
Abstract
Introduction
This study aimed to investigate factors related to fat infiltration in patients with lumbar degenerative diseases (lumbar disc herniation and/or spinal stenosis), examining a wide range of potential risk variables.
Materials and methods
We studied consecutive adult patients who underwent posterior lumbar spinal surgery for degenerative diseases at our hospital between July 2013 and June 2017. Preoperative magnetic resonance imaging was used to evaluate the presence or absence of fat infiltration at the level of the L4-5 lumbar paraspinal muscles using Kjaer’s evaluation method. Patients without fat infiltration (0%–10%) were rated as grade 0, grade 1 for moderate fat infiltration (10%–50%), and grade 2 for severe fat infiltration (>50%). Patients were then divided into two groups: Group A (without fat infiltration, grade 0) and Group B (with fat infiltration, grade 1 or 2). Detailed patient clinical data were collected and analyzed.
Results
A total of 205 consecutive patients were enrolled; 54 (26.3%) patients were assigned to Group A and 151 (73.7%) to Group B. Logistic regression analysis revealed two independent risk factors for fat infiltration of the lumbar paraspinal muscles: female sex and older age (P < .001).
Discussion
Fat infiltration of the lumbar paraspinal muscles is reported to be associated with the development of pain and dysfunction of the lumbar region and postoperative complications of spinal instrumented fusion surgery. To the best of our knowledge, no previous studies have identified female sex and older age as independent risk factors for fat infiltration in the lumbar paraspinal muscles using multivariate analysis.
Conclusions
Female sex and older age were independent risk factors for fat infiltration in the lumbar paraspinal muscles. The results of the current study may provide useful information for the study of preventive measures for fat infiltration.
Introduction
Between the ages of 70 and 80 years, a 20%–40% loss of muscle strength due to age-related muscle weakness has been reported. 1 Lower back pain is a very prevalent clinical symptom and is reported to affect 65%–85% of the population throughout the life of humans. 2 Additionally, it has been reported that lumbar pain is related to the degeneration of the paraspinal muscles of the trunk, which is often seen in daily clinical settings.3-5
In the recent years, skeletal muscle research has been attracting attention not only in terms of muscle strength and muscle volume, but also in terms of the qualitative evaluation of intramuscular fat infiltration. Muscle strength and fat infiltration are important factors in the field of rehabilitation related to activities of daily living and physical activities. Loss of muscle volume causes poor physical performance, and qualitative changes in muscle due to fat infiltration also have a negative correlation with muscle strength;6,7 preliminary detection of lumbar fat infiltration may be useful in planning rehabilitation programs and patient education. Previous studies have shown that a loss of muscle volume is associated with reduced functional performance 8 and self-reported disability.9,10 Furthermore, fat infiltration of the paraspinal muscles is related to lower back pain,11,12 which is affected by aging. 13 In addition, lower back pain is known to be associated with lumbar function. 14 Several studies have also reported that patients with acute or chronic lower back pain had smaller paraspinal muscles than healthy participants.15-17
Fat infiltration of the lumbar paraspinal muscles is related to lower back pain, 11 and patients with lower back pain showed significantly more fat infiltration of the paraspinal muscles than healthy participants.12,18 In addition, it has been reported that dysfunction of the lumbar region causes pain and eventually leads to fat infiltration.19,20 Moreover, several studies described that fat infiltration of the paraspinal muscles is associated with postoperative complications of lumbar spinal surgery, such as bone nonunion, pedicle screw loosening, and proximal junctional kyphosis.21-24
Muscle fat infiltration is assessed using ultrasound, 25 computed tomography, 19 magnetic resonance imaging (MRI),11,14,26 and magnetic resonance spectroscopy.11,27 Among them, Kjaer et al 28 have reported a method of grading the degree of fat infiltration using MRI, 28 which is used in clinical settings.14,29,30 The method of Kjaer et al 28 is considered to be a useful method for both medical doctors and physiotherapists to evaluate fat infiltration, including that of the lumbar paraspinal muscles. 31
The purpose of this study was to clarify the risk factors for fat infiltration of the lumbar paraspinal muscles using MRI. If the risk factors for fat infiltration of the lumbar paraspinal muscles are clarified, they could be helpful in preventing fat infiltration, back pain, and performance deterioration.
Materials and Methods
Data Source
We retrospectively investigated the clinical data of adult patients (≥18 years) who had undergone posterior lumbar spinal surgery (laminectomy, herniotomy, and/or instrumented fusion) for lumbar degenerative diseases (lumbar herniated disc and/or spinal stenosis) from July 2013 to June 2017 at the division of orthopedic surgery of our hospital. The current study conforms to the principles laid down in the Declaration of Helsinki and its amendments. This study was approved by the Institutional Review Board of our Medical University.
Exclusion Criteria
Patients who underwent revision lumbar surgical procedures were excluded from the current study. We also excluded patients aged <18 years and those who underwent percutaneous vertebroplasty and removal of posterior spinal instrumentation for homogeneity of the study group.
Fat Infiltration on MRI
The patients’ MRI preoperatively performed for the medical diagnostic procedure was used for radiological evaluation in the current study. We used patients’ axial T2-weighted MR images at the level of L4-5 to evaluate fat infiltration of the lumbar multifidus muscles. In the present analysis, preoperative MRI of all enrolled patients was evaluated by two examiners.
According to the criteria proposed by Kjaer et al,
28
fat infiltration in the lumbar paraspinal muscles was visually evaluated and assigned to either of the three grades: grade 0 (0%–10% fat infiltration), grade 1 (10%–50% fat infiltration), and grade 2 (>50% fat infiltration) (Figure 1). The patients were then assigned to two groups: Group A (without fat infiltration: Kjaer grade 0) and Group B (with fat infiltration: Kjaer grade 1 or 2). The grading method of L4/5 fat infiltration on T2-weighted magnetic resonance imaging used in this study. Fat infiltration rated as (A) grade 0 in the absence of fatty degeneration (0%–10%), (B) grade 1 in the case of slight fat infiltration (10%–50%), and (C) grade 2 in the case of severe fat infiltration (>50%).
Data Collection
We retrospectively reviewed patient clinical characteristics including age at the time of surgery, sex, body mass index, smoking status, diabetes, hemodialysis, American Society of Anesthesiologists physical status (ASA) score,
32
preoperative oral administration of steroids, motor paralysis in the lower extremities, disease duration with physical symptoms (months), bladder bowel dysfunction, and L1-5 lumbar lordotic angle (degrees). The lumbar lordotic angle was measured as the angle of intersection between the upper edge of the L1 vertebra and the lower edge of the L5 vertebra using lateral plain radiographs of the lumbar spine (Figure 2). Measurement of the lumbar lordotic angle. According to Cobb’s method, tangent lines are drawn along the superior end plate of L1 and inferior end plate of L5 using a lateral plain radiograph.
Statistical Analysis
We analyzed the relationships between the absence or existence of fat infiltration of the lumbar paraspinal muscles (Group A or B) and patients’ clinical variables. Statistical analysis was performed using the χ2 test and the Mann–Whitney U test in the univariate analysis. The significant variables and the variables that were correlated (P < .2) with the existence of fat infiltration of the lumbar paraspinal muscles (Group A or B) in the univariate analysis were entered into a stepwise multiple logistic regression model. Data were analyzed using SPSS version 25.0 (IBM Japan, Tokyo, Japan). Statistical significance was set at P < .05.
Results
Univariate Analysis of the Groups Without Fat Infiltration and With Fat Infiltration.
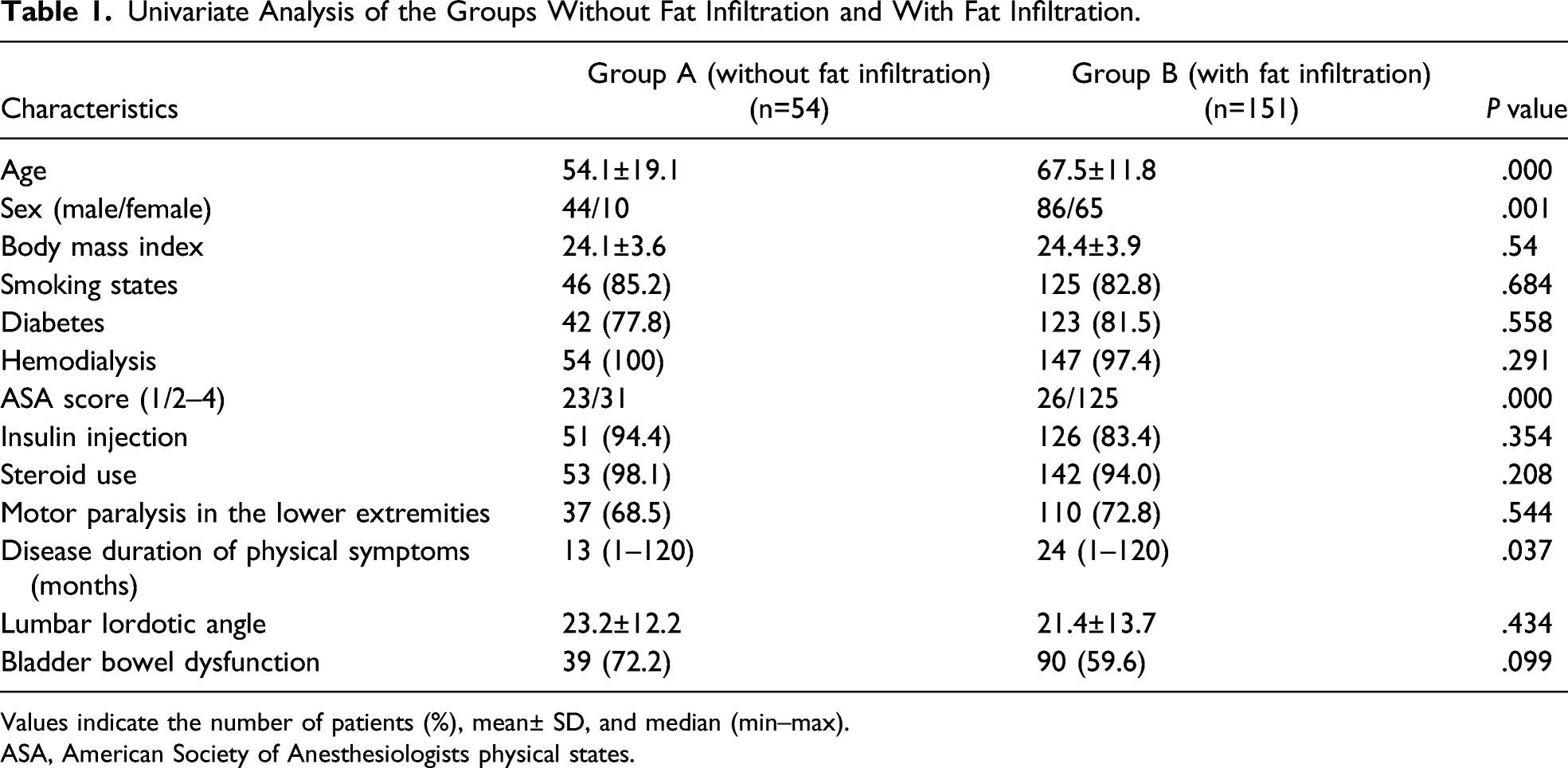
Values indicate the number of patients (%), mean± SD, and median (min–max).
ASA, American Society of Anesthesiologists physical states.
Multivariate Logistic Regression Analysis Comparing With and Without Fat Infiltration Groups.
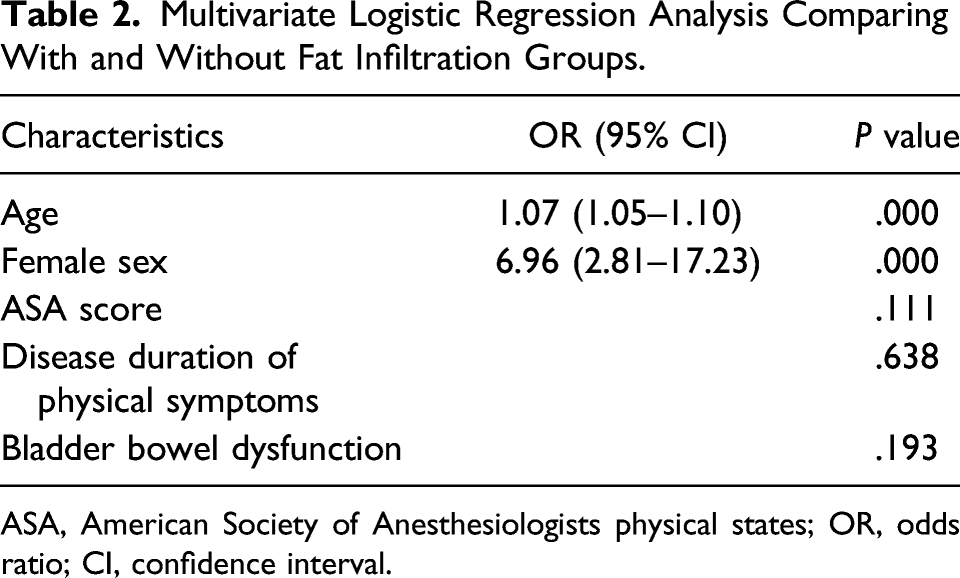
ASA, American Society of Anesthesiologists physical states; OR, odds ratio; CI, confidence interval.
Discussion
We investigated factors related to lumbar paraspinal muscle fat infiltration in patients with lumbar degenerative diseases. In the current study using multivariate analysis, female sex and older age were strongly and independently associated with the risk of fat infiltration in the lumbar paraspinal muscles. Several studies have described the association of fat infiltration of the lumbar paraspinal muscles with female sex and/or older age in univariate analysis.28,33,34 To the best of our knowledge, no previous studies have identified female sex and older age as independent risk factors for fat infiltration in the lumbar paraspinal muscles using multivariate analysis.
Regarding lumbar spinal surgery, fat infiltration of the paraspinal muscles has been reported to be related to the development of postoperative complications.21-24 Lee et al. described that the bone union rate decreased as the fat content of lumbar paraspinal muscles increased in patients with spinal degenerative diseases after instrumentation fusion. 22 Kim et al. reported that preoperative higher fat infiltration of the paraspinal muscles was significantly associated with pedicle screw loosening. 23 In addition, Hyun et al. investigated patients who received multilevel spinal instrumented fusion surgery stopping at the thoracolumbar junction for adult spinal deformity, and described that higher fat infiltration of the paraspinal muscles was identified as a risk factor for proximal junctional kyphosis. 24 Even in the presence of a high degree of fat infiltration of the paraspinal muscles, surgical intervention for the lumbar spine should be considered if severe pain and/or serious neurological symptoms, such as the cauda equina syndrome, are noted. Routine preoperative measurement of fat infiltration of the paraspinal muscles can be helpful for spinal surgeons to recognize the risk of postoperative complications, especially in instrumented fusion procedures.
In Fat infiltration in skeletal muscles is found not only in the lumbar spine35,36 but also in the shoulder joints, thighs, and lower leg muscles.37-42 In the shoulder joint, fat infiltration of the rotator cuff is known to affect postoperative clinical results, pain, and range of motion.37,38 Regarding the lower extremities, it has been reported that the amount of fat in the skeletal muscles of the thighs and calves increases when the level of physical activity decreases, and it has been pointed out that the lack of exercise is associated with fat infiltration. 39 In addition, it has been reported that an increase in the intramuscular fat volume of the quadriceps femoris and vastus medialis muscles was associated with the risk of progression of knee osteoarthritis by MRI;40,41 not only the muscle strength of the quadriceps femoris but also qualitative changes, such as fat infiltration, affect the extension of the knee joint. 42
Similar to the shoulder joint, fat infiltration in the musculoskeletal system has a negative effect on physical function. In the current study, because the participants were patients who underwent lumbar surgery for spinal degenerative diseases with neurological symptoms, patients with sarcopenia and dynapenia associated with hypoactivity due to lumbar degenerative diseases may also be included. In individuals with sarcopenia and dynapenia, fat infiltration in the skeletal muscles tends to increase and is associated with muscle weakness and motor dysfunction.43,44 As described above, systemic fat infiltration is a structural problem that affects physical function, and it is considered that the prevention of systemic fat infiltration is important to improve and avoid deterioration of muscle strength and physical function in the lumbar spine.
It has been reported that exercise therapy, such as resistance training and aerobic exercise,35,36,45 and diet therapy, such as taking beta-hydroxy-beta-methylbutyrate and vitamin D,46,47 are advantageous for the prevention of fat infiltration in the skeletal muscles. Additionally, it has been reported that the combined use of exercise therapy and protein intake leads to the suppression of skeletal muscle fat infiltration. 48 Welch et al reported that lumbar paraspinal muscle fat infiltration was significantly reduced following free-weight resistance training, 35 and Ryan and Harduarsingh-Permaul described that a lifestyle modification of diet-induced weight loss alone or with aerobic exercise training resulted in a significant reduction of the fat infiltration of the abdominal and spinal muscles of the trunk region. 36 Accordingly, active physical exercise therapy and/or curative intervention for neurological dysfunction due to lumbar degenerative diseases may be useful for the prevention of fat infiltration in the lumbar paraspinal muscles from an early stage of lumbar degeneration, especially in women.
In contrast, the ASA score, which is thought to be associated with hypoactivity, disease duration of physical symptoms, and lumbar lordotic angle, which are thought to be affected by muscle contraction, was not significantly associated as independent risk factors for fat infiltration in this multivariate analysis. Since the patients included in the current study were scheduled to undergo spinal surgery, it is speculated that there may have been a bias that patients with particularly poor ASA scores (poor general conditions) were less likely to be indicated for surgery because of the risk of general anesthesia; therefore, they were likely to be excluded from the study. As for the disease duration with physical symptoms, the severity of the disease (lumbar disc herniation and/or spinal stenosis) was not investigated, and we could not evaluate how the patients’ physical disability and severity of body pain were affected by the duration of physical symptoms. Regarding the lumbar lordotic angle, it has been reported that lumbar kyphosis was associated with back muscle weakness, 49 and patients with larger lumbar kyphosis have higher spinal muscle dystrophy and fat infiltration compared to healthy participants. 50 However, this study does not support the findings of previous studies.
The limitation of this study is that, since the participants were surgical patients comprising several elderly patients with highly degenerated lumbar spines, our study population may be biased compared to a normal healthy population. We did not collect data about preoperative symptoms, surgical outcomes, and postoperative complications in the current study; therefore, we did not acquire results about surgical outcomes or criteria for preoperative patient selection in relation to fat infiltration of the paraspinal muscles. In addition, we have no clinical data that prove that preoperative exercise can reduce fat infiltration of the paraspinal muscles. The strength of this study is that it analyzed data from a relatively large number of patients. Moreover, the fact that detailed medical information was available because the participants of the current study were patients who underwent lumbar surgery and the fact that various potentially risk-related factors could be reviewed were considered to be the advantages of the current study.
Conclusion
The current study revealed that lumbar paraspinal muscle fat infiltration is more likely to occur in women and older people, with statistical significance in adults undergoing elective lumbar spinal surgery. The results of the current study may provide useful information for the development of preventive measures for fat infiltration.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research ethics and patient consent
The present research conforms to the principles laid down in the Declaration of Helsinki and its amendments. This research was approved by the institutional review board of Saitama Medical Center, Saitama Medical University (No. 1969-II). Because of the retrospective nature of this study, the requirement for written informed consent was waived by the institutional review board. Information on opt-out was posted on the website of Saitama Medical Center, Saitama Medical University.