
Abstract
Introduction
Internal fixation is the treatment of choice for subtrochanteric fractures in most conditions. However, it may be an unsuitable procedure for patients with poor health status, osteomyelitis, and surrounding soft tissue compromise. This study aimed to ascertain the viability and reliability of using external locking plate fixation for these difficult cases.
Methods
Eleven patients with femoral subtrochanteric fractures who received external locking plate fixation in our institute from January 2014 to December 2019 were enrolled in our study. The bone union time, wound complication, alignment, and necessity for narcotic agents were evaluated.
Results
The average length of follow-up was 17.5 months (range, 14-26 months). The mean time for bone union was 17.7 weeks (range, 15-21 weeks). The indications included poor health condition, soft tissue compromise, and post-operative osteomyelitis. Pin tract infection was noted in two patients who were treated successfully with oral antibiotics administration and removal of the involved screws. Osseous union with varus deformity <10° was achieved in all patients except one. Three patients required an orally administered pain killer at the final visit. The average Harris Hip Score at one year post-operatively was 66.6 (range, 49-80).
Conclusions
Although the current study only involved 11 patients, we believe that our method may serve as a valuable alternative for the treatment of a femoral subtrochanteric fracture in selected cases.
Level of Evidence
Level IV, retrospective case series
Keywords
Background
Proximal femoral fractures have become a major public health issue during recent decades due to the increasing incidence and influence of post-injury issues. 1 Subtrochanteric fractures (STFs), account for 5-10% of proximal femoral fractures, 2 is defined as a fracture located within 5 cm of the lesser trochanter. The overall incidence of STF is estimated to be 15-20 per 100,000 individuals with a bimodal distribution. 3 It mainly affect elderly patients and almost all patients require surgical treatment. 4 Performing operations for these fragile patients remains a challenge even with the advance of peri-operative care and anaesthesia technique. High post-operative complications and mortality rates are still noted in literature.5,6
Surrounding soft tissue condition is also another major concern. Some elderly patients with STF are in bedridden before injury. Bedsore formation around the hip region can exist for these patients. 7 Furthermore, soft tissue compromise caused by open fractures can still occur. 8 The soft tissue problems, whether caused by bedsores or open fracture, may increase the surgical difficulty and post-operative infection rate which make traditional internal fixation technique unsuitable. 9
Osteomyelitis is one of the devastating complications after internal fixator for STF. 10 Management of these cases usually requires implant removal and extensive debridement. 11 For patients still having a non-union fracture, removing implants can result in severe hip pain and immobilization status. 12 Undesired complications such as pneumonia, pressure sore, and urinary tract infection can exist due to prolonged bedridden status. 13 Hence, to provide adequate fracture stability is crucial in treating these patients.
External fixator for hip fractures had been implemented for decades. 14 Although it never became the treatment of choice in managing patients with STFs; some surgeons consider that it could be a reasonable and effective alternative method for patients with high risk, open fracture, and limited medical resources in developing countries.15,16 These traditional external fixators are often bulky, uncomfortable, and inconvenient. In order to solve the problems related to traditional external fixators, many doctors use external locking plate technique to achieve a better fixation stability with low-profile and a comfortable frame.17-21 However, using external locking plate fixation in management STF had not been well described in the literature. In the present retrospective study, we aimed to analyse the results of 11 consecutive patients who received external locking plate fixation as a definitive treatment in our institute.
Patients and Methods
From January 2014 to December 2019, 16 patients with subtrochanteric fractures who received external locking plate fixation were enrolled in our study. The operative indications included poor health condition due to comorbidities with American Society of Anesthesiologist score III or IV, soft tissue compromise caused by open fracture or hip pressure sore, and post-operative osteomyelitis. Before operation, we explained our treatment strategies and discussed the pros and cons with patients and their family so they could decide which procedure, internal or external fixation, should be performed. The five patients who died and were unable to fulfil at least 1 year of follow up were excluded. After institutional review board approval (EMRP-103-051) and informed consent was obtained from the patients or family, all medical records were reviewed comprehensively.
Patient demographic data.

M, male; F, female; TA, traffic accident; DM, diabetes mellitus; HTN, hypertension; CAD, cardiovascular disease; ESRD, end-stage renal disease; COPD, chronic obstructive pulmonary disease; EF, external fixation.

A 76-year-old male (case 9) underwent open reduction and internal fixation with intramedullary nail for right femoral subtrochanteric fracture 2 months before visiting our institute. The anteroposterior (A) and lateral (B) view of right femur reveal that the fracture was still ununited. Debridement was performed several times due to osteomyelitis and resulted in surrounding soft tissue defect (C). The diagnosis of osteomyelitis was also proved by bone scan (D).
Surgical Technique
Before the operation, patients were evaluated with a complete history of illness, physical exam, and laboratory tests. Plain radiographs were obtained to detect the fracture pattern. Under regional anaesthesia or nerve block, the patient was placed on fracture table. For patients without soft tissue or infection problems, we performed closed reduction by traction to achieve an adequate alignment. If acceptable reduction could not be achieved through closed methods, an open technique through the open wound or short incision was performed. Then an external locking plate, which acted as a bridge to provide relative stability and promote fracture healing by callus formation, was applied (Figure 2). In this study, we use a contralateral side plate (LISS–DF, Synthes; VA-LCP Condylar Plate, Synthes) with ‘upside down position’ for stabilisation of the proximal femoral fracture. Four to six screws were placed into the proximal component of fracture to achieve a secure fixation. The screw length and position were ensured under fluoroscopy in two planes. Three to four screws were placed into the distal component to reach adequate stability. If osteomyelitis or soft tissue problems existed, extensive debridement and implant removal were performed before reduction and fixation procedures. After implants removal and extensive debridement. Open reduction for the fracture followed by external fixation with a locking plate was performed.
Post-Operative Care and Follow-Ups
Following surgery, regular aseptic wound care and pain control were provided for the patients. All patients were allowed to mobilize, change position, sit, and get out of bed if tolerated. Non-weight bearing gait training with assistance was started as soon as possible for patients with adequate muscle power. Subsequent physical therapy and partial or full weight bearing were scheduled after discussion with the physical therapists and surgeons. Clinical and radiographic follow-up examinations were performed at each visit until bone union (Figure 3). Radiographic bone union was defined as the presence of a bridging trabecular bone. If the external locking plate interfered with the evaluation of union on the radiographs, a computed tomography (CT) scan was performed to confirm union. The external locking plate was removed when sufficient bone union was achieved. The Harris Hip Score was used for functional evaluation at 1 year postoperatively. Bone union is revealed in the radiography (A) and computed tomography (B) 4 months after operation.
Results
Patients’ Results.
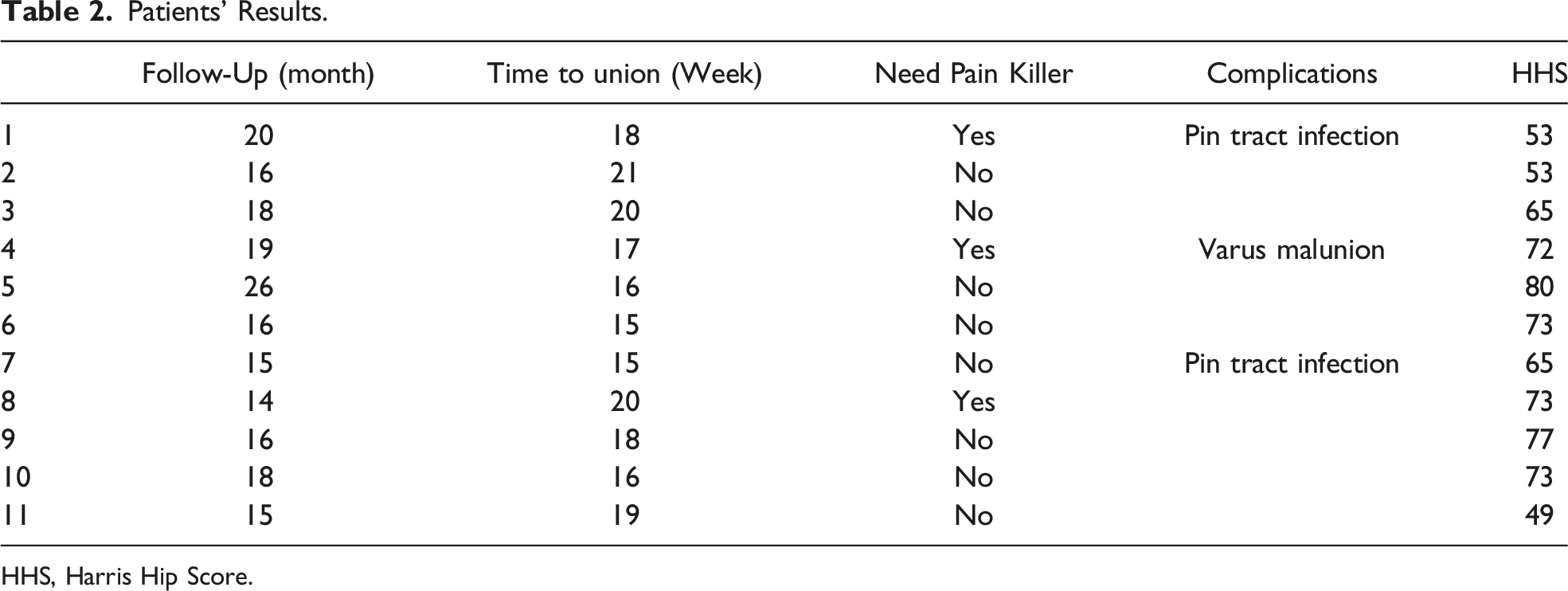
HHS, Harris Hip Score.
Discussion
In our case series, an acceptable outcome and low complication rate were achieved using external locking plate fixation for STF. This could be an alternative method to manage these difficult cases. To the best of our knowledge, this study is the first one to suggest the use of external locking plate fixation for treating patients with STF.
The subtrochanteric region of the femur is an area of high stress concentration which make it more prone to a delayed union or even non-union. 22 In terms of age, approximately two-thirds of STF occurs in elderly patients (>50 years old). 4 In consideration of high mortality rate and immobilization-related complications under conservative treatment, surgery is recommended by most of surgeons in the literature to allow early mobilization and reduce fracture related complications.4-6 In operation treatment, closed or open reduction followed by internal fixation with various implants such as fixed angle plate, intramedullary nailing, or locking plate are the standard treatments for STF.4-6 However, some fragile patients with severe comorbidities can complicate the anaesthesia process and post-operative care. Hence, significant post-operative morbidity and mortality has still been a concern in recent decades even with the advancement of medicine and implants. 23 According to the literature, the mortality rate in elderly patients with STF can be 27% at 1 year postoperatively. 5 For the reasons above, there are still a lot of room, especially in operation methods and perioperative care, to improve in managing this kind of patients.
Most bedsores are related to facilities (hospital and nursing home) and often develops in the heel, ankle, hip, and tailbone.24,25 It remains a common disorder with a prevalence of 5 to 9% and more than 70% occur in elderly patients (age >70 years old). 7 The presence of a hip bedsore could be an risk factor of septic contamination in the surrounding bone structure. Le Fort et al 26 retrospectively analysed 33 spinal cord-injured cases with septic hip arthritis and revealed that 25 (75.8%) were caused by a trochanteric pressure sore. Darouiche et al 27 evaluated 36 patients with pressure sore and six were diagnosed as osteomyelitis by pathologic examination of bone tissue. Hence, the presence of a pressure sore could be a risk factor of infection which may increase the possibility of contiguous osteomyelitis after internal fixation procedures.
Open fracture is another concern in performing surgery for hip fracture patients, although it is rare and often results from high energy trauma which can cause soft tissue envelop compromise. In managing these cases, direct internal fixation without considering soft tissue damage can result in an elevated infection risk. Hence, a two-stage protocol with temporary external fixation followed by converting into definite internal fixation after recovery of surrounding soft tissue has been proposed. Van den Bossche et al 28 treated 20 high-grade femur open fractures with temporary external fixator followed by conversion into an internal fixator in an average of 21 days and none of them developed a deep infection. Although good clinical outcomes are noted in literature they required at least two surgeries which incurred additional costs. Furthermore, some patients with subtrochanteric fractures are elderly persons and fragile which make it an unsuitable procedure in consideration with the risks related to multiple surgeries. Hence, external fixator as a definitive treatment method had been proposed for various kinds of fractures, including hip fractures, especially for patients with open fracture or poor soft tissue envelop. 29
In comparison with standard internal fixation, there are several advantages of using external fixation to treat subtrochanteric fracture.30,31 First, the surgery can be performed under regional anaesthesia or nerve block which can decrease the risk related to anaesthesia procedures. Second, shorter operation time and minimal blood loss can be achieved which is crucial for elderly patients with multiple comorbidities. In our case series, the mean surgical time was only 37.5 (range, 31-43) minutes if we exclude the three patients who required the additional procedures of debridement and/or removing previous implants due to open fracture or osteomyelitis. Third, soft tissue dissection was not needed which can be essential in preventing soft tissue complications. Fourth, the implants can be removed at outpatient clinics without any anaesthesia. For the reasons above, external fixation of subtrochanteric fractures seems to be a reasonable alternative choice and efficacy had been confirmed in literature.
However, this technique was associated with some undesirable complications such as pin-tract infection, decreased surrounding joint range of motion, delayed union, and chronic pain. 29 Furthermore, the bulky frame of a traditional external fixator could make the patients uncomfortable and cause inconvenience which decreases compliance and satisfactory rate.
tThe concept of using the locking plate as an external fixator was first introduced by Kloen. 32 The main advantage of this technique is the ability to construct a low-profile frame and relative high stability in comparison with traditional devices which make it popular in treating various kinds of injuries. Ma, et al used external locking plate technique to treat various kinds of tibial injuries, which included open fracture,17,18,21 non-union and massive bone defect,19,20 and the outcomes were satisfactory. It could be used as a temporary measure or definitive treatment method. In a biomechanical study, the axial stiffness of the external locking plate was significantly higher than that of the traditional external fixator. 18 The robust construct made it possible to apply this technique to treat a femoral fracture. 33 However, it is rare to use an external locking plate fixation to treat STF in the literature.
A locking plate is an implant that provides angular stability and behaves as an internal splint which is often used to treat complex comminuted and osteoporotic fractures. From the biomechanical view, the fixed angle device could acts as an external fixator if applied supracutaneously.17-21,32 Unlike a traditional locking plate which only allows fixed direction of screws, the new evolution of the variable angle design makes it much easy in applying the screws and purchase bone stock. 34 In this study, we chose a contralateral side distal femur locking plate (LISS–DF, Synthes; VA-LCP Condylar Plate, Synthes) with a reverse position to fit the anatomy of the proximal femur. The variable angle design can facilitate the application of screws during operation and the surgery should be performed under fluoroscopy to ensure the reduction quality and implants position.
The most frequent complication that occurs after external locking plate fixation is screw/pin-tract infection.17-21,32 Two of our patients encountered this problem and were treated successfully by removing the screws and oral administration of antibiotics. Infection may have been due to skin irritation induced by the threaded shaft of the locking screw and the screws being inserted too close between each other which make it difficult to clean the screw tract. Hence, we should keep the screws as far apart as possible which can be facilitated through using implants with a variable angle design during application in the metaphyseal region. In addition, patients should be educated to clean the pin tract regularly and correctly to prevent this unfavourable complication.
Loss of fracture reduction and malunion are also concerns. In our study, one case united in a varus deformity more than 10°. However, many of our patients were in a poor health or even bedridden. For these fragile patients, the most important treatment goal is pain relief through fracture fixation followed by early mobilization instead of perfect alignment. Hence, malunion may have occurred but it did not cause big problems in most cases. The condition of malunion can be avoided by using enough screws positioned adequately, protecting the injured leg properly, and implementing an appropriate rehabilitation program in a step-by-step progress under supervision.
Although the outcomes in our case series are acceptable, there are still several limitations in our study. First, the retrospective nature of the study design lacked randomization. Therefore, it was unable to enroll patients who underwent different surgical methods for subsequent comparison of clinical outcomes. Second, our case series only contains 11 patients; consequently, the sample size is too small to prove the feasibility and efficacy of using this method. Third, it was not a randomized study because the patients or family could decide what type of procedure was performed. Finally, we enrolled a diverse type of patients which included poor health condition, soft tissue compromise, and post-operative osteomyelitis. The broad inclusion criteria may affect the analysis. For the reasons above, further prospective randomized studies are required to prove the feasibility and reliability of this technique.
Conclusion
In conclusion, even though the current study included a small sample size, using an external locking plate as a definitive external fixator for femoral subtrochanteric fractures provided a simple and comfortable treatment with appropriate mechanical loading. Hence, our technique can serve as a valuable alternative for the treatment of femoral subtrochanteric fracture especially for patients with poor surrounding soft tissue envelop and health condition.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Fund from E-Da hospital (EDAHP 104018, EDAHP 106051) was received in support of this work.
Ethical Approval
The Study Was Approved by the Institutional Review Board (EMRP-103-051).
Informed consent
Informed consent was obtained from all individual participants included in the study.