
Abstract
Objective
We investigated cases with opacification on maxillary sinus computed tomography (CT) among patients with rhinosinusitis with opacification in both paranasal sinuses (bilateral rhinosinusitis) to confirm the involvement of odontogenic infections.
Methods
This study included 75 patients who were diagnosed with bilateral rhinosinusitis based on clinical examination and evident opacification on at least one side on maxillary sinus imaging with computed tomography CT. The definition of odontogenic sinusitis was determined by examining EPT and oral findings, in addition to the CT and orthopantomography (OP), by one oral surgeon and two otolaryngologists.
Results
We found that 45.3% of patients had odontogenic infections, which were associated with multiple infected teeth in some cases. Odontogenic infection was observed in both sinuses in some patients. Sinusitis with polyps was frequently associated with dental infection, and some cases were also associated with mycosis. Almost no oral symptoms were observed.
Conclusions
The results suggest that clinicians should consider odontogenic infection in patients with bilateral rhinosinusitis with opacification, on at least one side on maxillary sinus imaging. This means that accurate diagnosis may be challenging for otolaryngologist or dentists alone, suggesting that a collaboration between the two would be suitable for this task.
Introduction
Chronic rhinosinusitis (with or without nasal polyps) is characterized by the presence of two or more symptoms, one of which should be either nasal blockage, obstruction, congestion, or nasal discharge ± facial pain/pressure and/or ± reduction or loss of smell in adults, ± cough in children for over 3months. 1 Chronic rhinosinusitis (CRS) is a common condition, which frequently manifests bilaterally. Most cases of unilateral CRS are dental or mycotic in origin. While most cases of unilateral sinusitis are caused by dental or fungal infections, some may be associated with cancer or tumors, which must be considered in the differential diagnosis. 1 Several reports have indicated that 10 to 40% of cases of maxillary sinusitis are associated with or are odontogenic in origin.2–4 We confirmed the presence of odontogenic infections in 70% of patients with unilateral rhinosinusitis in our preliminary investigation, which was higher than that reported by earlier studies. 5 However, odontogenic infections could naturally be considered as an etiologic factor in patients with bilateral opacifications in the paranasal sinuses (bilateral rhinosinusitis) on maxillary sinus imaging, as it is in unilateral rhinosinusitis. Therefore, we aimed to confirm the involvement of odontogenic infections in patients with bilateral rhinosinusitis with opacification on maxillary sinus imaging.
Patients and Methods
Our study population included 75 patients who were diagnosed with bilateral rhinosinusitis based on clinical examination and evident opacification on at least one side on maxillary sinus imaging with computed tomography (CT) or orthopantomography (OP) and had visited the Otolaryngology and Oral Surgery departments of our hospital between 2005 and 2012. We defined sinusitis with opacification in the right and left paranasal sinuses and opacification in at least one maxillary sinus on CT as bilateral rhinosinusitis with maxillary sinus opacification. The presence or absence of odontogenic infection was confirmed before surgery. Rhinosinusitis was diagnosed according to the criteria set by European position paper, i.e., patients with more than two symptoms, one of which should be either nasal blockage, obstruction, congestion, or nasal discharge ± facial pain/pressure and/or ± reduction or loss of smell in adults, ± cough in children for over 3 months. 1 We excluded patients with less than two points on the Lund-Mackay score 6 and those with cystic disease or paranasal or sinonasal tumors. We defined cases with odontogenic origins, based on the diagnostic criteria reported by Matsumoto et al., 5 which included CT or OP imaging findings, results of electric pulp testing (EPT), or findings of intraoral observation (inspections and percussion were performed to confirm caries, broken teeth, and swaying teeth). EPT was performed on all cases with maxillary sinus opacification. We used the imaging findings of periodontal disease, apical periodontitis, periodontal cysts, fractured or decayed teeth, and jaw necrosis-induced osteomyelitis to indicate odontogenic infections. An otolaryngologist examined the endoscopy findings and sinus culture. We further studied these findings with the help of an oral surgeon, to investigate the involvement of odontogenic infections in bilateral rhinosinusitis.
This study was approved by our ethics committee (R01-137).
Results
We investigated a total of 75 patients, of which 41 were men and 34 were women. Their ages ranged from 10 to 74 years (mean age: 45.9 years). We confirmed the involvement of odontogenic infections in 34 patients (45.3%), of which 20 were men (28-71 years, mean age: 46.9 years), and 14 were women (21-74 years, mean age: 52.3 years). Fourteen patients had bilateral odontogenic infection, while unilateral odontogenic infection was observed in 20 patients. The percentage of patients with bilateral odontogenic infection was 41.1%. Unilateral infection with sinusitis was observed on the right side in 8 patients and on the left side in 12 patients (Figure 1). Most infections originated from the first molar (24 cases), followed by the second molar (20 cases), second premolar (8 cases), first premolar (7 cases), lateral incisor (3 cases), central incisor (2 cases), canine (2 cases), while the infection originated from multiple teeth in 26 cases. According to the imaging findings of odontogenic infections, 24 cases were of apical periodontitis, 16 of periapical lesion, 8 of periodontal cysts, and 12 cases showed evidence of multiple infections (periapical lesion + periodontal cyst = 3, periapical lesion + apical periodontitis = 6, periodontal cyst + apical periodontitis = 1, periapical lesion + periodontal cyst + apical periodontitis = 2). CRS was observed with polyps in 26 cases and without polyps in 7 cases; fungal sinusitis was observed in 1 case (Figure 2). Twenty-one cases had polyps bilaterally (9 were bilateral odontogenic infection, 12 were unilateral odontogenic infection), 5 cases had polyps unilaterally and odontogenic infection were on the same side of polyps (Figure 3). Patients complained mainly of nasal symptoms such as nasal obstruction, nasal discharge, or hyposmia. Only two patients had oral symptoms such as gum swelling and tooth pain. Symptoms were olfactory dysfunction in 19 patients, nasal congestion in 11 patients, nasal discharge in 8 patients, and post-nasal drip in 3 patients. Nasal endoscopy revealed polyps in 26 patients and nasal discharge in 8 patients. A culture test was performed on 8 patients with nasal discharge out of 34 patients with dental sinusitis. Consequently, there were 7 cases of Staphylococcus aureus, 4 cases of Pseudomonas aeruginosa and Streptococcus, 1 case each of MRSE, Neisseria and Citrobacter koseri, and 1 case of Gram-positive cocci although the bacterial strain could not be identified.

Site distribution of odontogenic sinusitis. Twenty patients had unilateral odontogenic sinusitis (12 on the left side and 8 on the right side) and 14 patients had bilateral odontogenic sinusitis.
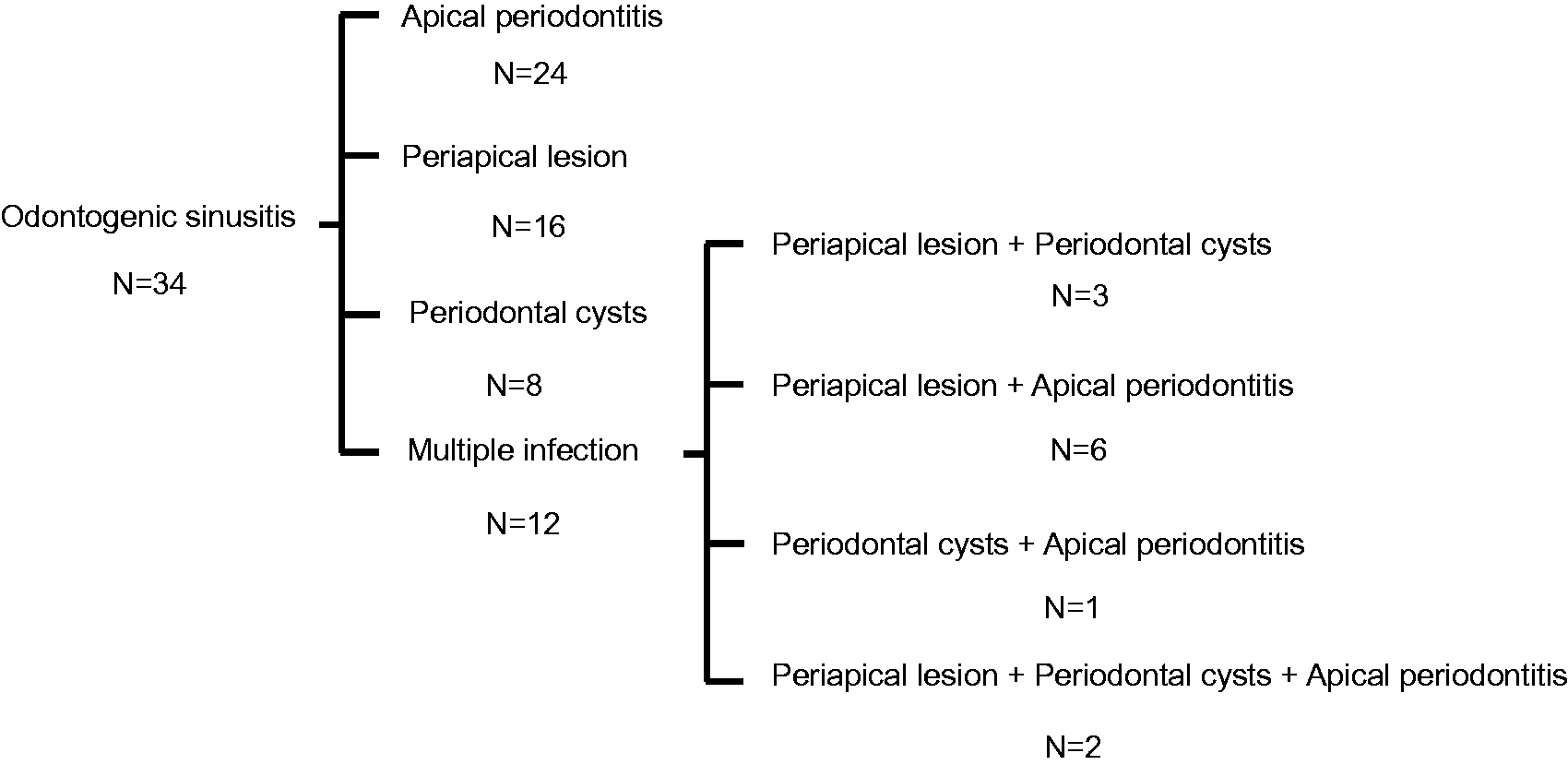
The frequencies of dental pathologies in Odontogenic sinusitis.

Clinical features of bilateral rhinosinusitis with opacification in the maxillary sinus. The highest frequency of complications was observed with chronic rhinosinusitis with polyps. CRS: chronic rhinosinusitis.
Discussion
CRS usually occurs with bilateral opacification of the paranasal sinuses. It can have a variable pathological presentation, including bacterial infection-induced neutrophilic inflammation, or eosinophilic inflammation like eosinophilic sinusitis. 1 Several epidemiological studies have suggested that sinusitis of dental origin, including odontogenic maxillary sinusitis, usually presents as unilateral rhinosinusitis, 7 where odontogenic infections are often taken into consideration in the differential diagnosis. However, odontogenic sinusitis and paranasal mycosis may be excluded from the differential diagnosis of bilateral rhinosinusitis, as they are usually associated with unilateral rhinosinusitis. However, the pathological changes associated with odontogenic sinusitis can occur bilaterally. Therefore, clinicians should consider this possibility in patients with bilateral opacifications in the paranasal sinuses. Several studies have reported that the incidence rate of odontogenic maxillary sinusitis coincides with that of unilateral rhinosinusitis. We should be aware that odontogenic sinusitis is most commonly a unilateral condition.1,5,8 However, we were able to find only a few studies on the involvement of odontogenic infections in bilateral rhinosinusitis during our search of the literature.7,9,10 While there were no reports in the past, we show the involvement of odontogenic infection in bilateral sinusitis with maxillary sinus opacification on at least one side. We examined 75 patients with sinusitis who had at least one maxillary sinus opacification and multiple sinus opacification on both sides. Odontogenic sinusitis is a clinically defined condition. Patients with sinusitis were selected based on symptoms, intranasal findings, and Computed Tomography (CT), orthopantomography (OP), intraoral findings and EPT results, and all examinations were performed in the presence of two otolaryngologists. It was judged by one oral surgeon to be applicable. As a result, 34 cases (45.3%) of bilateral sinusitis showed the involvement of odontogenic sinusitis. There were 14 cases (16.7%) of dental sinusitis on both sides and 20 cases (26.7%) of odontogenic sinusitis on only one side. Molars were most common source of infection in unilateral rhinosinusitis. Multiple teeth were responsible unilaterally or bilaterally. The spread of inflammation from the responsible teeth to the apical area was thought to be the cause of sinusitis in all 34 patients. Zirk et al. conducted a study on odontogenic maxillary sinusitis and reported bilateral manifestations in 7.4% of patients, 7 and Molteni et al. reported that 94.5% had unilateral maxillary opacification, while only 5.4% started as bilateral inflammation. About 34.6% of the latter cases presented a bilateral odontogenic focus, while the other remaining 65.4% had a history of unilateral dental pathology based on a study of 480 patients, 9 while our study found that 45.3% of patients had evident odontogenic infection in bilateral sinusitis with maxillary sinus opacification on at least one side. These results suggest that odontogenic sinusitis should also be considered in patients with bilateral rhinosinusitis.
Several studies have reported that the incidence rate of maxillary sinusitis of odontogenic origin ranges from 10 to 40%,2–4 while we observed a significant level of involvement of odontogenic infections in our investigation on bilateral rhinosinusitis. This may be related to our collaboration with the oral surgery department of our hospital. We suspected the involvement of odontogenic infections, irrespective of the unilateral or bilateral manifestation, while confirming the presence of opacification in the maxillary sinus on CT of the paranasal sinuses, and performed conservative treatment combined with tooth extraction or endodontic or periodontal treatment at the oral surgery department of our hospital. Therefore, it is possible that co-investigation with dentists for the confirmation of the presence/absence of odontogenic infections was responsible for the strong association observed in our study.
The number of patients with rhinosinusitis with polyps was rather high in our study, probably due to the refractory pathology of odontogenic sinusitis. In this group, interestingly, we had two cases of intractable pathology of eosinophilic rhinosinusitis. We diagnosed those cases with eosinophilic sinusitis based on their symptoms and clinical observations and performed ESS. 11 However, we confirmed the presence of mild opacification mainly on maxillary sinus CT during follow-up. The recurrence of eosinophilic sinusitis should have been predominant in the ethmoid sinus, 12 while those cases showed lesions mainly in the maxillary sinus. Therefore, we conducted a closer examination, since we suspected the involvement of odontogenic infections. We also performed dental treatment, which improved the clinical outcome, owing to the high probability of odontogenic infection involvement observed in the apical area on OP. Combined therapy (with dental treatment) was effective in both patients. We should consider the possibility of complications with odontogenic infection-induced neutrophilic inflammation in addition to eosinophilic inflammation.
Complications can occur with eosinophilic sinusitis or fungal sinusitis in odontogenic sinusitis. Our results suggest that various clinical conditions should be always considered while treating these complications, which is supported by the study by Matsumoto et al. on unilateral rhinosinusitis. 5
Inflammation tends to spread to areas connected to the maxillary sinus in cases of odontogenic sinusitis, and over 80% of patients with apical lesions with the maxillary molars show thickening of the maxillary sinus mucosa, and the lesions tend to increase in number, according to age. 13 Therefore, confirmation of the presence/absence of odontogenic infections in all cases with evident opacification at the maxillary sinus seems to be essential. Another study reported that patients presenting with halitosis or maxillary pain, in addition to nasal discharge, required dental treatment. 14 However, the patients in our study were mostly unaware of subjective oral symptoms even if the involvement of odontogenic infections was probable, and lesions were discovered for the first time by dentists during the diagnostic procedure in several such cases. A dentist who cannot identify odontogenic sinusitis would find it difficult to identify the involvement of odontogenic infection in sinusitis. Communication between dentists and otolaryngologists can facilitate proper diagnosis and effective treatment of this disease.
Although some items in the treatment guidelines for odontogenic sinusitis are currently under investigation, 15 it has been reported that surgical treatment has proven to be adequate and effective for patients of Odontogenic sinusitis and sinonasal complications of dental disease treatment. 11 In addition, it has been reported that extraction of causative tooth is an effective treatment of chronic odontogenic sinusitis caused by apical periodontitis. 16 We used a combination of otorhinolaryngological and dental treatment for patients with sinusitis and apical lesions. We performed surgery after conservative treatment, if the outcome was thought to be poor.
The results of our investigation and that by Matsumoto et al. 5 suggest that clinicians should consider the involvement of odontogenic infections in patients with opacification in the maxillary sinus, irrespective of the laterality (unilateral or bilateral) of presentation. They should also consider the multiple pathological manifestations of sinusitis and plan treatment accordingly.
One of our study’s limitation was the sample size of 75 patients who were diagnosed with bilateral rhinosinusitis based on clinical examination and evident opacification on at least one side on maxillary sinus imaging. We should intend to include a larger sample size for this analysis in the future.
Conclusion
There are only a few published studies on bilateral rhinosinusitis and the involvement of odontogenic infections (compared with those on unilateral rhinosinusitis), as suggested by the results of this study. When diagnosing patients with sinusitis with maxillary sinus opacification, it is necessary to consider whether odontogenic sinusitis is on both sides or on one side, and confirm nasal findings such as the presence or absence of polyps and oral findings. Cooperation with not only otolaryngologists but also oral surgeons is important for the diagnosis and follow-up of odontogenic sinusitis.
Footnotes
Authors’ Note
Copyright © 2020 Yuma Matsumoto et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Ethical Approval
This study was approved by our institutional review board.
Data Availability
The data used to support the findings of this study are available from the corresponding author upon request.
Disclosure
The corresponding author had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.