
Abstract
Objective
Demonstrate feasibility, safety and outcome metrics of geriatric sinus surgery (GESS).
Study Design
Retrospective review of patients undergoing sinus surgery for indication of chronic rhinosinusitis with and without nasal polyposis.
Setting
Tertiary referral center.
Participants
Patients who underwent FESS from 2008–2017; excluding skull base, craniofacial, or oncologic surgery. Primary study group were patients aged 65 years and older. Patients aged 40–64 years of age were included for comparison.
Main Outcomes and Measures: Multivariate analysis was performed to identify independently associated patient characteristics and perioperative variables. Preoperative medical and treatment history, revision and primary surgery, preoperative and post-operative SNOT-22 and NOSE scores, Lund-McKay scores were recorded when available. Post-operative data was assessed at a minimum of two months after the index procedure. Post-operative complications were included.
Results
Ninety-one (91) patients met criteria. 21.2% of the geriatric patients were taking systemic anticoagulation prior to surgery, and underwent treatment with nasal steroids (25.0%), oral antibiotics (67.7%), nasal irrigations (48.4%), and systemic steroids (37.5%) over an average of 7.3 months prior to surgery. There was an average post-operative reduction of 15.0 points (p < 0.0001) and 42.5 points (p = 0.0008) for SNOT-22 and NOSE scores, respectively. Average operative time was 117.4 minutes in geriatric patients compared to 183.4 minutes in younger patients (p = 0.004), with an average estimated blood loss of 55.6 milliliters (mL) compared to younger patients (111.8 mL) (p = 0.04). Linear regression identified revision surgery as associated with reductions in Sinonasal Outcome Test (SNOT-22) scores (p = 0.011). Geriatric patients had a shorter operative time (p = 0.011) while male sex was associated with a longer operative time (p = 0.014). Patients over 65 had fewer minor complications (p = 0.01), and there were no major complications in either group.
Conclusions and Relevance
Geriatric sinus surgery is effective and safe in this cohort of patients.
Introduction
Chronic rhinosinusitis (CRS) is the sixth most common disease affecting the elderly population. 1 The scope of the disease and the fundamentals of its management have been well described in the Otolaryngology literature, yet limited data exists to codify surgical outcomes of functional endoscopic sinus surgery in a geriatric cohort (GESS). Otolaryngology practice is being fundamentally altered to care for an increasingly aged population, and as such more data is needed to describe the surgical management of geriatric patients suffering from CRS.
The study clarifies the impact of functional endoscopic sinus surgery (FESS) to manage symptoms of CRS in geriatric patients compared to a cohort of younger peers, the number of complications in this age group, and compare our data to the existing literature. We hypothesize that the risk of surgery is mitigated by potential benefits from the operative management of CRS in geriatric patients and that the risk of surgery is acceptably low.
Our study retrospectively assesses the extent of improvement in parameters such as Sinonasal Outcome Test (SNOT)-22 scores, operative time, blood loss and intraoperative complications during FESS compared to a demographically matched younger cohort.
Methods
A retrospective chart review between 1990 to 2017 was performed on a geriatric cohort of patients aged 65 years and older and control patients (aged 40 to 65 years of age) who underwent endoscopic sinus surgery for indication of chronic rhinosinusitis with and without nasal polyposis at two tertiary-level hospitals and one Otolaryngology specialty hospital. Presbynasalis has been broadly defined as occurring in patients older than 60 to 65. 2 In our study we included patients 65 years and older as our geriatric age group. While there are differing definitions for what defines an elderly-person, a commonly used cutoff for a geriatric patient is 65 years old. 3 A broad age range of 40 to 64 years old was chosen for the control group; this was felt to represent an appropriate age range comparator with the geriatric cohort given the range was also quite large (65 to 90 years old). The patients of three academic Rhinologists, one senior faculty and two junior faculty were chosen for chart review.
Preoperative medical history as well as treatment history was annotated, with special attention to nasal irrigations, intranasal steroid use, oral steroids, intranasal decongestants, and antibiotic usage. Patients undergoing revision and primary surgery were included. The datasets were queried to identify cases with any of the following Current Procedural Terminology (CPT) codes: 31254, 31255, 31276, 31287, 31288, 31256, 31267, and 61782. Preoperative and post-operative SNOT-22, Nasal Obstruction Symptom Evaluation (NOSE) Lund-McKay scores were recorded when available. Post-operative scores were assessed at a minimum of two months after the index procedure. Post-operative complications were noted.
Results
Demographic Data
91 patients met inclusion criteria, 67 geriatric and 24 matched controls. In the combined cohort 39 (42.9%) were male, mean pre-operative SNOT-22 and NOSE scores were 40.7 and 74.7 respectively. 35/67 (52.2%) and 13/24 (54.2%) SNOT-22 scores were available while 6/67 (9.0%) and 13/24 (54.2%) NOSE scores were available for the geriatric and non-geriatric cohorts, respectively. Of the data available (19/24 non-geriatric and 65/67 geriatric patients), 36.8% (7/19) of non-geriatric patients had polyps while 55.4% (36/65) of geriatric patients had polyps. Reports of allergic testing was not available for this cohort. A majority of the elderly combined with control patients followed a pre-operative medical regimen. In the combined group, 37.7% using nasal steroids, 69.8% taking oral antibiotics, 51.2% used some form of high volume nasal irrigation (with or without steroids), and 38.8% had been on an oral steroid prior to the index procedure. On average in the combined geriatric and non-geriatric cohorts, patients were treated 7.5 months prior to surgery. 9.1% were active smokers, 43.2% were former tobacco users, 15.9% were using an anticoagulant prior to surgery, and the most common premorbid conditions were hypertension (36.3%), coronary artery disease (13.2%), and hyperlipidemia (11%). The two groups were well matched with some exceptions. Geriatric patients were less likely on pre-operative nasal steroids (25% versus 76.2%, p = 0.0001), more likely to be taking anticoagulation (21.2% versus 0%, p = 0.017), and more often hypertensive although this fell short of significance (41.8% versus 20.8%, p = 0.07). Among geriatric patients with available ASA data (53/67), 45.3% had an ASA class greater than 2, one patient was ASA 4 (Table 1). No ASA data was available in our comparison group.
Clinical and Demographic Data With Statistical Analysis for Geriatric and Non-Geriatric Patients Undergoing Sinus Surgery.

Abbreviation: COPD, chronic obstructive pulmonary disease.
*Outcomes presented as N (%) unless otherwise noted.
Surgical Outcomes
The majority of patients were discharged home uneventfully following sinus surgery in the operating room and general anesthesia. Eight geriatric patients admitted subsequent to the sinus procedure (12.1% versus 0% of younger patients, p = 0.19). In patients admitted overnight, 87.5% were admitted for pain, one patient was admitted for pain and urinary retention, and one of the patients admitted for pain was also admitted for management of a hypertensive episode; 87.5% of admitted patients required only one day of inpatient care. Operative time was significantly shorter in the geriatric cohort (117.4 minutes versus 183.4 minutes, p = 0.004). Additionally, geriatric patients had a lower mean blood loss (78.4 milliliters versus 106.9 milliliters, p = 0.04). In both groups, post-operative average SNOT-22 scores fell significantly from original values, however geriatric patients had a lower percentage change in their post-operative average SNOT-22 scores (−38.1% reduction versus −72.9%, p = 0.0009). NOSE scores fell significantly in both cohorts (−42.5 in geriatric patients, p = 0.0008 and −45.0 in non-geriatric patients, p = 0.0006). There was no statistical difference when comparing the change in NOSE scores between the two groups (p = 0.87). Minor complications were collated and most frequently included pain and epistaxis, minor complications were more likely to occur in the non-geriatric patients (7.5% versus 41.7%, p = 0.0001) and no major complications occurred in either group. Of note, geriatric patients were less likely to be prescribed post-operative nasal steroids (33.9% versus 69.6%, p = 0.003) or nasal irrigations (74.2% versus 95.7%, p = 0.03) and more likely to receive systemic steroids then their counterparts (50% versus 17.4%, p = 0.007). No differences were noted in the prescribing patterns for post-operative antibiotics (Tables 2 and 3).
Post-Operative Outcomes for Geriatric and Non-Geriatric Patients Undergoing FESS.
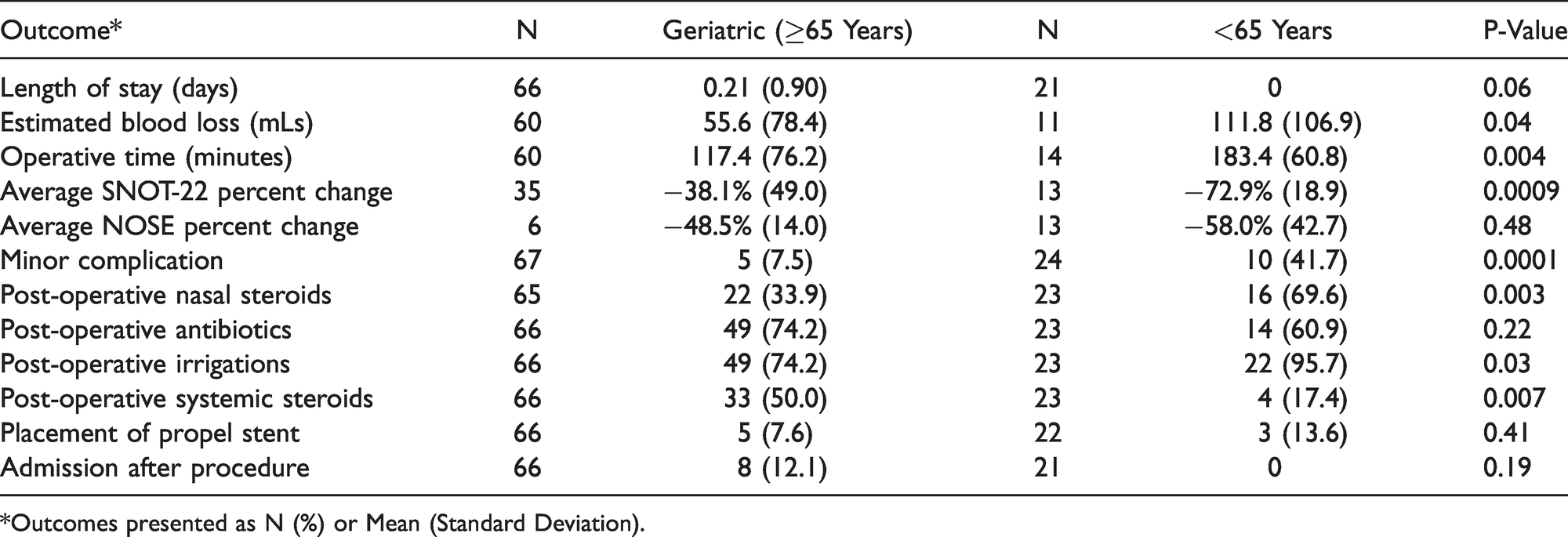
*Outcomes presented as N (%) or Mean (Standard Deviation).
Effect of Geriatric Status Using Adjusted Analysis.

*Data presented as odds ratio for categorical variables with [95% confidence interval] and point estimates for continuous variables with (standard error).
Discussion
This study adds to a relatively sparse literature concerning GESS. Our study demonstrated no adverse outcomes in our geriatric cohort and identified good outcomes post-operatively. This is an important finding, as CRS is the sixth most common condition of the elderly and has considerable morbidity. 1 Geriatric CRS mirrors adult CRS, and features multiple symptoms including nasal stuffiness, postnasal drip, cough, impaired olfaction, odynophagia and fever of unknown origin. Geriatric CRS can also cause hallucination, cognitive dysfunction, and delirium and is thus especially critical to treat in this population. 4 The elderly sinusitis patient represents a vulnerable population, as many are hearing impaired, have a higher incidence of balance disorders, atrophic rhinitis, olfactory dysfunction, and dysphagia and often require a greater number of social resources post-operatively. 5 Elderly patients may also be more susceptible to side effects from prolonged medical management such as antibiotics. Nonetheless, Marioni et al demonstrated that geriatric patients can be safely and successfully managed with a similar surgical treatment algorithm and approach as what is used for younger adults. 6
Our data demonstrates that geriatric patients have reduced operative time and blood loss, have significant reductions in post-operative SNOT-22 and NOSE scores, and have fewer minor complications than the younger cohort. These findings are in spite of a higher rate of overall pre-operative comorbidities such as hypertension and increased use of anticoagulants. The reduced overall reduced operative time (117.4 minutes versus 183.4 minutes, p = 0.004) did not impact improvements in overall post-operative SNOT-22 and NOSE scores and did not appear to increase adverse outcomes. Operative time is a useful quality metric for patient outcomes and in the Neurosurgical literature, prolonged operative time is associated with increased risk for thromboembolic events, urinary tract infections, and the need for prolonged intubation. 7 Mitigating prolonged operative time is therefore an especially important finding. Reh et al. observed no difference in pre-operative symptoms, endoscopy, or imaging (CT) characteristics in elderly versus younger patients. 8 Furthermore, volumetric analyses suggest larger nasal volume in elderly patients. 9 Taken together, for the same disease process there may very well be improved intranasal maneuverability and ease of surgery. Moreover, it is reasonable to speculate that the operating surgeon may seek to expedite the operative case and perform more conservative surgery in the setting of the aged patient with more medical comorbidities.
The higher rate of post-operative steroids in the elderly cannot be readily explained. Ad-hoc analysis illustrated that this prescription pattern was not due to higher rates of polyposis. The overall rate of geriatric patients with polyps was comparable to the rates among non-geriatric patients (44.8% versus 50%). The similar number of polyps between the two groups implies that the presence of polyps alone does not explain the higher rate of post-operative steroid use in geriatric patients.
Elderly patients had a lower mean blood loss (78.4 milliliters versus 106.9 milliliters, p = 0.04) than their younger peers. A reduction in blood flow to the nasal mucosa with advanced age has been noted in the literature. 10 Furthermore, with advanced age the nasal epithelium and submucosa have reduced levels of pro-inflammatory cytokines, chemokines and other downstream factors. 11 Reduced small vessel blood flow has been observed in the elderly and is a source of inferior nasal heating and humidification. This reduction in the pro-inflammatory milieu and reduced microvasculature may contribute to the reduced blood loss illustrated in our study. 12 Prior to our study, the authors speculated that polypharmacy might contribute to a higher rate of intraoperative bleeding in the elderly. Despite a fifth of elderly patients taking anticoagulants preoperatively, at our center the majority stop their anticoagulants within a pre-appointed and medication-specific time prior to surgery, and thus the influence of the anticoagulant is likely reduced. While not specifically collated, elderly male patients have a higher incidence of benign prostatic hypertrophy, and are more frequently on alpha reception blockers (e.g. doxazosin and terazosin). While such medications lower mean arterial blood pressure, they are also associated with higher bleeding and coagulation times and have been demonstrated to reduce platelet aggregation. 12 Despite this, high blood loss was not noted among the geriatric cohort in our study.
Despite the relative dearth of literature pertaining to GESS, several authors have noted better subjective outcomes in elderly patients than their younger, disease-matched peers.5,13 Colclasure et al. demonstrated reduction in mean post-operative symptom scores, noting improvements in the three-, six-, and 12-month SNOT-20 scores. Indeed, post-operative patients experienced 64% improvement of symptom scores by three months, 73% improvement by six months, and 75% improvement by 12 months with concurrent improvements in nasal endoscopy. 14 Lee et al. observed no statistical differences in polyp extent or Lund-Mackay score between adult, pediatric and geriatric age groups. 13 The objective surgical outcome based on the endoscopic findings was worst in the pediatric group (45%), whereas the geriatric group showed the best results (90%). The authors concluded that FESS provides subjective and objective improvements in sinusitis symptoms in pediatric and geriatric populations alike. The authors noted that geriatric patient have excellent outcomes; even patients with massive polyposis showing excellent healing postoperatively. Marioni et al. demonstrated that compared to younger patients, histologically eosinophilic CRSwNP or high blood eosinophil counts were not significantly associated with a higher recurrence rate in geriatric patients.
Several studies demonstrate geriatric FESS to be safe and effective, with few minor complications including intranasal crusting, lateralized middle turbinate, epistaxis, and no major complications.5,14 This finding is supported by our data. Indeed, minor complications were more likely to occur in the non-geriatric patients (7.5% versus 41.7%, p = 0.0001). No episodes of postoperative epistaxis, orbital complications, or cerebrospinal fluid (CSF) leaks occurred in either group. Several studies showed a higher overall complications rate in elderly patients. Jiang and Hsu observed that complications in GESS were significantly higher at a rate of 15.2% compared with 9.5% in adult FESS and 4.1% in PESS. 2 Ramadan and VanMetre also observed a higher complication rate in elderly patients requiring revision FESS (21.7% for the elderly compared with 12.8% for the younger group), but noted an overall lower need for revision FESS in this age group. 15 Indeed, the older group had a 24% revision rate compared with 34% in the younger group. These findings are in contrast to Vleming et al al. who showed that complications following FESS were independent of patient age. 16 Terris and Davidson also reviewed complications in all patients undergoing FESS, noting that 63% experienced very good results, 28% experienced good results, and 9% had poor results. 17 They reported CSF leaks in 0.6% of patients, postoperative epistaxis in 1.5% of patients, and minor complications in 2% of patients. Our data, compared with similar studies shows that sinus surgery in the elderly is safe, timely, and leads to less blood loss then younger patients with similar improvements in quality-of-life metrics.
There are several limitations of our study, including its retrospective nature. Our data contains data of the ASA class for our geriatric cohort, but unfortunately this is not available for the comparison group and was excluded from data analysis. Additionally, our data did not parse revision versus non-revision patients during the data analysis. Only subjective FESS results were included in this paper, there was no data concerning objective and surgeon identified surgical success available. While this is indeed a deficiency, including primary with revision patients together may also strengthen our data as it does not allow for selection of primary cases and instead takes “all comers”. Nonetheless, geriatric patients are less likely to undergo revision surgery, with 9.9% of geriatric patients undergoing revision FESS compared to 11.7% and 13.2% in adult and pediatric populations respectively. 3 Hence it is feasible that the higher rates of revision in adult patients may skew the operative time and blood loss but we feel that such an influence is likely to be negligible.
Conclusion
There are clear risk factors for surgery in the elderly that must be weighed. Nonetheless our data shows marked improvements in quality-of-life parameters combined with reduced operative times and blood loss. Similar to many studies in the existing literature, our data demonstrates minimal minor post-operative complications, and no intraoperative or major complications, suggesting that GESS is a safe and effective procedure.
Footnotes
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.
Authors’ Note
This work was presented as a poster at the Triological Society 121st Annual Meeting—COSM 2018, April 2018, National Harbor, MD.
Ethical Approval
De-identified patient information was parsed from the Mount Sinai Hospital, Beth Israel Mount Sinai Medical Center, and New York Eye and Ear Infirmary of Mount Sinai medical records by HIPAA-certified researchers. Permission from the Mount Sinai institutional review board was obtained for this retrospective review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.