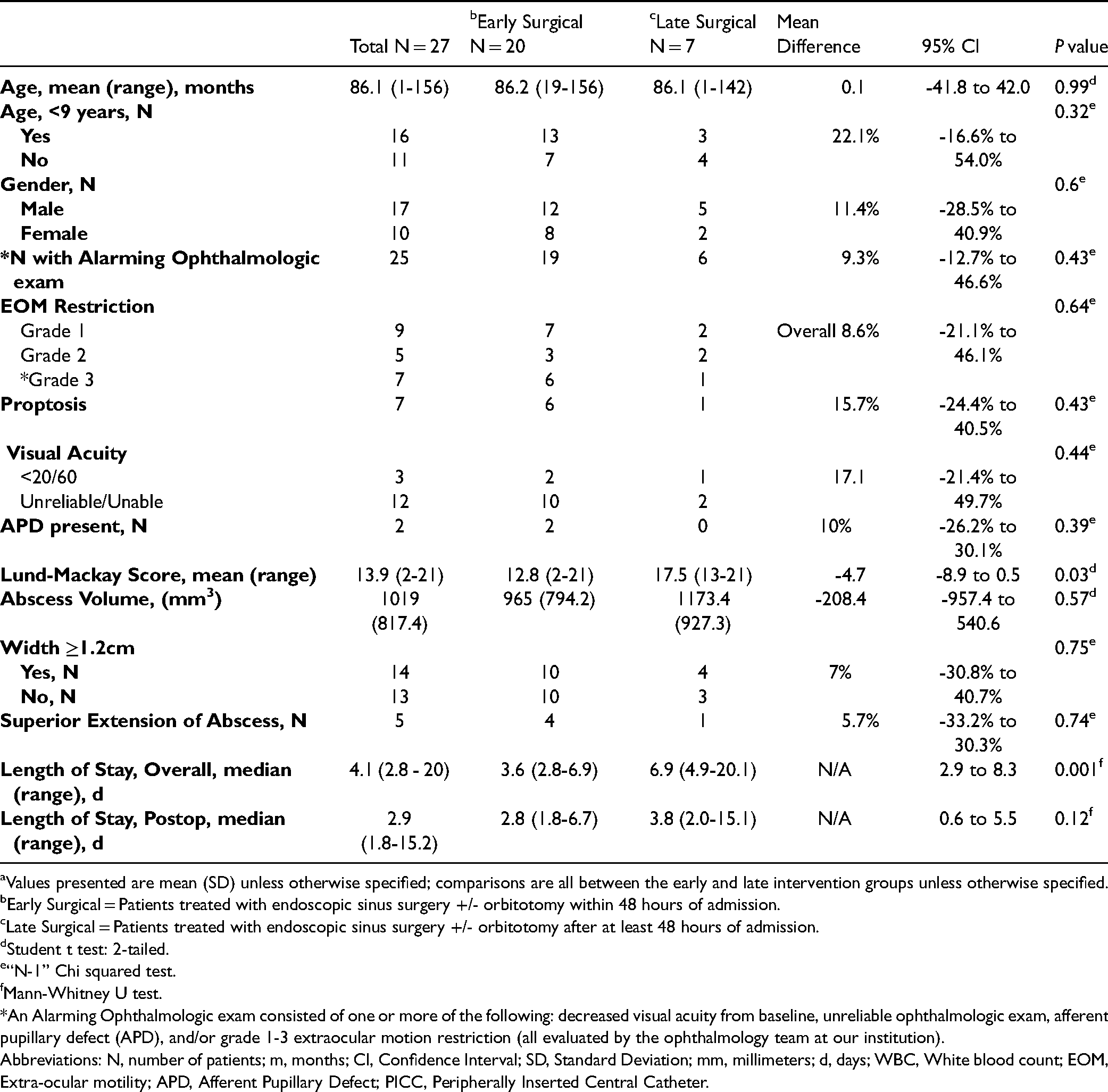
Values presented are mean (SD) unless otherwise specified; comparisons are all between the early and late intervention groups unless otherwise specified.
Early Surgical = Patients treated with endoscopic sinus surgery +/- orbitotomy within 48 hours of admission.
Late Surgical = Patients treated with endoscopic sinus surgery +/- orbitotomy after at least 48 hours of admission.
Student t test: 2-tailed.
“N-1” Chi squared test.
Mann-Whitney U test.
*An Alarming Ophthalmologic exam consisted of one or more of the following: decreased visual acuity from baseline, unreliable ophthalmologic exam, afferent pupillary defect (APD), and/or grade 1-3 extraocular motion restriction (all evaluated by the ophthalmology team at our institution).
Abbreviations: N, number of patients; m, months; CI, Confidence Interval; SD, Standard Deviation; mm, millimeters; d, days; WBC, White blood count; EOM, Extra-ocular motility; APD, Afferent Pupillary Defect; PICC, Peripherally Inserted Central Catheter.
Cultures grew Viridans Streptococci in seven patients, Streptococcus Pyogenes in twelve patients, methicillin-sensitive staphylococcus in sixteen patients, and Enterobacter cloacae in one patient. Two patients had negative cultures. Four patients (three Chandler II and one Chandler III) had methicillin-resistant Staphylococcus (MRSA), including two infants (
MRSA ( + ) Cases.

ESS = endoscopic sinus surgery.
Overall, during the 10-year study-period, no Chandler III patients re-presented at our institution with recurrence or progression of symptoms. All patients had resolution or near-resolution of their ophthalmologic symptoms, and subsequent transition to PO or IV antibiotics, prior to discharge from the hospital. Our retrospective review revealed no long-term sequelae among the Chandler III cohort, but long-term follow up was not consistently performed.
Discussion
Ophthalmologic examination and radiographic findings commonly guide the therapeutic pathway in patients presenting for orbital complications related to sinusitis.1,10,14–16 Criteria for intervention in the setting of this disease have evolved over the past 20 years. Previous studies and common practice have dictated that patients younger than 9 who present with mild symptoms and without alarming ophthalmologic symptoms respond well to a trial of IV antibiotics and close observation.1,7,10–12,17–20 On the contrary, the presence of frontal sinus disease, odontogenic origin, large abscess volume and emergent ophthalmologic symptoms generally favor surgical intervention, even in those younger than 9 years of age.1,10,11,14–16,18,19 Despite common practice, determining which patients will ultimately require surgery remains difficult to predict on initial evaluation, especially with regards to Chandler III patients, and prior studies have produced conflicting recommendations.1,5,7,9,10,12,17,21 Recent studies suggest that larger abscess volume and an alarming ophthalmologic exam are predictors of surgical intervention, while age does not play a large role.14–16
A recent systematic review by Wong et al consolidated various factors to devise an algorithm that may help guide decision-making in patients with orbital complications of sinus disease. 1 In this algorithm, patients presenting with symptoms concerning for SPAO should obtain a CT scan of the sinuses within 24 hours of admission. 1 Patients with a CT-confirmed SPAO who have worrisome ophthalmologic findings are then started on antibiotics with plans for early surgical intervention. 1 Patients without concerning ophthalmologic findings, who are under 9 years old, should be considered for medical vs surgical intervention, a decision primarily driven by abscess size (with 3.8 ml used as a cutoff) and the presence or absence of frontal sinus involvement.1,10 More recent systematic reviews and meta-analyses echo this recommendation for surgical intervention in those with large abscess volume and/or alarming ophthalmologic findings,14–16 but age does not play a major role in decision-making. 14
Our study adds to this discussion, as this is one of the largest institutional cohort studies examining Chandler class III (n = 42) patients to date. Other studies have reported data on varying numbers of Chandler III patients, such as Knipping et all 22 (n = 12), Chang et all 23 (n = 16), Sciarretta et all 24 (n = 9), Crosbie et all 25 (n = 20), Quintanilla-Dieck et all 26 (n = 40), Nation et all 27 (n = 48), Tabarino et all 28 (n = 32), Todman et all 20 (n = 29), Tanna et all 29 (n = 13), Rodriguez et all 30 (n = 23), and others.1,14–16
Using a novel measurement method, we have found that an orbital abscess with a width ≥1.2 cm is associated with higher rates of surgical intervention. However, overall abscess volume was not associated with higher rates of surgical intervention in our cohort. The retrospective nature of this study limits the ability to utilize width as a clinical decision-making tool. Nonetheless, this finding adds to what has been previously reported1,7,9,10,12,17,20,21 and can serve as the basis for further studies assessing size-based indications for surgery. Of note, prior studies have commented on width, reporting >4mm, 31 >4.5mm, 32 and >10mm 33 as predictors for surgery.
Age did not play a significant role in decision-making for our patients, as children younger and older than 9 years old underwent similar rates of surgical and medical management. A recent study similarly found that age was not a key factor in predicting surgery, reporting that patients with large abscess volumes (greater than 1250 mm3) underwent surgery regardless of age. 20 A recent meta-analysis corroborated this finding as well. 14 Similar to prior studies, 34 our patients had a predominance of Streptococcus and Staphylococcus species isolated from blood and wound cultures, and we also observed four cases of MRSA. MRSA patients in this cohort all required surgical intervention; this highlights the need to consider MRSA as a potential etiology in the workup and management of SPAO.
Our study also importantly finds that, of those who will ultimately undergo surgical intervention, early intervention within 48 hours of presentation is associated with a significantly decreased overall LOS (by an average of over 3 days). Shorter LOS has numerous health-related and economic implications. The average cost of hospitalization for pediatric orbital cellulitis is nearly $21,000 per patient, with an average LOS of 5.7 days. 35 The implications of children missing days at school, and parents missing work, are important to consider. Our findings are contrary to numerous studies which have historically recommended trialing conservative therapy for at least 48 hours prior to surgically intervening.1,36–38 Of note, 28 of 28 SPAO patients ultimately required surgery in these studies after failing conservative management.1,36–38 Overall, our study is supportive of the clinical and economic benefits of early surgical intervention in appropriate candidates who are unlikely to benefit from medical therapy alone.
Retrospectively, it is difficult to fully elucidate why some patients had early vs late intervention, but the ophthalmologic exam appears to have played an integral role in identifying appropriate candidates. There was a higher rate of EOM restriction (especially grade 2 and 3 restriction), proptosis, and decreased visual acuity among the early intervention cohort vs the late intervention cohort, although this was not statistically significant (
Finally, it should be noted that all patients with superior extension of their abscess underwent surgery at our institution (5/5), and 4/5 underwent orbitotomy along with endoscopic endonasal drainage. This suggests that orbitotomy should be considered in patients with superior extension of their abscess.
There are limitations to our study. The retrospective design entails inherent biases and shortcomings, including selection and information biases. In addition, as a tertiary referral center, we treated many patients who did not follow up at our institution, and thus we may not have captured a full assessment of long-term patient outcomes. This may limit our ability to comment on the cost-effectiveness of patients’ medical and surgical care. In addition, with a relatively small number of patients and numerous statistical tests, there is an inherent chance of having inaccurate conclusions. However, we tried to allay this by utilizing appropriate statistical tests for each outcome being measured. Finally, multiple Otolaryngology attendings were involved in the decision-making process for patients over the 10-year review period, introducing some subjectivity based on surgeon preference and threshold for surgery. However, we feel that this variation makes the study more generalizable.
In addition, restricting our focus to Chandler Class III patients was a limitation of this study. However, we would argue that this was necessary in the scope of what the study aimed to achieve; we hoped to add to the discussion on medical vs surgical intervention in Chandler III patients, for whom management has been most-debated historically.1,10
Conclusion
Orbital complications from pediatric sinusitis require prompt evaluation by an otolaryngologist and an ophthalmologist. We have reported predictors of surgical intervention in this cohort, including a quantification of alarming ophthalmologic symptoms (grade 3 EOM restriction, proptosis, unreliable or poor visual acuity, APD). When indicated, early surgical intervention (≤48 hours) by ESS with or without orbitotomy leads to a decreased overall length of stay. Future studies are needed to further delineate the timing and appropriateness of surgical intervention.