
Abstract
Introduction
Ankle fractures in geriatric patients can be devastating injuries, as they limit an individual’s mobility, autonomy, and quality of life. This study examines the functional outcomes and complications related to hindfoot nails (HFN) in geriatric patients who have suffered an ankle malleolar or distal tibia fracture.
Materials and Methods
This is a single-surgeon case-series of patients who underwent HFN for acute fixation or delayed reconstruction after an ankle or distal tibia fracture. Demographic information, comorbidities, baseline functional status, AO/OTA classification, surgical indications, need for external fixation, total operative time, length of stay (LOS), ambulation at discharge, and discharge disposition were recorded. Primary outcomes included 30-day complications, ambulation at follow-up, and time to fracture union and fusion.
Results
There were 22 patients, with average age 80.8 years. Mean LOS was 7.0 days, and 68.2% were discharged to subacute rehabilitation. Within 30 days, 1 patient developed a deep vein thrombosis and bilateral pulmonary emboli, and 2 experienced wound dehiscence requiring antibiotics. At 6-weeks, 1 patient sustained a fall with periprosthetic fracture requiring HFN revision, and another developed cellulitis necessitating hardware removal. Fracture healing was seen in 72.7% at 19.4 weeks, while radiographic fusion occurred in 18.2% at 43.0 weeks. 72.7% were ambulating with an assistive device at discharge, and 100.0% at 12-weeks post-operatively or last follow-up. Upon final examination, all patients were ambulating without pain.
Discussion
HFNs provide a reliable alternative to traditional open reduction internal fixation and have the ability to improve quality of life for geriatric patients through a faster return to weight-bearing. Additionally, radiographic fusion rates show that patients have favorable functional outcomes even without formal arthrodesis.
Conclusion
HFN is beneficial for elderly patients with low functional demand and complex medical comorbidities, as it allows for early mobility after sustaining an ankle or distal tibia fracture.
Introduction
Ankle fractures are the third most common musculoskeletal injury in the growing elderly population. 1 Depending on the characteristics of the fracture itself and the patient’s goals for recovery, there are multiple approaches for addressing ankle fractures in the geriatric population. In patients with an unstable, displaced fracture, open reduction internal fixation (ORIF) remains the standard of care. 2 Though it does delay return to weight bearing by up to 12 weeks, ORIF allows many patients to achieve near-baseline levels of activity, while limiting the development of posttraumatic osteoarthritis.3–5 Still, this injury can have a devastating impact on senior patients, as it limits their ability to independently perform activities of daily living and has been associated with 1-year mortality rates as high as 12%. 1 Some of the morbidity and mortality may be due to prescribed, prolonged non-weight-bearing to the affected limb after ORIF.6,7 Studies have shown that patients older than 65 years are only compliant with non-weight-bearing restrictions 22% of the time. 8 Noncompliance can lead to prolonged bed rest and complications from immobility or failure of fixation and fracture displacement. 8 Given the reduction in quality of life and potential for serious morbidity, effectively treating ankle fragility fractures is crucial.
Recently, there has been momentum in the orthopaedic community to develop techniques and protocols that allow for immediate weight-bearing as tolerated.6,7 Augmented ORIF and hindfoot nailing (HFN) have been proposed as alternatives that may permit earlier weight-bearing in the geriatric ankle fracture population.2,7 HFN has been shown to provide more stability in those with poor bone quality and allow for immediate weight-bearing, but at the expense of ankle and subtalar motion.9,10 It has also been associated with shorter hospital stays. 6 For these reasons, HFN has been explored as an alternative for acute and delayed reconstruction of ankle and distal tibia fractures. 6 Al-Nammari et al 11 reported that in their cohort of 48 elderly patients treated with HFN, 90% returned to their pre-injury level of function. Similarly, based on their randomized controlled trial, Georgiannos et al 6 concluded that there was no difference in rate of return to baseline functionality between those treated with HFN vs ORIF. Additional studies have demonstrated complication rates of HFN that are comparable to other ankle fracture fixation methods. 2 However, there is still a paucity of studies addressing the utility and safety of HFN in elderly patients, and consequently, the optimal management of fragility ankle fractures remains controversial.
Given the lack of consensus within the orthopaedic surgery community on when and in which patients to use HFN for definitive fixation of ankle and distal tibia fractures, each study contributes much-needed evidence to the question at hand. 3 Through this case series, we aim to determine whether hindfoot nails without open subtalar and tibiotalar joint preparation reliably achieve favorable outcomes, with minimal complications, in geriatric patients who have suffered an ankle malleolar or distal tibia fracture.
Materials and Methods
This study is a case-series of patients who underwent HFN as definitive treatment for fractures of the ankle or distal tibia. All procedures were performed as inpatient surgeries by a single trauma-trained orthopaedic surgeon between April 2020 and December 2021. Each patient received a Stryker T2™ Ankle Arthrodesis Nail (Kalamazoo, MI, USA), implanted with the assistance of intraoperative fluoroscopy and without a separate procedure to prepare the tibiotalar and subtalar joints. The procedure was the same for fixation of acute fractures and delayed reconstructions, as shown in Figure 1 and Figure 2. HFN was performed with the patient lying supine on a regular operating room (OR) table. The patient was positioned with the legs off the bottom of the table, from mid-calf. An intraoperative positioner (Bone Foam® Leg Ramp, Bone Foam, Corcoran, MN, USA) was used to ensure proper leg position and adequate access during placement of the nail. When removal of prior hardware was not needed, the surgery was performed in a minimally invasive, percutaneous fashion. Directly following surgery, patients were made weight-bearing as tolerated in a controlled ankle motion (CAM) boot and instructed to follow up in clinic 2 weeks post-operatively. Once the incisions healed (14-21 days), the patients were allowed to wean themselves from the boot to regular sneakers. Physical therapy was provided for patients who could not be weaned from the boot by 12 weeks post-operatively or by patient request. 97-year old female with a left trimalleolar fracture/dislocation (image A) was treated with a hindfoot nail (images B, C) at 6 weeks post-operatively. 81-year old male with a right, open peri-implant distal tibia and fibula fracture underwent ORIF (image A), which was complicated by infected nonunion. He was treated with removal of hardware, temporary external fixation, and definitive fixation with a hindfoot nail (images B, C) at 6 weeks post-operatively.

In January 2022, we used the database of a single surgeon, practicing at a private health system in New York, and identified 22 patients who had undergone the above procedure. The electronic medical record was used to perform a retrospective chart review of relevant data. This included demographic and comorbidity information such as age, sex, Charlson Comorbidity Index (CCI), American Society of Anesthesiologist (ASA) class, and baseline level of mobility.12,13 Data regarding the fracture itself included the AO/OTA classification, indications for surgery, and the need for external fixation prior to definitive treatment. 14
Outcomes to characterize the patient’s hospital stay included length of stay (LOS), length of operation, ambulation at discharge, and discharge disposition. Complications were collected for 30 days postoperatively and for the duration of the patient’s follow up. These included deep vein thrombosis (DVT), pulmonary embolism (PE), pneumonia, myocardial infarction, infection, hardware failure, and death. Our long-term outcomes included ambulation status and use of mobility aids at each follow-up visit, time to fracture union, and time to fusion. Office radiographs were used to assess union and fusion. Microsoft Excel was used for both data organization and statistical analysis.
Baseline Patient Characteristics.

Fracture Classification and Indications for Operative Intervention. a

aBased on the Orthopaedic Trauma Association Fracture Classification.
Results
Hospital Stay Characteristics.
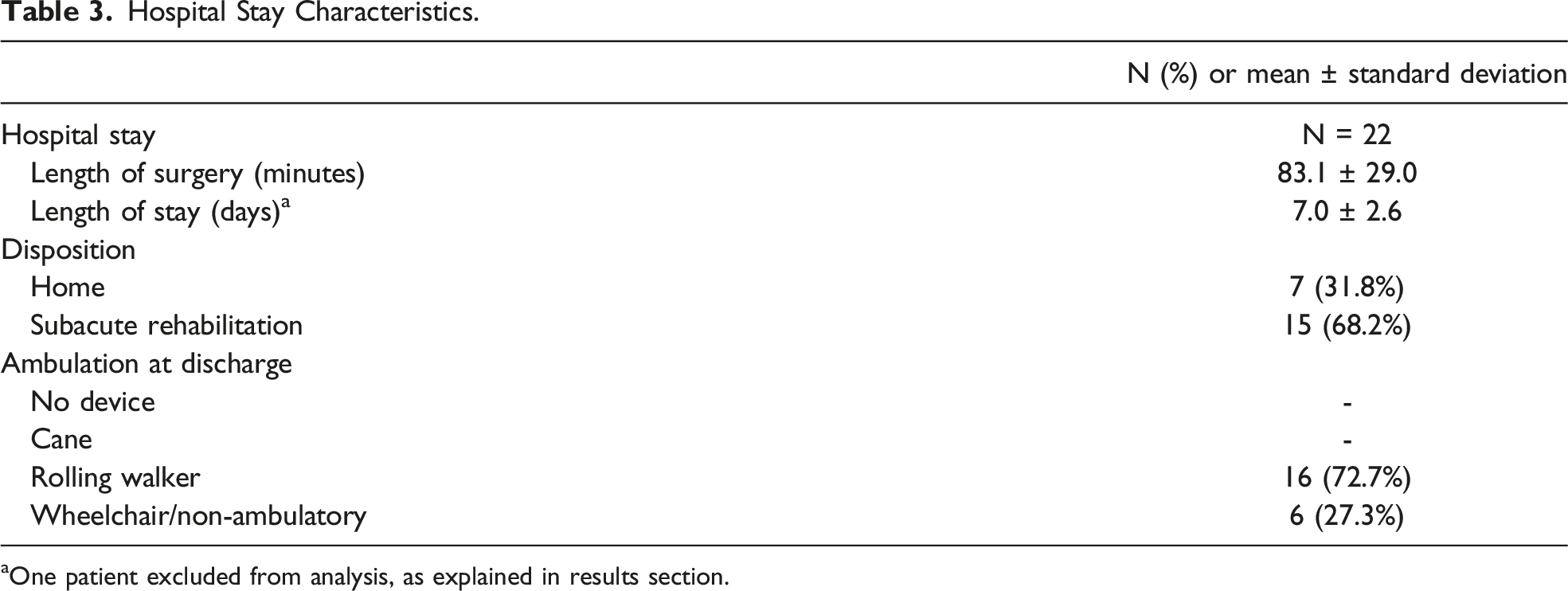
aOne patient excluded from analysis, as explained in results section.
The average LOS was 7.0 days (range 2-12 days), excluding 1 patient with a 44-day LOS (Table 3). This patient sustained an open, peri-implant distal tibia fracture around a bimalleolar ankle fracture ORIF, complicated by infected nonunion. The patient presented in septic shock and underwent removal of hardware and HFN. The postoperative course was complicated by COVID-19 infection with bilateral PE's, eventually necessitating placement of an inferior vena cava filter. Upon discharge, 31.8% of patients were sent home, while 68.2% were discharged to a subacute rehabilitation facility (Table 3).
Post-Operative Outcomes.

Complete fracture healing was seen in 16 patients at an average time of 19.4 weeks (Table 4). The 5 fractures that did not achieve radiographic union during the study period presented for fewer than 10 weeks of follow-up. Four of these 5 patients had transsyndesmotic bimalleolar fracture equivalents. All patients who presented for follow-up were ambulating without pain upon final examination (Table 4). Radiographic evidence of both tibiotalar and subtalar fusion was seen at a mean of 43.0 weeks in 4 patients (Table 4). Zero patients demonstrated fusion of the tibiotalar or subtalar joints in isolation.
Prior to surgery, 40.9% of patients ambulated without assistive devices (Table 1). At the time of hospital discharge, 16 (72.7%) patients were able to ambulate with use of a walker. At 2-week follow-up, 18 of 21 patients were ambulatory with either a cane or walker. All patients who presented for follow-up were ambulatory by 6 weeks postoperatively (Table 4). At the time of latest follow up, all patients remained ambulatory, though all required some form of assistive device.
Discussion
As patients are living longer with more medical comorbidities, it is important for the management of fractures to evolve in a way that maximizes quality of life. This case series demonstrates that hindfoot nails are an effective tool to treat ankle and distal tibia fractures in geriatric patients who have multiple medical comorbidities and are consequently at increased risk for perioperative complications.3,6 Of the 22 patients treated with HFN, the majority were indicated for acute closed bi- and trimalleolar fractures of the ankle. This finding is consistent with other literature demonstrating that in geriatric patients, unstable ankle fractures are the typical indication for surgical reduction and fixation with a hindfoot nail.6,15
Functional outcomes in the inpatient and outpatient setting demonstrated both benefits and challenges resulting from HFN. In our cohort, 68.2% of patients were discharged to a subacute rehabilitation facility. This is comparable to a recent review of Medicare data which found that 59.2% of geriatric ankle fractures were discharged to a nursing facility. 16 After surgery, patients were immediately able to bear weight as tolerated in a CAM boot, and at discharge, 72.7% were able to walk with a rolling walker. By their 2-week follow-up, 81.8% of patients were ambulatory. The ability to immediately resume weight-bearing after HFN is critical for geriatric patients, as early mobilization has been associated with improvement in quality of life and functionality following ankle fracture. 17 In already frail patients, this also reduces the risk of muscle atrophy, which can develop with just a few weeks of disuse. 17 Of the patients who did not demonstrate radiographic fracture healing, all were ambulating without pain. It is likely that fibrous union, along with the stability afforded by the load-sharing hindfoot nail, is sufficient to produce satisfactory results in this low-demand population.
While there was no formal open or arthroscopic cartilage resection to facilitate fusion, 4 patients demonstrated fusion of their subtalar and tibiotalar joints. One of the criticisms of HFN for geriatric fractures is that, typically, no formal arthrodesis is performed. However, studies have shown that for low-demand elderly patients, fusion is not required for good outcomes.18,19 Only one patient required removal of hardware for screw loosening, indicating that even without arthrodesis, these patients were able to achieve a stable construct sufficient for their activities of daily living.
Lastly, in concordance with other similar studies, 13.6% of our patients experienced complications within 30 days post-surgery. 3 Elmajee et al. 3 reported that based on a systematic review comprised of 7 studies, with 194 patients undergoing HFN, the overall complication rate was 16.5%, of which the most common adverse events were nail or screw breakage, return to the OR, and infection. Consistent with these results, infection requiring antibiotics, without operative intervention, was the most common complication in our series. While there is further work to be done in mitigating these negative outcomes, the complication rates seen with HFN may be lower than that of ORIF, which are reportedly as high as 36%.6,20
These findings should be interpreted in light of the limitations inherent to a retrospective case series, namely selection and recall bias. Data extraction is limited by the information documented in the medical record at the time of patient care. Follow-up times varied greatly—ranging from 2.7 to 80.1 weeks—which limits our ability to comment on long-term complications for many patients. All surgeries in this case series were performed by a single surgeon to highlight a specific surgical technique; however, this can inhibit generalizability of findings to a broader population. HFN is also a procedure with rather narrow indications, leading to a small cohort of patients available for analysis and a limited capacity to detect complications which occur at lower rates.
Conclusion
For geriatric patients with low functional demand and complex medical comorbidities, the hindfoot nail provides a reliable means of fixation for ankle and distal tibia fractures that otherwise would have been treated with an extended period of non-weight-bearing. Patients have good functional outcomes even without formal arthrodesis. Larger prospective studies with a control group are needed to determine the most relevant factors in predicting which geriatric ankle fractures would benefit from a hindfoot nail, rather than traditional ORIF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.