
Abstract
Background
Although the close relationship between the upper and lower airways has been highlighted previously, little is known about the association between lung function and the recurrence of chronic rhinosinusitis with nasal polyps (CRSwNP). This study aimed to evaluate the factors associated with pulmonary function that affect CRSwNP recurrence after surgery.
Methods
We performed a series of routine pulmonary function tests for general anesthesia prior to CRSwNP surgery. The values for each parameter were compared in the presence or absence of recurrence.
Results
Sixty-nine patients with CRSwNP were included. The percent predicted forced expiratory volume in one second (%FEV1) in the recurrent group was significantly lower than that in the non-recurrent group (P = .005). A multivariable logistic regression model revealed that %FEV1 was a positive predictor of recurrence (odds ratio: 0.96, 95% CI: 0.92-0.99, P = .023). There were no significant differences in the other pulmonary functions between the two groups.
Conclusions
We found that %FEV1 may be a predictor of CRSwNP recurrence after surgery. As %FEV1 is a pulmonary function test that is routinely performed before surgery, this parameter is readily applicable. Moreover, as %FEV1 appears to have the potential to reveal concealed asthma, %FEV1 might be a particularly useful tool for the prediction of CRSwNP recurrence after surgery.
Keywords
Introduction
Chronic rhinosinusitis (CRS) is one of the most common chronic diseases globally, 1 affecting 4.5 to 12% of the American and European populations. 2 CRS is characterized by a range of symptoms including nasal blockage, nasal discharge, facial pain and reduction in the sense of smell, and is confirmed by endoscopy and/or computed tomography (CT). 3 It has been divided into two subgroups: CRS with nasal polyps (CRSwNP) and CRS without nasal polyps (CRSsNP). 3
As the nose and lung are localized in the common airway and share common histological structures such as the ciliary epithelium, basement membrane, lamina propria and glands, a close relationship between CRS and asthma has been reported. For instance, the presence of CRS is one of the risk factors for the development of asthma, and patients with asthma have a high prevalence of CRS. 4 These associations can be explained by the “united airway” hypothesis. 5
Functional endoscopic sinus surgery (FESS) is an effective form of intervention for most CRS patients who do not respond to conservative treatment and has been shown to improve quality of life. 6 However, some patients experience recurrence after FESS and require revision surgery. 17 One explanation for this is that CRS can be regarded as a syndrome that includes many different disease phenotypes and endotypes. 8 Numerous studies were performed to elucidate the predictive factors for recurrent CRS after FESS. Nasal polyps, peripheral blood and tissue eosinophilia, comorbidity of bronchial asthma, degree of the sinus shadows on CT scans, female gender and Hispanic ethnicity are all thought to be potential predictive factors for recurrence. 19 Although the close relationship between the upper and lower airways has been highlighted previously, little is known about the association between pulmonary function and CRS recurrence.
In this study, we aimed to clarify the factors associated with pulmonary functions that affect the rate of recurrence in patients with CRS after FESS.
Patients and Methods
Patients
We retrospectively examined patients diagnosed with CRSwNP who underwent FESS at the Department of Otolaryngology, Hokkaido University between June 2007 and December 2016. The diagnosis of CRSwNP was based on patient history, clinical examination, nasal endoscopy and CT, in accordance with the European Position Paper on Rhinosinusitis and Nasal Polyps 2012. 3 All patients received conservative treatment, such as topical steroids and saline irrigation, for at least 3 months before surgery. Patients in whom symptoms remained unresolved after conservative treatment were treated with FESS. All patients underwent ethmoidectomy and maxillectomy. Additionally, frontal sinusotomy or sphenoidotomy was performed if mucosal thickening was observed in the frontal or sphenoid sinus. Our study excluded patients treated with systemic corticosteroids before surgery, patients who were followed up for less than 6 months after surgery and patients diagnosed with chronic obstructive pulmonary disease (COPD).
All patients had to be cleared for treatment, and written informed consent was obtained from all patients after a full explanation of the potential risks and benefits. This study was approved by the Institutional Review Board of the Hokkaido University Hospital for Clinical Research (No.017-0151).
Methods
All patients underwent a thorough history-taking and physical examination. Blood samples were taken for the measurement of a full blood count and blood biochemistry, radioimmunosorbent testing (RIST) for total IgE and capsulated hydrophilic carrier polymer radioallergosorbent testing (CAP-RAST: ImmunoCAP™ specific allergens Thermo Fisher Scientific, MA, USA) for 13 types of antigen-specific IgE. Pulmonary function testing and CT were performed before surgery. CT findings were scored according to the Lund-MacKay scoring system (LMS). 10 The degree of nasal polyps was evaluated using the endoscopic polyp scoring system1112 as follows. 0; no visible polyps 1; small polyps within the middle meatus, 2; polyps extending beyond the middle meatus, and 3; polyps completely obstructing the nasal cavity. Atopy was defined as a positive result on the CAP-RAST for at least one antigen-specific IgE. Exhaled nitric oxide (FeNO) concentrations were measured with a NIOX MINO® monitor (Aerocrine, Stockholm, Sweden) using a single-breath online method, according to the American Thoracic Society guidelines. 13 All patients diagnosed with asthma were evaluated by a pulmonologist based on the Japanese Guidelines for Adult Asthma. 14 Further, all patients diagnosed with asthma were evaluated by spirometry. Recurrence of CRS was defined as the presence of nasal polyps (grade 2 or more) on nasal endoscopy.
Pulmonary Function Testing
Pulmonary function testing was performed prior to FESS. Chestac (Chest MI Inc., Tokyo, Japan) was used for spirometric measurements. Maintenance and calibration were performed in accordance with the guidelines for pulmonary function tests of the Japanese Respiratory Society (JRS). 15 Predicted values for the spirometric measurements were also derived from the guidelines for pulmonary function tests issued by the JRS. 15 The following parameters were measured: percent predicted vital capacity (%VC), forced expiratory volume in one second (FEV1), percent predicted forced expiratory volume in one second (%FEV1), forced expiratory volume in one second/vital capacity (FEV1/VC), maximum expiratory flow rate at 50 percent of vital capacity (V50), maximum expiratory flow rate at 25 percent of vital capacity (V25), and maximum expiratory flow rate at 50 percent of vital capacity/maximum expiratory flow rate at 25 percent of vital capacity (V50/V25).
Histopathological Analysis
Tissue samples from nasal polyps or polypoid lesions from the ethmoid sinus were taken during surgery and fixed in 10% formalin. These samples were embedded in paraffin and stained with hematoxylin-eosin. The number of eosinophils per high-power field (HPF; x400) was counted in the three densest areas and the mean number of eosinophils was calculated.
Follow-up
After the completion of FESS, subsequent clinical visits were scheduled every 1 to 3 months for the first year, every 3 to 6 months for the second year, and every 6 months thereafter. Endoscopic examinations were carried out at each visit. Patients were treated with a nasal rinse twice a day and a topical steroid (Fluticasone Furoate 110 µg/day) after surgery.
Statistical Analysis
Statistical analysis was performed using the program R version 3.4.1 (R Foundation for Statistical Computing, Vienna, Austria). Values are presented as means ± SD. Mann-Whitney U test was used for intergroup comparisons. Differences in proportions were examined using the Chi-square test or Fisher’s exact test. Spearman's rank correlation coefficient was used for investigating correlation between two variables. A multivariate logistic regression was performed for assessing the predictors of recurrence. A value of P < .05 was considered to be statistically significant.
Results
Patient Characteristics
Sixty-nine patients with CRSwNP who underwent FESS in our hospital during the study period were included. The profiles of the patients are shown in Table 1. Patients consisted of thirty-four male patients and thirty-five female patients, with a mean age of 55.3 ± 13.3 years (range 17 to 78 years). The median follow-up period was 62 months (range 9 to 114 months). Thirty-six (52.2%) patients had bronchial asthma, with 16 of those asthma patients showing aspirin intolerance (aspirin-exacerbated respiratory disease: AERD) and 20 showing aspirin-tolerant asthma (ATA). Atopy was observed in 77.8% of patients and the most elevated antigen was mite antigen (67.8%), followed by house dust (64.5%) and birch pollen (25.8%). The percentage of patients who underwent ethmoidectomy, maxillectomy, frontal sinusotomy and sphenoidotomy were 100%, 100%, 72.5% and 79.7%, respectively. The type of frontal sinusotomy; i.e., Draf 1, 2a, 2 b, and 3, were 2%, 98%, 0%, and 0%, respectively.
Clinical Characteristics of Patients.

Abbreviations: AERD: Aspirin-exacerbated respiratory disease, ATA: aspirin-tolerant asthma; LMS: Lund-MacKay scoring system.
Pulmonary Function and Recurrence of CRS
Pulmonary function data for CRS patients with and without recurrence are shown in Figure 1. The %FEV1 values in the recurrent group were significantly lower than those in the non-recurrent group (P = .005); however, there were no significant differences in %VC, FEV1, FEV1/VC, V50, V25 or V50/V25 between the two groups.
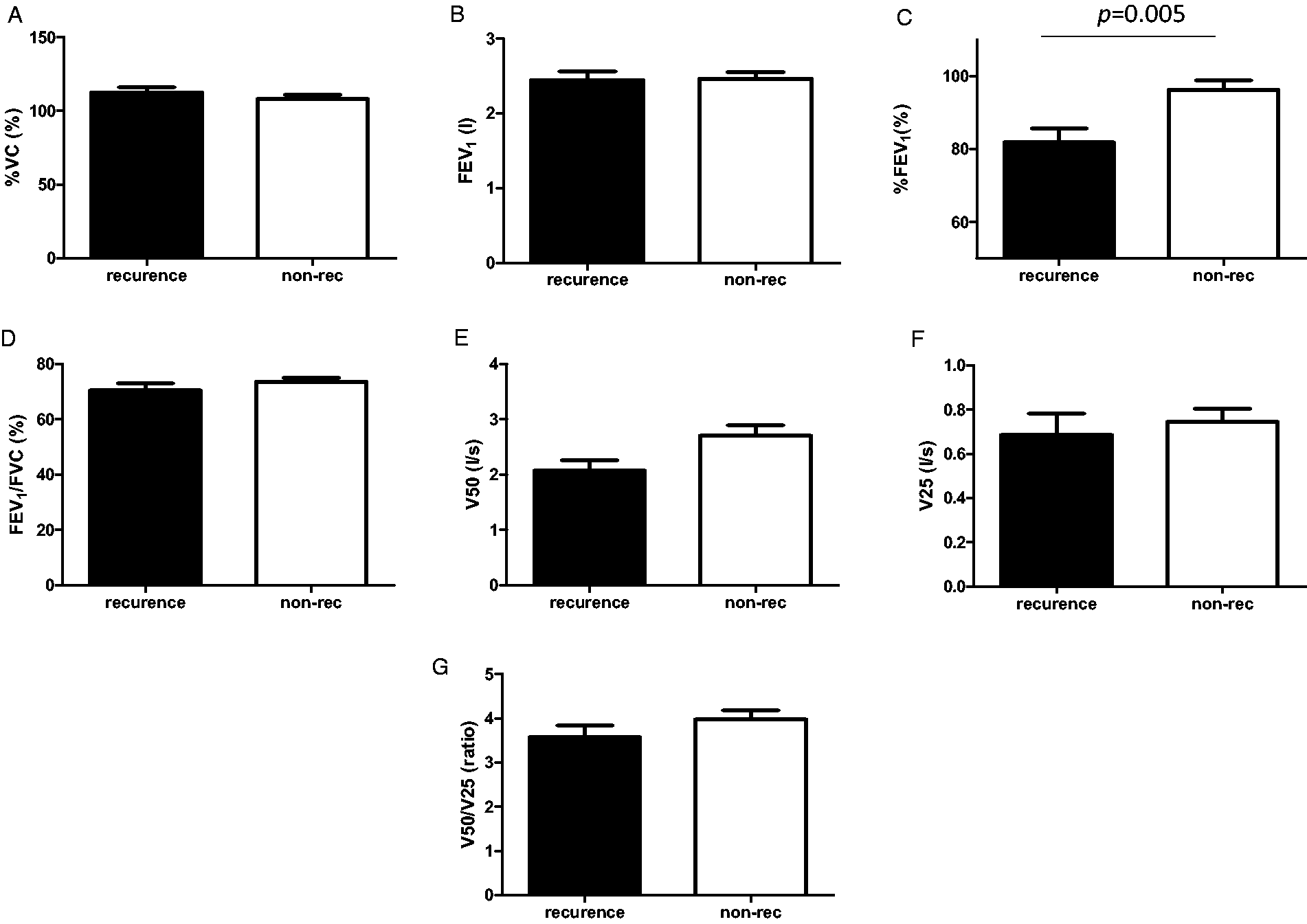
Pulmonary function in CRS patients with and without recurrence. The %FEV1 value in the recurrent group was significantly lower than that in the non-recurrent group. There were no significant differences in %VC, FEV1, FEV1/VC, V50, V25 or V50/V25 between the two groups. A, Percent predicted vital capacity (%VC). B, Forced expiratory volume in one second (FEV1). C, Percent predicted forced expiratory volume in one second (%FEV1). D, Forced expiratory volume in one second/vital capacity (FEV1/VC). E, Maximum expiratory flow rate at 50 percent of vital capacity (V50). F, Maximum expiratory flow rate at 25 percent of vital capacity (V25). G, Maximum expiratory flow rate at 50 percent of vital capacity/maximum expiratory flow rate at 25 percent of vital capacity (V50/V25).
Factors Other than Pulmonary Function Associated with Recurrence
We found that 23 patients (33.3%) had recurring nasal polyps. Factors significantly associated with the recurrence of the disease were comorbidity of asthma (P < .001), the degree of LMS (P < .001), polyp score (P < .001) and tissue (P = .009) and peripheral blood eosinophil counts (P < .001). Asthma (especially AERD) was more frequently observed in the recurrent cases than in the non-recurrent cases. There were no differences between the recurrent and non-recurrent groups in terms of gender, age, atopy, total IgE and FeNO (Table 1).
Multivariable Logistic Regression Showing Predictors of Recurrence
Among the six factors (%FEV1, comorbidity of asthma, the degree of LMS, polyp score and tissue and peripheral blood eosinophil counts) significantly associated with recurrence, the degree of LMS vs. polyp score (r = 0.698, P < .001by Spearman's rank correlation coefficient), tissue eosinophil vs. peripheral blood eosinophil counts (r = 0.378, P = .003 by Spearman's rank correlation coefficient)and % FEV1 vs. comorbidity of asthma (P < .015 by Mann–Whitney U test) were closely associated with each other. We, therefore, used a multivariable logistic regression model with three factors (%FEV1, polyp score and tissue eosinophil count) (Table 2). In the multivariable logistic regression model, all three factors remained positive predictors for recurrence; % FEV1 (odds ratio: 0.96, 95% CI: 0.92–0.99, P = .023), polyp score (odds ratio: 1.90, 95% CI: 1.18–3.06, P = .008), tissue eosinophil count (odds ratio: 1.00, 95% CI: 1.00–1.01, P = .024). The P value of the likelihood ratio test was <0.001. P values of the coefficients for %FEV1, polyp score and tissue eosinophil count were 0.018, 0.008 and 0.028, respectively. The variance inflation factor (VIF) for %FEV1, polyp score and tissue eosinophil count were 1.110, 1.057 and 1.116, respectively. The Area Under the Curve of the ROC curve was 0.845 (95%CI 0.747–0.942).
Multivariable Logistic Regression Showing Predictors of Recurrence.

Discussion
In this study, we found that %FEV1 was negatively correlated with the recurrence of CRSwNP, not only by univariate analysis but also by multivariable analysis. The %FEV1 value before surgery may, therefore, be a predictor for CRSwNP recurrence after FESS.
Forced expiratory volume (FEV) measures how much air a person can exhale during the first second of a forced breath. %FEV1is the ratio between the measured value and the predicted value for a person of similar age, gender, body size, and ethnicity, who does not have lung disease. As %FEV1 represents the degree of obstructive ventilatory impairment, this parameter is used for grading obstructive lung diseases such as asthma 16 and COPD. 17 In patients with CRSwNP, the %FEV1 value was significantly lower than that in patients with CRSsNP as well as in healthy controls.1819 Moreover, it was negatively correlated with peripheral blood eosinophil count, duration of CRS 19 and CT score. 18
There have been several mechanisms proposed for this association between the upper and lower airways. These hypotheses include 1) a systemic reaction, 2) a naso-bronchial and pharyngo-bronchial reflex, 3) stimulation of the lower airway by inflammatory secretion in the upper airway, and 4) inhalation of dry, cold air and pollen. 18 Among these explanations, the systemic reaction appears to well account for the relationship between the %FEV1 value and CRS recurrence after surgery. The upper and lower airways have the same mucosal susceptibility to exogenous irritants, and they can be affected and responses amplified through common systemic inflammatory mediators. 20 When allergic inflammation occurs at one site in the airway mucosa, inflammatory mediators, cells and cytokines enter the blood, resulting in inflammation of other sites in the airway mucosa. 20
There are several lines of evidence supporting this hypothesis related to a systemic reaction. For instance, after a nasal challenge with allergens, the lower airway responsiveness in patients with allergic rhinitis without asthma was increased and total eosinophils and eosinophils expressing eosinophil-cationic protein were increased in the induced sputum. 21 On the other hand, segmental bronchial provocation induces nasal inflammation in allergic rhinitis patients. 22 Inflammation in the lower airway might have a negative influence on the upper airway through the production of inflammatory mediators. From the perspective of crosstalk between the upper and lower airway, % FEV1 might reflect the mucosal susceptibility to irritants not only in the lower airway but also in the upper airway. This appears to provide a reasonable explanation for % FEV1 being a predictor of CRS recurrence after surgery.
FEV1/FVC is the other parameter used to evaluate obstructive lung impairments. In the GOLD guidelines, patients are qualitatively diagnosed with COPD by use of FEV1/FVC < 70%. After the diagnosis of COPD, patients are quantitatively divided into 4 stages by the use of %FEV1. 23 This means that FEV1/FVC (especially <70%) can qualitatively express the existence of obstructive ventilatory impairment, but this parameter cannot assess impairment in quantitative terms. These differences between %FEV1and FEV1/FVC might have influenced the results showing that % FEV1, but not FEV1/FVC, is associated with CRSwNP recurrence.
It was reported that several factors are associated with CRS recurrence. For example, the existence of nasal polyps is commonly used for predicting recurrence due to the fact that the classification system for CRS uses the presence/absence of nasal polyps; i.e., CRSwNP and CRSsNP. CRSwNP is characterized by Th2-skewed eosinophilic inflammation and is more prone to recurrence than CRSsNP, which shows predominantly Th1-type inflammation.124 Based on this information, we focused on patients with CRSwNP. However, different phenotypes exist even within CRSwNP. Some patients with CRSwNP showed excellent results after FESS, while patients with other types of CRSwNP are more prone to recurrence. 1 Tomassen et al. reported the endotyping of CRS 8 in which they performed cluster analysis of CRS with the use of biomarkers such as IL-5, IFN-γ, IL-17A and TNF-α. The clusters were divided into 3 based on IL-5 positivity (negative, moderately positive and highly positive). The highly positive IL-5 cluster was closely linked to prevalence of nasal polyps and asthma. This report suggested that there are different phenotypes in CRS. Apart from nasal polyps, eosinophilia, comorbidity of asthma, degree of sinus shadow, gender and ethnicity have all been reported as predictive factors. 19 In agreement with previous results, comorbidity of asthma, the degree of sinus shadow, polyp score and tissue and peripheral blood eosinophil counts were all found to be significantly associated with recurrence in this study.
Among these factors, comorbidity of asthma was associated with % FEV1.
As patients with CRSwNP without asthma were reported to have lower % FEV1 values than control subjects, 18 there might be a certain percentage of patients who actually suffer from asthma without any diagnosis. %FEV1 is a commonly used pulmonary function examination prior to general anesthesia and is useful for revealing concealed asthma. Therefore, the measurement of %FEV1 prior to FESS appears to be a simple and useful method for predicting CRSwNP recurrence after surgery.
There were limitations to this study in that the number of patients enrolled in this study was relatively small and it was performed as a retrospective study. A larger prospective study should be performed to confirm whether %FEV1 can truly predict CRSwNP recurrence after surgery.
Conclusion
In this study, we found that %FEV1 may be a predictor of CRSwNP recurrence after FESS. Although %FEV1 is associated with comorbidity of asthma, %FEV1 reflects the status regarding lower airway impairment more precisely than does the presence of asthma. There are some patients who have impaired lung function but are not clinically diagnosed with asthma. For this reason, % FEV1 might be useful tool for predicting CRSwNP recurrence after surgery as with previously mentioned factors such as asthma comorbidity, eosinophilia, and high LMS.
Footnotes
Ethical Approval
This study was approved by our institutional review board (No. 017-0151).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
All patients had to be cleared for treatment, and written informed consent was obtained from all patients after a full explanation of the potential risks and benefits.