
Abstract
Background
With the increasing elderly population and prevalence of osteoporosis, geriatric intertrochanteric fragility fractures pose a major challenge to orthopedic practice. These fractures have a significant impact on patient outcomes, with a reported mortality rate of 13.3% within 30 days and 24.5% within one year.
Case Presentation
This report presents a rare case of delayed iatrogenic deep femoral artery (DFA) injury due to progressive displacement of the lesser trochanter following intertrochanteric fracture fixation. An 87-year-old female patient developed significant thigh swelling and pain 33 days postoperatively. Imaging confirmed migration of the lesser trochanter fragment, leading to DFA injury and active bleeding.
Discussion
Through a comprehensive literature review, we explore the incidence, diagnostic modalities, and management of vascular injuries associated with pertrochanteric fracture fixation. We emphasize the importance of identifying significantly displaced lesser trochanter fragments (>1 cm) preoperatively, as they markedly increase the risk of DFA injury. While debate continues over routine fragment fixation, our case suggests that surgical fixation may be beneficial in selected patients with large displacements to prevent vascular complications. Early CT angiography is highlighted as a crucial non-invasive diagnostic tool for timely detection and intervention in these high-risk cases.
Conclusion
This case underscores the need for careful postoperative monitoring and early intervention to optimize patient outcomes. As PFFs become more prevalent, further research is essential to improve geriatric orthopedic care.
Keywords
Introduction
Geriatric intertrochanteric fragility fractures are becoming increasingly common in developed regions due to the aging population and the increasing incidence of osteoporosis and sarcopenia.1,2 These fractures pose a major challenge as the mortality rate is 13.3% after 30 days and 24.5% within the first year, and more than a third of patients do not regain their preoperative level of function and independence. 3 Surgeons often use intramedullary (IM) nailing because of its minimally invasive nature and shorter operation times, although its biomechanical superiority over older implants such as the Dynamic Hip Screw (DHS) has not been proven. 4 Anatomically, the DFA (profunda femoris) branches posterolaterally from the common femoral artery and courses within 1-2 cm of the lesser trochanter, placing it at risk of injury from displaced bone fragments. Comparative studies by Gokmen et al, 5 on cementless bipolar hemiarthroplasty, and by Varmış et al 6 on proximal femoral nail antirotation (PFN-A) vs INTERTAN nail fixation, provide relevant data on implant selection in intertrochanteric fractures. However, IM nailing is not without complications. Femoral artery injuries occur in approximately 0.49% of cases. 7
Vascular complications following hip fractures, including vascular injury, hemorrhage, and arterial thromboembolism, are predominantly iatrogenic and due to factors, such as fracture reduction, implant placement, and postoperative fragment migration. 7 Migration of the lesser trochanter fragment, facilitated by traction of the iliopsoas muscle during physiotherapy, is a common cause of DFA injury. In this study, we present a case of delayed iatrogenic DFA injury due to progressive displacement of the lesser trochanter during physical therapy that occurred 33 days after surgery. We also conducted a literature review to investigate the incidence of such cases and to evaluate the clinical presentations, diagnostic methods, and treatment modalities. In addition to presenting a rare case, this study offers an updated synthesis of current diagnostic approaches and treatment strategies, aiming to improve clinical awareness and outcomes for patients with similar vascular complications.
Case Report
An 87-year-old female patient was admitted to our emergency department with hip pain after a ground level fall on her left hip. On clinical examination, she was unable to walk on her left leg, which appeared shortened and externally rotated. Any manipulation of her left leg resulted in worsening groin pain. There was no neurovascular deficit. The patient’s medical history only indicated elevated blood pressure, which was controlled with medication. The patient did not report any anticoagulant medication or allergies.
She underwent radiographic evaluation, including an anteroposterior (AP) pelvic radiograph and a left hip radiograph, which revealed a multifragmentary intertrochanteric femoral fracture classified as 31 A2 according to Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association (AO/OTA 31A2) (Figure 1). Lesser trochanter displacement was 27 mm, defined as the mean distance between the highest and lowest points of the fragment and the fracture site. AP radiograph of the hip and pelvis on admission to the emergency department.
Initial laboratory tests revealed a hematocrit value of 0.319 and a hemoglobin value of 106 g/L. The other laboratory values were within normal limits. After consultation with the anesthesiologist on duty, she underwent closed internal IM fracture fixation on the same day (Figure 2). Postoperatively lesser trochanter fragment displacement was 9 mm. Intraoperative C-arm radiographs of the left hip show good reduction of the fracture in both planes. The lesser trochanter is displaced.
During the postoperative period, the hematocrit decreased to 0.270, and no blood transfusion was required during her first hospitalization. Physical therapy was started on the second postoperative day. This included gait training with a walker, learning to stand and transfer activities, coordination and balance training, muscle strengthening exercises, endurance exercises, breathing training, and thrombosis prevention exercises, all of which were performed under the guidance of a trained physical therapist 2-3 times daily during the hospital stay. The rehabilitation program continued after the patient was discharged with the same exercises being performed 5 times a week for 3 weeks. The patient was discharged 7 days after surgery (our average hospital stays after this type of surgery) with parenteral anticoagulation therapy, enoxaparin sodium. On the day of discharge, her pain in the operated leg was minimal at rest and when walking. A rehabilitation program was started at home 2 weeks after the surgery. Physical therapy was uneventful until day 33 after the first surgery, when she experienced severe pain in the groin during hip flexion, followed by significant swelling of the left thigh.
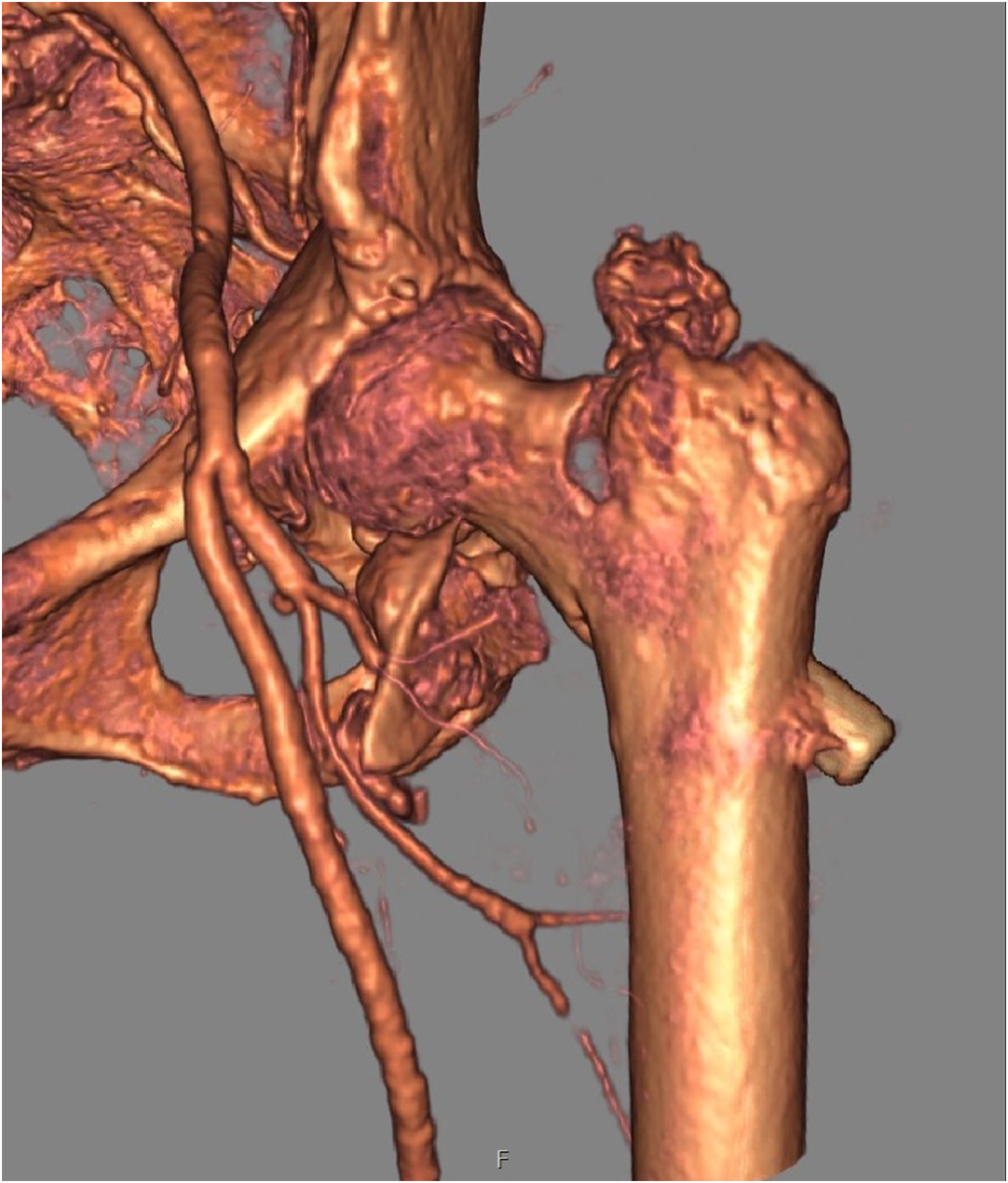
She underwent a physical examination in our emergency room, where she was again found to have a swollen and painful left thigh. The pain increased with hip flexion. An accentuated pulse of the common femoral artery was found with normal distal blood flow to the left leg. A radiograph of the hip (Figure 3) and Computed Tomography (CT) angiography (Figures 4 and 5) of the iliac and left femoral vessels showed proximal migration of the lesser trochanter, coming into contact with a branch of the profunda femoris artery, resulting in laceration of the vessel wall and active bleeding. The exact location of the vascular injury was 5.5 cm caudal to the origin of the left DFA, with a femoral hematoma measuring 16 x 4 x 6 cm. At this point, the displacement of the lesser trochanter was measured at 52.5 mm. AP radiograph of pelvis on second admission to the emergency department. CT angiography 3D image shows DFA injury caused by sharp edge of displaced lesser trochanter. The greater trochanter was also displaced by the traction of the abductor muscle. 3D CT image shows an unchanged position of the proximal femoral implant, the relationship to the lesser trochanter and the injured DFA.

After consultation with the vascular surgeon on duty, the patient was emergently transported to the operating room. The femoral triangle was explored, and the hematoma was removed along with the ligation of the damaged artery (Figure 6). Figure 6 shows a detailed intraoperative image demonstrating the sharp-edged fragment of the lesser trochanter (LTF) in direct contact with the wall of the DFA, resulting in vascular injury. The spike of the lesser trochanter, which was in contact with the ruptured vessel wall, was resected. Intraoperative image showing the sharp-edged fragment of the lesser trochanter (LTF) in contact with the wall of the deep femoral artery (DFA). The image also shows the superficial femoral artery (SFA), the resected bone fragment and the area where the hematoma has been evacuated.
Postoperatively, the pain was gone the next day. The patient received three units of packed red blood cells during her second hospital stay. She was discharged 5 days after the second surgery with no persistent morbidity. The patient recovered well and physiotherapy was continued after the wound had healed and the thigh swelling had completely subsided. At the follow up examination 2 months after the second operation, the fracture had healed, and she was able to walk with a walking aid without pain. At the final follow up examination, after completion of physiotherapy, she had regained her preinjury hip function and was able to walk with two crutches without pain.
Literature Review
A comprehensive literature search was conducted in PubMed, Science Direct, Cochrane Library and Embase Ovid. Medical keywords included PFFs, femoral artery, hemorrhage, fracture fixation, and lesser trochanter. Articles with English abstracts reporting surgically treated intertrochanteric fractures with femoral artery injury and resulting in laceration and hemorrhage or pseudoaneurysm formation due to a trapped bone fragment of the lesser trochanter were included in the analysis. We initially identified 45 articles through March 2015 that were summarized in Barquet’s review and provided a broad overview of cases of femoral artery injury from the lesser trochanter during fixation of proximal femoral fractures. According to this review, the lesser trochanter was identified as the cause in 25.7% of vascular injuries associated with internal fixation of proximal femoral fractures. Most patients in these cases were diagnosed with pseudoaneurysm formation, followed by rupture and hemorrhage. The earliest documented case was reported in 1965 by Aufranc et al. 8
Characteristics of Fragment Displacement
Cases of Femoral Artery Injury due to a Migrated Fragment of the Lesser Trochanter After Intertrochanteric Fracture Fixation, March 2015-2023, by Case.

These more recent cases specifically describe femoral artery injuries directly caused by migrated fragments of the lesser trochanter after intertrochanteric fracture fixation, regardless of the fixation method used. The choice of fixation method, whether with intramedullary nails or hemiarthroplasty, may influence not only mechanical outcomes but also the pattern and risk of fragment migration, as suggested by recent comparative clinical studies.5,6 Including our own case, this brings the total number of reported cases to 60.
Summary of Reported Cases
Summary of Reported Cases of Vascular Injury due to Lesser Trochanter Fragment Displacement (2015-2023).

The most commonly reported vascular lesion was a pseudoaneurysm of the DFA, documented in 7 out of 14 cases, while direct lacerations or active bleeding from DFA branches occurred in the remaining cases. The time to symptom onset varied considerably, ranging from 2 days to 6 months postoperatively, with the majority of complications emerging within the first three weeks after surgery. Common clinical manifestations included thigh swelling, pain, hypotension, tachycardia, and anemia, often requiring urgent intervention. Treatment strategies primarily involved endovascular approaches, such as coil embolization (7 cases), followed by open surgical techniques including arterial ligation with or without removal of the bone fragment (5 cases), and in some instances, stent implantation or vein patch repair (2 cases). This comparative overview emphasizes the importance of recognizing early clinical signs and tailoring diagnostic and therapeutic approaches to the type of lesion and timing of symptom onset.
Comparison with Current Case
Including our own case, we identified 14 other cases between March 2015 and 2023 in which a vascular injury was directly attributed to lesser trochanter fragment displacement. These cases emphasize the importance of close postoperative monitoring, especially in patients with significant fragment displacement. For example, the direction and proximity of displacement to the DFA were key factors in the reported injuries. Proximal displacement toward the femoral artery, often aggravated by physical therapy, resulted in delayed vascular injuries, as in our case. The literature supports the view that a careful evaluation of the displacement characteristics should determine the follow up strategy. 9 In patients with larger and more proximal displacements, early diagnostic imaging, such as CT angiography, should be considered to preemptively identify and treat potential vascular complications.
The inclusion of fragment displacement characteristics in the literature review has improved the understanding of risk factors for vascular injury following fixation of intertrochanteric fractures. This expanded analysis supports the need to individualize patient care based on the size, direction, and length of displacement of the lesser trochanter fragment, with a lower threshold for imaging and intervention in high-risk cases.
Discussion
Incidence and Types of Vascular Injuries
Vascular injuries associated with PFF fixation are potentially limb- and life-threatening. Fortunately, their overall incidence is low, at 0.49% according to the 2015 review by Barquet et al. 7
Extrapelvic vessels are most commonly affected (91.20%), as opposed to intrapelvic vessels (8.24%). A single case of combined injury affecting both intra- and extrapelvic vessels was recorded. In the group of intrapelvic vessels, the external iliac vessels (EI) had the highest incidence, followed by the internal iliac vessels and their branches. In the extrapelvic vessels group, there was a notable prevalence of injury to the DFA and its branches (78.31%), accompanied by fewer cases of injury to the superficial femoral vessels (10.84%). A minority of cases involved the other femoral arteries. 7
According to the literature, vascular injuries in IM fixation of PFFs are even rarer, occurring in 0.2% of trochanteric fractures. In most cases, the injured artery is a branch of a DFA. 25
Etiology of Vascular Injuries
The etiology of vascular injuries associated with IM nailing can be divided into iatrogenic and non-iatrogenic causes. Iatrogenic causes are significantly more common (96.15%) and often result from the reduction process, careless insertion of retractors or in-instruments, or implant related factors such as over drilling or screw penetratio. 7 Non-iatrogenic causes are less common and typically involve displaced bone fragments, eg, from the lesser trochanter, either in non-operatively treated patients or prior to surgical fixation. 7
The frequent involvement of the DFA in these injuries is related to its anatomical location. As a branch of the femoral artery, it runs deep in the medial thigh, close to the posteromedial surface of the thigh. The configuration of the arterial supply around the femoral neck combined with the relatively fixed DFA and muscle septa attached to the medial cortex of the thigh may contribute to arterial wall injury in this area.7,10,26,27
Studies have quantified the proximity of the DFA to the femur, with the smallest mean distance being 12.8 ± 2.38 mm at the distal insertion site of the screw in IM nail-ing. 10 The reduction process for a PFF, which involves traction, adduction and internal rotation, may compress the femoral arteries between the bone and the surgical instruments. This increases their susceptibility to injury from fracture fragments or instrument penetration.7,10,28,29 Minimizing traction and adduction may reduce this risk, as can choosing a neutral limb position during screw insertion.30,31
Elderly patients with atherosclerotic and fragile arteries are especially susceptible to such injuries.7,32
Patient Monitoring and Aftercare
Certain patients require more careful follow-up care due to higher risk factors: 1. Elderly patients: Patients over 65, especially with concomitant vascular disease such as atherosclerosis, should be monitored closely.7,32 2. Displaced fragments: A significant displacement (>1 cm) of the lesser trochanter increases the risk of vascular injury and requires close postoperative monitoring.
33
3. Symptoms of vascular injury: Patients with groin pain or hematoma, even with intact distal pulses, should be closely monitored for possible vascular injury.22,28,34
Recommendations for Monitoring and Aftercare
Due to the high risk of vascular complications associated with displaced fragments of the lesser trochanter, especially when displacement is 1 cm or more, a comprehensive follow-up plan is crucial. Surveillance should include frequent clinical and radiologic evaluations until two important milestones are reached: 1. Radiographic confirmation of fracture healing: to reduce the risk of complica-tions, it is important to ensure that the fracture has healed adequately. 2. Successful completion of physiotherapy: Full functional recovery should be confirmed to minimize the risk of subsequent problems.
Even after reaching these milestones, it is important to continue to monitor for potential vascular complications.
Detailed Aftercare Plan
• Imaging: routine CT angiography is recommended in patients with risk factors or clinical suspicion of vascular injury. In patients with displaced fragments of the lesser trochanter or in elderly patients, CT angiography should be considered both preoperatively and, if symptoms occur, postoperatively.7,28,35 • Duration of follow-up: As symptoms may develop later, follow-up should extend beyond the immediate postoperative period. The recommended examination includes clinical and imaging follow-up at 1, 3 and 6 months postoperatively as well as additional visits based on clinical findings.28,35 • Intervention Strategy: ○ Asymptomatic pseudoaneurysms: Conservative surveillance may be sufficient for small, asymptomatic pseudoaneurysms. ○ Symptomatic or enlarged pseudoaneurysms: Timely intervention is necessary. Options range from less invasive techniques such as ultrasound-guided compression to more invasive procedures such as open surgical repair, especially in cases with displaced fragments of the lesser trochanter.29,33,35
These recommendations emphasize the importance of tailoring follow-up plans to the specific risk factors and clinical scenario of each individual patient. Further research is needed to refine these guidelines and improve outcomes for patients undergoing PFF fixation, particularly with regard to vascular complications.33,36
Case Report Insights
In our case, there was an iatrogenic delayed injury to the DFA due to an arterial wall injury caused by a proximally migrated, sharp-edged fragment of the lesser trochanter. This migration occurred during physical therapy and repetitive hip flexion, with traction of the iliopsoas muscle contributing to the rotation and proximal migration of the lesser trochanter. Thirty-three days after the original surgery, this resulted in perforation of the arterial wall and an acute clinical presentation characterized by severe groin pain and hematoma formation.
Diagnostic Challenges: Pseudoaneurysms are often difficult to diagnose due to their often-nonspecific symptoms such as pain and swelling. In addition, the deep location of the DFA means that clinical signs such as an audible bruit or pulsatile mass are often absent. It is important to note that intact distal pulses and normal distal perfusion do not rule out vascular injury. Diagnosis is further complicated by the variable time interval between fracture and onset of symptoms, as well as overlap with other conditions such as deep vein thrombosis (DVT). Therefore, maintaining a high index of suspicion is crucial.22,28,34
Diagnostic Testing: Diagnostic methods for this condition include ultrasound, Doppler ultrasound, CT angiography, magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA). Angiography or percutaneous catheterization may also be required for both diagnosis and treatment. Although there is a trend towards the use of less invasive methods such as ultrasound and MRI, CT angiography remains the gold standard for both diagnosis and treatment when there is a high clinical suspicion of a DFA pseudoaneurysm.
Management Guidelines: Recent guidelines recommend that the treatment of pseudoaneurysms should be based on their size and symptoms.35,37 Small, asymptomatic pseudoaneurysms may be monitored conservatively, whereas larger, symptomatic pseudoaneurysms (>3 cm) often require interventions such as open surgical repair, ultrasound-guided compression, thrombin injection or coil embolization. 37 Despite the increasing use of less invasive methods, CT angiography remains a valuable tool for both diagnosis and treatment, especially when clinical suspicion is high.10,28
CT Angiography and Clinical Decision Making: Although CT angiography is a highly effective diagnostic tool, it should not be considered mandatory for all cases of fractures of the lesser trochanter. Instead, its use should be guided by individual clinical scenarios, especially when pseudoaneurysms are suspected. In the preoperative assessment, especially when there is evidence of displaced fragments of the lesser trochanter, the decision to perform CT angiography should be based on the clinical presentation and available imaging results.
Treatment of Displaced Fragments of the Lesser Trochanter
Treatment of displaced fragments of the lesser trochanter is an important consideration. Ehrnthaller et al. (2017) 38 demonstrated biomechanically that refixation of the lesser trochanter fragment in unstable A2 fractures improves construct stability and may reduce migration. Recent cadaveric studies suggest that fixation of such fragments may improve overall stability and reduce the rate of migration, potentially preventing complications. However, some clinical studies suggest that not treating the lesser trochanter has no significant effect on functional outcomes.33,36 Qi Sun et al (2018) 33 found that displacement of more than 1 cm correlated with higher complication rates and postoperative pain, suggesting that fixation may reduce complications and improve pain outcomes. However, this approach is technically demanding and may increase operative time and the risk of infection. 33 The balance between potential benefits and risks should be carefully considered, and further research is needed to determine the optimal treatment strategy for displaced lesser trochanter fragments to minimize iatrogenic injury and complications.
Recommendations for Dislocated Fragments of the Lesser Trochanter
If a displaced lesser trochanter is identified preoperatively, we recommend early active treatment of even small, asymptomatic pseudoaneurysms that are discovered incidentally. The risk of enlargement or rupture of the pseudoaneurysm or further displacement of the lesser trochanter leading to rupture of the pseudoaneurysm emphasizes the importance of timely intervention. Open surgical repair is preferred in such cases as it allows direct treatment of the vascular injury and addresses the underlying cause by removing all or part of the lesser trochanter. A multidisciplinary approach involving a vascular surgeon is advisable to ensure comprehensive treatment of both the vascular injury and the associated orthopedic problems.
Conclusion
Vascular injuries after pertrochanteric fracture fixation are rare but potentially life-threatening, particularly in elderly patients with significantly displaced lesser trochanter fragments. Displacement greater than 1 cm, especially proximally toward the DFA, increases the risk of vascular complications. Early recognition through careful monitoring and timely CT angiography is crucial. Although the benefit of fragment fixation remains unclear, individualized assessment and vigilant postoperative follow-up are recommended. Further research is necessary to establish optimal prevention and management strategies.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Author Contributions
S.Č. contributed to data collection, manuscript drafting, literature review and critical revision. J.K. participated in data acquisition, literature review, and manuscript writing. V.F., M.P. and T.I. were responsible for vascular surgery expertise, case management, and interpretation of imaging findings. P.Č. and S.I. contributed to patient follow-up, clinical data analysis, and manuscript revision. M.L., N.K., and T.I. assisted with literature review, data interpretation, and manuscript editing. All authors critically reviewed the manuscript, approved the final version, and agreed to be accountable for all aspects of the work
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interest
The authors declare that there are no conflicts of interest related to this study.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.