
Abstract
Introduction:
Demographic changes have resulted in an increase in injuries among geriatric patients. For these patients, a rigid cervical collar is crucial for immobilizing the cervical spine. However, evidence suggests that patients with a geriatric facial structure require a different means of immobilization than patients with an adult facial structure. This study aimed to analyze the remaining motion of the immobilized cervical spine based on facial structure.
Materials and Methods:
This study was performed on 8 fresh human cadavers. Facial structure was evaluated via ascertaining the mandibular angle by computer tomography. A mandibular angle below 130°, belongs to the adult facial structure group (n = 4) and a mandibular angle above 130°, belongs to the geriatric facial structure group (n = 4). The flexion and lateral bending of the immobilized cervical spine were analyzed in both groups using a wireless motion tracker system.
Results:
A flexion of up to 19.0° was measured in the adult facial structure group. The mean flexion in the adult vs. geriatric facial structure groups were 14.5° vs. 6.5° (ranges: 9.0-19.0 vs. 5.0-7.0°), respectively. Thus, cervical spine motion was (p = 0.0286) significantly more reduced in the adult facial structure group. No (p = 0.0571) significant difference was oberserved in the mean lateral bending of the adult facial structure group (14.5°) compared to the geriatric facial structure group (7.5°).
Conclusion:
Emergency medical service personnel should therefore follow current guidelines and recommendations and perform cervical spine immobilization with a cervical collar, including in patients with a geriatric facial structure.
Introduction
Global demographic changes have resulted in an increasing number of cervical spine injuries among geriatric patients. 1 Increased age is a risk factor for cervical spine injuries even in cases of minimal trauma. 2,3 Thus, current immobilization protocols recommend cervical spine immobilization in geriatric trauma patients. 4,5 In up to 98% of trauma patients, a cervical collar is used to immobilize the cervical spine. 6 This is to secure the cervical spine in a neutral position to avoid secondary injury. 7,8
The remaining motion of the cervical spine and thus the effectiveness of the cervical collar depend significantly on the fit of the device. 9,10 Although various cervical collar designs have been developed, every cervical collar is in intense contact with the occiput, sternum or clavicle, shoulders, and upper back. 10 -12 The most important contact of the cervical collar is its contact with the patient’s mandible.
The human facial structure may change during the course of life (Figure 1A1 and 1B1). 13 The typical geriatric facial structure is mainly caused by bony and dental changes to the mandible. 14,15 These changes can be quantified by an increase in the mandibular angle (Figure 1A2 and B2). 16,17 To our knowledge, no study has investigated the influence of facial structure on the fit of a cervical collar and thus on the remaining motion of the cervical spine.
Current literature has proposed that elderly patients may require an alternative technique of cervical spine immobilization. 18 Hence, the influence of the geriatric facial structure on cervical spine immobilization should be analyzed. This study therefore aimed to investigate the extent of the remaining motion of the cervical spine in fresh human cadavers, according to the facial structure.
Materials and Methods
Study Design
This study was approved by the relevant local ethics committee (Mainz, Rheinland-Pfalz, Germany, ID: 837.156.16) and was registered in the German Clinical Trials Register (ID: DRKS00010499).
Fresh human cadavers were provided by the body donation program of a local university. Before death, the body donors provided written informed consent for the use of their bodies for scientific research and medical teaching purposes. The fresh human cadavers were frozen shortly after death. Subsequently, for biomechanical experiments, the cadavers were thawed. This process allows simulation of the joint elasticity and soft tissue condition of a living body. So far, biomechanical studies have not found any significant difference in cervical spine motion between fresh human cadavers and patients. 7,19,20
Only fresh human cadavers were included in this study, according to the following criteria: (1) existing written consent to donate the body for scientific research; (2) absence of injuries, diseases, or operations on the cervical spine and mandible; and (3) complete medical records.
The complete medical history of all examined fresh human cadavers was analyzed. Those with diseases such as tumors, thyroid diseases, or similar conditions were excluded from the study.
Evaluation of the Mandibular Angle
A computer tomography (CT) scan of the mandible and cervical spine of each cadaver was performed. The mandibular angle was measured during the procedure as shown in Figure 1A2 and B2. Following the descriptions of the literature 16,17 cadavers with a mandibular angle below 130° were categorized as having an adult facial structure (Figure 1A), while those with a mandibular angle above 130° were defined as having a geriatric facial structure (Figure 1B).

Facial structure of an adult (A1) and a geriatric person (B1). Lateral view of an adult mandible with an angle of <130° (A2). Lateral view of a geriatric mandible with an angle of >130° (B2).
Subsequently, the CT scans of the cervical spine were analyzed for previous injuries, using Horos™ version 3.3.6, a free and open source code software under the LGPL license at Horosproject.org (sponsored by Nimble Co. LLC d/b/a Purview, Annapolis, Maryland, USA).
Biomechanical Test Set-Up
The remaining motion of the cervical spine was measured, and the endpoint of the measurements was taken as the maximum range of flexion and lateral bending.
The fresh human cadavers were placed supine on a spineboard (Laerdal BaXstrap, Stavanger, Norway) and fixed with a fixation system (MIH-Medical Spiderstrap, Georgsmarienhütte, Germany). The cervical spine was immobilized with a cervical collar (Ambu Perfit, Ambu GmbH, Bad Nauheim, Germany). Immobilization was performed by experienced emergency medical service (EMS) personnel and supervised by an emergency physician.
The range of remaining flexion and lateral bending of the cervical spine was measured with a wireless human motion tracker (Xsens Technologies, Enschede, Netherlands). This measurement method has been used before 21 -23 and guarantees exact measurement results compared to other methods. 24 In the experimental setup, the motion trackers were attached to the forehead and to the thorax of the fresh human cadaver (Figure 2). This experimental test setup allowed the recording of the remaining motion of the cervical spine. To measure flexion and lateral bending, the head of the fresh human cadaver was first moved ventrally and afterward laterally to the right in the transverse plane with a tractive force of 100 N. This corresponds to the force and the direction of motion on the cervical spine as applied during intubation or patient transport, which can therefore cause or aggravate a possible injury. 25 -27 The tractive force was measured using an electronic spring balance (LENI; Fa. Korona, Sundern, Germany). To standardize the measurement, the spring balance was always attached to the bregma. The ventral and lateral movement with the spring balance was always performed in the transverse plane.
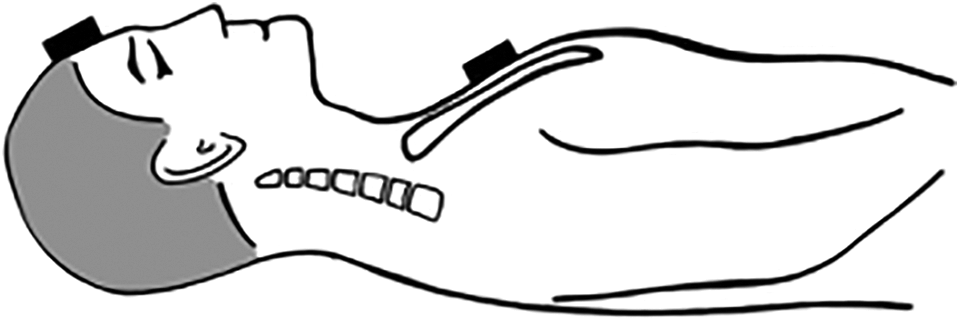
A fresh human cadaver positioned supine on a spineboard. The motion trackers are fixed to the forehead and the sternum.
Statistical Data Analysis
Statistical calculations were performed to determine differences between the adult facial structure group and geriatric facial structure group. The Mann-Whitney test was used to make nonpaired comparisons between both groups. A p-value of <0.05 was considered statistically significant. An exploratory analysis of the measured values was performed. For all measurements, descriptive data with medians and ranges were given. Statistical data analysis was performed using GraphPad PRISM version 8.2.1 (San Diego, California, USA).
Results
Characteristics of Patients
The adult facial structure group (Figure 1A) consisted of 3 female fresh human cadavers and 1 male fresh human cadaver (n = 4). The median mandibular angle in this group was 121.8° (range: 120.0-123.5°; Figure 3B). Meanwhile, the geriatric facial structure group (Figure 1B) consisted of 2 female and 2 male fresh human cadavers (n = 4). The median mandibular angle in this group was 134.3° (range: 130.5-148.0°; Figure 3B). A significant difference in the mandibular angle was observed between the adult facial structure group and the geriatric facial structure group (p = 0.0286; Figure 3B). Further evaluation of the CT images showed that all of the patients in the geriatric facial structure group had a significantly reduced dental status compared to the adult facial structure group. Since the age at death was in the range of 75 to 94 years vs. 56 to 85 years in the adult facial structure group vs. the geriatric facial structure group, it becomes clear, that facial structure does not mainly depend on age but maybe on dental status.

Cervical spine motion in an immobilized fresh human cadaver with adult facial structure during flexion (A). Distribution of the mandibular angle in the adult vs. geriatric facial structure group (B). Range of remaining motion of the cervical spine during flexion (C) and lateral bending (D).
Measurement of the Remaining Motion
With a tractive force of 100 N a remaining passive flexion up to 19.0° was measured in a cadaver from the adult facial structure group (Figure 3A). The median remaining flexion in the adult facial structure group was 14.5° (range: 9.0-19.0°; Figure 3C). In the geriatric facial structure group, the flexion was significantly more reduced by the use of a cervical collar (p = 0.0286). The median remaining flexion in the geriatric facial structure group was 6.5° (range: 5.0-7.0°; Figure 3C). Thus, the median remaining flexion in the geriatric facial structure group was 45% of that in the adult facial structure group.
The median remaining lateral bending in the adult facial structure group was 14.5° (range: 10.0-15.0°; Figure 3D), whereas that in the geriatric facial structure group was 7.5° (range: 6.0-10.0°; Figure 3D). However, there was no significant difference in the remaining lateral bending between both groups (p = 0.0571).
Discussion
The main objective of this study was to quantitatively measure and evaluate the remaining motion of the immobilized cervical spine based on the facial structure. In this biomechanical study, adult and geriatric facial structures showed significantly different remaining flexion of the immobilized cervical spine. However, the current study could show that having a geriatric facial by the means of a geriatric mandible structure did not mainly depend on the patients age but maybe on the dental status. Thus, categorizing a patient’s facial structure as “geriatric” should not be principally based on the age but on the clinical facial habitus as shown in Figure 1. However, the mandibular angle seemed to influence the fit of the cervical collar and contribute to the effectiveness of the device. Results also showed that an increased mandibular angle, as found in a geriatric facial structure, contributed to a decreased remaining flexion in the immobilized cervical spine. These findings suggest that patients with a geriatric facial structure do not need an alternative technique of cervical spine immobilization due to their altered mandible structure. In contrast to patients with an adult facial structure, flexion is avoided by the use of a cervical collar in patients with a geriatric facial structure. Further studies must therefore analyze if there are other factors that justify the application of different immobilization techniques in geriatric patients. 18 Other anatomical changes in geriatric patients, such as increased thoracic kyphosis, may also contribute to an impeded immobilization of the spine. 18 Furthermore, changes in the skin, which are often seen in elderly patients, can increase the risk of pressure ulcerations caused by the use of cervical collars. 28 Innovative concepts have been proposed to reduce pressure ulcerations caused by immobilization devices in general. 29,30 In particular, Worsley et al. investigated the effects of cervical collar designs and how an acceptable range of remaining motion was achieved with gentle soft tissue adaptation by adjusting the contact pressure on the bony structures. 12 Special immobilization techniques using a vacuum mattress without a cervical collar can also provide good spinal immobilization 22 and can be used alternatively.
As a side result of this study, we found an immense remaining flexion of up to 19° in the immobilized cervical spine. This finding is consistent with the findings of other studies describing the relevant remaining motion of the cervical spine under immobilization. 21,31 Therefore, there is an ongoing need for the development of newly designed cervical collars to improve cervical spine immobilization. 11,32
This study is limited to some extent. According to some authors, the geriatric facial structure is better characterized by evaluating the position of the gonion and taking into account the width of the mandible rather than measuring the mandibular angle, 33 and we have not considered this in the study. Furthermore, the tractive force was applied in a standardized manner only to the ventral and lateral right sides, and combined movements were not performed and analyzed. No literature has provided any indication of the magnitude and direction of the force required to aggravate cervical spine damage. While previous studies have shown that after an initial trauma, no further aggravation can occur through further manipulation, 34 recent biomechanical studies have shown a direct correlation between manipulations and the width of the dural sac in the injured upper cervical spine. 25,26,35 The present study is limited by the very small group of fresh human cadavers. In a continuing study on living subjects, the accuracy of fit of the cervical collars could be verified.
Conclusion
In conclusion, the findings of this study suggest that EMS personnel should follow current guidelines and recommendations 36 and perform cervical spine immobilization using a cervical collar, even in patients with a geriatric facial structure.
Footnotes
Authors’ Note
The local ethics committee reviewed and approved the present study (ID: 837.156.16).
Acknowledgments
The authors would like to thank Professor Dr. Erik Popp for his technical support in the preparation of the fresh human cadavers. We would like to thank the staff of the Anatomical Institute of the University of Heidelberg for providing the premises and for their support in handling fresh human cadavers. We would also like to thank Mr. Geir Dillan for taking the photographs.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.