
Abstract
Introduction
Osteoporosis can affect the surgical outcomes of proximal humeral fractures in older people. Recently, the cortical bone thickness of the proximal humerus on plain radiograph has been proposed to reflect local osteoporosis of the proximal humerus; however, its effect on the surgical outcome of proximal humeral fractures remains unclear. The purpose of this study is to investigate the influence of cortical bone thickness on postoperative radiographic outcomes after osteosynthesis for proximal humeral fractures.
Materials and Methods
We retrospectively identified 190 patients (≥50 years) who underwent osteosynthesis with an intramedullary nail or plate for proximal humeral fractures. The patients were categorized into 2 groups according to the cut-off value of an average proximal humerus cortical bone thickness of 6 mm on plain radiographs: patients with and without local osteoporosis. After propensity score matching, we compared the incidence of postoperative radiographic complications between the 2 groups. We also performed subgroup analyses of outcomes in a subgroup of patients who underwent intramedullary nailing and those who underwent plate fixation.
Results
Propensity score matching yielded 60 patients in each group. No significant difference in complication rates was observed between the 2 groups. However, in the intramedullary nailing subgroup, the incidence of reduction loss was significantly higher in patients with local osteoporosis than in those without local osteoporosis (51.7% vs 14.3%, P = .002).
Discussion
The proximal humeral cortical bone thickness had no significant effect on the overall radiographic outcome; however, reduction loss after intramedullary nailing was susceptible to local osteoporosis of the proximal humerus.
Conclusion
Our study suggests that plate fixation is advantageous in preventing postoperative reduction loss in patients with lower cortical bone thickness.
Introduction
Proximal humeral fractures are common, particularly in older patients with osteopenia or osteoporosis. 1 However, surgical treatment of proximal humeral fractures in osteoporotic bones remains challenging. Several studies have shown an association between decreased bone mineral density (BMD) and mechanical failure after osteosynthesis of proximal humeral fractures.2-4 Since reduction loss and screw cut-out are the most common reasons for revision surgery, 5 osteoporosis can be 1 of the factors negatively affecting the postoperative outcome of proximal humeral fractures; therefore, preoperative evaluation is important.
Currently, dual-energy X-ray absorptiometry (DXA) is the gold standard for BMD evaluation; however, clinically, DXA is not always available in acute settings or is inaccessible in many parts of the world. 6 Recently, to address this issue, the cortical bone thickness of the proximal humerus has been proposed as an index to reflect local osteoporosis of the proximal humerus. Proximal humeral cortical bone thickness has been reported to correlate not only with BMD of the humerus, but also with that of the lumbar spine and the proximal femur.7-9 However, the influence of cortical bone thickness on the postoperative outcomes of proximal humeral fractures remains largely unknown.
This study aimed to investigate the influence of proximal humeral cortical bone thickness on radiographic outcomes after osteosynthesis of proximal humeral fractures.
Methods
This study was approved by the Independent Ethics Committee of our hospitals.
Study Design and Patients
This was a retrospective study of patients who underwent osteosynthesis for proximal humerus fractures between January 2008 and December 2019 at 3 general hospitals. We included patients (≥50 years) who underwent osteosynthesis using an intramedullary nail or plate for proximal humerus fractures during this period and had a 1-year postoperative follow-up. The exclusion criteria were pathological fracture, open fracture, multiple injuries, isolated greater tuberosity fracture, isolated lesser tuberosity fracture, head-split fracture, fractures extending to the metaphysis, and previous surgery on the involved shoulder.
Radiographic Evaluation of the Proximal Humeral Cortical Bone Thickness
Mather et al proposed an evaluation to measure the average proximal humeral cortical bone thickness at 2 levels separated by 2 cm on plain radiographs (Figure 1) and reported that an average proximal humerus cortical thickness of 6 mm could be a potential threshold value for predicting local osteoporosis.
8
We adopted this measurement in this study since it reportedly has excellent inter- and intra-observer reliability.8,9 A single examiner evaluated the preoperative anteroposterior view of each shoulder radiograph. The patients were divided into 2 groups: patients with cortical bone thickness ≥6 mm (the local osteoporosis (–) group) and patients with cortical bone thickness ˂ 6 mm (the local osteoporosis (+) group). Radiographic assessment of proximal humeral cortical bone thickness. On an anteroposterior view of the shoulder radiograph, the cortical bone thickness of the proximal humerus was measured at 2 levels separated by 2 cm. In this study, we defined the average cortical bone thickness <6 mm as local osteoporosis.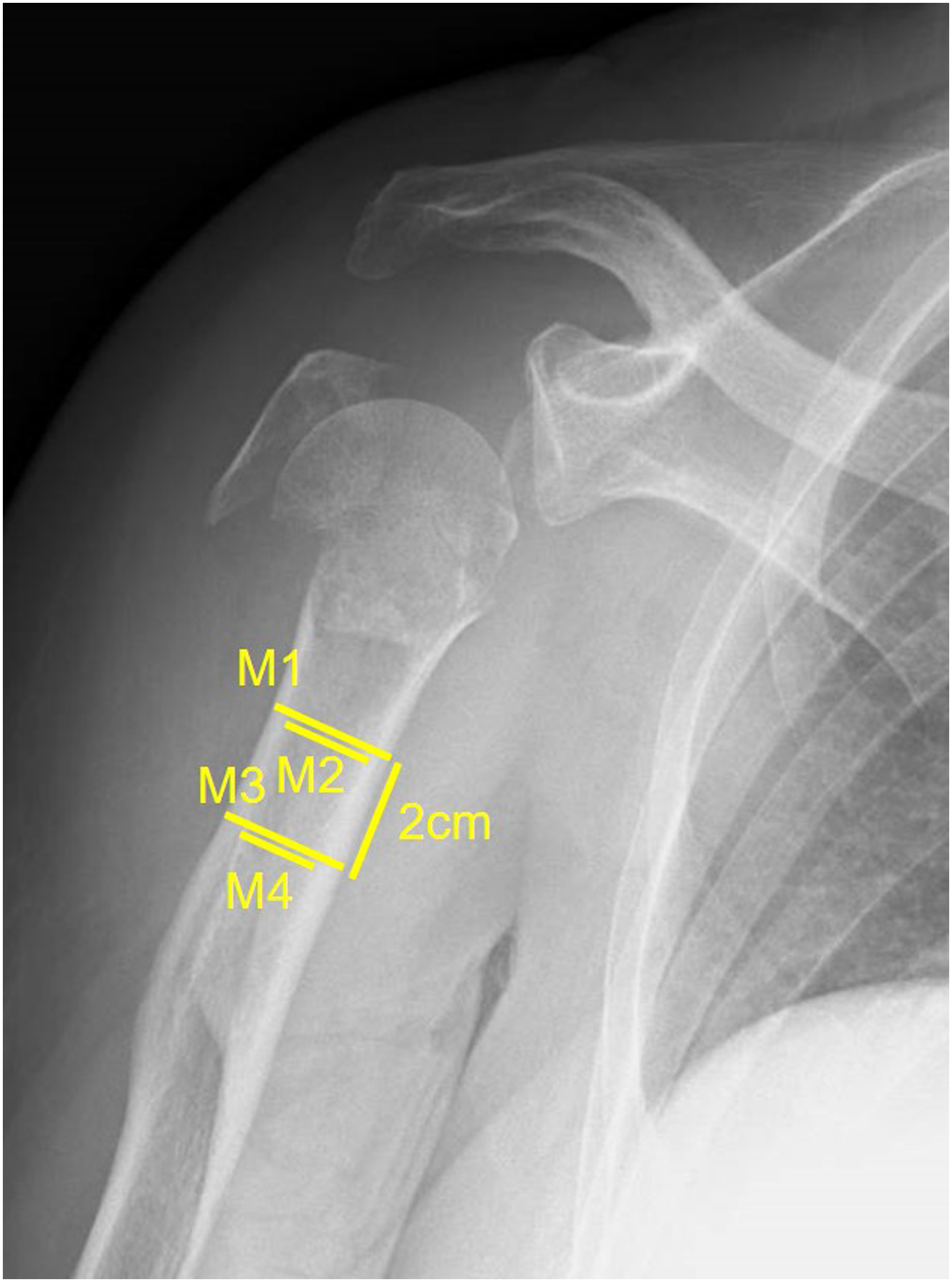
Propensity Score Matching
Due to the absence of randomization, there were confounding factors and internal variability between these 2 groups. We performed logistic regression-based propensity score matching for all patients that met the study inclusion and exclusion criteria to minimize potential selection bias. Potential confounding factors (age, sex, side of injury, smoking history, body mass index, preoperative nerve injury, time from injury to surgery, type of fractures, surgical approach, and implant used for surgery) were matched. We performed matching using a 1:1 matching protocol (nearest-matching algorithm), with caliper width equal to .25 of the standard deviation of the logit of the propensity score.
Surgical Procedure
The surgical procedures were performed by 11 orthopedic surgeons. In all cases, the surgery was performed in the beach-chair position under general anesthesia. Intramedullary nail fixation was performed using the MultiLoc® humeral nail (DePuy Synethes, Oberdorf, Switzerland), Polarus 2 humeral nail (Acumed, Hillsboro, OR, USA), T2 humeral nail (Stryker, Kalamazoo, MI, USA), and ARISTO® humeral nail (MDM, Tokyo, Japan). Plate fixation was performed using a PHILOS® plate (DePuy Synethes, Oberdorf, Switzerland), an NCB® proximal humerus plate (Zimmer Biomet, Warsaw, IN, USA), and a MODE® proximal humeral plate (MDM, Tokyo, Japan). In all cases where intramedullary nails were inserted, we measured the width of the medullary canal from the preoperative computed tomography and selected their size accordingly. We did not perform the reaming to avoid iatrogenic fracture or neurovascular injury. The reduction suture applied to the rotator cuff was finally fastened to the suture hole of the plate or the screw head of the intramedullary nail at the surgeon’s discretion. We did not perform any procedures such as bony allograft augmentation, screw cement augmentation, or additional calcar screws in this study. The SB VACTM (Sumitomo Bakelite, Tokyo, Japan) was inserted and drained at the fracture site within 2 days postoperatively at the surgeon’s discretion. Immobilization was achieved by fixation using a sling for 1-2 weeks, during which passive range of motion (ROM) training was started, and active ROM training was started at 4-6 weeks postoperatively.
Outcome Measures
Postoperative outcomes included the incidence of complications (delayed bone union, nonunion, screw cut-out, avascular necrosis, malreduction, and reduction loss) and ROM (elevation and external rotation (ER) at the side) at 1 year postoperatively. Delayed bone union was defined as a lack of bone bridging at 1 year postoperatively. Malreduction was defined as head-shaft displacement of >5 mm, head-shaft alignment of <110° or >150°, or cranialization of the greater tuberosity on the plain radiographs taken within 1 week postoperatively, according to a previous report. 10 Reduction loss was defined as ≥ 10° of angulation in any direction or fixation failure based within 1 year postoperatively on a previous report. 4 A single examiner, blinded to local osteoporosis results, investigated the postoperative complications based on the clinical notes and plain radiographic images, and the surgeon who performed osteosynthesis or the occupational therapist assessed the ROM using a goniometer at 1 year postoperatively.
We compared the postoperative outcomes between the local osteoporosis (–) and local osteoporosis (+) groups. Subsequently, we performed subgroup analyses of outcomes in a subgroup of patients who underwent intramedullary nailing and those who underwent plate fixation.
Statistical Analysis
All statistical analyses were conducted using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). We compared the average continuous values (age, body mass index, time from injury to surgery, and ROM) using the Mann–Whitney U-test and the proportion of discrete variables (sex, side of injury, smoking, preoperative axillary nerve injury, type of fracture, surgical approach, implant used for osteosynthesis, and postoperative complications) using the chi-square test. Continuous data, including age, body mass index, and the time from injury to surgery, were presented as the mean ± standard deviation. The ROM data were presented as the mean [95% confidence interval]. The threshold for significance was set at P < .05.
Reportedly, the incidence of poor postoperative radiographic outcomes in patients over 50 years of age who underwent osteosynthesis for proximal humerus fractures was 42%; therefore, 11 based on a power analysis assuming a 42% rate of postoperative radiographic complications, approximately 52 patients in each group would be required to show a 25% difference in the incidence of postoperative radiographic complications in this study.
Results
The Demographics of all Patients.

Continuous values are presented as the mean ± standard deviation.
*P < .05.
Patient Demographics in the Matched Cohort.

Continuous values are presented as the mean ± standard deviation.
Comparison of Incidence of Postoperative Complications.

Additionally, no significant difference was observed between the local osteoporosis (−) and local osteoporosis (+) groups in the ROM of elevation (127° [119-136°] vs 121° [111-130°], respectively, P = .378) and ER (46° [42-52°] vs 42° [37-48°], respectively, P = .449) at 1 year postoperatively. Data on ROM were missing for elevation in 18 patients and ER in 55 patients.
Subgroup Analysis of the Incidence of Postoperative Complications in the Intramedullary Nailing Group or Plate Fixation Group.

*P < .05.
Discussion
In this study, we investigated the effect of proximal humeral cortical bone thickness on radiographic outcomes 1 year postoperatively in 120 patients who underwent osteosynthesis of proximal humeral fractures and were enrolled using a propensity score matching. The results of this study showed that cortical bone thickness had no significant effect on the overall radiographic outcome. However, in the group that underwent osteosynthesis using intramedullary nails, reduction loss was significantly more frequent in patients with local osteoporosis.
The only previous study to evaluate the influence of proximal humeral cortical bone thickness on surgical outcomes demonstrated no significant association between cortical bone thickness and radiographic outcome in 48 patients who underwent plate fixation of proximal humeral fractures, 11 which is congruent with the results of this study. In addition, in a previous study, although there were significantly more women and older patients with local osteoporosis, fracture type did not differ significantly between patients with and without local osteoporosis. 11 These findings are consistent with those of this study.
However, subgroup analyses of our study revealed that local osteoporosis had a significant effect on reduction loss only in patients who underwent osteosynthesis using intramedullary nails. To date, the preoperative risk factors affecting reduction failure after osteosynthesis of proximal humeral fractures include older age, displaced varus fractures, medial comminution, and osteoporosis.3,4 Although some studies have shown that local osteoporosis did not significantly affect the frequency of radiological complications after plate fixation,11,13 no clinical studies have evaluated the influence of osteoporosis on postoperative outcomes after intramedullary nailing. A cadaveric study showed no significant association between humeral BMD and failure load of intramedullary nails, 14 which contradicts our study results. This discrepancy can be partly explained by the fact that previous studies used in vitro biomechanical models, which do not fully reflect the complex loading conditions and force generated by various muscles and ligaments attachment in vivo. The reason for the higher frequency of reduction loss in patients who underwent intramedullary nailing for proximal humeral fractures with local osteoporosis remains unclear; however, several hypotheses have been proposed. First, the intramedullary nails used in this study included many second-generation intramedullary nails. One of the disadvantages of these nails is the inadequate safety of proximal interlocking screws. 15 To prevent postoperative reduction failure, some studies have proposed medial calcar fixation support3,4; however, these second-generation nail screws engage only the osteoporotic bone of the proximal humerus, which often results in fixation loss with screw backout. 15 The fixation of these interlocking screws may have been more fragile in the proximal humerus, with severe osteoporotic changes. This could be improved by using third-generation intramedullary nails with a more secure locking mechanism that allows the insertion of more proximal screws in posteromedial regions with good bone quality. Second, in almost all patients who underwent plate fixation, the reduction sutures applied to the rotator cuff tendons were fastened to the suture holes of the plate, whereas in only a few patients who underwent intramedullary nail fixation, the reduction sutures were fastened to the suture holes of the proximal screw heads. This difference may have affected postoperative varus progression of the proximal humerus. Finally, the proximal tip of the intramedullary nail to anchor in the zone of dense subchondral bone is critically important in countering varus displacement force.14,16 In osteoporotic bones, thinned subchondral bone may have weakened fixation by head anchoring. Further studies are needed to clarify the mechanism of the association between local osteoporosis and radiographic outcome after intramedullary nailing. Our study suggests that plate fixation is advantageous in preventing postoperative reduction loss in patients with lower cortical bone thickness.
However, this study has several limitations. First, the propensity score matching was performed to adjust unbalanced baseline factors; however, due to difficulties in assessing and balancing all possible factors affecting the outcome, overlooked residual, unmeasured confounders may also have played a role in the difference between the groups. For example, the surgery was performed by 11 orthopedic surgeons; however, we did not investigate the effects of the skills of these surgeons and their assistants. Moreover, the choice of implants and surgical procedures should be consistent based on the fracture type. The fact that the choice of implants depended on each surgeon’s preference could be a limitation of this study. Second, this study did not include functional outcome using a questionnaire; therefore, we could not assess the association between local osteoporosis and functional outcome. Third, although propensity score matching reduced the possibility of substantial confounding, this procedure restricted the sample size of our study, potentially limiting our power to precisely evaluate the effects.
Conclusions
This study provides new information on the effect of local osteoporosis of the proximal humerus on the postoperative outcomes of osteosynthesis for proximal humeral fractures. The proximal humeral cortical bone thickness had no significant effect on the overall radiographic outcome; however, reduction loss after intramedullary nailing was susceptible to local osteoporosis of the proximal humerus.
Supplemental Material
Supplemental Material - Influence of Proximal Humeral Cortical Bone Thickness on the Radiographic Outcome After Osteosynthesis of Proximal Humeral Fractures: Propensity Matching Score Analysis
Supplemental Material for Influence of Proximal Humeral Cortical Bone Thickness on the Radiographic Outcome After Osteosynthesis of Proximal Humeral Fractures: Propensity Matching Score Analysis by Ryogo Furuhata, MD, Atsushi Tanji, MD, Satoshi Oki, MD, and Yusaku Kamata, MD in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Author Contributions
All authors contributed to the conception and design of the study. The study design was planned by RF and AT. Material preparation, data collection, and analysis were performed by RF, SO, and YK. The first draft of the manuscript was written by the RF. AT, SO, and YK contributed to previous versions of the manuscript. All authors have read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors certify that they or their institutions did not receive any support (eg, grants, funding, payment, or other benefits) or a commitment or agreement to provide such benefits in connection with the research or preparation of this manuscript. The authors also did not receive any funding for the study design, collection, analysis, and interpretation of data and for writing the manuscript.
Consent to Participate
Owing to the retrospective nature of the study, consent was obtained using the opt-out method for each patient on our hospital bulletin board and website. Opt-out consent relies on implicit consent, where willingness to participate is tacit or presumed and can be retracted by active objections.
Ethical Statement
Data Availability Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.