
Abstract
Background
Total joint arthroplasties are among the most common surgical procedures performed in the United States. Although numerous safeguards are in place to optimize patient health and safety pre-, intra-, and postoperatively, patient frailty is often incompletely assessed or not assessed at all. Frailty has been shown to increase rates of adverse events and length of stay. We discuss the impact of frailty on patient outcomes and healthcare economics as well as provide widely accepted models to assess frailty and their optimal usage.
Methods
Several databases were searched using the keywords “frailty,” “TJA,” “THA,” “frailty index,” “frailty assessment,” and “frailty risk.” A total of 45 articles were used in this literature review.
Results
It is estimated that nearly half of patients over the age of 85 meet criteria for frailty. Frailty in surgical patients has been shown to increase total costs as well as length of stay. Additionally, increased rates of numerous adverse events are associated with increased frailty.
Conclusions
The literature demonstrates that frailty poses increased risk of adverse events, increased length of stay, and increased cost. There are several models that accurately assess frailty and can feasibly be implemented into preoperative screening.
Introduction
Total joint arthroplasties (TJA) are among the most common surgical procedures performed in the United States, with the volume of procedures steadily increasing over recent years. 1 Over 250,000 total hip arthroplasties (THA) are performed annually, with a projected growth of 71% to 635,000 procedures annually by 2030. 1 Although numerous steps are taken pre-, peri-, and post-operatively to ensure patient safety and optimal outcomes, patient frailty is often not assessed properly or not assessed at all. This plays an important role in the setting of TJA, as these patients are typically older in age. Frailty places patients at risk of adverse events due to minor stressors, thus posing a drastic risk in major surgery.2,3 In the setting of THA, Schmucker et al found postoperative acute myocardial infraction, pneumonia, and sepsis/septicemia/shock to be associated with increased frailty (95% CI, .638-.677). Surgical site bleeding and pulmonary embolism had similar association (95% CI, .537-.616). 4 Serious adverse events increase healthcare costs and utilization due to increased lengths of stay, readmissions, and transfers to intensive care. Examining over 3.5 million Medicare patients, Simpson et al. found the mean cost in a 9-month follow-up period for a frail, pre-frail, and robust patients were $25,320, $16,305, and $8,099, respectively. 5 Hence, the complications associated with frailty tend to increase the cost of care for frail patients.
Methods
PubMed and GoogleScholar were searched using the keywords “frailty,” “TJA,” “THA,” “frailty index,” “frailty assessment,” and “frailty risk.” Only studies published in English were included. Abstracts were screened for suitability, defined as either addressing the concept of frailty, frailty in the setting of total joint arthroplasty, or economic impact of frailty among surgical patients. Full text articles were then screened and reference matching was conducted, resulting in a total of 45 articles included in this literature review.
Discussion
Definition of Frailty
The concept of frailty is generally associated with older age, but the definition itself is more complicated and can be interpreted differently from person to person. Due to this lack of a universally accepted clinical definition of the term, understanding frailty and its implications can be complex. 6 More recently, frailty has been characterized by the reduction of homeostatic reserves, which causes individuals to be at greater risk for negative health-related outcomes due to common stressors.2,3 Morley et al. defined physical frailty as a “medical syndrome with multiple causes and contributors,” characterized by diminished strength, endurance, and physiologic function that increases an individual’s risk for increased dependency and mortality. 3 Pandey et al posed a simpler definition for frailty, as a significant decline in reserve and function of multiple physiological systems. 7 Whether or not to screen for frailty can be hard to determine, but age older than 70 years and significant weight loss as a result of a chronic disease have been shown to merit further investigation. 3 It appears that the physical decline associated with frailty occurs cumulatively over time, following relatively minor stressor events. 8
The Importance of Screening in the Setting of TJA
Major Findings of Frailty Research in TJA.

mFI: Modified Frailty Index; TKA: total knee arthroplasty; THA: total hip arthroplasty; MI: myocardial infarction; PE: pulmonary embolism; LOS: length of stay; OR: odds ratio.
Models to Assess Frailty
There have been several proposed models to assess frailty. All models utilize similar methods and patient-specific data. As such, the accuracy of predictive surgical outcomes does not differ significantly between the different assessment models.
10
However, it does appear that the Clinical frailty scale is the most feasible to use prior to surgery compared to other models.10,11 The common modalities for assessing frailty are seen in Figure 1. Clinical models to assess frailty.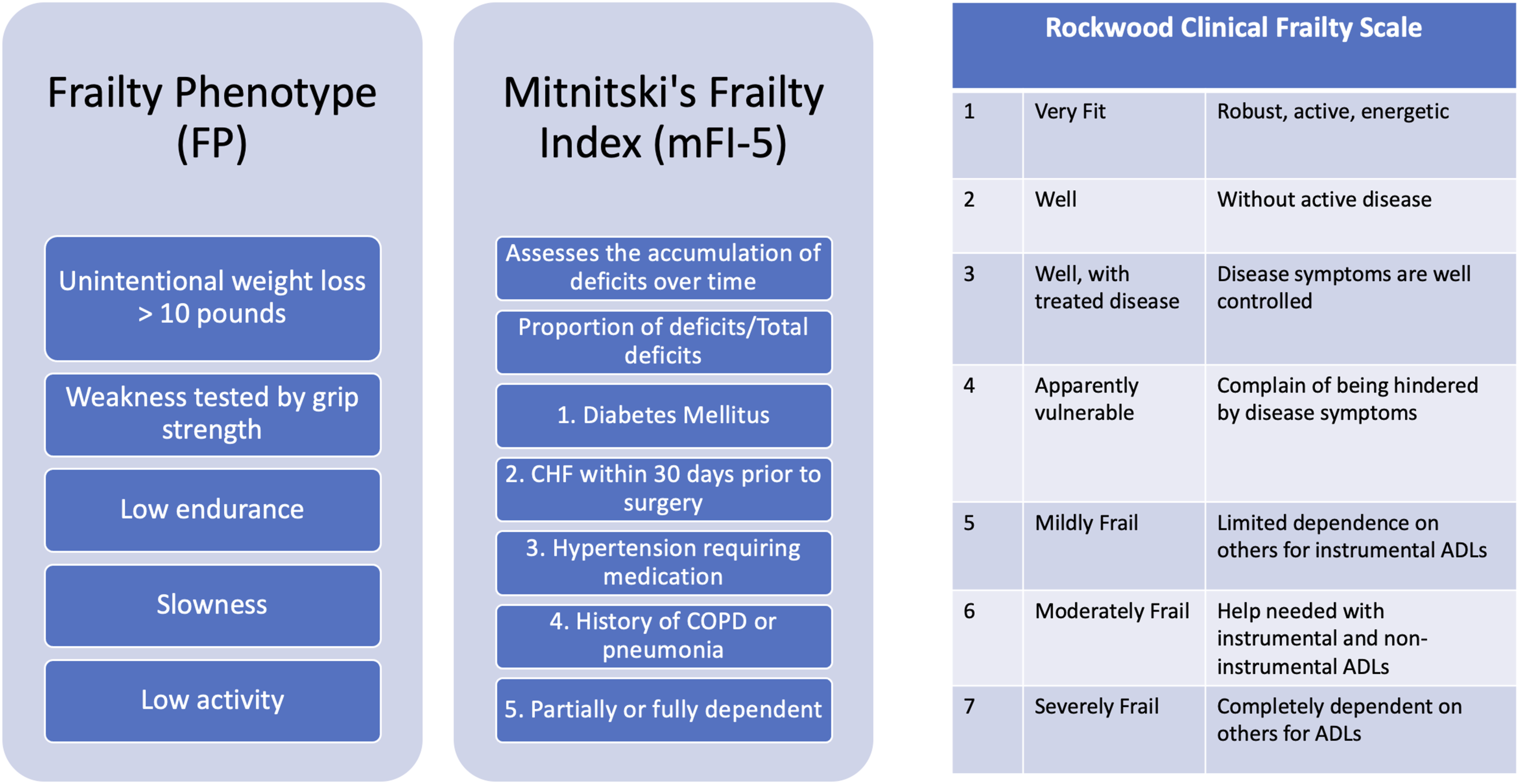
Frailty phenotype, frailty index, and clinical frailty scale
There are several models for assessing frailty, each considering various factors. Fried’s Frailty Phenotype (FP) takes into account five different features, including unintentional weight loss greater than 10 pounds, weakness characterized by grip strength, low endurance (exhaustion), slowness, and low activity. 11 Mitnitski’s Frailty Index (FI) assesses the accumulation of deficits across a broad array of domains (ie, functional status, health and social status, medical problems, mental health problems, and brain and body measures) which occurs over time as the individual ages, in which the “index” is the proportion of accumulation.11,12 In this conceptualization, frailty is measured as the proportion of deficits relative to the total number of deficits evaluated, expressed as a value from 0-1, with higher scores indicating increasing frailty. 11 A database of elderly Canadians determined this deficit accumulation tends to occur at a rate of 3% per year. 12 Cooper et al considered the Frailty Phenotype and Frailty Index among 415 orthopedic patients to explain hospital LOS >5 days and discharge to post-acute institutional care. It was determined that there was a high level of frailty in these patients, 35% using FP and 41% using FI. 13 Another frailty assessment model is Rockwood’s Clinical Frailty Scale. This is a 7-point scale, with 1 being very fit (characterized by a robust, active, energetic, and motivated) and 7 being severely frail (characterized by being completely dependent on others for daily living or being terminally ill). 6
Modified Frailty Index
Frailty presented as an index provides an easier way to identify patients with an increased risk of postoperative complications. To create a more universal method in evaluating patient frailty, the Canadian Study of Health and Aging Frailty Index (CSHA-FI) was created. CSHA-FI consists of 70 variables, each representing the presence or absence of disease. It was simplified to the Modified Frailty Index, consisting of the mFI-11and mFI-5.6,14 The mFI-11 consists of 11 factors, while the mFI-5 consists of 5; each one representing a health deficit. The total existing deficits are divided by the total number of all considered deficits, thus giving an index from 0-1. This index was designed to obtain information retrospectively from medical records and datasets.6,14 Studies have shown that the mFI appears to be a reliable predictor of THA adverse outcomes, including 30-day complications rate, reoperation risk, and length of stay and mortality.15-17
mFI in TKA
The mFI is a valid method for predicting postoperative complications, reoperations, and readmissions in patients who are undergoing TKA. 16 Among 90,260 patients who underwent TKA, Runner et al found that as the mFI score increased, 30-day mortality (OR, 2.10; 95% CI, 1.73-2.55), postoperative complications (OR, 1.22; 95% CI, 1.19-1.25), infection (OR, 1.24; 95% CI, 1.13-1.36), and readmission (OR, 1.41; 95% CI, 1.25-1.59) also increased (P < .001). 16 MFI was a stronger predictor of reoperation rates and showed a strong association (OR, 3.32; 95% CI, 1.36-8.11; P = .009) compared with age >60 years (OR, 1.02; 95% CI, 1.01-1.03; P < .001), male gender (OR, 1.46; 95% CI, 1.29-1.65; P < .001), and BMI >40 kg/m2 (OR, 1.59; 95% CI, 1.35-1.89; P < .001). 16 Given this association between mFI score and postoperative complications, utilization of this index can act as an effective risk assessment tool to assist in preoperative optimization before undergoing TKA.
mFI in THA
Patients with frailty based on both mFI-5 and mFI-11 have significantly less satisfactory functional results following THA. 17 These index tools can be used in preoperative counseling so that more informed decisions pertaining to surgery can be made. 17 Upon investigation of how mFI-5 and mFI-11 scores compare in their measurement of the effects of frailty in patients undergoing THA, it was concluded that, after age adjustment, mFI-11 (P < .05) had better predictive properties of the patient’s health status than mFI-5 (P = .07). The correlation index was stronger for mFI-11 (r = .22) than mFI-5 (r = .19). 17 It should be noted that regardless of age, for both mFI-5 and mFI-11, higher frailty was associated with a longer length of hospital stay. Similar to the setting of TKA, the mFI is a clinical tool proven to be useful in predicting poor functional outcomes after THA.
Frailty and Surgery
Frailty poses a significant risk for adverse outcomes of any surgery. Unfavorable outcomes have been associated with frail people and vascular surgery, including increased complication risk, readmission rates, and short-term mortality. 18 With a minimum follow up of 5-years, preoperative frailty was shown to be associated with significantly increased long-term mortality compared with the non-frail patients. 18 Birkelbach et al examined the relationship between frailty and the occurrence of in-hospital postoperative complications among surgical patients, and found that the rate of post-operative complications was significantly higher in frail patients compared to non-frail patients, regardless of age or surgical procedure.19,20 This particular study implemented Fried’s Frailty Phenotype for assessing frailty among the patients prior to surgery, demonstrating the effectiveness of this tool for identifying patients with increased risk prior to surgery. However, it is important to note that this study excluded patients of elective cardiac surgery. 19 Frailty in oncological surgery patients has been shown to be associated with greater postoperative complications and mortality as well as increased rates of chemotherapy intolerance and percutaneous coronary intervention.21,22 Zhang et al demonstrated that frailty significantly increases all-cause mortality and hospital readmissions among cardiac implantation procedures for advanced heart failure. 23 Similar results have been demonstrated among dialysis and liver transplant patients.24,25 Hewitt et al examined the relationship between frailty in elderly acute-care general surgical patients and length of hospital stay. It was found that frail patients had increased LOS and were more likely to die during the two measuring periods at 30- and 90-days. 26 Based on a growing breadth of literature in administrative data, prospective registries, and systematic reviews, frailty is consistently associated with an increased risk of morbidity, readmissions, and mortality.10,27-29
Demographics and Risk Factors of Frailty
It is estimated that 25-50% of people over the age of 85 are frail, putting them at a significantly greater risk of disability, long-term care, and death. 8 Considering the high prevalence of frailty in the elderly population, it is important to note that the global population of elderly people over 60 years of age was greater than 600 million in the year 2000, and is expected to increase by 2 billion by the year 2050. 30 Frailty is less prevalent in males, while those of lower education and income levels, those with depressive symptoms, comorbid chronic disease, smoking history, and BMI’s outside of normal-range, and those lacking a spouse show higher rates of frailty.31-34 Increased markers of inflammation (CRP) and blood clotting (factor VIII and d-dimer) have been associated with frailty.35,36 An examination of hemoglobin and frailty found that frailty risk was highest at the lowest hemoglobin levels, and the risk was lowest at mid to normal hemoglobin levels, thus indicating that anemia is a risk factor of frailty, 37
Economic Impact
Wilkes et al demonstrated that frail patients had increased length of hospital stay (.8 vs 2.1 days; P < .001) and had increased mortality (0% vs .4%; P < .001). 38 This resulted in higher total costs ($6934 in non-frail vs $13,319 in frail patients), and lower net hospital income ($5447 vs $3129). 38 A multivariate analysis of the same data found that frailty was independently associated with an increase in direct cost (OR 2.2; P < .001), indirect cost (OR 1.9; P < .001), total cost (OR 2.2; P < .001), and decreased net income (OR .8; P < .001). 38
A similar study examining the impact of frailty on the economic evaluation of geriatric surgery found that frail patients had a higher hospital cost compared to non-frail patients (22,282.541 vs 16,388.844 €, P < .001) and had increased LOS (10.16 vs 8.4 days, P < .001), with an opportunity cost in frail patients estimated to be 1019.56 €. 39 Additionally, frailty has been strongly associated with higher rates of intensive care unit admissions (OR: 2.52), discharge to institutional care (OR: 2.09), 30-day mortality (HR: 3.03), increased LOS (incidence rate ratio [IRR]: 1.62), and an increase in total health-care costs at 30-day follow up. 4
Pepper et al specifically utilized the mFI in calculating increased cost among frail patients. 40 Among 1821 patients undergoing total joint arthroplasties, there was a .68% increase in cost per incremental age increase. Additionally, statistically significant increased cost was seen among patients with an mFI score of 2 or greater. 40
Feasibility and Value
In a study examining frailty assessment prior to thoracic surgery, comprehensive frailty assessments using the Modified Frailty Index were found to be feasible in pre-operative outpatient settings for both patients and surgeons. 41 The value of using frailty as a predictor for surgical outcomes includes being able to identify vulnerability and can help in treatment planning resulting in optimized clinical outcomes and resource allocation. 41 In another study, researchers used the Edmonton Frail Scale (EFS) and examined its feasibility in identifying postoperative complications among elderly patients. The researchers assessed the patients’ postoperative morbidity using the Comprehensive Complication Index (CCI) and Postoperative Morbidity Survey (POMS). Their findings suggested that operative risk in elderly patients undergoing major abdominal surgery can be predicted using EFS and that the assessment was completed quickly, was feasible, and was well accepted by the patients. 42 Aucoin et al examined various assessment tools and concluded that the highest reported measure of feasibility was the Clinical Frailty Scale, which showed accurate predictability of mortality and non-favorable discharge. 43
Frailty in TJA Patients
There is scarcity of literature regarding measuring frailty in total join arthroplasty (TJA) patients. However, one study examined frailty as a predictor of hospital length stay after TJA in elderly patients. In this study, the patient’s frailty status was assessed using the Clinical Frailty Scale and the FRAIL Scale. The study concluded that higher scores on the Clinical Frailty Scale were significantly associated with increased LOS and discharge to rehabilitation centers among the TJA patients. The FRAIL scale, on the other hand, did not present any significance in that regard. This suggests the possibility that the Clinical Frailty Scale may be a useful instrument for measuring frailty in total joint arthroplasty. 20
A similar study examined the hospital frailty risk score (HFRS) in hip and knee arthroplasty patients, with each patient being scored with subsequent rates of adverse events being compared between patients with low, intermediate, or high frailty risk scores. In order to assess the relationship between HFRS and post-operative adverse events, a multivariable logistic regression model was used. They found that the HFRS accurately predicted adverse events after revision total hip arthroplasty and knee arthroplasty. 44 Intermediate to high frailty risk increased rate of 30-day readmission (23.8% vs 9.9%, P = .006), surgical complications (28.6% vs 7.8%, P < .001), medical complications (11.9% vs 1.0%, P < .001), other complications (28.6% vs 2.3%, P < .001) Clavien-Dindo grade IV complications (14.3% vs 4.8%, P = .009), and transfusion (33.3% vs 6.1%, P < .001). 44 Regression analyses demonstrated an odds ratio of 3.45 for surgical complications, 7.29 or medical complications, and 14.15 for other complications. 44
In another study measuring frailty in arthroplasty patients, the John Hopkins ACG Frailty Defining Diagnoses Indicator was used as the assessment system for determining frailty status among elderly patients undergoing total joint arthroplasty. The ACG system is a binary variable that factors in 12 types of diagnoses. The study found higher readmission rates among patients classified as having intermediate to high frailty risk compared to non-frail patients (after 30 days: 23.8% vs 9.9% P = .006; 90 days: 26.2% vs 13.0% P < .018), higher surgical complications (28.6% vs 7.8%, P < .001), and higher medical complications (11.9% vs 1.0%, P < .001) in addition to all other complications (28.6% vs 2.3%, P < .001). 45 Similarly, a recent prospective cohort study demonstrated that frailty is an independent risk factor of one-year mortality following elective orthopaedic surgery.46 Clinical Frailty Score was used to assess frailty prior to surgery, with 30% of patients being categorized as frail. A total of 7.7% of patients died within one year of surgery, and multivariate logistic analysis demonstrated higher CFS was an independent risk factor of one year mortality (OR = 2.271).46
Schmucker et al conducted a systemic literature review examining frailty as a risk factor for short-term clinical outcomes of total joint arthroplasty (TJA) among older adults. The researchers make note of the lack of a “gold standard” for measuring frailty and conclude that establishing a standardized measurement of frailty would be beneficial to geriatric care and frailty, allowing for the assessment of functional outcome measures as well as improving outcomes in frail patients undergoing arthroplasty. 4
Conclusion
As the rate of TJA grows in the United States, its valuable to understand how the assessment of pre-operative patient frailty can contribute to predicting adverse events. While frailty has commonly been associated with older age, literature has shown that there are many other factors that characterize frailty as a predictor of surgical outcomes. Models such as Fried’s Frailty Pheotype, Mitnitski’s Frailty Index, and Rockwood’s Clinical Frailty Scale have all been found to be accurate models of measurement for patient frailty. The Modified Frailty Index is also a valid method for predicting postoperative complications, re-operations, and readmissions in patients undergoing TKA. Frailty based on both MFI-5 and mFI-11 have proven themselves a useful tool for producing poor functional outcomes after THA as well, regardless of age. The presence of frailty has shown to be lower in males and highest in those over the age of 85, of lower education and income levels, with depressive symptoms, comorbid chronic disease, smoking history, BMI’s outside of normal-range, and lacking a spouse. Frailty also holds a strong presence in economic impact. Frail patients have increased length of hospital stays, mortality, higher total costs, and result in lower net hospital income. While there is still a lack of “gold standard” for measuring frailty in TJA patients, studies have still found that frailty is a valuable assessor of functional outcomes for frail patients have been found to have higher readmission rates, surgical complications, and medical complications. Based on a growing breadth of literature, frailty is consistently associated with an increased risk of morbidity, readmissions, and mortality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our study did not require an ethical board approval because it is a review of the literature.