
Abstract
Background
Hip fractures in the geriatric population are frequently encountered. There is increasing focus on minimizing the delay to surgery in these patients. This study was designed to evaluate factors responsible for a delay to surgery in a geriatric hip fracture population and how time to surgery affects mortality.
Methods
A retrospective cohort of patients sustaining low energy geriatric hip fractures in either an American College of Surgeons (ACS) verified Level 1 trauma center or a local university affiliated community teaching hospital were reviewed. The following variables were evaluated as independent risk factors for delay to surgery: demographic data, surgical details, use of cardiology resources, treatment center, and comorbidities. As a secondary objective, the effect of time to surgery on 1 year mortality was analyzed.
Results
1157 patients met inclusion criteria. The following factors increased the risk of delay to surgery greater than 48 hours: male sex, treatment in a community hospital (versus trauma center), older age, multiple comorbidities (eg, cardiovascular-related conditions or other fractures), cardiology consultation, and an American Society of Anesthesiologists physical status score of 3 or 4. Cardiology consultation was the strongest independent predictor of risk for delay to surgery of >48 hours (odds ratio, 6.68; 95% confidence interval, 4.40 to 10.14; P < .001). The 1-year mortality of patients did not differ when surgical treatment occurred before 48 hours or after 48 hours (Log-rank test P = .109).
Conclusion
The presence of cardiovascular comorbidities and cardiology consultations can delay surgical treatments for hip fractures in patients greater than 65 years old, but the delay did not influence 1-year all-cause mortality.
Level of Evidence
Level IV.
Introduction
Hip fractures are a common orthopedic condition that is treated operatively, with a worldwide annual incidence rate estimated to be 6.26 million by 2050. 1 Notably, the in-hospital mortality rate for patients with hip fractures can be as high as 14%, with 1-year mortality rate reaching 36%.2-6 There is some evidence that a timely treatment of these fractures (within 24 to 48 hours) reduces the mortality and results in better outcomes.7-9 A delay in treating hip fractures has been associated with an increased risk of mortality, longer hospital stays, and an increase of nonsurgical complications, such as pneumonia, decubitus ulcers, and venous thromboembolism.5,10-16
Surgical treatment may be delayed because of preoperative optimization (such as cardiology consultation and/or additional cardiac testing), associated injuries, the day of admission, and staff availability. 17 The American College of Cardiology Foundation and the American Heart Association consider surgical treatment of hip fractures as an intermediate risk procedure, with a 30-day cardiac event rate of 1%-5%. 18 The main causes of in-hospital death after hip fracture include cardiac failure and myocardial infarction; the latter is responsible for 35%-42% of these in-hospital deaths.5,6 Although patients may benefit from a thorough cardiac evaluation to address modifiable risk factors before they undergo surgical procedures, indiscriminate consultations and testing results may unnecessarily delay treatment and provide no discernible benefit. 19
Clinical reasoning should be applied to surgical treatments for hip fracture, and there is a need for guidelines in the design of future hip fracture protocols. Previous publications may not be generalizable to all healthcare settings. Thus, we investigated factors that delay hip fracture surgery more than 48 hours in a geriatric population. We hypothesized that cardiology consultations delay surgical treatment and that patients with a time to surgery of >48 hours have higher mortality rates.
Methods
Study Design and Patient Population
This was a retrospective review of patient records. Patients undergoing treatment for intracapsular or extracapsular hip fractures (AO/OTA 31-A and 31B fractures) 20 according to diagnostic codes at 2 hospitals between January 2010 and January 2018 were identified. An Institutional Review Board reviewed and approved this study. A waiver of consent was granted.
Inclusion/Exclusion Criteria
Electronic medical records were screened for male and female patients aged 65 years and older coming to either of the 2 included hospitals during the cohort period that were surgically treated for a hip fracture. The following International Classification of Disease (ICD) codes were used: 821.00 (ICD-9) and S72.0 (ICD-10). Patients with pathologic fractures, periprosthetic fractures, open fractures, incomplete medical records, or hip fractures sustained from in-hospital falls, those requiring trauma activation in the level I trauma center, and in-hospital deaths were excluded.
Hospital and Admission Settings
This study involved an American College of Surgeons-verified level I adult trauma center with 909 beds and a private university-affiliated teaching community hospital with 484 beds. Although these are from separate hospital systems, a single orthopedic surgery residency program trains in both hospitals, and attending surgeons that are part of the same group practice manage all orthopedic surgery consultations (including all hip fractures). During the study period, neither hospital had an established hip fracture protocol to standardize care such as a consistent admitting service, pain control regimens, and pre-operative clearance testing requirements.
In the trauma center, patients >65 years of age with hip fractures were admitted to one of several medical services. Throughout the study period, a geriatric medical service typically admitted patients, though on occasion, other medical services admitted patients secondary to service volume. Decisions for preoperative workup and risk stratification were made by the admitting medical service. The trauma center also serves as a safety net tertiary referral center and therefore frequently receives patients with low-energy hip fractures from regional facilities. In the community hospital, patients with hip fractures were exclusively admitted to one of several medical services. In a similar fashion, the preoperative workup and decision making were at the discretion of the admitting medical service. The community hospital also frequently receives patients from outlying hospitals without orthopedic surgery coverage or capabilities.
Data Extraction
Two reviewers independently screened the electronic medical records and extracted demographic, presurgery, and in-hospital postsurgery data. The following demographic and comorbidity data were obtained: age, sex, and history of chronic obstructive pulmonary disease (COPD), coronary artery disease (CAD), peripheral vascular disease (PVD), chronic heart failure (CHF), cardiovascular disease (CVD), arterial fibrillation (Afib), valvular heart disease (valvular HD), chronic kidney disease (CKD) with or without dialysis, insulin-dependent diabetes mellitus (IDDM), non-IDDM, or anticoagulation medication, presence of a pacemaker, American Society of Anesthesiologists (ASA) physical status score, and incidence of other fractures. The clinical details that were collected included fracture type (femoral neck or inter/subtrochanteric), type of surgery (hemiarthroplasty, total hip arthroplasty, placement of short intramedullary nail, long intramedullary nail, or sliding hip screw, or percutaneous screw fixation), time to surgery in hours (defined as the time from when the first diagnostic radiograph was taken [or uploaded for transfers] to the time the patient entered the operating room), length of stay in days from admission time to discharge after surgery, activation of cardiology consultation, indication for consult, preoperative transthoracic echocardiography use, and discharge disposition. Mortality data were obtained from a commercially available obituary database (https://www.obituarydata.com). If a notification of death was not obtained from the electronic medical record or obituary database, the patient was assumed to be alive, as done in a previous publication. 21
Outcome Measures
The primary outcome measure was time to surgical treatment. The secondary outcomes were 30-day, 90-day, and 1-year mortality rates.
Statistical Analysis
Data were assessed by per-protocol analyses. The normality of data for the main outcome variable (time to surgery in hours) was assessed using the Shapiro–Wilk test. For comparisons of data that were not normally distributed, the Mann–Whitney U was used. Binary and categorical data were compared with χ2 tests or Fisher’s exact test. Data for the time to surgery were binary: 1, less than 48 hours; 2, greater than 48 hours. The 30-day, 90-day, and 1-year mortality rates were calculated by dividing the number of recorded deaths at each time point by the sample size. Patient demographics, comorbidities, clinical characteristics, and outcomes are presented as univariate statistics. The independent odds ratio (OR) for a delay to surgery of greater than 48 hours was calculated with 95% confidence intervals (CIs). A Kaplan–Meier curve was created for data up to 1-year from the time of the surgical treatment, and survival of patients with delays of surgery of less than 48 hours and greater than 48 hours were compared with a log-rank test. A Cox proportional hazards regression was used to compare time to surgery as a continuous variable to 1-year mortality. Indications for cardiology consults were compared between those who had a history of cardiac comorbidity and those who had acute changes or distress at the time of surgery (eg, active chest pain, recent syncope, changes in electrocardiogram or laboratory tests, or unknown murmur). To identify independent risk factors for poor outcomes, the ORs for 1-year mortality were calculated for each demographic and clinical characteristic. A P value of < .05 was considered significant, and statistical analyses were performed using SPSS, version 28.
Results
Patient Characteristics
Clinical and Surgery Characteristics and Outcomes.

Afib, arterial fibrillation; ASA, American Society of Anesthesiologists; CAD, coronary artery disease; CHF, chronic heart failure; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CVD, cardiovascular disease; HD, heart disease; IDDM, insulin-dependent diabetes mellitus; PVD, peripheral vascular disease.
Sample demographics stratified by hospital setting are presented in Table S1 in Supplemental Digital Content 1. Patients in the community hospital had significantly higher incidences of some cardiovascular comorbidities (P < .05) and had more severe presentation based on preoperative ASA physical status score (P = .001); however, there were no differences in 30-day, 90-day, or 1-year mortality among patients in the 2 hospitals.
Risk Factors
Independent Risk Factors for a Time to Surgery of >48 h.

Afib, arterial fibrillation; ASA, American Society of Anesthesiologists; CAD, coronary artery disease; CHF, chronic heart failure; CI, confidence interval; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CVD, cardiovascular disease; HD, heart disease; IDDM, insulin-dependent diabetes mellitus; OR, odds ratio; PVD, peripheral vascular disease.
Note: Values in boldface font were statistically significant.
Table S2 in Supplemental Digital Content 2 presents the independent risk factors for greater than 48 hours to surgery stratified by hospital type. The analysis showed that, except for history of CAD and having a cardiology consult, no other cardiovascular comorbidities were associated with delays to surgery in both hospital settings.
Indications for Cardiology Consult.

Characteristics of Individuals With Indications for Cardiology Consult.
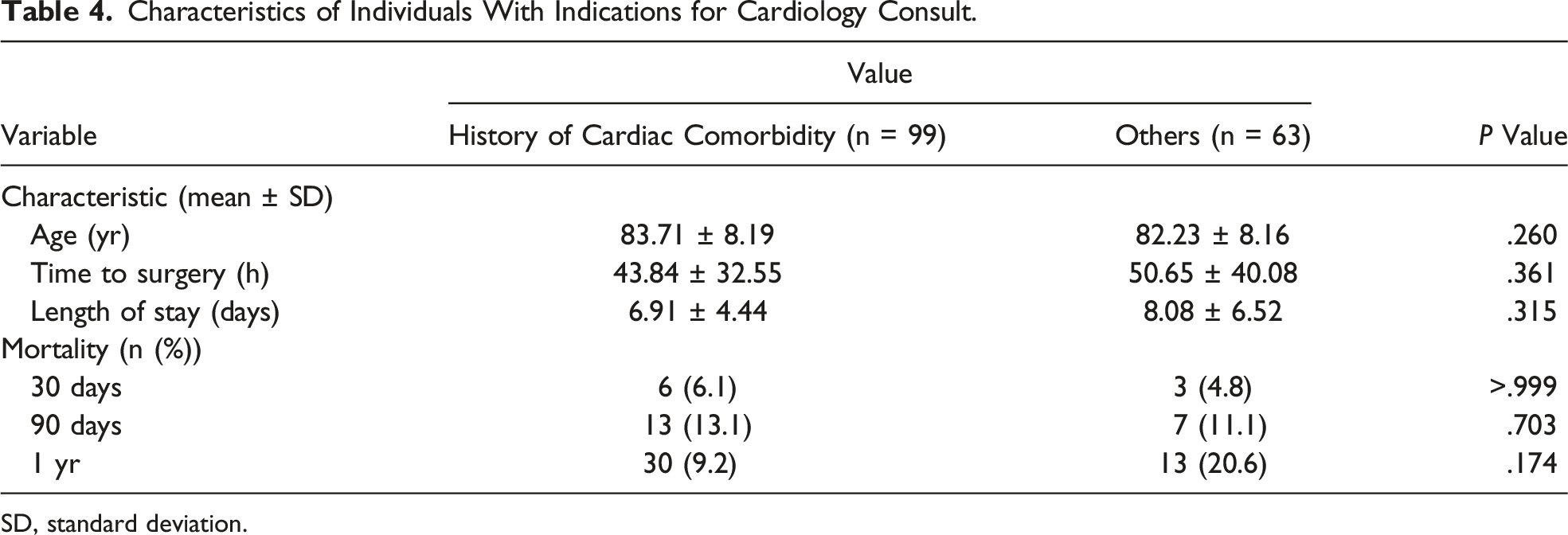
SD, standard deviation.
Mortality
The Kaplan–Meier curve in Figure 1 shows that survival up to 1 year did not differ between patients that underwent timely surgery (less than 48 hours) and those that underwent delayed surgery (greater than 48 hours). A Cox proportional hazard regression model revealed a minimal effect of longer time to surgery in hours as a continuous variable on 1-year mortality (hazard ratio, 1.007; 95% CI, 1.003-1.011; P = .001). Kaplan–Meier survival curve comparing 1-year mortality between patients with a time to surgery of less than or greater than 48 hours.
Independent Risk Factors for 1-Year Mortality.

Afib, arterial fibrillation; ASA, American Society of Anesthesiologists; CAD, coronary artery disease; CHF, chronic heart failure; CI, confidence interval; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CVD, cardiovascular disease; HD, heart disease; IDDM, insulin-dependent diabetes mellitus; OR, odds ratio; PVD, peripheral vascular disease.
Note: Values in boldface font were statistically significant.
Discussion
Our study found several factors associated with a time to surgery beyond 48 hours, including the need for a cardiology consultation and having a cardiac comorbidity, additional fracture, or an ASA score of 3 or 4. Female sex and treatment at the trauma center were associated with a lower risk that surgery would be delayed more than 48 hours. These findings are consistent with those from a previous study. 17 Notably, the risk of cardiology consultation delaying surgery was roughly 3-fold higher than the risk from any other factor, suggesting that the delay is the result of waiting for the consultation or advanced imaging/testing rather than the presence of a cardiac comorbidity.
Upon review of the indications to obtain both cardiology consultations and preoperative transthoracic echocardiography, we found a substantially higher number of consultations and studies were performed outside of the American Heart Association/American College of Cardiology recommendations; 18 61% (99/162) of patients received a cardiology consultation for a prior history of cardiovascular disease without an acute issue, which does not meet the current guidelines for a consultation. This finding is in line with that reported by Hoehmann et al 19 in a retrospective review of a cohort less than half of this study. In a review of 266 patients, Stitgen et al also found appropriate use of cardiology consultations in only 16 of 55 patient with significant delays to surgery and longer length of stay in patients receiving a consultation. 11 Furthermore, Smeets et al 6 reported an inappropriate preoperative screening rate as high as 13%, with 90% of these cases attributed to over screening. The true benefit of these preoperative services is difficult to assess. However, none of the patients in our study underwent a major preoperative intervention such as cardiac catheterization or pacemaker implantation.
We did not observe an association between time to surgery and mortality at any time point in our study. Previous studies have found varied results, ranging from no association to significant associations of delayed surgery and mortality at 30 days up to 1 year after the procedure.22-25 In a systematic review and metanalysis by Klestil et al, they found a 20% decreased risk in 1 year mortality in patients operated on before 48 hours, but no difference at 24 hours. 26 Bohm et al conducted a review of over 6000 patients within a healthcare system before and after implementation of a protocol to, among other things, improve time to surgery to within 48 hours. 9 1-year mortality rates were not statistically different between the pre and post intervention groups, however, when looking at the group as a whole having time to surgery within 48 hours showed decreased risk of in hospital and 1-year mortality. The HIP ATTACK investigators previously published results of a randomized controlled trial allocating patients to an accelerated treatment group (surgery within 6 hours) vs standard treatment. 27 Median time to surgery in each group was 6 and 24 hours, respectively. When comparing nearly 1500 patients in each group, they could not demonstrate a significant difference in mortality or complications between groups. The variable results of these studies demonstrate that the true effect of time to surgery has been challenging to study. Although confounding variables may be controlled for, significant bias may still exist. The consideration that patients receiving delayed surgery due to further investigation of pre-existing illness contributing to higher mortality rates is difficult to control for. Another consideration for the generalizability of the previously mentioned studies are the inclusion of younger patients (less than 65 years old) which likely does not represent a geriatric population. The aforementioned non-mortality related complications seem to be fairly consistent with delays greater than 48 hours, posing a significant burden to both the patient and the healthcare system, and we believe it is still in the best interest of the patient to have treatment in a timely fashion regardless of effect on mortality.
There are several limitations to this study. This was a retrospective study and therefore precluded us from showing causality. The time to surgery was based on the time from the initial diagnostic radiograph until the time a patient entered the operating room. Although these time points were reliably recorded for every patient, they do not represent the time from fracture. Time from fracture is an important variable but often unknown, because it is reliant on an accurate report from the patient. We believe our technique of deciding time to surgery does provide an accurate assessment of time to surgery. Utilizing this method, we also had complete data for all patients, as opposed to the previously mentioned study by Bohm et al with nearly 25% of patients included with missing time to surgery data. 9 Another limitation is mortality data was obtained from a combination of medical record reviews and an obituary database. These data may not be as accurate as those from a national registry; however, a more reliable source for this information was not available. Nevertheless, the 30-day and 1-year mortality rate for the patients in this study is similar to other published mortality rates, suggesting that this technique is reliable.25,28
In conclusion, our study indicates that preoperative cardiology consultations are associated with delays to surgery for hip fractures in patients older than 65 years in a relatively large sample size between 2 hospitals in the same city. These data add to the growing amount of evidence against injudicious use of transthoracic echocardiography and cardiology consultations for patients that have no definitive indications. These results have prompted collaborations between cardiology and internal medicine colleagues and the development of more strict criteria to order these services in the preoperative setting for these patients at our centers. Our current indications for pre-operative cardiology consultations include a myocardial infarction within 30 days from injury, unstable or severe angina, decompensated heart failure, severe valvular disease, and recent coronary artery stenting within 6 weeks.
Supplemental Material
Supplemental Material - Delay to Surgical Treatment in Geriatric Hip Fracture Patients
Supplemental Material for Delay to Surgical Treatment in Geriatric Hip Fracture Patients by Elias G. Joseph, MD, Jordan Serotte, MD, Mohammad N. Haider, MD, PhD, Sonja Pavlesen MD, MS, and Mark Anders MD in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Author’s Note
Work performed at: The Department of Orthopaedic Surgery, University at Buffalo, Jacobs School of Medicine and Biomedical Sciences, State University of New York at Buffalo, Buffalo, NY.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.