
Abstract
Chronic, non-traumatic pathologies of the foot and ankle can be mobility-limiting for patients of all ages. The objective of this study was to compare postoperative changes in LifeSpace Mobility Assessment (LSA) scores of adult and elderly patients following elective foot and ankle surgery. A prospective study of 184 patients undergoing elective ankle, hindfoot, and midfoot procedures conducted by one surgeon between 2015 and 2019 was undertaken. Patient-reported LSA scores were collected at preoperative, 6-month, and 12-month follow-up. Patient data was compared using an independent sample t-test for continuous, normally distributed data and a chi-squared or Fischer’s exact test for categorical data. Alpha and beta were .05 and .8. Patients were divided based on age. 140 patients were observed in the younger (<65) group, 44 patients were observed in the elderly (≥65) group. The average LSA score of elderly patients at the preoperative visit was 58.3 (SD 38.0) vs 79.3 (SD 38.8) in the younger cohort (P = .041). Both patient cohorts saw decreased mobility at 3-month postoperative visits but surpassed preoperative mobility scores by 6 months and 1 year postop. No difference in average mobility score was observed between young (85.6, SD 36.1) and elderly (90.1, SD 34.3) cohorts at 1-year follow up. Given the increased rates of perioperative comorbidities and the heightened risks of intraoperative complications, physicians may be more inclined to manage elderly patients with longer periods of conservative treatment for similar pathologies. However, these results imply that elderly patients experience similar improvements after surgery to younger cohorts and should not be excluded from surgical consideration. Our results, in tandem with literature showing the deleterious effects of decreased mobility in the elderly, suggest that the discussion to pursue or hold surgical correction of chronic foot and ankle disease in patients over age 65 must consider the mobility benefits of surgery.
Introduction
Chronic, non-traumatic pathologies of the foot and ankle can be mobility limiting for patients of all ages. While there are numerous indications to perform elective foot and ankle surgeries, the common goal is to reduce pain and improve function and mobility. These surgeries, however, can be accompanied by lengthy postoperative recoveries, required weight-bearing restrictions, and decreased mobility. The patient and surgeon must consider the implications of recovery and ultimately weigh the cost of potential further decline with the possibility of improvement. Given increased rates of perioperative comorbidities and the heightened risks of intraoperative complications, physicians may be more inclined to manage elderly patients with long periods of conservative treatment for similar pathologies.1,2 Previous work has shown that decreases in the mobility of elderly patients affects longevity and is linked to increased rates of all-cause and non-cancerous morbidity and mortality. 3
By comparing the preoperative and postoperative mobility scores between elderly and younger patients, surgeons might better understand if surgical repair and the ensuing recovery from mobility-limiting conditions could benefit the overall health of the elderly. Additionally, surgeons can better counsel patients about postoperative expectations and rehabilitation. As the incidence of foot and ankle pathology increases in older, more frail populations, it is critical that surgeons better understand the recovery timeline and mobility gains associated with the surgical procedures used to address these pathologies.
The primary objective of this study was to assess changes in the LifeSpace Mobility Assessment (LSA) scores of elderly patients following surgery to address non-traumatic ankle, hindfoot, and midfoot conditions. The Life-Space Assessment Questionnaire (LSA) is a validated tool utilized to quantify how patients mobilize after a medical event as they return to their previous daily environment, such as their home, neighborhood, and community (so deemed their “life-space.”) Furthermore, the LSA is a scoring system used to assess real-world mobility during daily life in geriatric patients. 4 LSA scores are directly associated with physical capacity and other factors that may limit mobility. 5 Scored on a scale of 0-120 – with higher values correlating with increasingly independent mobility – the LSA evaluates the frequency and range of mobility from one’s bedroom, other household rooms, outside of their home, in their neighborhood, their town, and outside of their town. Additionally, the LSA incorporates the use of ambulatory aids or another individual’s assistance into its scoring. The questionnaire has been validated and utilized in foot and ankle literature.3,6 We hypothesized that elderly patients with non-traumatic pathologies of the foot and ankle would be more mobility-limited pre- and postoperatively when compared to a younger cohort with similar conditions.
Methods
Study Design
Baseline Characteristics.
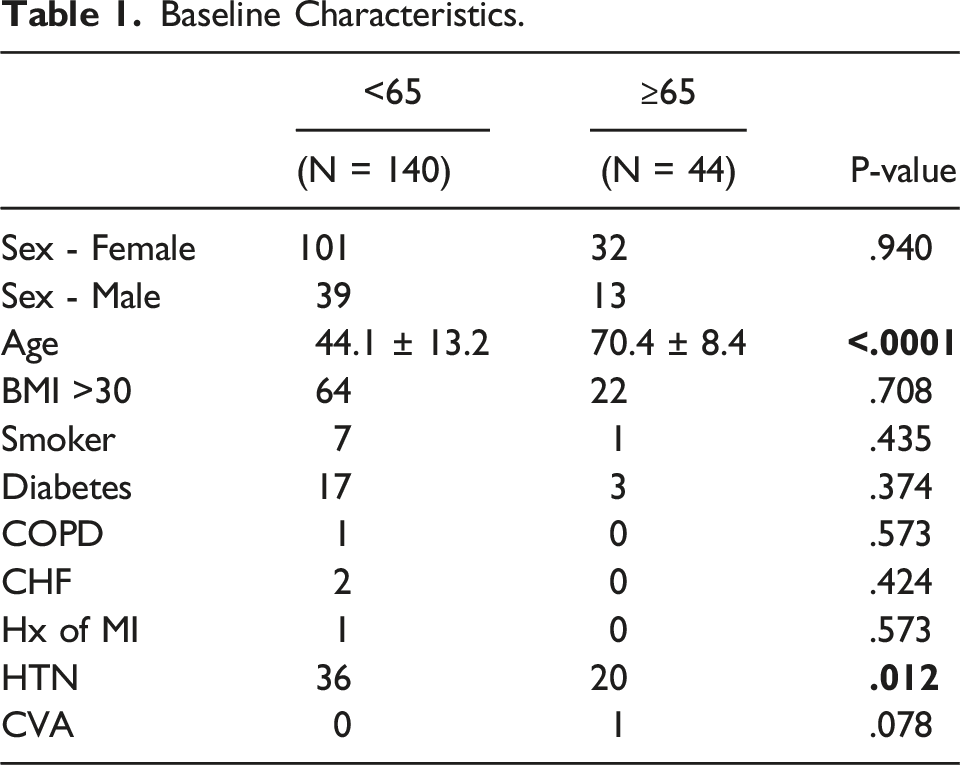
Patient demographics, operative characteristics, and clinical outcomes were queried and recorded from a review of the electronic medical record. Per the single surgeon’s postoperative protocol, patients were evaluated at regular preoperative, and at 3-, 6-, and 12-month postoperative time points. During each of these visits, patients were administered routine visual analog pain scale (VAS) and Short Form-36 (SF-36) questionnaires, along with a Life-Space Mobility Assessment (LSA).
Statistical Analysis
Following collection of all demographic and outcome data, a Sharpiro-Wilk test was utilized to test their normality. Continuous data that were normally distributed were compared with independent sample t-tests. Those which were continuous, but not normally distributed were compared with Mann-Whitney U tests. Categorical data were compared using chi-squared or Fischer’s exact tests. Alpha and beta were assumed to be .05 and .8, respectively. Following grouped analyses, a post hoc power analysis of VAS, SF-36, and LSA comparisons was conducted using OpenEpi: Open Source Epidemiologic Statistics for Public Health version 3.1 (https://www.openepi.com/Menu/OE_Menu.htm). All other analyses were carried out using SPSS software version 27.0 (IBM Corporation, Armonk, NY).
Results
Demographics
Disease Processes.

Life-Space Outcomes
Overall, average grouped LSA scores improved significantly from preoperative to 1-year postoperative visits (Figure 1). While a significant depression in LSA was noted 3-months postoperatively, patients had significantly improved from their preoperative LSA scores by the 6-month postoperative visit. The average LSA score of elderly patients at the preoperative visit was 58.3 vs 73.9 in the younger cohort (Table 3). Both the young and elderly patient cohorts experienced decreases in mobility at their 3 months postoperative visits but regained and surpassed their preoperative mobility scores by 6 months and 1 year postop. No difference in average mobility score was observed between young and elderly cohorts at 1-year follow up. Both cohorts showed similar changes in average LSA score from preoperative to 3-, 6-, and 1-year postoperative visits. Grouped mean LSA scores at preoperative (mean 70.3 ± 38.8), 3-month (mean 57.1 ± 34.8), 6-month (mean 81.7 ± 33.9), and 1-year postoperative (mean 87.5 ± 34.9) visits. Comparisons displayed are between each postoperative timepoint and the preoperative baseline LSA score. * denotes P-value <.05, ** denotes P-value < .01. LifeSpace Outcomes.

Subgroup Analysis.

VAS/SF-36 Outcomes
Patient-Reported Outcomes.

Discussion
The influence of mobility on morbidity and mortality in elderly populations cannot be understated.7,8 Moreover, pathology of the foot and ankle in these cohorts is strongly linked to increases in fall risk and greater general functional impairment. 9 However, in surgical intervention for nonemergent foot and ankle disease, the cost and benefits of surgery are not well understood. Therefore, the purpose of the present study was to observe whether elderly patients undergoing nonemergent midfoot, hindfoot, and ankle surgery experienced similar postoperative mobility benefits to younger patients undergoing similar procedures. We observed a cohort of elderly patients with significantly increased mobility limitation preoperatively as compared to a younger preoperative group. However, at the 1-year post-operative mark, the mobility of the elderly cohort had reached that of the younger cohort. Notably, the young and older groups achieved the minimum clinically important difference (MCID) for the LSA of 5.16 by 1-year postoperatively. 10 We also found that both groups of patients responded similarly to surgical intervention in VAS pain score reduction and increased SF-36 PCS and MCS scores at their 1-year follow-ups.
These results agree with several previous studies that noted positive outcomes for older patients undergoing various elective foot and ankle procedures. In an age-stratified analysis of patients undergoing first metatarsophalangeal joint fusion, Lunati et al 6 showed that those over the age of 65 had similar improvements in VAS, SF-36, and LSA scores as younger patients and were at no increased risk of postoperative compilation. Similarly, in a small set of patients undergoing surgical repair of chronic insertional Achilles tendinopathy, Phen et al 11 noted no increase in complication rate for patients over the age of 60 relative to a younger cohort with similar improvements in VAS and SF-36 scores. In a comparison of patients aged 50-60 and those above the age of 70, Tenenbaum et al 12 showed equivalent VAS and SF-36 outcomes following total ankle arthroplasty. The mobility improvement pattern observed in our cohort was also akin to those found by Kurkis et al 3 in a subset of surgical foot and ankle patients, with notable decreases in mobility at 3 months likely associated with postoperative weight bearing restrictions.
Though the body of literature for mobility outcomes after nonemergent foot and ankle surgery is limited, good data exists supporting surgical intervention after acute ankle injuries in elderly patients.13–17 Work from Shivarathre et al 17 examined 92 patients over the age of 80 who underwent open reduction and internal fixation (ORIF) of unstable ankle fractures, finding that upwards of 86% of patients were able to regain preoperative mobility by 3-6 months postop. Furthermore, foot and ankle surgery as a whole is often able to fulfill patient expectations, as Henry et al 18 found in a large sample of patients, a clinically important proportion of expectations were fulfilled with up to 34% of patients stating that their expectations were surpassed and 58% stating that their expectations were partially fulfilled. Better outcomes and satisfaction in orthopedic foot and ankle surgery may be due in part to the patient population, as Ali et al 19 describe an elevated baseline health of many surgical foot and ankle patients relative to age-matched peers within other orthopedic pathologies. Patients in the present study over the age of 65 appear to follow this trend, and their overall lack of significant medical comorbidity may help explain their large postoperative mobility gains.
While older patients in the present study regained a significant amount of absolute mobility via LSA postoperatively, the finding of depressed preoperative LSA relative to younger patients is arguably more significant. Mobility deficits and decreases in LSA scoring have both been correlated to significant increases in morbidity and mortality.20–24 Though chronic foot and ankle pathologies in elderly patients are not traditionally recognized as requiring expedited surgical intervention, the degree to which preoperative mobility was depressed in our cohort is noteworthy. In a population of elderly women, Mackey et al found that LSA scores less than 60 were associated with a 1.5 times increase in all-cause mortality relative to those with scores above 80. 24 These thresholds are notable in the context of our results as the elderly patients crossed from a higher mortality risk preoperatively, with an average LSA 58.3, to a lower mortality risk 1-year postoperatively, with an average LSA of 90.1. This represents a population that encompasses the LSA score parameters mentioned by Mackey et al by undergoing surgery and is therefore at less risk for mobility deficit associated mortality. Additionally, Auais et al 25 present a linear relationship between one point decreases in LSA score and one point increases in fear of falling. Fear of falling has a significant impact on patient quality of life, as Rivasi et al 26 remind us that this fear may be crippling and take a heavy toll on the mental and physical health of elderly patients. Indeed, in a study by Kim et al, a statistically significant association was made between those very afraid of falling and all-cause mortality in a population of over 10 000 individuals. 27 While we cannot directly surmise from our data that prior to surgical intervention our pre-operative elder cohort was at increased risk of falling, we can assert that fear of falling and the associated detrimental effects on psychological well-being did contribute to decreased SF-36, VAS, and LSA scores in our patients prior to surgery, and as such, contributed to all-cause mortality. Falls are responsible both globally and in the United States for significant mortality, a high number of years of life lost, and an increasing number of years lived with disability, with ankle injury being one of the most common injuries sustained by fall victims.28,29 Presently, foot and ankle surgeons may be more apt to continue conservative management of nonemergent pathologies in the elderly due to increased rates of perioperative complication and increased medical complexity.30,31 However, our data suggest that with the increased baseline health of foot and ankle patients relative to other operative patients of similar age, earlier surgical intervention may be justified.
Limitations
The present study has many strengths, including the use of multiple validated patient outcome measures to detect surgical intervention effectiveness. While analyzed retrospectively, all patient-reported outcomes were collected prospectively at routine clinic visits to minimize recall bias risk. Additionally, since the same single surgeon treated all patients, postoperative restrictions and therapeutic protocols were the same regardless of age. This study also has limitations inherent to its design that must be noted. The generalizability of our results is limited.
Given that all surgeries were performed by a single surgeon within a large multispecialty hospital system, the routine postoperative care patients received may not apply to all. Additionally, with a relatively short 1-year follow-up time point, it is unclear how far the mobility benefits observed in the elderly population extend after surgery. While no statistically significant differences in LSA, VAS, nor SF-36 scores were noted between cohorts, our study was not adequately powered to detect differences at the 1-year postoperative timepoint via post hoc power analysis. However, the limitations of post hoc power analysis should also be noted, given that the results of such analyses are the product of a given study’s effect and sample sizes. 32 To detect a significant difference of 5 points in LSA at the 1-year visit between our groups (MCID is 5.16), given the standard deviation observed in our cohort, a sample size of 1462 patients would be needed.
Conclusion
Our study provides evidence that chronic pathologies of the midfoot, hindfoot, and ankle are more mobility limiting in elderly patients when compared to a younger cohort undergoing comparable surgeries. Additionally, elderly patients were found to regain more mobility following surgical correction of these conditions, allowing them to ambulate at similar levels postoperatively compared with younger patients. These results, in tandem with literature highlighting the drastic deleterious effects of decreased mobility in the elderly, suggest that the discussion to pursue or hold on surgical correction of chronic foot and ankle pathology must consider the mobility benefits of surgery.
Footnotes
Author’s Note
Investigation performed at the Emory Clinic, Atlanta, Georgia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.