
Abstract
Keywords
Introduction
India stands at the brink of a significant demographic shift, characterized by a rapidly aging population that presents unique challenges and opportunities for healthcare. From a modest count of 20 million elderly individuals in the early phases, the number has surged to 57 million by 1991, with projections estimating a staggering rise to approximately 324 million by 2050. This burgeoning demographic segment predominantly grapples with various health issues necessitating medical interventions, particularly orthopedic surgeries, owing to prevalent degenerative diseases and the fragility of aging bones. The escalating number of elderly patients undergoing such procedures underscores an urgent need to enhance healthcare quality by minimizing medical and surgical complications, curtailing hospital stays, and reducing readmission rates.1-4
Traditionally, chronological age has been the cornerstone for predicting surgical outcomes. However, this approach often fails to encapsulate the physiological intricacies of aging, leading to a critical evaluation of “frailty” as a more representative parameter. Frailty, a syndrome marked by decreased strength, endurance, and physiological function, heightens an individual’s susceptibility to dependency, morbidity, and mortality. It embodies a pivotal risk factor for adverse outcomes in elderly surgical patients, meriting comprehensive assessment to tailor preemptive and postoperative care.5-7
In light of these considerations, the present study embarks on an exploratory journey to assess frailty among elderly individuals undergoing major orthopedic surgeries, utilizing the Edmonton Frailty Scale (EFS) as a benchmark. 8 By delving into the correlation between frailty and socio-demographic variables such as age and gender, this research aims to unveil patterns and predictors that could revolutionize preoperative evaluations and care strategies. This endeavor not only seeks to bridge the gap between chronological and physiological aging but also to enrich the understanding of frailty’s multifaceted impact on surgical outcomes and recovery processes. Through a meticulous examination of frailty’s prevalence and its association with socio-demographic factors, the study endeavors to contribute to the overarching goal of augmenting healthcare delivery for one of society’s most vulnerable groups.
Objectives
The primary objectives of this study are to: • • •
Material and Methods
Study Design
This research is conceived as a single-center, prospective cohort study, aimed at exploring the nuances of frailty within a defined patient demographic undergoing orthopedic surgeries.
Study Period
Patients admitted and undergoing surgery between June 2019 and June 2021 were included, with a follow-up duration extending to 90 days post-surgery to monitor immediate postoperative outcomes.
Sample Size
The sample size was meticulously calculated using the formula:
Where: Z represents the confidence level (95%, equating to 1.96), p the estimated prevalence (50%), and C the confidence interval (±7.8%), culminating in a total of 157 patients for a robust statistical analysis.
Inclusion Criteria
• Patients aged 60 years and above. • Those requiring orthopedic surgical intervention.
Exclusion Criteria
• Patients younger than 60 years. • Cases involving revision surgery, peri-prosthetic fractures, implant failures, infections, pathological fractures, isolated fractures of non-load-bearing bones, cancer patients, single-level discectomies, outpatient procedures, and conservatively managed patients.
Data Collection
Data were gathered through a comprehensive geriatric assessment, which included the FRAILTY assessment, administered upon admission as part of a broader initiative to enhance patient care. This assessment encompassed various variables, including demographic details, medical history, medication usage, and previous hospital admissions. During this period, we assessed 276 patients aged >60years and requiring major orthopedic surgical intervention including: • Major hip surgery • Spine surgery • Inter-trochanteric fracture fixation • Fracture neck of femur • Total knee and hip replacement • Lumbar spine fixation • Cervical spine fixation
Out of these 276 patients, 157 patients included in this study (Figure 1) Patient Assessment Flowchart.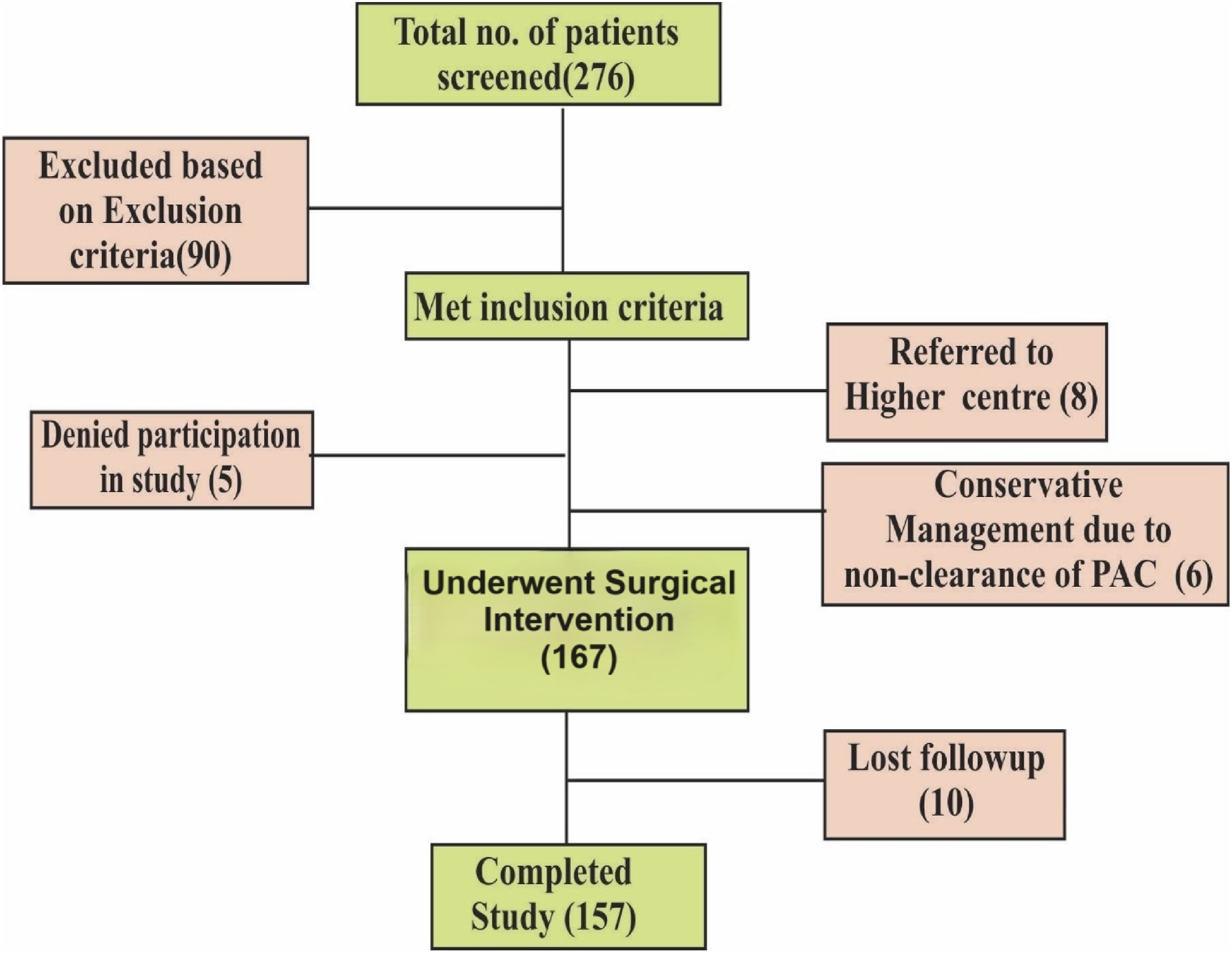
STROBE Guidelines followed while preparing the manuscript.
Assessment of Frailty
Table for Edmonton Frail Scale and Scoring Cut off for Different Group of Frailty.


Outcome
Data was used to evaluate the prevalence of frailty in elderly population presenting for major surgery and also, the distribution of frailty on basis of age and gender of patients.
Statistical Analysis
Data were analyzed to extract meaningful insights into the correlation between the frailty index and socio-demographic variables, with specific attention to age and gender. Statistical analysis was performed using Pearson chi-square tests, independent sample t-tests and one-way ANOVA.
Statistical Software SPSS version 25 use to ascertain the significance of observed patterns and trends, facilitating a comprehensive understanding of frailty’s impact on the elderly undergoing orthopedic surgeries. A P-value of less than .05 was considered statistically significant.
Results
Age & Gender Distribution of Study Participants.

Among the 157 participants, 59.2% (n = 93) are males aged 60 and above, while the remaining 40.8% (n = 64) comprise females within the same age category (Table 2).
Frequency Distribution of Frailty Categories.

On assessment of the general health status of participants , 2.5% of patients exhibited excellent health, marked by zero hospitalizations, while 41.4% had fair health (1 point), and 10.2% experienced multiple hospital admissions (2 points). Moreover, 16 (10.2%) and 8 (5.1%) individuals were categorized with 3 and 4 points, respectively, indicative of deteriorating health conditions necessitating frequent hospitalizations.
Functional independence, crucial for daily activities, varied among participants. A significant proportion (23.6%) displayed complete autonomy, while 63.1% could perform some tasks independently but relied on assistance for others. Additionally, 13.4% relied entirely on others for routine activities, highlighting varying degrees of dependency within the group.
Medication adherence emerged as a concern, with 40.8% managing without regular medication, 45.2% occasionally missing doses, and 14.0% struggling with consistent adherence, often due to a regimen of five or more prescriptions. Weight loss, reported by 37.6%, and differing emotional states were also noted, with 60.5% feeling content and 39.5% experiencing sadness or depression.
Cognitive function, evaluated using standardized scales, revealed diverse profiles, with 42% exhibiting good cognition, 16% poor cognition, and 42% demonstrating an intermediate level. Furthermore, urinary control issues affected 12.7% of participants, while the majority (87.3%) reported no such concerns.
Prevalence of Individual Components of Frailty Criteria.

On observing gender prevalence in different frailty groups we found that although the number of males is more in almost all groups except severe frail but as the frailty severity increases, the proportion of females increases in each group (Figure 2) Gender Disparity in Frailty Distribution Among Elderly Orthopedic Surgery Patients.
On observing age distribution in different frailty groups we found that as the frailty severity increases the proportion of older individual increases (Figure 3) Age-Related Variations in Frailty Severity Among Elderly Orthopedic Surgery Patients.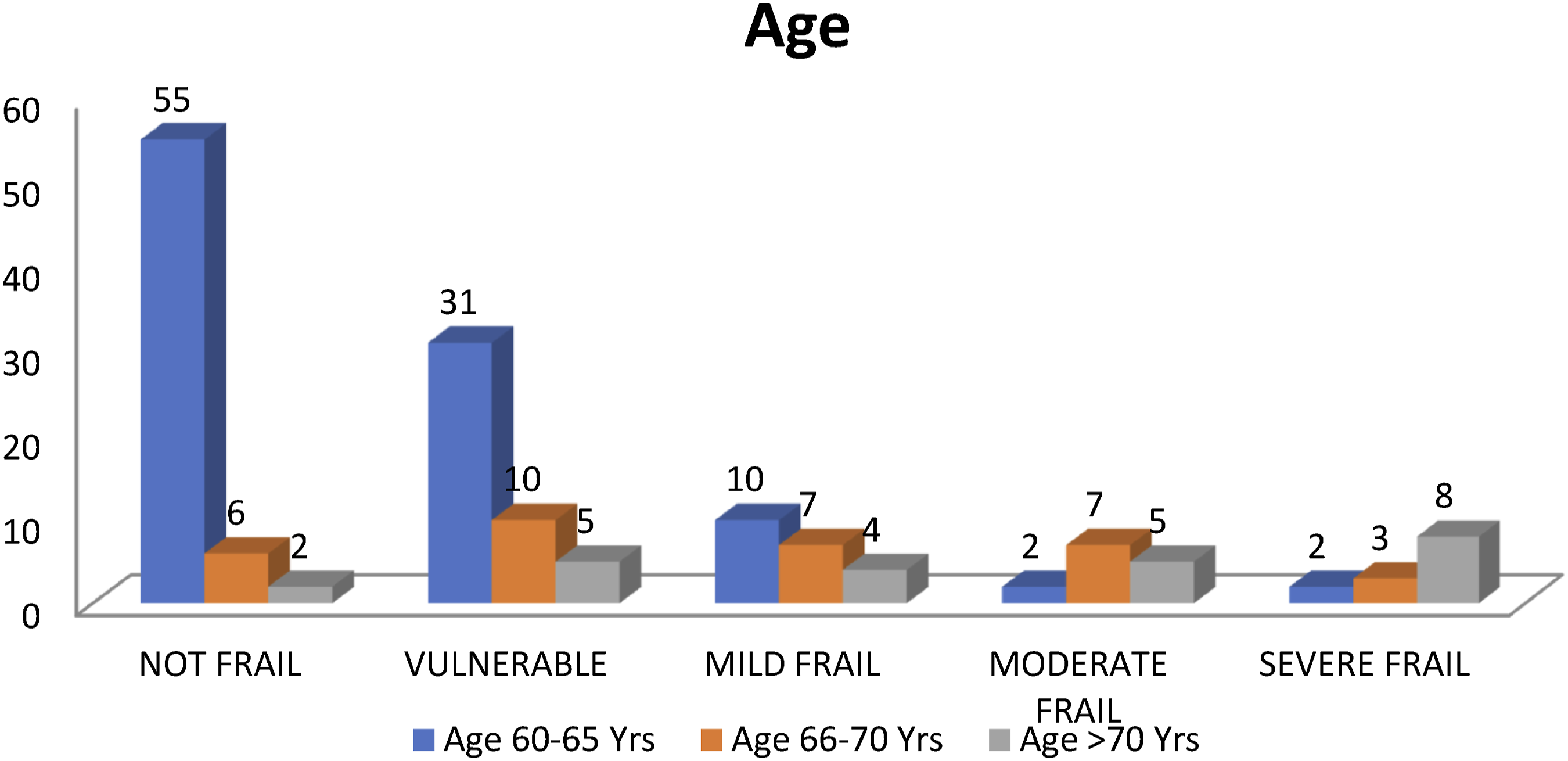
Association of Frailty Levels With Age and Gender Among Elderly Orthopedic Surgery Patients.

Discussion
The study examined the prevalence and implications of frailty among elderly patients undergoing major orthopedic surgeries, utilizing a robust dataset and the Edmonton Frail Scale (EFS) for assessment. The results illuminate the complex interplay between frailty, age, and gender within this demographic.
This study sheds light on the intricate relationship between frailty and socio-demographic variables, particularly age and gender, among elderly patients undergoing major orthopedic surgeries. The utilization of the Edmonton Frailty Scale (EFS) facilitated a nuanced understanding of frailty, highlighting its prevalence and varying degrees among the study population.
Frailty prevalence in older adults is a significant concern, as evidenced by this study’s findings. The research reveals that only 40% of the study population exhibited non-frail status, while the remaining 60% were classified as either vulnerable (29.3%) or frail (∼31%). Discrepancies in reported frailty prevalence across studies stem from variations in definitions, inclusion criteria, and study populations. For instance, the SHARE study, encompassing 10 European countries and Israel, reported an overall frailty prevalence of 17%, highlighting regional variations influenced by factors such as sex, age, ethnicity, and socioeconomic status. 9 In India, limited studies are available on frailty prevalence. A hospital-based study in India reported a frailty prevalence of 33%, while a large population study using the frailty index found a prevalence of 55.5%.10,11 Additionally, research by Rohrmann et al 12 highlighted that frailty increases with age and is more prevalent in women than men. Similarly, a meta-analysis by O’Caoimh et al 13 across 62 countries found common frailty prevalence rates, with variations based on the frailty measurement scale and geographical area, emphasizing the higher prevalence among females using different assessment methods. These findings underscore the need for comprehensive approaches to address frailty among older adults, considering its multifactorial nature and demographic variations.
Frailty components were meticulously assessed in this study, revealing significant findings. Among the patients with a history of multiple hospital admissions, only a small proportion (2.5%) reported excellent general health, while a concerning 5.1% experienced frequent and multiple hospitalizations, indicative of very poor general health. The majority described their general health as fair. Functional independence was notably limited, with only 23.6% being functionally independent, while the majority were either partially dependent (63.1%) or completely dependent (13.4%) on others for daily activities. Polypharmacy emerged as a concern, with 40.8% not requiring regular medication and 14.0% managing five or more prescription drugs but often forgetting doses. Significant weight loss affected 37.6% of the population, while depression was prevalent in 39.5%. Poor cognition was noted in 16%, and urinary incontinence history was reported by 12.7%, highlighting the multifaceted nature of frailty.
Gender disparities in frailty were observed, with a higher overall number of males across different frailty groups. However, the proportion of females increased with the severity of frailty, suggesting a greater vulnerability among females. This aligns with previous studies showing that women are more prone to frailty, with research indicating that women are two times more vulnerable than men in elderly populations.14,15 Age played a significant role in frailty determination, with patients of all age groups represented across frailty categories. Nonetheless, the mean age increased with frailty severity, indicating the association between aging and frailty. Frailty was defined as a complex age-associated syndrome by Kadjo Yves Cedric Adja, resulting from physiological system decline, leading to increased vulnerability to stressors and impaired homeostatic ability. 16 These findings emphasize the intricate relationship between gender, age, and frailty, highlighting the need for comprehensive approaches to address frailty among elderly populations.
Limitations
Despite its insightful findings, this study is not without limitations. This study was conducted during the global COVID-19 pandemic, which may limit generalizability to the current post-pandemic situation. The descriptive and single-center nature of the research also limits the generalizability of the results to wider populations. The study’s relatively small sample size and the specific demographic of railway employees and their dependents, who have relatively easy access to healthcare services, may not fully represent the broader elderly population undergoing orthopedic surgeries. Additionally, the absence of long-term follow-up restricts the ability to assess the sustained impact of frailty on postoperative outcomes.
Conclusion
The study conclusively demonstrates the pervasiveness of frailty among elderly individuals undergoing major orthopedic surgeries and its significant correlation with socio-demographic variables, particularly age and gender. The Edmonton Frailty Scale proves to be a valuable tool in identifying frailty, underscoring the importance of comprehensive preoperative assessments to tailor care plans and interventions. Addressing frailty in this demographic is imperative for improving surgical outcomes, enhancing recovery processes, and ultimately, elevating the quality of life for the elderly.
Recommendations
Based on the study’s findings, it is recommended to increase awareness among healthcare professionals about the significance of frailty in elderly patients, emphasizing routine frailty assessments in preoperative evaluations. A multidisciplinary approach integrating nutritional, psychological, and rehabilitative support alongside medical interventions should be adopted to manage frailty effectively. Gender-sensitive assessment and treatment protocols should be developed to address observed differences between males and females. Further research through larger-scale, multi-center studies with diverse populations and longer follow-up periods is essential to validate and expand upon the study’s findings. Standardization of frailty assessment tools across healthcare settings is crucial for early identification and intervention. Additionally, preventive strategies focusing on physical activity programs, nutritional support, and medication management plans should be developed to delay the progression from pre-frailty to frailty, ultimately enhancing the care and outcomes for elderly patients undergoing orthopedic surgeries.
Footnotes
Acknowledgements
We sincerely thank Dr Ajay Jaiswal for their invaluable assistance with data collection and analysis. Special thanks to Dr Amol and Mr. Tanwar for their expert guidance on statistical methodologies and Miss Shalini Kumari for their support in manuscript preparation, editing and providing technical support throughout the study. We are grateful to all the participants who took part in this study, without whom this research would not have been possible.
Statements and Declarations
Author Contributions
This study was designed and organized by Dr Rushama Tandon and Dr Ashutosh Kapoor. Data collection, analysis and writing of the first draft was by Dr Rajan Kumar Singh, supported by Dr anil kumar verma and Dr Nand kishor kaushal. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.