
Abstract
Purpose
Posterior short-segment fixation (SSF) and long-segment fixation (LSF) are two methods for the treatment of Kummell disease, but the safety and effectiveness of these two surgical methods still lack adequate medical evidence. This study aimed to evaluate the two methods.
Methods
Database searches for randomized controlled trials, case-control studies, and cohort studies of posterior SSF and posterior LSF in the treatment of Kummell disease were performed. After the document quality was evaluated with the Newcastle-Ottawa Quality Assessment Scale, a meta-analysis was carried out.
Results
Meta-analysis revealed that the operation time and intraoperative blood loss in the LSF group were higher than those in the SSF group [MD = −18.17, 95% CI (−30.31, −6.03), z = 2.93, P = .003; MD = −82.07, 95% CI (−106.91, −57.24], z = 6.48, P < .00001). The postoperative last follow-up local kyphosis angle in the SSF group was greater than that in the LSF group (MD = 3.18, 95% CI [.56, 5.81], z = 2.38, P = .02), and there were no significant differences in perioperative complications, bone cement leakage rate, incidence of adverse events during follow-up, postoperative follow-up visual analog scale, postoperative Oswestry dysfunction index, and postoperative immediate local kyphosis angle between the two groups (P > .05).
Conclusion
SSF and LSF are effective and safe for the treatment of Kummell disease. SSF can reduce the operation time and intraoperative bleeding; LSF can better maintain the long-term stability of kyphosis. The methods should be evaluated by clinicians according to the individual situation of the patients.
Keywords
Introduction
Kummell disease is a complication of osteoporotic vertebral compression fractures (OVCFs). It was first described in 1891, and most researchers believe that Kummell disease is caused by ischemic necrosis secondary to the vertebral body and that vascular damage causes impaired bone healing.1,2 Currently, the treatment strategy for Kummel disease is controversial. For stages I and II of Kummell disease, percutaneous myeloplasty vs vertebroplasty, percutaneous vertebroplasty is an effective and minimally invasive surgical treatment.3,4 In patients with stage III Kummell disease with severe neurological defects or kyphosis, traditional long-segment fixation (LSF) has been widely used. 5 However, this procedure may be associated with severe multiple complications, which are unfavorable for recovery in elderly patients; therefore, short-segment fixation (SSF) can compensate for the deficiency of LSF. 6 Recently, some clinical studies have carefully explored the advantages and disadvantages of the two surgical methods of SSF and LSF for the treatment of Kummell disease. However, due to the small number of cases and the low level of evidence, a unified understanding of the effectiveness and safety of SSF and LSF surgery for Kummell disease is still lacking. Therefore, according to the inclusion and exclusion criteria, we collected the literature comparing the effectiveness and safety of SSF and LSF in Kummell disease, to provide more evidence-based medical evidence support for spine surgeons.
Materials and Methods
Search Strategy
PubMed, the Cochrane Library, Web of Science database, EMBASE, Chinese Biomedical Literature Database, China National Knowledge Infrastructure, VIP, and Wanfang databases were retrieved from relevant studies without language restrictions from their inception dates to November 1, 2021. Papers were retrieved using the title and keywords in the abstract: “Kümmell’s disease” “Kummell disease” “Kümmell disease” “vertebral osteonecrosis” “vertebral pseudarthrosis” “Vertebral Compression Fracture nonunion” “intravertebral vacuum cleft” “delayed vertebral collapse ” “avascular osteonecrosis of vertebral body” “fixation” “instrumentation” “hybrid stabilization” “short segment” “short-segment fixation” “long segment” “long-segment fixation”. For PubMed, as an example, the retrieval formula was:#1 Kümmell’s disease; #2 Kummell disease; #3 vertebral osteonecrosis; #4 vertebral pseudarthrosis; #5 Vertebral Compression Fracture nonunion; #6 intravertebral vacuum cleft; #7 delayed vertebral collapse; #8 avascular osteonecrosis of vertebral body; #9 fixation; #10 instrumentation; #11 hybrid stabilization; #12 short segment; #13 short-segment fixation; #14 long segment; #15 long-segment fixation; #16 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8); #17 (#9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15); #18 (#16 AND #17). To expand the search scope, the computer manually retrieved the relevant references in the literature and tracked the full text.
Inclusion Criteria
1. Type of study: clinical controlled trial, including retrospective cohort study, case-control study. 2. Diagnosis as a single vertebral lesion with Kummell disease. 3. The Chinese and English literature of the original data published in the full text.
Exclusion Criteria
1. Study groups are not defined or no grouping. 2. Non-randomized controlled trial, non-cohort study, non-case-control study, review literature, case reports 3. Repeat studies, animal experiments. 4. Kummell disease in double or multiple segments, osteoporosis vertebral compression fracture, vertebral hemangioma, primary or metastatic fractures 5. Conservative treatment or other surgical methods.
Quality Assessment
Two researchers will retrieve the literature independently by computer and extract the data according to the above inclusion and exclusion standards and observation indicators. The final included literature was used by the Newcastle-Ottawa Quality Assessment Scale (NOQAS) to evaluate the quality of the literature, mainly including sample selection, control, and outcome indicators. The total score is 9 points, and more than 6 points will be regarded as a high-quality study.
Clinical Outcomes
Operation time, intraoperative bleeding, incidence of perioperative complications (such as unplanned operation, surgical incision infection, lung infection, urinary tract infection, etc.), bone cement leakage rate, incidence of adverse events during follow-up (such as adjacent vertebral fracture, screw loosening, internal fixation failure, concurrent neurological symptoms, etc.), visual analog scale (VAS) of preoperative and last follow-up, Oswestry disability index (ODI), and local kyphotic angle (LKA).
Statistical Analysis
The extracted data were statistically analyzed using Review Manager 5.3 software provided by the Cochrane Library Collaborative Network, the heterogeneity of the included data was judged by calculating the I2 values; if I2 < 50% and Q test showed P > .1, which indicates low heterogeneity between the study groups, and a fixed-effects model will be used for the analysis if I2 ≥ 50% and Q test show P ≤ .1, which indicates high heterogeneity between the study groups and a random-effects model will be used for the analysis. The data of declassification variables were analyzed using hazard ratio (HR) and 95% interval (95% confidence interval, 95% CI). For the continuity variables, the weighted mean difference (MD) and the 95% CI were used for the effect size, and the 95% confidence interval was calculated. The difference between the indicators was considered significant if P < .05, after comparison of the indicators examined.
Results
Included Studies
A total of 1131 papers were initially retrieved, and duplicate papers were checked and deleted by EndNote and NoteExpress software (n = 586); 545 documents were excluded after reading titles and abstracts according to the exclusion criteria, and 52 papers were initially included. After reading the full text, seven studies were included for meta-analysis, all of which were publicly published clinical controlled studies, two of which were retrospective case-control studies and five were retrospective cohort studies with 288 patients, including 156 in the SSF group and 132 in the LSF group.7-13 The literature screening process is shown in Figure 1, and the basic information of the included literature is shown in Table 1. Two authors evaluated the quality of the seven included studies according to the NOQAS, from three aspects: case selection, control, and outcome index. Six points and above were high-quality studies. The five retrospective clinical control studies literature scored 6 points, and one study scored 7 points and 8 points, respectively. Flow chart of the literature screening. Basic Characteristics of the Included Studies. SSF: short-segment fixed; LSF: long-segment fixed; A: intraoperative bleeding; B: operation time; C: visual analog scale, VAS; D: local kyphotic angle, LKA; E: Perioperative complications; F: Bone cement leakage rate; G: Incidence of adverse events during follow-up; H: Oswestry disability index, ODI.

Meta-Analysis
Intraoperative Bleeding
Six of the seven included articles showed detailed comparisons of intraoperative bleeding. There was heterogeneity between the literature (Chi2 = 42.88, df = 5, I2 = 88%, P <.00001), and a random effect model was selected for meta-analysis. The amount of intraoperative bleeding in the SSF group was less than that in the LSF group (MD= −82.07, 95% CI [−106.91, −57.24], Z = 6.48, P < .00001) (Figure 2) (Units: milliliters). Forest plot of intraoperative bleeding between the two groups.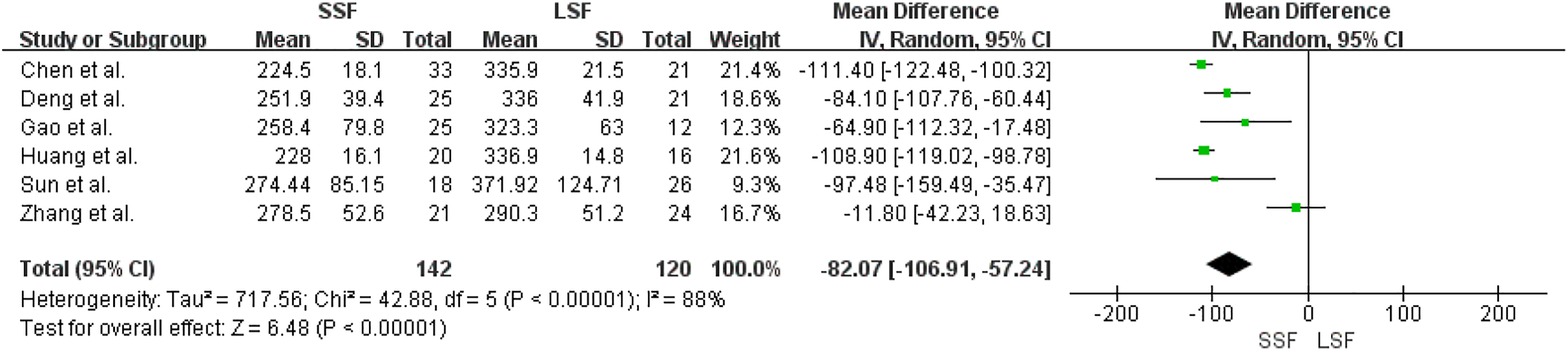
Operation Time
Six of the seven included articles showed detailed comparisons of the operation time. There was heterogeneity between the literature (Chi2 = 194.13, df = 5, I2 = 92%, P < .00001), and a random effect model was selected for meta-analysis. The operation time of the SSF group was shorter than that of the LSF group (MD = −18.17, 95% CI [−30.31, −6.03], Z = 2.93, P = .003), as shown in Figure 3 (Units: minutes). Forest plot of operation time between the two groups.
Incidence of Perioperative Complications
Six of the seven included articles showed a detailed comparison of the incidence of perioperative complications. There was no heterogeneity between the literature (Chi2 = 5.10, df = 5, I2 = 2%, P = .4), and a fixed-effect model was selected for meta-analysis. The incidence of perioperative complications in the SSF and LSF groups was not significantly different (MD = .53, 95% CI [.23, 1.26], Z = 1.44, P = .15), as shown in Figure 4. Forest plot of incidence of perioperative complications between the two groups.
Bone Cement Leakage Rate
Two of the seven included articles showed detailed comparisons of bone cement leakage rates. All included patients were treated with bone cement reinforced screws during vertebral fixation, and there was no heterogeneity between the literature (Chi2 = .78, df = 1, I2 = 0%, P = .38), and a fixed-effect model was selected for meta-analysis. The bone cement leakage rates of the SSF and LSF groups were not significantly different (MD = .73, 95% CI [.31, 1.74], Z = .70, P = .48), as shown in Figure 5. Forest plot of bone cement leakage rate between the two groups.
Incidence of Adverse Events During Follow-Up
Two of the seven included articles showed detailed comparisons of the incidence of adverse events during follow-up, such as adjacent vertebral fracture, screw loosening, internal fixation failure, and concurrent neurological symptoms. There was no heterogeneity between studies (Chi2 = .22, df=1, I2 = 0%, P = .64), and a fixed-effect model was selected for meta-analysis. The incidence of adverse events during follow-up in the SSF and LSF groups was not significantly different (MD = .86,95% CI [.28, 2.59], Z = .27, P = .79), as shown in Figure 6. Forest plot of incidence of adverse events during follow-up between the two groups.
Visual Analog Scale
Seven included articles showed detailed comparisons of the visual analog scale and VAS scores of the preoperative and final follow-up. There was no heterogeneity between preoperative VAS scores in the literature (Chi2 = 1.22, df = 6, I2 = 0%, P = .98), and a fixed-effect model was selected for meta-analysis. There was heterogeneity between the final follow-up VAS of literature (Chi2 = 78.79, df = 6, I2 = 92%, P < .00001), and a random effect model was selected for meta-analysis. There was no significant difference in the preoperative and final follow-up VAS scores between the SSF and LSF groups.[MD = −.15, 95% CI (−.34, .05), Z = 1.49, P = .14; MD = .34, 95% CI (−.14, .81), Z = 1.39, P = .17], as shown in Figure 7. Forest plot of VAS between the two groups. (A) Preoperative VAS score comparison; (B) Final follow-up VAS score comparison. VAS: visual analog scale.
Oswestry Disability Index
Six of the seven included articles showed detailed comparisons of the Oswestry Disability Index and ODI of the preoperative and final follow-up. There was no heterogeneity between the preoperative ODI of the literature (Chi2 = 4.54, df = 5, I2 = 0%, P = .47), and a fixed-effect model was selected for meta-analysis. There was heterogeneity between the final follow-up ODI of the literature (Chi2 = 48.03, df = 5, I2 = 98%, P < .00001), and a random effect model was selected for meta-analysis. There was no significant difference in the preoperative and final follow-up ODI between the SSF and LSF groups [MD = 1.63, 95% CI (−4.00, 7.26), Z = .70, P = .48; MD = .54, 95% CI (−.97, 2.06), Z = .57, P = .57], as shown in Figure 8. Forest plot of ODI between the two groups. (A) The preoperative ODI comparison; (B) The final follow-up ODI comparison. ODI: Oswestry disability index.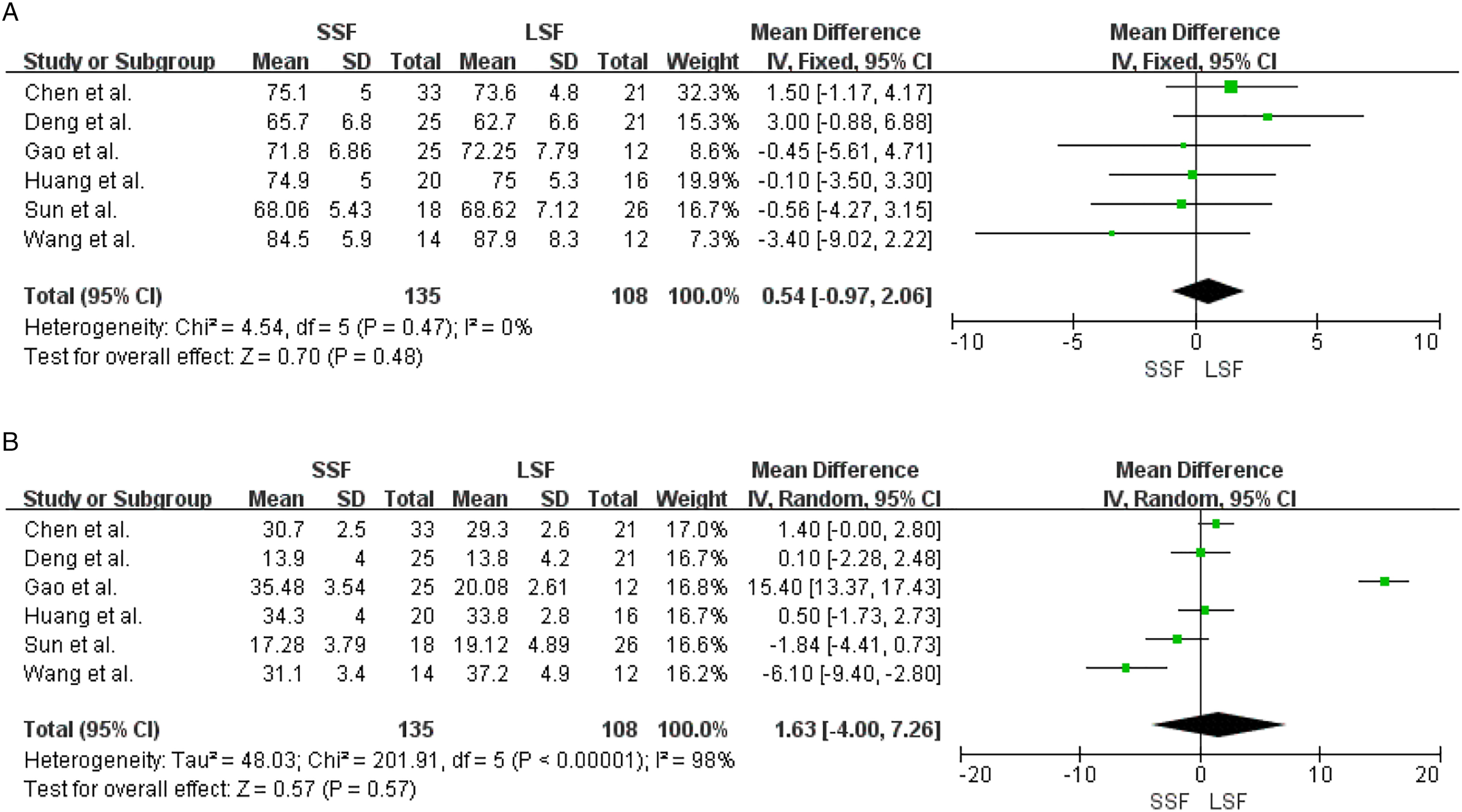
Local Kyphotic Angle
Seven included studies showed a detailed comparison of preoperative, postoperative, and final follow-up LKA, and there was heterogeneity between the preoperative LKA of literature (Chi2 = 172.64, df = 6, I2 = 97%, P <.00001), and a random effect model was selected for meta-analysis. There was heterogeneity between the postoperative LKA of literature (Chi2 = 14.78, df = 6, I2 = 59%, P = .02), and a random effect model was selected for meta-analysis. There was no significant difference in preoperative and final follow-up LKA between the SSF and LSF groups.[MD = −4.04, 95% CI (−9.71, 1.63), Z = 1.40, P = .16; MD = .39, 95% CI (−.34, 1.13), Z = 1.05, P = .29]. There was heterogeneity between the final follow-up LKA of the literature (Chi2 = 11.81, df = 6, I2 = 96%, P < .00001), and a random effect model was selected for meta-analysis. The final follow-up LKA in the SSF group was greater than that in the LSF group [MD = 3.18; 95% CI (.56, 5.81), Z = 2.38, P = .02], as shown in Figure 9. Forest plot of LKA between the two groups. (A) Preoperative LKA comparison; (B) Postoperative LKA comparison; (C) Final follow-up LKA comparison. LKA: local kyphotic angle.
Discussion
Previous contributions and limitations of other studies in SSF and LSF treatment of Kummel disease
Kummell disease is a complication of OVCF caused by some reasons such as reduced bone formation, disc degeneration, microfracture, brittle fractures, insufficient vertebral blood supply, and pseudo joint formation etc.1,2,14-16 Usually, the diagnosis of Kummell disease is based on a vacuum fissure sign in the vertebral body, and the involved vertebrae show an abnormal increase in vertebral activity range and vertebral collapse, which is more obvious when the spine is hyperextended.17,18 Patients with stage I and II Kummell disease had no neurological symptoms. Therefore, the treatment purpose of patients at this stage is to reduce the hyperactivity of the fractured vertebral body and reconstruct the stability of the spine. 19 Patients with stage III Kummell disease have severe vertebral collapse, kyphosis, spinal canal stenosis, and osteoporosis. The use of bone cement-reinforced fixation and internal fixation can reconstruct the stability of the injured vertebrae and provide rapid analgesia.4,20,21 It is considered to be a reasonable surgical method for the treatment of this type of disease; however, there are many studies on the selection of the length of internal fixation segments, and there is no unified opinion on their effectiveness and safety.
Zhang et al 22 showed that posterior SSF combined with vertebroplasty is an effective method for the treatment of Kummel disease with neurological deficits. Park et al. 23 conducted a prospective study of 10 patients with single-segment Kummell disease with severe osteoporosis. He adopted the treatment scheme of bone cement-reinforced percutaneous SSF for all patients and considered that the operation scheme is a safe and effective method for the treatment of Kummell disease. Zhang et al treated 12 cases of Kummel disease with neurological deficits. They underwent modified transpedicular subtraction and disc osteotomy combined with LSF. As a result, all cases successfully corrected kyphosis and achieved solid fusion. The neurological function of nine patients improved to varying degrees. 24 Huang et al studied 36 patients with Kummel disease treated with long-term or bone cement-augmented SSF. The results showed that compared with LSF, BCASSF had lower bleeding volume and shorter hospital stay; The two techniques have similar clinical results and imaging findings. 13 However, a study by Zhu et al. demonstrated that LSF was effective in the treatment of advanced Kummell disease and was beneficial for the recovery of vertebral body height. 25 Therefore, doctors often choose the length of spinal fixation segments according to the patient’s situation and personal habits, and there is a lack of evidence-based medical evidence for the effectiveness and safety of these treatment methods.
Efficacy and Safety of Posterior Short-Segment Fixation and Long-Segment Fixation in the Treatment of Kummell Disease
From the perspective of biomechanics, the longer the fixed segment, the more dispersed the stress, and the stronger the stability of the internal fixation.26,27 However, due to the generally older age of patients with Kummell disease, the longer the spinal segment of internal fixation, the greater the impact on the operation safety of patients, and the corresponding operation cost also increases. Chinese scholars have proposed that the indications of short segment enhanced fixation combined with vertebroplasty in the treatment of stage III Kummell disease include: (1) Local kyphotic angle ≤40°; (2) The course of disease >3 months, and the patient tolerated the operation; (3) Only single segment vertebral body was involved; (4) When changing posture, the pain is aggravated and there is spinal instability. 7 Currently, there is a lack of literature on the long and SSF of Kummell disease. In a comparative study of LSF and SSF in the treatment of tuberculosis, it is considered that although the operation time and bleeding volume of the long segment are increased, it has advantages in kyphosis correction and maintenance of spinal stability. 28 Our study showed that the SSF group had more advantages than the LSF, in terms of intraoperative bleeding and operation time, but there was no significant difference in perioperative complications, postoperative VAS score, ODI index, and immediate postoperative LKA, which also proves that the two surgical methods are safe. Of course, this situation occurs when the surgeon is proficient in surgical methods. 29 However, in long-term follow-up, LSF shows excellent biomechanical advantages. For the maintenance of the local kyphosis angle, many scholars also believe that long-segment spinal internal fixation has more advantages.24,30 Our study showed that LSF was more effective in maintaining spinal stability than SSF at the last follow-up.
For some patients with severe osteoporosis, in addition to nail rod system fixation, many studies have also used bone cement reinforcement. Therefore, there is a certain risk of bone cement leakage during LSF and SSF.13,31 However, the probability of leakage has been controversial because of the small amount of bone cement annotation of reinforced pedicle screws. 32 As the reinforced pedicle screws do not damage the anterior wall of the spinal cone, the probability of bone cement leakage is very low, and it can effectively prevent screw loosening after internal fixation.33-35 Three of the studies we included compared the safety of long and short segments by reinforced pedicle screw fixation in the treatment of Kummell disease. The current meta-analysis results showed that there was no significant difference in postoperative bone cement leakage and postoperative screw loosening between LSF and SSF.
Therefore, in the selection of treatment options for Kummell disease, our meta-analysis results suggest that LSF and SSF are both safe and effective, but long segmental fixation has more advantages in the maintenance of long-term kyphosis and spinal biomechanical stability, which is consistent with some previous research results.36,37 Our results also suggest that LSF may be a more effective method for the treatment of patients with Kummell disease with severe kyphosis.
Limitations of this Meta-Analysis
The limitations of the study are that: (1) Among the seven studies included, there are few high-quality clinical control research articles and lack of prospective research, which inevitably leads to publication bias and selection bias; (2) the number of included cases is small, only 288 patients, which is far from the large sample and multi-center data required in the statistical analysis of evidence-based medicine; (3) there are differences in the age and disease stage of the included patients, and there is some heterogeneity among the studies; (4) It is difficult to grasp the implementation details of each study, such as whether the patients were assisted with bone grafting, the proficiency of doctors, and the authenticity and integrity of medical records. Therefore, it is difficult to accurately evaluate the effectiveness and safety of different surgical methods; therefore, the conclusions of this meta-analysis should be treated strictly.
Conclusion
The results of a meta-analysis of seven studies showed that SSF has significant advantages in reducing intraoperative bleeding and shortening operation time in the treatment of Kummell disease. LSF has the advantage of correcting long-term kyphosis in patients. Therefore, based on the analysis of the current literature statistical data, it is concluded that SSF and LSF are effective and safe for the treatment of Kummell disease. The specific operation methods of the two groups have their advantages and disadvantages, which need to be selected by clinicians according to the individual situation of the patients. Due to the limited number and quality of the included studies, the above conclusions need to be verified by more high-quality studies.
Footnotes
Author Contributions
Yikang Yu and Hanbing Zeng drafted the manuscript, Enpin Guo, Binbin Tang and Yuan Fang were responsible for document retrieval and data processing, Lianguo Wu and Chao Xu Chao were responsible for checking the included indicators and provided project guarantee for the research, Yi Peng, Bin Zhang and Zhen Liu processed the charts and figures.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Special project for the modernization of traditional Chinese medicine in Zhejiang Province in 2021 (NO.2021ZX009), General Research Project of Zhejiang Education Department (NO.Y202044448) and supporting discipline of national clinical research base of traditional Chinese medicine (prevention and treatment of osteoarthropathy with integrated traditional Chinese and Western Medicine).
Data Availability
All data generated or analysed during this study are included in this published article.