
Abstract
Keywords
Introduction
Thanks to the improvement of optics and instruments, frontal sinus surgery has evolved toward less invasive and safer surgery. Endoscopic approaches combined with navigation tools allow a more precise treatment of sinonasal pathologies while better respecting the physiology of the nose and sinuses. Challenges remain for unreachable lateral and supraorbital pathologies of the frontal sinus and for some complex anatomies of the frontal recess where an extended endoscopic approach or external approach are still necessary. The aim of any frontal sinus surgery is to remove the pathology and to prevent its recurrence while minimizing surgery-related risks and sequels.
Open surgery of the frontal sinus is indicated for neoplasia and revision cases when the endoscopic surgery is not feasible or has failed. Compared to endoscopic sinus surgery (ESS), external approaches have higher morbidity such as greater blood loss, external scarring, more risk for the supraorbital nerve, more orbital complications, and cerebrospinal fluid (CSF) leak. 1
An extended endoscopic approach such as Draf III provides adequate outcomes, with a 90.7% patency rate and a 12.6% revision rate. 2 This approach is associated with 1.3% CSF leak, 0.2% persistent anosmia, and 13% worsening of the hyposmia. 3 Moreover, Draf III in comparison with Draf IIa is associated with significantly worse extranasal and facial symptoms during the early postoperative period, requiring more follow-up visit and antibiotic use. 4
To avoid the above-mentioned drawbacks of these invasive procedures, we started to combine flexible interventional bronchoscopy with ESS through a Draf IIa approach to address lateral frontoethmoidal cells and for the treatment of lateral and supraorbital frontal sinus pathologies whose proper visualization and treatment would have required an extended approach. In 2011, Carniol et al 5 described the utility of flexible endoscopy to confirm the complete removal of lateral pathologies in the frontal sinus surgery. In 2020, Png et al 6 described the use of flexible bronchoscopy to treat a lateral frontal mucocele. We herein describe our experience in 1 revision case of frontal sinus surgery and 1 fungus ball of the frontal sinus with frontoethmoidal cell resection through a limited Draf IIa approach.
Case 1
The first case is a 64-year-old patient, presenting with a right progressive frontotemporal headache and a normal endonasal examination. The computerized tomography (CT) scan showed an expanding process in the right frontal sinus with lysis of the right orbital wall, posterior table, and interfrontal wall. There was an extension in the left frontal sinus associated with a hyperdensity consistent with a fungal infection. On the left side, there was a mucus or a fungal retention lateral to pneumatized frontoethmoidal cells (Figure 1). We performed a conventional bilateral endoscopic Draf IIa under vision with a rigid 4 mm 0° and 45° rod telescope (Karl Storz and Co) and rigid angulated instruments (Figure 2A and B). We flushed the frontal sinus through the neuronavigated Wigan suction until we obtained clear saline rinse. Despite abundant rinsing of the lateral frontal sinus as controlled with the neuronavigation, the complete visualization of the frontal sinus with the flexible bronchoscopy (Video Bronchoscope BF-P190, 4.2 mm outer diameter, Olympus) demonstrated remaining fungal material in the anteromedial part of the frontal sinus, above the frontal beck and in the lateral recess (Figure 2C, D, F and H). Direct vision allowed complete removal of the remaining fungus ball in the anterior part and in the lateral recess with rinsing through the 2 mm working channel of the bronchoscope (Figure 2E and G). Through-the-scope flexible biopsy forceps (1.8 mm biopsy forceps, Olympus) allowed the controlled removal of the left frontoethmoidal cell's wall through the right Draf IIa (Figure 3A-C). This procedure was carried out by 2 experienced surgeons, 1 handling the bronchoscope and the second the forceps to ensure good stability and control of the force used to break the cell's wall. This step lasted 20 min and we experienced excellent visualization and ease to break the thin bony wall of the cell. The patient was discharged 2 days after the surgery with minimal pain and there were no signs of recurrence after 4 months of follow up.

(A) Axial, (B) coronal, and (C) sagittal computerized tomography (CT) scan revealing mycotic sinusitis of the frontal sinuses (right>left) with lysis of the orbital wall, the posterior wall of the right frontal sinus, and the interfrontal wall. Demonstration of 2 left supraorbital frontoethmoidal cells (*) with lateral retention.

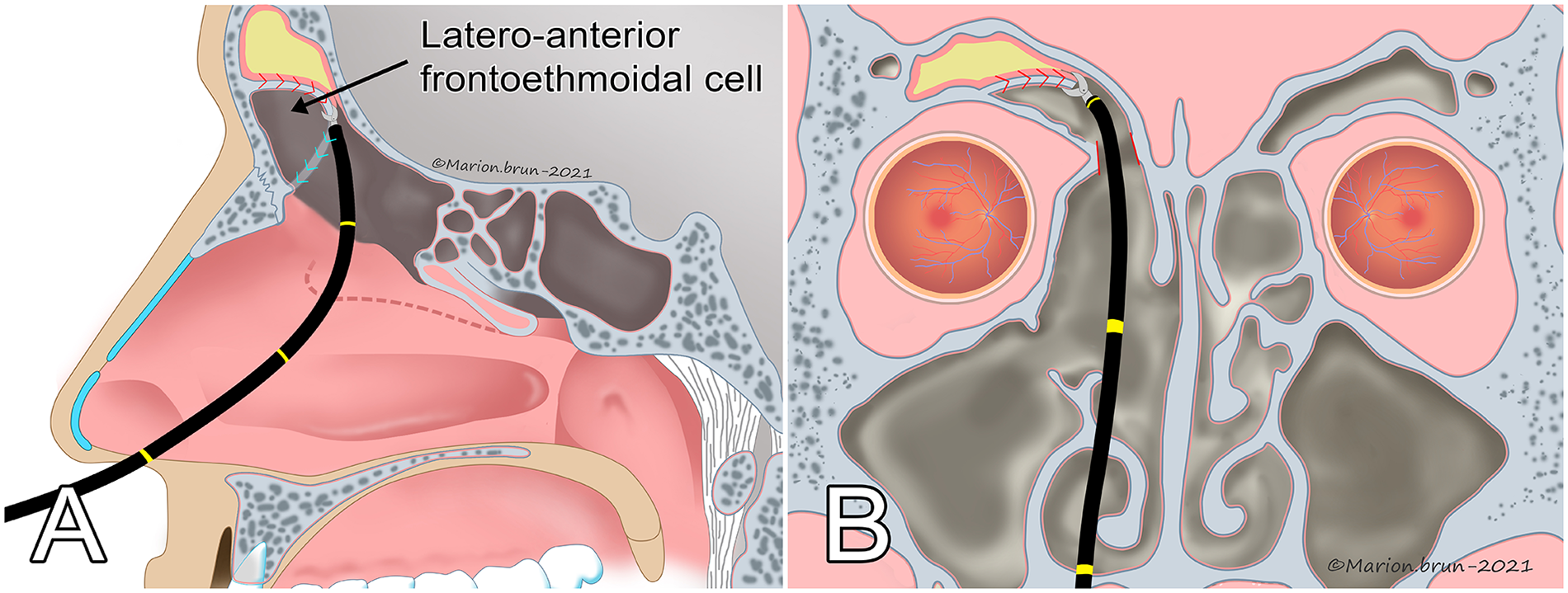
Intraoperative pictures after a right Draf IIa procedure. (A) 0° rigid optic vision, (B) 45° rigid optic vision, (C) bronchoscopic vision revealing a persistence of fungus ball in frontal sinus after rinsing using the Wigan aspiration, (D) right lateral recess before rinsing with the bronchofibroscope, (E) right lateral recess after rinsing with the bronchofibroscope, (F) medial wall of left frontal sinus before rinsing with the bronchofibroscope, (G) medial wall of left frontal sinus after rinsing with the bronchofibroscope, and (H) diagram illustrating the exploration and rising of the frontal sinuses using the bronchofibroscope through the Draf IIa.

(A) Intraoperative picture with the flexible bronchofibroscope of the left frontoethmoidal cell (* left frontoethmoidal cell, X medial part of the left frontal sinus), (B) intraoperative picture of frontoethmoid cell wall resection using biopsy forceps through the working channel of the bronchofibroscope (# superior wall of frontoethmoidal cell, ° biopsy forceps), and (C) diagram of frontoethmoid cell wall resection using flexible bronchoscope and biopsy forceps.
Case 2
The second case is a 56-year-old patient, known for chronic rhinosinusitis with bilateral frontoethmoidectomy 20 years before. He complained of progressive frontal headaches predominantly on the right side. Endoscopically, the ethmoid was open on both sides, but the frontal recess was not patent on the right side. The CT revealed retention in the right frontal sinus lateral to a frontoethmoidal cell that could be the etiology of his symptoms (frontoethmoidal cell obstructing the frontal sinus drainage path) (Figure 4A and B). Medical treatment with topical and systemic corticoid associated with antibiotics showed no improvement. The patient consented for a Draf IIA, IIB, or III if necessary. We did a conventional revision of the Draf IIa under visualization with a rigid 0° and 45° Hopkins rod telescope and Hosemann and Cobra forceps (Hosemann frontal sinus/recess punch 70° upturned and frontal sinus punch with link chain sheath 70° upturned backward cutting, Karl Storz and Co). Conventional ESS allowed opening the inferior part of the frontoethmoidal cell but not the superior and lateral walls. These were efficiently addressed in 15 min using the flexible interventional bronchoscope (Video Bronchoscope BF-P190, 4.2 mm outer diameter, Olympus) and a through-the-scope biopsy forceps with the two surgeon's technique (Figure 5A and B). We could then easily control and rinse the entire frontal sinus. The patient was discharged 1 day after surgery with a clear improvement of his symptoms. He described no recurrence at the last follow-up visit 15 months after surgery.

(A) Coronal and (B) sagittal computerized tomography (CT) scan revealing a frontoethmoidal cell (*) filling the drainage path of the right frontal sinus with lateral retention.
(A) Sagittal section and (B) coronal section of the excision of the right frontoethmoidal cell wall with the flexible bronchoscope and biopsy forceps through the working canal.
Discussion
In these 2 cases, the use of a flexible interventional bronchoscope through a Draf IIa approach could spare a more extended procedure (Draf IIb and Draf III) while efficiently treating the pathologies.
Thanks to this less invasive procedure, we induce less mucosal trauma in the frontal recess resulting in an overall less bony exposition. This reduces the known risk of chronic inflammation which could result in restenosis due to neo-osteogenesis. This phenomenon occurs at various intensities during the 2 postoperative years after a Draf III procedure. 7
A total of 15 to 20 min were required to remove the otherwise unreachable part of the frontoethmoidal cell with the bronchoscope forceps. To the best of our knowledge, these are the first cases described in the literature for those indications. The two surgeon's technique with through-the-scope biopsy forceps is a bit tedious and repetitive but avoids the above-mentioned morbidity and risks of Draf III and finally saves operating time. A nonstop clear view while using the biopsy forceps allows safe and complete resection of any thin bony wall in the frontal sinus. Thus, the risk of injury to the orbit and the base of the skull is extremely low.
Flexible interventional bronchoscopes provide excellent optical definition and are easily available with a few extra costs in most centers. They exist in different outer diameter, from 3.1 to 6 mm with working channels of 1.2 to 2.8 mm and various single use through-the-scope instruments (including biopsy forceps) are available. Its handling is very intuitive and ergonomic, making it a very useful tool to add to the classical ESS. Blood and secretions can be rinsed and aspirated to keep a clear vision. The flexible end of the bronchoscope allows thorough examination of a frontal sinus to search for residual pathology (fungus ball, inverted papilloma) after an ESS, as described in our first case above.
We reported the use of the biopsy forceps but it is also possible to use the narrow-band imaging (NBI) and/or a laser fiber to delineate and to treat tumors (eg, inverted papilloma). Through-the-scope dilatation balloons could also be used to perform distal dilatation (eg, lateral recess of the frontal sinus) under direct vision. All this technology is already used and validated for its use at the tracheobronchial level and need to be validated in ESS.
We reported the combination of classic rigid ESS and flexible bronchoscopy for hard-to-reach regions of the frontal sinus. The same technique could be applied to the lateral recess of the sphenoid sinus or the anterior wall of the maxillary sinus, hence limiting the need for extensive approaches like transpterygoid approaches in case of lateral recess pathologies of the sphenoid sinus or endoscopic prelacrymal or Caldwell luc approach for maxillary sinus surgery.
This technique is suitable for the majority of Draf IIa because the 4.2 mm bronchoscope can easily pass through the frontonasal recess which is on average 5 to 6 mm. 8 For smaller frontonasal recess, the 3.1 mm bronchoscope could be used to visualize and to rinse the frontal sinus, but an extended approach may be indicated to ensure the long-term patency of the frontal sinus drainage pathway.
The main limitation of this technique with flexible bronchoscope is the lack of tactile feedback and the lack of force that can be applied (eg, using biopsy forceps) because the bronchoscope goes backward if the instrument is pushed forward. Hence, it is currently not possible to excise a very hard lesion that would require the development of a through-the-scope burr or an anchoring system for the bronchoscope. The excision of more complex lesions (eg, tumors) by this technique is currently difficult but could be possible with the development of new flexible endoscopes with several working channels that can be rigidified on demand (robotic endoscope).
Conclusion
The use of flexible interventional bronchoscopy in ESS allows a minimal invasive treatment of lateral and supraorbital frontal sinus pathologies that are not visualizable, accessible, and treatable with rigid optics and instruments. This technique can avoid, in selected cases, more invasive procedures (extended endoscopic and external procedure). The use of the flexible bronchoscope with biopsy forceps through a Draf IIa approach allows the excision of lateral frontoethmoidal cells. This new technique requires further prospective studies to confirm its safety and long-term efficacy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from both patients for their anonymized information to be published in this article.