
Abstract
Introduction
The fungal balls of the paranasal sinuses are usually seen in the maxillary and sphenoid sinuses. Although, the lesion of the concha bullosa, without sinus participation, is very uncommon. We report the case of a fungal ball of concha bullosa in an 88-year-old patient.
Objective
The objective of our review of literature is to investigate the epidemiological, clinical, paraclinical, and therapeutic characteristics of patients diagnosed with fungus ball in concha bullosa.
Methods
A case of a patient who was diagnosed with concha bullosa of a fungus ball is reported. Demographic data, clinical presentation, imaging, and treatments were recorded. Key images were obtained. A review of the literature was also performed.
Results
A total of 12 cases have been reported so far in the literature revealed by different symptoms. The mean age was 38.8 years and the gender ratio was ∼12 (female):1 (male). The endoscopic surgical approach was the most frequently used treatment and provides good outcomes. Neither postoperative complications nor recurrences were noted, however, there is insufficient follow-up data.
Conclusion
Concha bullosa fungal ball is a rare diagnosis that can be revealed by different symptoms. It should be considered in patients with and unexplained chronic facial pain. A preoperative computed tomography scan is an essential tool in making a diagnosis. Endoscopic surgery is the treatment of choice, with a low morbidity and recurrence rate.
Introduction
Concha bullosa (CB) is a pneumatization of the middle turbinate, it is a very common anatomical variation with a prevalence ranging from 14% to 53%. 1 The exact cause is still unknown. 2 The most accepted hypothesis is the expansion of sinus pneumatization into the turbinate during the intrauterine period. 3 The second hypothesis is the fusion abnormality in intrauterine development. The chondral lamella and ossification areas were emerged between the fifth and seventh months of the intrauterine period and fused in the ninth month. Fusion abnormality might lead to CB during this period. 2
Several types of sinonasal diseases have been attributed to fungal pathogens. Fungus balls are extra mucosal dense accumulations of degenerating fungal hyphae especially within chronically inflamed paranasal sinuses ascribed to infection by Aspergillus spp. which are the most frequently documented fungal agents associated with the disease but we can also find other pathogens in some cases such as Mucor spp., Candida, and Aureobasidium. It is common in the maxillary sinus followed by the sphenoid sinus. Fungal diseases of the paranasal sinuses are categorized as either invasive or noninvasive based on the presence or absence of tissue invasion. Most patients diagnosed with fungal balls (FBs) are either asymptomatic or present with nonspecific signs similar to those of chronic sinusitis.4,5 FB in a CB is considered to be a rare location, only 14 cases were reported in the literature to the best of our knowledge. The objective of our review of literature is to highlight the epidemiological, clinical, paraclinical, and therapeutic characteristics of patients diagnosed with fungus ball in CB.
Methods
Ethical approval has been exempted by our institution. Written informed consent for publication of their clinical details and/or clinical images was obtained from the patient. A case of a patient who was diagnosed with CB of fungus ball is reported. Demographic data, clinical presentation, imaging, and treatments were recorded. Key images were obtained. A review of the literature was also performed. A literature search was performed using the PubMed/MEDLINE database for the following keywords: “Concha Bullosa,” “Fungus Ball,” and “Aspergillosis.” Articles in English whose full texts could be obtained were included. To date, 14 cases of FB of CB have been identified in the literature, of which 12 were available in English and amenable to review.
Results
Case Presentation
An 88-year-old woman with a history of multiple myeloma treated with chemotherapy was presented to our ENT department with facial pain, chronic nasal obstruction, and postnasal discharge for the past 2 years. An endoscopic examination revealed a prominent left middle turbinate and right septal deviation. The nasal mucosa was normal and no pus was detected. A paranasal computed tomography (CT) scan showed chronic sphenoidal sinusitis, as well as a CB of the left middle, turbinate filled with a high-density material (Figure 1). A paranasal magnetic resonance imaging (MRI) revealed a CB filled with a material iso signal T1 heterogeneous signal T2 with a central void signal measuring 14 mm related to a FB associated with a nonspecific chronic sphenoidal sinusitis (Figure 2). The patient was counseled on the need for surgery, but she refused any surgical intervention and insisted on conservative management.
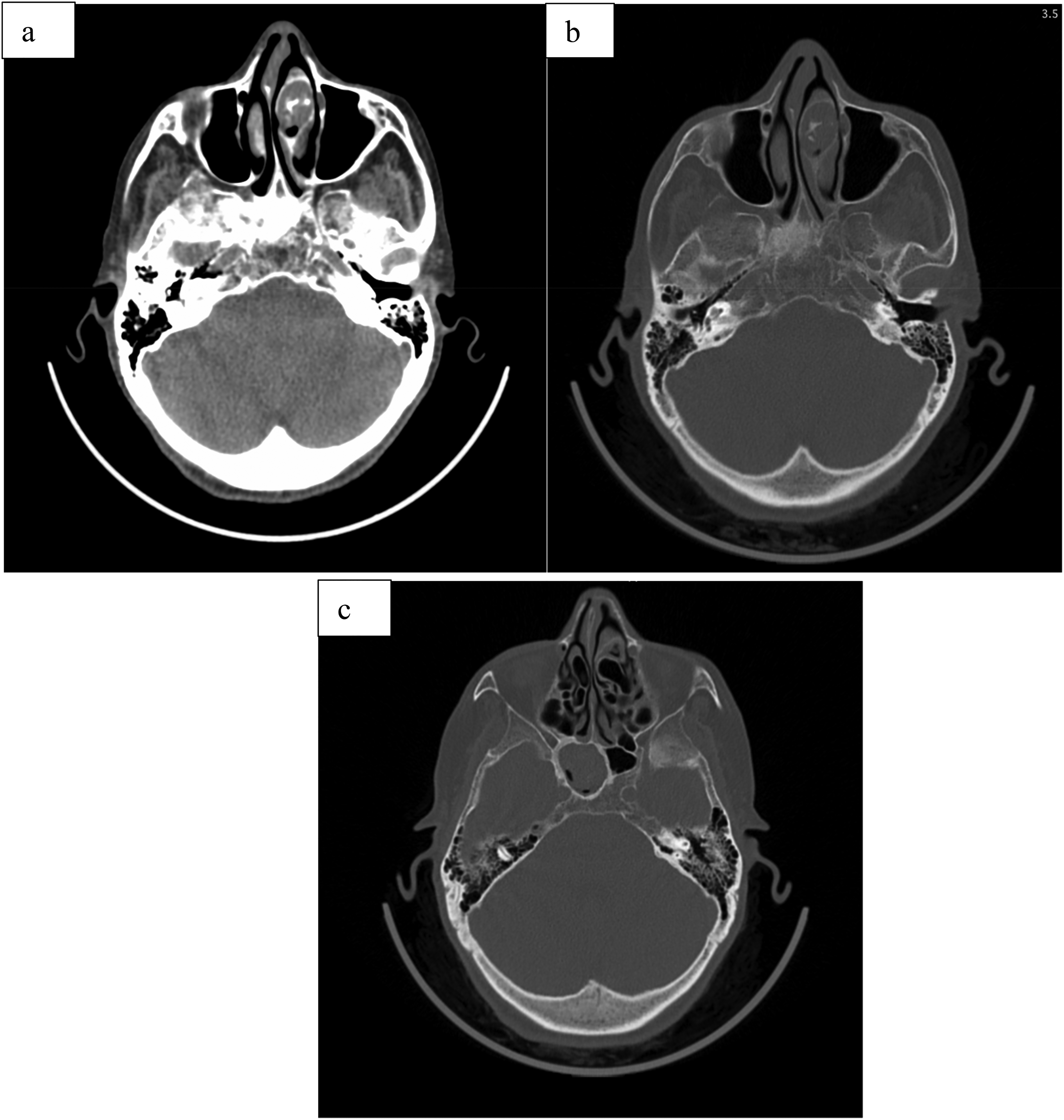
Paranasal computed tomography (CT) scan: (a), (b) axial section: concha bullosa of the left middle turbinate filled with a high-density material, and (c) axial section: chronic sinusitis of the right sphenoidal compartment.

Paranasal magnetic resonance imaging (MRI): (a) left concha bullosa filled with a material heterogeneous signal T2 with a central void signal related to a fungal ball and (b) nonspecific right chronic sphenoidal sinusitis.
Therefore, the patient was placed on symptomatic treatment; analgesic, and nasal irrigation with a mild improvement. On the subsequent follow-ups, she had remained stable.
Literature Comparison
Findings from the patient in our case compared with 12 cases reported in the literature are presented in Table 1.
Clinical Radiological and Histopathological Features of Fungus Ball in Concha Bullosa Reported in the Literature.

Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging; F, female; M, male.
Blank cells indicate absent or no mention of data in patient charts or case reports.
NED indicates no evidence of disease.
Discussion
Our current review gathering all these 12 studies is the first in the literature. It emphasizes the epidemiological, clinical, radiological, and histopathological findings of FB in CB in comparison with other locations.
CB is a pneumatization of the middle turbinate, it is a very common anatomical variation with a prevalence ranging from 14% to 53%. 1
Several types of sinonasal diseases have been attributed to fungal pathogens. An FB can be defined as a dense accumulation of extra mucosal fungal hyphae, most commonly in the maxillary sinus, ascribed to infection by Aspergillus spp., which are the most frequently documented fungal agents associated with the disease. Other pathogens can be found in some cases such as Mucor spp., Candida, and Aureobasidium. Involvement of an FB in the sphenoid sinus comprises 4.5% to 26.8% of cases. 18 FB can affect adult patients in almost all cases with a higher incidence in older ones. 4 Fungal rhinosinusitis includes various forms with different pathophysiologies, they can be categorized into noninvasive types: saprophytic fungal infection, FB, allergic fungal rhinosinusitis and invasive ones, acute and chronic forms. 19 Various terms, such as mycetoma, aspergilloma, and chronic noninvasive granuloma have been used interchangeably in the literature to designate sinus FB. 19 Up to now, these terms have been abandoned.
FB in a CB is considered to be a rare location, only 14 cases were reported in the literature to the best of our knowledge. According to DuFour et al 20 conducting a case series study of 173 patients with FB in a CB, they have only described 2 cases without any clinical or radiological information. Furthermore, in the study of Yoon et al 21 gathering 538 patients, any cases of FB in CB were identified. Moreover, the association with sphenoiditis is described for the first time in our case report as far as we can tell.
The incidence of FB is constantly increasing. The percentage of FBs to the total cases of endoscopic sinus surgery (ESS) was only 3.55% in 1996 versus 13.99% in 2015. 22 While no definite reason for this increase is apparent, it is thought to be the result of improved knowledge of the disease, improved diagnostic technologies, including nasal endoscopy and imaging tools, as well as the abuse of broad-spectrum antibiotics, and the population aging. 21 The maxillary sinus is the most frequently affected site (86.1%), followed by the sphenoid (4.5% to 26.8%), 18 but its incidence in CB is still unknown and uncommon reflected by the low number of cases reported in the literature.
In the literature, the mean age is 39.8 years with extremes ranging from 13 to 88 years old. Women were the most affected (92.3%) with a sex ratio of 12:13. It was also reported in Yoon's study (363 female patients [67.5%] vs 175 [32.5%]) as well as DuFour with a female predominance of 60.1%. Ferguson 23 suggest that the higher female rate may be due to the longer life expectancy of women in western populations, several studies have suggested that environmental and hormonal factors can be involved in the pathogenesis of FB.20,23,24 Same epidemiological findings in our case report.
Considerable controversy surrounds the pathogenesis of this disease: Some authors 25 have suggested that the cause of the infection is the colonization of the sinus by the material used for root canal treatment in dentistry, however, this theory cannot explain the location of fungus balls in a CB. For other authors, the infection would be caused by the inhalation of spores, which may be present in a saprophytic state in the sinus, whose proliferation is promoted through anaerobic conditions responsible for the development of the fungal agent. 26
FB in CB has manifold clinical presentations with unspecific symptoms, however, nasal obstruction, hyposmia, and facial pain were the most frequent reasons for consultations (Table 2), consistent with our patient's symptomatology. This is in line with the results found in DuFour and Yoon's studies except for rhinorrhea which is much less frequent for FB in CB; only 8.3%. It is around 50% for other locations of FB. In the literature, all the patients with FB in CB were symptomatic. In contrast, a fungus ball located in the maxillary sinus may be totally asymptomatic. 20 Patients with FB of sphenoid sinus can be presented with headache and visual disturbances that can be explained by the variation of its size and pneumatization as well as the important anatomical structures that lie adjacent to the sphenoid sinus (eg, cavernous sinus, pituitary gland, internal carotid artery, and cranial nerves II, III, IV, V1, V2, and VI). 27 The reflective facial pain of FB either in the paranasal sinus or in CB can be related to the fact that the anterior craniofacial structures are innervated by branches of the trigeminal nerve, and stimulation of various intranasal mucosal regions may cause pain that is felt in the cutaneous distribution of the ophthalmic (V1) or maxillary (V2) division. 28 Another possibility is that the fungus ball may cause mucosal inflammation by 3 mechanisms. First, the fungus ball may act as the site of bacterial infection, which causes acute bacterial mucosal inflammation. Second, obstruction of the natural ostium of the sinus by the fungus ball itself may cause acute mucosal inflammation. Third, the fungus ball itself provides soluble antigens or irritants that may cause mucosal inflammation. 12
Different Symptoms for FB in CB Described in the Literature.

For FB in CB, clinical examination is unspecific: middle turbinate hypertrophy and septal deviation are the most frequently encountered clinical signs, in accordance with what we have found in our case report. Nasal septal deviation is probably attributed to pneumatized middle turbinate explained by the gradual mass effect caused by CB.
Cone beam, CT scan, and MRI can all help in the diagnosis of FB. The Gold standard imaging technique is a CT scan showing different aspects: homogenous, heterogenous filling, and calcifications. Metal dense body images have been attributed to zinc oxide from overfilled dental cavities, 29 however, this theory cannot explain what is found in CB. It is likely due to metal ions deposited within necrotic areas of the mycelium. 30 Intrasinus calcifications or metallic densities are highly suggestive of a fungus ball. 31
Today we have many radiological studies available that describe other characteristics of the disease. According to the retrospective study of Ho et al conducted in 2018 evaluating the diagnostic features of maxillary sinus fungus ball (MSFB) on CT scan, focusing on patients without intralesional hyperdensity (IH), and found that sclerosis of the lateral sinus wall erosion of the inner sinus wall, and irregular surface of the material were significantly more common in the MSFB without IH group than in the unilateral chronic rhinosinusitis (UCRS) group. Erosion of the inner sinus wall and irregular surface of the material had the highest specificity and positive predictive value (PPV). In the subgroup of patients with total opacification of the maxillary sinus, the sensitivity, specificity, PPV, and negative predictive value (NPV) of erosion of the inner sinus wall were all >90%. When reading the preoperative CT images of the sinus as a first step, unilateral opacification of the maxillary sinus with IH or calcification is suggestive of a diagnosis of MSFB. Erosion of the inner sinus wall is a good indicator of MSFB when there is total opacification of the maxillary sinus. However, the irregular surface of the material can be used to distinguish MSFB from UCRS if there is partial opacification of the maxillary sinus. 32 To date, there is no study describing these radiological features in the case of FB of CB. MRI is a more reliable tool for the diagnosis of sinonasal fungus balls. However, not all patients can afford it due to its high cost. MRI shows typical features of sinonasal fungus ball 33 : hyper signal intensity portions in the fungal mass on T1-weighted images in conjunction with dark signal lesions surrounded by high signals, hypertrophic mucosal walls in paranasal sinuses on T1-weighted.
A CT scan associated with MRI provide sufficient information for the preoperative differentiation of a sinonasal fungus ball from other forms of sinusitis. 33
In the literature, the most common imaging technique used to diagnose CB FB was CT scan, used in all cases (100%) versus MRI that was used in only 3 patients (23.1%). According to the study of DuFour et al 20 and what we have analyzed from all the radiological findings in all the studies that we gathered from the literature, there were 3 different aspects of sinus CT scan that were identified: homogenous filling (38.5%), heterogenous image (38.5%), and microcalcifications (23.1%). (Table 1)
On MRI findings, there was an image in hyper signal T1 and signal void T2. It is interesting to note that 2 patients (15.4%) had involvement of the surrounding structures detected on imaging; anterior ethmoidal, sphenoidal sinus as well as middle turbinate for the first patient versus sphenoidal sinus for our case report. This sphenoidal lesion can be explained probably by a different pathophysiology.
Histopathology is the most sensitive way to confirm the diagnosis. As a matter of fact, 69.2% of the cases reported have been confirmed using this technique (Figure 3). Noting that 3 (23.1%) cases did not report their histopathology results.

Endoscopic photograph showing a fungus ball in the right concha bullosa. This figure has been reproduced with permission from Ozkırıs et al. 16
Another relevant finding is the percentage of microbiological isolation. In our study, culture was positive in 38.5%. This percentage is relatively high compared to the general literature of FB (22%-34%). Aspergillus spp. has been most frequently identified, it was reported in 4 cases (30.1%) (Table 3).
The Mycology Results Found in the Literature.

The treatment of this disease is exclusively surgical, 21 except in the case of general surgical contraindication. All the patients had undergone ESS except our patient for some reasons as described above. The surgical technique as reported by Bran and Stammberger. 34 Under local or general anesthesia, consists of the opening of the CB which is performed by inferior and superior incisions in front of the middle turbinate dividing it into lateral and medial parts. Then, with nasal forceps, the posterior part of the middle turbinate is cut from its insertions to remove the lateral part of the middle turbinate. In all operated patients, a brownish-yellow, soft and friable material was observed and aspirated from within the CB (Figure 4). In the case of other sinus lesions, their surgical drainage is recommended. Neither postoperative complications nor recurrences were noted, however, there is insufficient follow-up data.

Characteristic septate hyphae of Aspergillus (hematoxylin–Eosin, ×400). This figure has been reproduced with permission from Ozkırıs et al. 16
Conclusion
FB in CB has the same characteristics as the more frequent localizations.
It is an unusual and unknown entity. Clinicians should keep in mind the possibility of this disease in case of facial pain and nasal obstruction without any evident cause.
The pathophysiology is still unknown.
There is an unexplained female predominance.
The treatment is mainly surgical.
Footnotes
Acknowledgments
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical Approval
We confirm that Ethical Committee approval was not necessary, and this is acknowledged within the text of the submitted manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
We confirm that guidelines on animal rights and treatment have been met and any details of approval obtained are indicated within the text of the submitted manuscript—this statement is not relevant to our work.
Statement of Informed Consent
We confirm that guidelines on patient consent have been met and any details of informed consent obtained are indicated within the text of the submitted manuscript.