
Abstract
Background
Hip fractures are a major public health concern with a high mortality rate. Numerous risk factors for hip fracture have been identified, and efforts made to reduce complications and improve outcomes. This study aimed to assess recent trends in postoperative complications amongst early-career orthopaedic surgeons.
Methods
This retrospective study analyzed surgical cases submitted to the American Board of Orthopaedic Surgery (ABOS) for the Part II Oral Examination from 2013 to 2022. The database includes patient demographics and medical and surgical complications. Current Procedural Terminology codes reflecting operative fixation for hip fracture were selected. Data was split into two cohorts: 2013-2016 and 2017-2020. Univariate and multivariable logistic regression analyses were used to identify significant differences between cohorts.
Results
49,418 cases were analyzed. Compared to 2013-2016, 2017-2020 had a reduction in the overall medical complication rate (−1.49%, P = 0.0005), saw slight increases in congestive heart failure (+0.18%, P = 0.049), renal failure (+0.37%, P = 0.004), hypotension (+0.41%, P = 0.0007), and hypoxia (+0.41%, P = 0.0016). Minor decreases in myocardial infarction (−0.18%, P = 0.047) and pneumonia (−0.34%, P = 0.021) were noted. No differences occurred in confusion/delirium, deep vein thrombosis/pulmonary embolism, and mortality. There were no significant differences in overall surgical complications. The 90-day readmission rate increased with time (+1.17%, P < 0.0001). Multivariable logistic regression identified a decrease in the likelihood of overall medical complications (Odds Ratio (OR): 0.92 [0.89, 0.96]; P < 0.0001). Decreases were noted for the likelihood of myocardial infarction (OR: 0.81 [0.68, 0.98]; P = 0.031), pneumonia (OR: 0.87 [0.78, 0.97]; P = 0.013), fracture (OR: 0.80 [0.69, 0.92]; P = 0.002), and recurrent/persistent/uncontrolled pain (OR: 0.72 [0.56, 0.92]; P = 0.008). The likelihood of renal failure (OR: 1.18 [1.04, 1.34]; P = 0.009) and readmission increased (OR: 1.14 [1.07, 1.20]; P < 0.0001).
Conclusion
This study found little change in postoperative complication patterns over the past decade. These findings suggest that more efforts are needed to improve hip fracture care and outcomes.
Introduction
Hip fracture represents a major public health concern in the United States. It carries a reported mortality rate of 2%-14% for patients during hospital admission and a one-year mortality rate of 14%-36%.1-3 Hip fracture care is expensive, costing an estimated $10.3 billion to $15.2 billion annually in the United States. 4 The risk of hip fracture increases with age, and in an aging population, the associated complications are also likely to increase.5,6
Hip fracture risk has been associated with poor nutritional status, tobacco use, low body mass index (BMI), and the presence of osteoporosis.7-9 Advancing age, frailty, poor functional status, cognitive impairment, delayed surgical management past 48 hours, concomitant fractures, and medical comorbidities (malignancy, pulmonary disease, diabetes mellitus, and cardiovascular disease) are independently associated with complications following hip fracture surgery as well as one-year mortality.10-13
Many efforts have been made to reduce hip fracture complications including anticoagulation, optimized anesthetic management, improved hip fracture implants, and Enhanced Recovery after Surgery (ERAS) protocols. 3 Co-management of patients by orthopaedic surgeons and geriatricians, and the use of an organized hip fracture program, which many hospitals currently utilize, are thought to result in shorter times to surgery, shorter length of stay (LOS), and fewer complications following operation.14-16
However, the specific trends in hip fracture fixation practices and outcomes among early-career orthopaedic surgeons have not been extensively studied. During the recent Coronavirus 19 (COVID-19) pandemic, training disruptions for early-career orthopedic surgeons led to reduced hands-on experience due to the sharp decline in elective surgeries.17,18 Additionally, reduced automotive traffic from travel restrictions significantly decreased the number of trauma admissions to emergency departments.19,20 These factors contributed to a decrease in overall procedural volume, which, in conjunction with a shift toward virtual learning environments, potentially impacted the skill development of new surgeons. 21
The purpose of this study is to investigate the recent trends in post-operative complications following hip fracture among candidates submitting cases to the American Board of Orthopaedic Surgery (ABOS) for the Part II Oral Examination. Given the challenges involved with the management of patients with hip fracture, we hypothesize that despite recent improvements in care (protocols, implants, organized co-managed care programs), there have been no significant improvements in surgeon reported post-operative complications over the past 10 years.
Materials and Methods
Study Design
This is a retrospective study analyzing surgical cases submitted to the American Board of Orthopaedic Surgery (ABOS) by candidates taking the Part II Oral Examination from 2013 to 2022. The data was split into two primary cohorts based on examination years: 2013-2016 and 2017-2020. Additionally, a sub-analysis examined the impact of COVID-19 on complication rates by splitting the data into two cohorts: 2018-2019 and 2021-2022.
Data Source and Analysis
The demographics and data collection utilized in the ABOS database have been previously discussed.22-24 In short, this Case List database consists of all self-reported consecutive surgical cases recorded over a six-month period by applicants for ABOS Initial Board Certification. Each case has a maximum of seven months follow-up and was deidentified for research purposes. Due to the COVID-19 pandemic, the 2021 Examination Year includes nine months of cases instead of six months. The surgical cases listed by each candidate must be independently certified by the hospitals/institutions where the procedure was performed.25-28 70% of candidates take the Part II Oral Examination within the first two years after completion of their training (residency or fellowship), and 98% take it within the first five years. 29
A research proposal was submitted and approved by the ABOS research committee to query the database for cases with Current Procedural Terminology (CPT) codes that are reflective of operative fixation for hip fracture. CPT codes included 27235 (percutaneous skeletal fixation of femoral neck fracture), 27236 (open treatment of femoral neck fracture, internal fixation/prosthetic replacement), 27244 (treatment of pertrochanteric femoral fractures with a plate or screw type implant), and 27245 (treatment of pertrochanteric femoral fracture with intramedullary implant). Other elements that were assessed include patient demographics, such as the patient’s age and sex, and the geographic region and fellowship training of the candidate surgeon performing the case. Patients younger than 18 years old were excluded. Anesthetic, and various medical and surgical complications associated with the procedure, as well as unexpected 90-day readmissions and 90-day reoperations, were also collected from the database. Complication categories were determined by ABOS. Medical complications included: anemia, arrhythmia, cerebrovascular accident (CVA), confusion/delirium, congestive heart failure (CHF), deep vein thrombosis (DVT), gastrointestinal (GI) bleeding/ulcer/gastritis, hypotension, hypoxia, myocardial infarction (MI), pneumonia, pulmonary embolism (PE), renal failure, respiratory failure, urinary tract infection, and unspecified. Mortality was also collected. Surgical complications included: bone fracture, compartment syndrome, failure of tendon/ligament repair, hemarthrosis/effusion, hematoma/seroma, implant failure/fracture/malfunction, limb ischemia, loss of reduction, malunion, nonunion/delayed union, wound healing delay/failure, skin ulcer/blister, pain – recurrent/persistent/uncontrolled, vascular injury, nerve palsy/injury, and unspecified. This study was approved by our university Institutional Review Board.
Statistical Analysis
All analyses were completed using JMP Software (Version 16.0, SAS Institute Inc., Cary, NC). An alpha of 0.05 was used for statistical significance.
The data was first split into two cohorts using examination years: 2013-2016 and 2017-2020. Patient and candidate characteristics, as well as complications, between these two cohorts were calculated using the mean with standard deviation (SD) for continuous variables and total number (n) with percentage for categorical variables. Univariate analysis was performed in order to identify significant differences between the two cohorts. Independent-sample t-tests and Pearson’s chi-square tests were used to evaluate the continuous and categorical variables, respectively. Multivariable logistic regression analyses adjusting for potential cofounders were subsequently performed to determine adjusted differences in the rate of complications over time.
A sub-analysis further examined the impact of COVID-19 on complication rates. For this analysis, the data was split into two cohorts using examination years: 2018-2019 and 2021-2022. Univariate analysis was performed using a similar process as above.
Results
Patient Demographics for Patients Undergoing Hip Fracture Fixation Between 2013-2016 and 2017-2020.
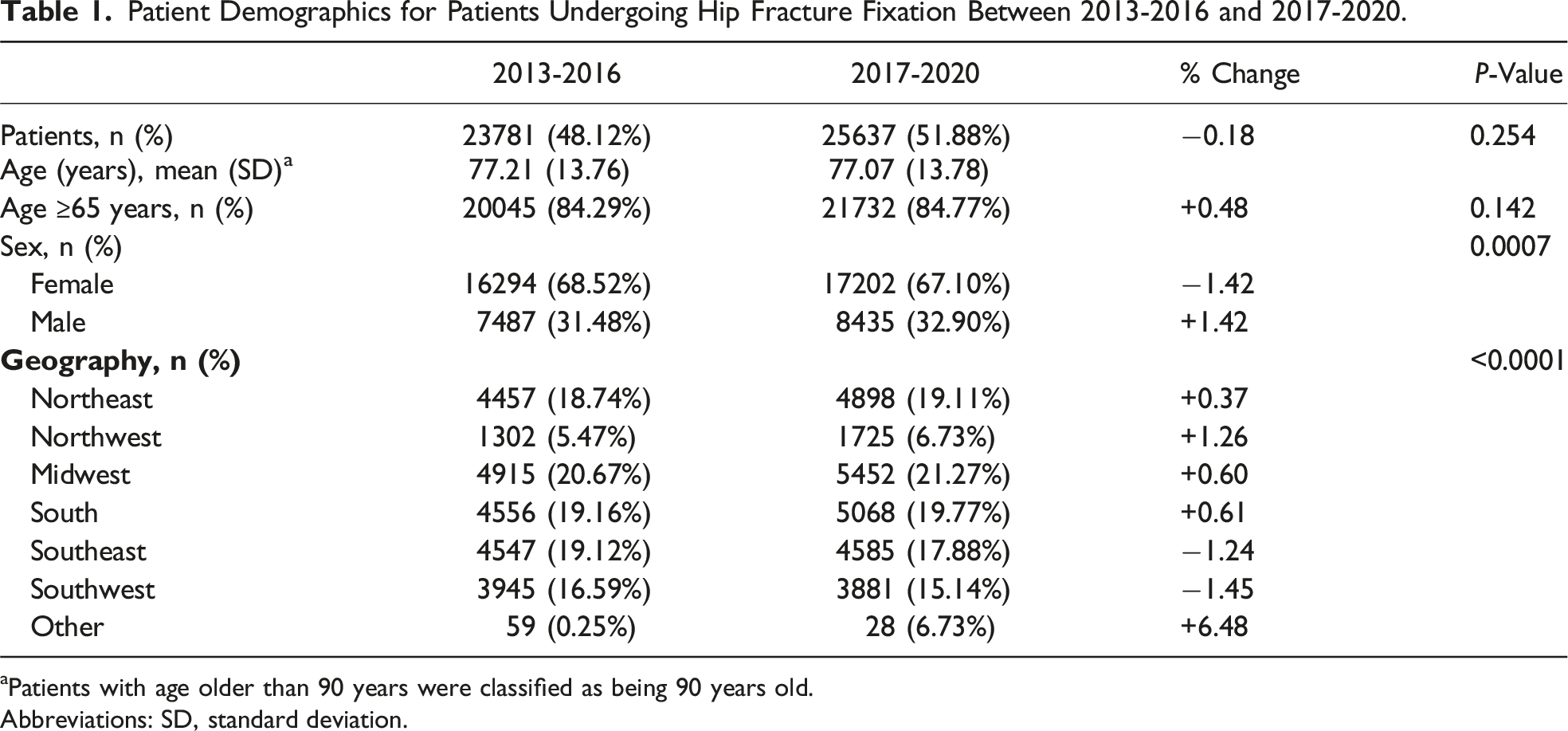
aPatients with age older than 90 years were classified as being 90 years old.
Abbreviations: SD, standard deviation.
Cases/Candidate Data for Patients Undergoing Hip Fracture Fixation Between 2013-2016 and 2017-2020.

Abbreviations: CPT, Current Procedural Terminology; ABOS, American Board of Orthopaedic Surgery.
27235: percutaneous skeletal fixation of femoral neck fracture.
*27236: open treatment of femoral neck fracture, internal fixation/prosthetic replacement.
*27244: treatment of pertrochanteric femoral fractures with a plate or screw type implant.
*27245: treatment of pertrochanteric femoral fracture with intramedullary implant.
Postoperative Complication Rates for Patients Undergoing Hip Fracture Fixation Between 2013-2016 and 2017-2020. a

aComplications with rates less than 0.5% were excluded from this table.
Abbreviations: CVA, cerebrovascular accident; CHF, congestive heart failure; DVT, deep vein thrombosis; PE, pulmonary embolism; GI, gastrointestinal; UTI, urinary tract infection.

Visual representation of the complication rates, 90-day readmission rate, and 90-day reoperation rate over time in patients with hip fracture. The overall complication rate ranged from 37.3% to 44.6%, with most complications being medical in nature (Range: 30.5% to 38.8%). However, addressing surgical complications (Range: 9.7% to 13.2%) could potentially yield easier improvements.
90-day Readmission and Reoperation Rates for Patients Undergoing Hip Fracture Fixation Between 2013-2016 and 2017-2020. a
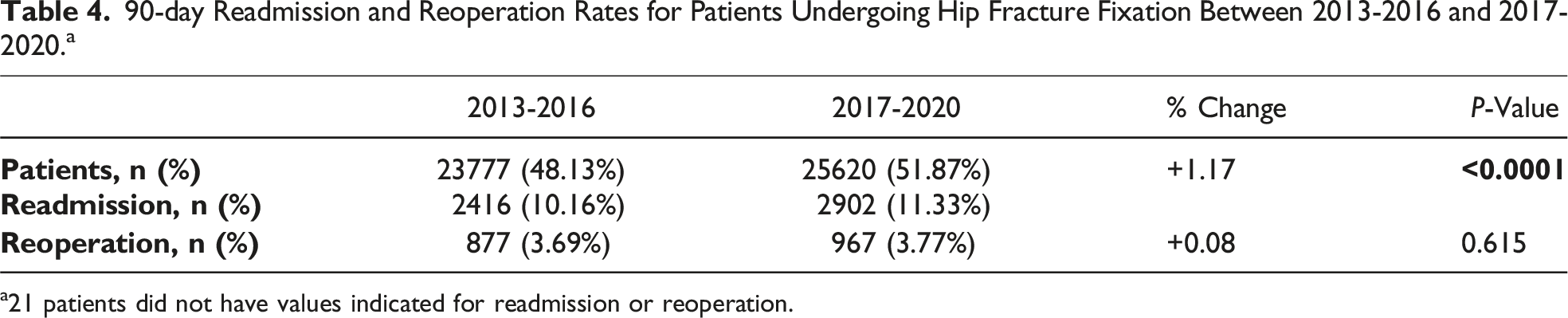
a21 patients did not have values indicated for readmission or reoperation.
Multivariable Logistic Regression by Complication for Patients Undergoing Hip Fracture Fixation. a

aOnly complications considered to be clinically severe were included. For each complication, age, sex, CPT code, trauma fellowship status, and time period were used in a logistic regression. Only those factors found to be independent risk factors are reported.
Abbreviations: OR, odds ratio; CI, confidence interval; CPT, Current Procedural Terminology; CHF, congestive heart failure; MI, myocardial infarction.
Demographic, Postoperative Complication, Re-admission, and Re-operation Results for Patients Undergoing Hip Fracture Fixation During Non-COVID (2018-2019) and During COVID (2021-2022). a
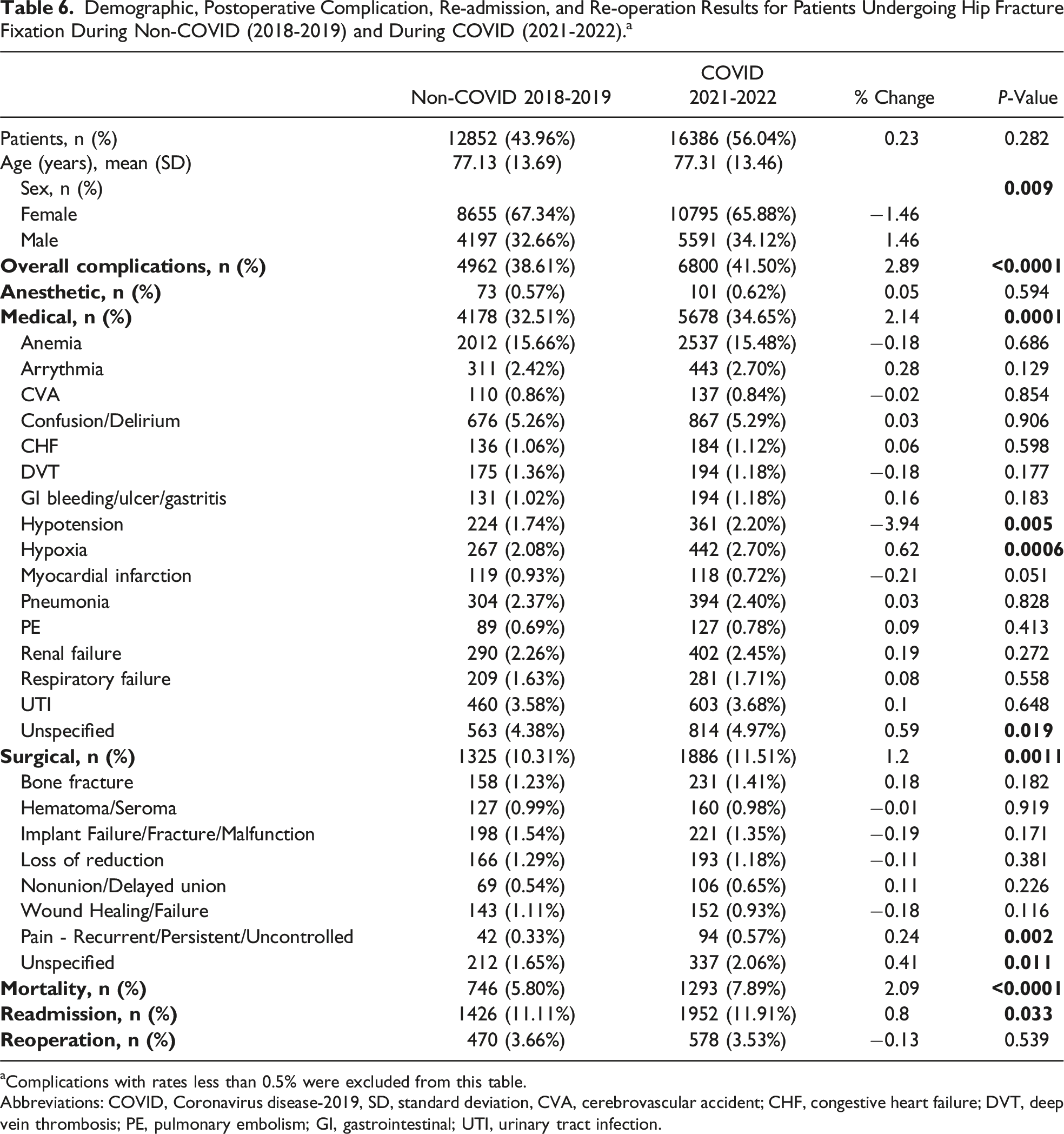
aComplications with rates less than 0.5% were excluded from this table.
Abbreviations: COVID, Coronavirus disease-2019, SD, standard deviation, CVA, cerebrovascular accident; CHF, congestive heart failure; DVT, deep vein thrombosis; PE, pulmonary embolism; GI, gastrointestinal; UTI, urinary tract infection.
Discussion
The incidence of hip fracture has slightly decreased but the prevalence continues to rise with the aging population.16,30 Despite numerous advances targeting preoperative optimization, intraoperative management, and postoperative models of care, our analysis of the ABOS Part II Oral Examination Case List database found that in recent years, there was only a slight decrease in the overall complication rate with many postoperative medical and surgical complications showing no significant change and some even increasing in incidence. To our knowledge, this is the first study that has reported temporal trends in complications following hip fracture surgery amongst early-career orthopaedic surgeons.
Our study identified no significant difference between patients treated by early-career orthopaedic surgeons in the latter half of the past decade and patients treated in the first half with respect to age. Although females represented most patients in both cohorts, an increasing number of males are being treated for hip fracture. The reduced rate of females experiencing hip fractures may reflect screening recommendations from the U.S. Preventive Services Task Force pertaining to postmenopausal women.31-33 Our study also found an increase in trauma-fellowship-trained orthopaedic surgeons treating hip fracture. This is reflective of the rise in orthopaedic residency graduates seeking fellowship training as well as the increase in fellowship-trained surgeons performing procedures within their area of subspecialty training.34,35 Multivariable analysis found that the completion of a trauma fellowship was associated with a variety of complications (Table 5). This was previously studied by Ottesen et al, who concluded that this may be a result of a more acute and medically complex subset of patients treated by orthopaedic traumatologists. Additional evidence is required to support or refute this hypothesis. 35
Similar to Smith et al, our study found an increase in the number of hip fractures being treated with an IMN as opposed to a SHS. 36 Furthermore, in our multivariable analysis, fractures treated using an IMN were associated with medical complications, including MI and renal failure, surgical complications, including periprosthetic bone fracture, and readmission. However, our analysis did not control for type of hip fracture. As such, it is possible that many fractures treated with IMN were subtrochanteric in nature, which have been found to have a higher risk for nonunion. 37 Given these results, it is important to consider the individual’s specific fracture characteristics before choosing an implant for treatment. A recent Cochrane review found that a SHS yields very similar functional outcomes to an IMN in the management of extracapsular fragility hip fractures. 38 The review reported a reduced risk of infection and non-union with an IMN; however, there is an increased risk of implant-related fracture that is not attenuated with newer designs. There may be limited exposure of orthopedic trainees to SHS, reinforcing the ongoing preference for more expensive IMN, impacting both residency education and healthcare costs despite the lack of clear evidence for improved outcomes.39,40
Our study found a slight reduction in the overall complication rate of hip fractures treated by early-career orthopaedic surgeons. Specifically, rates of medical complications, such as MI and pneumonia, and surgical complications, such as periprosthetic bone fracture and recurrent/persistent/uncontrolled pain slightly decreased. While it is unclear whether these results are associated with any intervention, it is possible that these decreases are attributable to improved protocols tailored towards perioperative optimization of patients with hip fractures. One example of such a protocol is ERAS, which consists of selected interventions performed preoperatively, intraoperatively, and postoperatively, with the purpose of improving clinical outcomes. 41 In a propensity score-matched analysis, ERAS protocols applied to intertrochanteric fractures decreased LOS, alleviated patient pain, promoted early recovery of the patient’s hip function, and effectively mitigated complications. 42 Although orthogeriatric care has been postulated to reduce LOS, in-hospital and 1-year mortality, and delirium in hip fracture patients, a recent meta-analysis states that evidence for this is of moderate quality, suggesting the need for adequately powered randomized controlled trials to better evaluate the effect of various orthogeriatric care programs on hip fracture management. 43
Despite the decline in short-term complication rates, our study reveals high overall medical and surgical complication rates of 33.4% and 11.3%, respectively, among early-career orthopedic surgeons. This contrasts with the National Inpatient Sample (NIS) database, which covers orthopedic surgeons across all career stages and reported a lower overall complication rate of 26.8% for 2016.; however, some specific complications such as CVA, delirium, and renal failure were not assessed. 30 The higher rates in our study may underscore the need for more practice and skill refinement among newly trained surgeons. It may also highlight the importance of improving patient management across the healthcare continuum, from preoperative assessments to postoperative care and follow-up. 44
Our study found an increase in the rate of postoperative renal failure. Prior work suggests acute renal failure is a common complication of surgery in elderly patients who sustain a hip fracture and is associated with increased mortality up to one year after surgery, even after adjusting for coexisting co-morbidities and medications before surgery. 45 In our study, we were unable to assess pre-existing co-morbidities, such as chronic kidney disease (CKD) that may predispose a patient to postoperative renal failure. Low preoperative albumin levels, use of angiotensin-converting enzyme (ACE) inhibitors or angiotensin II receptor blockers (ARBs), the need for blood transfusion, and coronary artery disease were shown to be independent risk factors for acute kidney injury following hip fracture surgery. 46
Of note, many troublesome medical complications, such as CVA, confusion/delirium, DVT/PE, and mortality did not significantly change over the course of our study. Confusion/delirium was the most common complication in our study at a rate of <6%. This complication was likely underreported given a prior meta-analysis suggesting an incidence of up to 54% in hip fracture patients. 47 A recent quality improvement project found that common reasons that may explain this underreporting in hip fracture patients include difficulties in identifying delirium and challenges in accurately documenting the diagnosis despite successful identification. 48 Delirium is a common, poorly understood, challenging clinical problem for older adults, often complicating major surgery. 49 Delirium has been shown to increase the risk of readmission, which, in turn, increases healthcare expenditures as well as the risk for mortality.50,51 Our study also found an increase in the rates of readmission over the past decade. Readmission after hip fracture is highly undesirable, with a mortality rate of approximately 20%. 50 Unfortunately, there are no validated approaches to reducing the rate of readmission following hip fracture. The persistent challenges with delirium diagnosis and management in hip fracture patients underscore the need for enhanced education on these aspects during residency for early-career orthopedic surgeons.
It is important to note that certain complications may result from the type of procedure performed. For instance, interventions utilizing polymethyl methacrylate (PMMA) or bone cement for trauma cases have been found to contribute to bone cement implantation syndrome (BCIS) which is an amalgam of medical complications, including hypoxemia, hypotension, and unexpected loss of consciousness. 52 Recognizing these specific procedure-related risks is crucial for understanding the broader spectrum of complications and tailoring preventative strategies.
The mortality rate did not significantly change over time in our study. The inpatient mortality rate of approximately 6% between the years 2017 and 2020 is higher than the 2.4%-3.1% reported in the literature.30,53-55 Sub-analysis showed that the mortality rate increased to approximately 8% during the years 2021 to 2022, during the COVID-19 pandemic. Using the National COVID Cohort Collaborative (N3C) Data Enclave, 56 Levitt et al found that the 30-day mortality was 14.6% in patients with COVID-19 and hip fracture, compared to 3.8% in COVID-19-negative patients. 57 This increase in mortality rate may not be directly related to COVID-19 sequelae alone, but may also have been influenced by a higher Charlson Comorbidity Index in the COVID-19 positive group, potential delays to surgery, and other systemic health care factors. 57
This study is not without limitations. With regards to the study sample, neither a power analysis nor normality checks were performed. All patients provided by ABOS were included in this study. The reported complications represent short-term follow-up only (7.3 weeks +/− 6.1 weeks). When interpreting our findings, a key consideration is the possibility that the rising rates of postoperative complications may be attributable to enhanced surveillance and/or a lower threshold for reporting complications. The inherent biases of any retrospective review hold true in this study. Furthermore, the ABOS dataset does not provide granular patient co-morbidity data, thus limiting our analyses. Additionally, as the data is surgeon self-reported, there is a possibility of data entry errors, underreported cases, and variations in the classification of complications, as such, the database may not capture all complications and 90-day readmission rates. Nevertheless, the ABOS database cases are independently certified by the hospitals where the procedures were performed.25-27 Additionally, specific variables, including baseline comorbidities, co-management of care, and time to surgery, were not assessed in our multivariable analysis as they were not included in the database. These remain significant factors impacting short-term outcomes in hip fracture care 58 and future studies should aim to incorporate these critical variables to provide a more comprehensive understanding of hip fracture trends.
Conclusion
There remains much room for improvement in the management of hip fractures. Using the ABOS database, we identified a reduction in the rates of postoperative medical complications, such as MI and pneumonia, and surgical complications, such as bone fracture and recurrent/persistent/uncontrolled pain. This may reflect increased utilization of ERAS and improved pain management protocols. However, this study identified several postoperative complications that have either shown no improvement or have increased in incidence, including delirium, renal failure, and mortality. Strict adoption of evidence-based treatments aimed at mitigating these complications and a focus on enhancing perioperative medical care for patients with hip fracture presents a promising route towards improving patient outcomes. This suggests a future course of study and research.
Footnotes
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is partially supported by Clinical Translational Science Award CTSA: #1UL1TR002649.
Ethical Statement
Data Availability Statement
The data that support the findings of this study are available from the American Board of Orthopaedic Surgery, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data may however be available from the authors upon reasonable request and with permission of American Board of Orthopaedic Surgery.