
Abstract
Introduction
Corneal abrasion (CA) is the most common ocular complication in patients undergoing nonocular surgery. Corneal abrasions can be caused by a variety of mechanisms, the most common being drying of the cornea due to reduced tear secretions, loss of eyelid reflex, and the loss of pain recognition during surgery. Though CA heals well with eye lubricants, it can result in significant ocular pain and some cases may go on to develop ocular complications. With the current switch to outpatient total joint replacement, CA could potentially lead to discharge delays.
Materials and Methods
We examined the results of a quality improvement project to reduce CA during general anesthesia to determine the rates of CA during hip and knee total joint replacement. We compared rates of CA for 6 months before and 6 months after the intervention.
Results
A total of 670 hip and knee arthroplasty procedures were performed during this period. Two events of CA occurred, one occurred before and one after the intervention to decrease eye injuries. Both incidences occurred during total hip arthroplasty (THA) procedures with the patient in the lateral decubitus position and recovered without long-term deficit.
Discussion
Surgeons and anesthesiologists alike should be cognizant of this avoidable complication and take precaution to protect the eyes during surgery, especially during THA when the patient is placed in the lateral decubitus position.
Conclusion
Corneal abrasion during total joint arthroplasty is a rare complication and is infrequently addressed in the literature. CA is mostly self-limiting, however, but may lead to patient dissatisfaction and to delays if same-day discharge is attempted. Preventative measures and attentive care may help reduce the incidence of CA in patients undergoing total joint arthroplasty. The lateral decubitus position and longer surgeries times are risk factors for CA.
Introduction
Corneal abrasion (CA) is a condition where the epithelial layer of the cornea is removed from the underlying basement membrane, leading to a defect in the corneal epithelial surface. 1 Although most corneal abrasions heal without significant long-term complications, the patient can experience intense discomfort, tearing, photophobia, and blurred vision in the affected eye. 2 Although rare, CA may result in ocular complications such as persistent corneal defect, corneal infection, and recurrent erosions. 3 CA is the most common ophthalmic complication to occur under general anesthesia (GA).2-5 In a time where enhanced recovery after anesthesia (ERAS) protocols are employed to expedite recovery, this can potentially limit early mobilization. Current literature reports the incidence of CA to range between 0.013% and 0.17% for nonocular surgeries.1,3-9 The American Society of Anesthesiologists closed-claims analysis found that perioperative CA was the single most common of all perioperative ophthalmic injuries. 6 While relatively benign, injuries such as this may lead to delays in discharge from the hospital due to the need for ophthalmology consultation and management and a halt in ERAS protocols and increased treatment costs. It can also result in a decrease in patient satisfaction surrounding the hospital stay.
Lateral and prone positioning in surgery have been previously implicated in corneal abrasion events.1,2,5,7,10 The literature reports incidents of corneal abrasions in nonocular surgeries, specifically spine and cardiac surgeries.7,11 There is a paucity of literature on the incidence of CA in orthopedic surgery, specifically total joint arthroplasty (TJA). Here, we present a report of two patients who sustained perioperative CA injury during TJA surgeries performed in the lateral decubitus position. We also sought to review the literature on eye CA and other important injuries during joint replacement to give surgeons guidance to prevent these injuries.
Materials and Methods
After obtaining Institutional Review Board approval, the results for a quality improvement program instituted by the Department of Ophthalmology at our institution were reviewed. The protocol was implemented on August 14, 2018 to reduce general anesthesia associated CA. Prior to the interdepartmental protocol implementation, no specific protection protocol was in place. During this period, it was the decision of the anesthesia provider and/or surgeon whether paper tape, plastic tape, lubricant, or no protection during surgery was used. When enacted, the introduced protocol for eye protection consisted of several different methods to protect the eyes during surgery. The anesthesia provider used carboxymethylcellulose sodium 0.5% (Refresh Plus) lubricant eye drops as artificial tears to promote epithelial repair and provide relief from discomfort. The artificial tears were placed after induction and then the eyes were sealed. Tegaderm transparent film (3M, St Paul, MN) is a bio-occlusive dressing used to cover the eyes during GA. This dressing is transparent, waterproof, and has a hypoallergenic adhesive that gently adheres to the skin and provides a barrier to external contaminants. Tegaderm™ was chosen based on the literature indicating that bio-occlusive dressings provide the most consistent protection.
12
The full eye protection protocol can be seen in Figure 1. Image of implemented eye protection protocol using artificial eye drops and hypoallergenic, bio-occlusive dressing.
We assessed the effect of this intervention on patients undergoing joint replacement. A pre-intervention time period from March 1, 2018 through June 30, 2018 was compared to a postimplementation period from August 14, 2018 to February 28, 2019. CA cases were identified by searching for a diagnosis of CA or ophthalmology consultation. There were 6506 total non-ophthalmic GA cases with 25 CA occurrences during the pre-intervention time period (0.38% total incidence rate).
Of this total cohort, 670 consecutive patients underwent TJA surgery between March 2018 and February of 2019. We included both primary, aseptic and septic (resections and reimplantation) revision hip and knee TJA cases from our single academic tertiary care referral center. All patients underwent general anesthesia for their surgery. We obtained variables pertaining to gender, race, age, patient positioning, surgery type, length of procedure, anesthesia provider type (resident vs nurse anesthetist), and medical comorbidities including smoking and diabetes. We used Excel (Microsoft, Redmond, WA) for descriptive data analysis.
Results
Over the timeframe from March 1, 2018 to February 28, 2019, a total of 15 375 nonocular surgical patients were followed at our institution. Twenty-five CA consultations were documented during the preintervention time period, and 4 CA consultations were documented during the post-intervention time period. There were 670 orthopedic total joint cases identified from the total 15 375 nonocular cases. Out of the 670, 173 (25.8%) were primary total knee arthroplasty, 164 (24.5%) were primary total hip arthroplasty, 99 (14.8%) were revision total knee arthroplasty, 87 (13.0%) were revision total hip arthroplasty, 21 (3.1%) were total knee resections, 35 (5.2%) were total knee reimplantations, 29 (4.3%) were total hip resections, 26 (3.9%) were total hip reimplantations, 18 (2.7%) were hip hemiarthroplasty, 10 (1.5%) were conversion total hip arthroplasty, 4 (0.6%) were unicondylar knee arthroplasty, 3 (0.4%) were one component hip revision arthroplasty, and 1 (0.1%) unicondylar conversion to total knee arthroplasty. The mean age of the patients was 63 years with a range from 19 to 85. There were 289 male patients (43.1%) and 381 female patients (56.9%). Two CA incidents were observed out of the 670 cases (0.30%) during the entire study period. One of the CA incidents was before the protocol was implemented, and one was after the protocol went into effect.
Total Joint Arthroplasty Associated Corneal Abrasion Incidents.
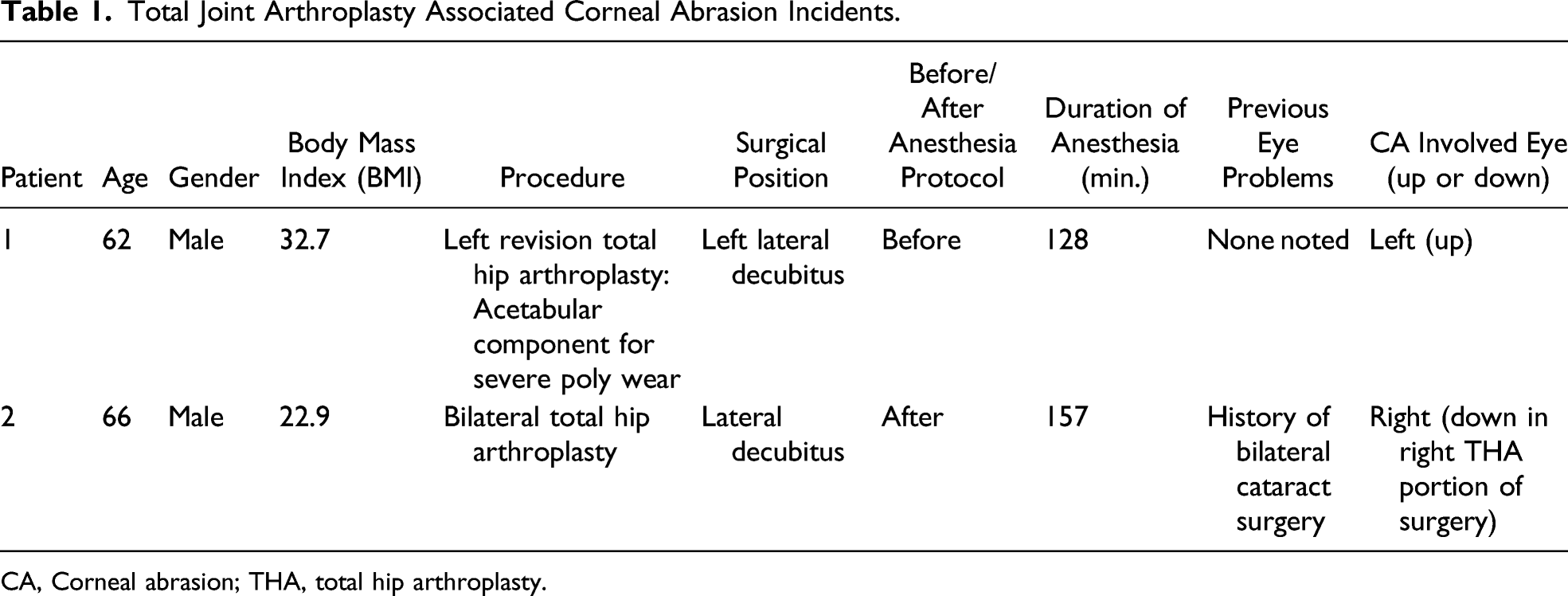
CA, Corneal abrasion; THA, total hip arthroplasty.
Discussion
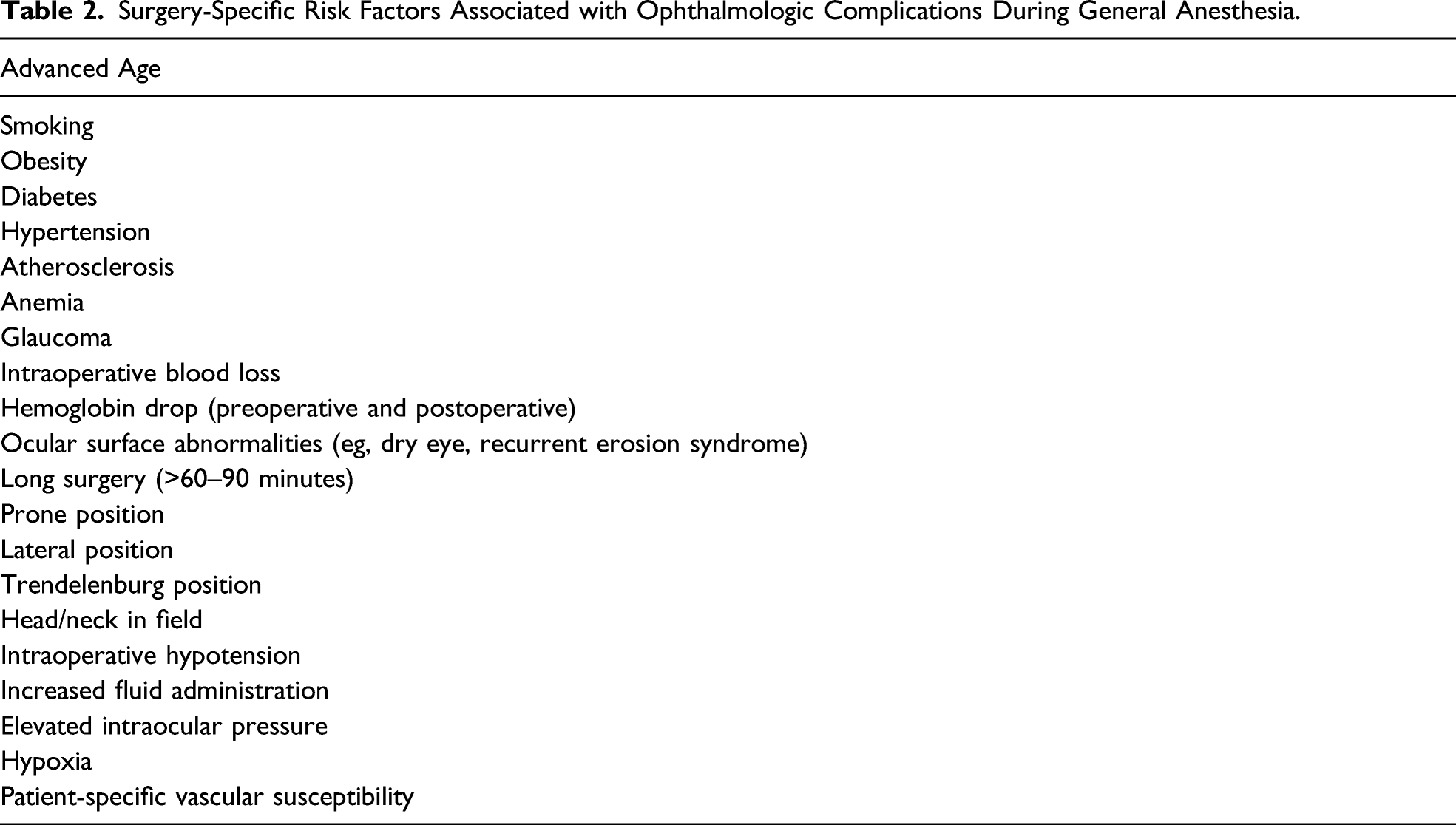
Surgery-Specific Risk Factors Associated with Ophthalmologic Complications During General Anesthesia.

Careful attention is required by the surgeon and anesthesiologist during the perioperative period to avoid inadvertent CA. Incomplete lid closure exposes the epithelial surface, making it prone to drying. Patients should have eyelids secured in the closed position directly after induction. Direct trauma is also believed to account for a minority of CA cases. Segal et al 3 found oxygen face mask use during transport and recovery to be a significant risk factor. It is recommended that a patient’s eyes should be taped shut immediately after anesthesia induction for protection except during rapid sequence intubation. 10 Horizontal eyelid taping is recommended for complete closure, allowing for proper positioning of upper and lower eyelids. 12 A strip of surgical tape is normally sufficient to maintain eyelid closure; however, high-risks cases may benefit from the use of transparent bio-occlusive dressings, such as Tegaderm (3M, St Paul, Minn.) or OpSite (Smith & Nephew, Largo, Fla.), 7 which can span the entire eyelid to provide a uniform closure. 2 The tape can become difficult to stick to the skin if lubrication gets onto the tape.2,12 Also CA can occur as a result of contact of the adhesive tape with the cornea or from the edges of the tape. 1 Specific preventative protocols, using artificial tears and bio-occlusive dressing application as in our study, are thought to decrease the risk of injury.4,12 Prevention of CA is enhanced when all participating providers are educated and involved in eye care. 2 In our series while a protocol for decreasing ophthalmological injury decreased rates of CA overall, this was not the case for TJA procedures. One case was before the protocol and the other after it was instituted. Further work will be required with larger numbers to better evaluate the usefulness of these CA protection protocols in the context of hip and knee surgery.
Both of our cases were hip procedures in the lateral position. We did not have a CA during knee replacement or with a supine positioned hip replacement. This could be a possible advantage of an anterior hip replacement.
Timely detection of CA is key for successful treatment. CA commonly resolves quickly due to the self-regenerating corneal epithelial cells.1,3 Complications that can occur from CA include infectious ulcers, persistent epithelial defects, scarring, or recurrent CA.1,2 With uncomplicated wound healing, discomfort from CA improves significantly after the first 24 hours and is usually resolved after 48 hours. 2 Most corneal abrasions can be treated with lubricants eye drops or antibiotic ophthalmic ointments.1-3 Both CA incidents reported here were discharged from the hospital with erythromycin ointment after an ophthalmology consult. Patching of the eye does not speed healing and is seldom required. 17
In our 2 cases, CA did not lead to a delay in discharge of the patient. Both were discharged home the following day after surgery as per our standard rapid recovery protocol. As same-day discharge for TJA becomes more common, delays in discharge are very important to prevent. 18 Longer surgeries and those in the lateral position may add to this particular risk during surgery. Care to avoid CA is important to allow for a successful outpatient TJA experience.
In addition to CA, other ocular complications have been reported after orthopedic procedures including ischemic optic neuropathy (ION), central retinal artery occlusion (CRAO), and cortical blindness (CB).11,19-26 Ischemic optic neuropathy (ION) is divided into 2 subtypes: anterior (AION) and posterior (PION). ION, thought to arise from hypoperfusion of the posterior ciliary arteries supplying the optic nerve, has been previously reported in TJA.19,23 Prone and Trendelenburg positioning during surgery can increase intraocular pressure, causing ophthalmic vein congestion leading to ION. 24 Additionally, hypotension, blood loss, lengthy surgery, and patient-specific factors may predispose to decreased oxygen delivery to the optic nerve leading to ischemic injury. 25 Perioperative visual loss (POVL) in non-ocular surgery is most frequently caused by an ION, often bilateral.20,24 Shen et al 11 reported an ION prevalence of 0.004% after hip surgery. One study reported sequential episodes of right AION following uncomplicated hip operations performed in the lateral decubitus position. 23 Patients and physicians should be aware that perioperative ION after one surgery may increase the chance of ION after subsequent surgeries. 23
Central retinal artery occlusion is a commonly reported cause of postoperative blindness that generally manifests unilaterally. 24 CRAO is frequently associated with spine surgery, and complete recovery is unusual.19,21,26 The occlusion results from obstruction of the central retinal artery, which is a major branch of the ophthalmic artery. CRAO is usually associated with increased intraocular pressure or an embolic phenomenon.21,24 Prone positioning in surgery increases the risk of CRAO commonly due to ocular compression produced by the weight of the head against the headrest. 24 The severity of vision loss depends on the vessel territory being occluded which in most patients is widespread. 19
Cortical blindness is due to ischemia or extreme hypoperfusion of the visual cortex in the occipital lobes that can manifest as bilateral vision loss. 24 The visual loss can range from bilateral homonymous hemianopsia to complete visual loss. 26 One study noted that patients younger than 18 years had a significantly higher prevalence of CB in nonocular surgery than patients older than 18 years. 11 The prognosis of CB is generally better than AION, PION, and CRAO.21,24,26 Most patients with CB recover, often with complete recovery of vision.
Patient risk factors that compromise optic nerve perfusion that may be causative of ocular injuries in nonocular surgery include diabetes mellitus, obesity, and hypertension.6,21,23,24 Factors including general anesthetic duration, blood loss, position during surgery, and fluid administration are important in preventing ocular complications. It has been recommended that procedures requiring prolonged anesthesia can be staged in order to decrease length of surgery.24,25 Additional risk factors associated with CA and other ocular injuries should be considered (Table 2).1-8,10-12,19-21,24-26 Increased attention to appropriate patient positioning during procedures should be prioritized. 26 Due to the different etiologies of ophthalmic complications in orthopedic procedures, disclosure of information prior to surgery is appropriate to consider.
Conclusion
Corneal abrasion during total joint arthroplasty is a rare complication and is infrequently addressed in the literature.5,11,20-24 CA is mostly self-limiting, however, but may lead to patient dissatisfaction and to delays if same-day discharge is attempted. Preventative measures and attentive care may help reduce the incidence of CA in patients undergoing total joint arthroplasty. The lateral decubitus position and longer surgeries times are risk factors for CA.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.