
Abstract
Objectives:
To better elucidate how the COVID-19 pandemic has affected the operatively treated geriatric hip fracture population and how the health care system adapted to pandemic dictated procedures.
Design:
Retrospective cohort study.
Setting:
A community hospital.
Participants:
Individuals ≥65 years of age presented with a proximal femoral fracture from a low-energy mechanism
Measurements:
We defined 3 phases of healthcare system response: pre-COVID-19, acute phase, and subacute phase. Thirty-day mortality, time to operating room (OR), length of stay, time to start physical therapy, perioperative complications, delirium rate, hospice admission rate, discharge dispositions, readmission rate, and the reason of surgery delay were assessed.
Results:
The number of hip fractures has remained constant during the pandemic. The 30-day mortality rate, time to OR, and length of stay were higher in the pandemic compared to the pre-pandemic. Those who had a longer wait time to OR (≥ 24 hours) had more complications and increased 30-day mortality rates. Some of the surgery delays were related to OR unavailability as a consequence of the COVID-19 pandemic. Surgery was delayed in 3 patients who were on direct oral anticoagulants (DOACs) in pandemic but none for pre-pandemic period.
Conclusion:
This is the first study to compare the effect of the acute and subacute phases of the pandemic on uninfected hip fracture patients. In the age of COVID-19, to provide the best care for the vulnerable geriatric orthopedic populations, the healthcare system must adopt new protocols. We should still aim to promote prompt surgical care when indicated. It is important to ensure adequate resource availability, such as OR time and staff so that hip fracture patients may continue to receive rapid access to surgery. A multidisciplinary approach remains the key to the management of fragility hip fracture patients during the pandemic.
Keywords
Introduction
In December 2019, the 2019 novel Coronavirus (2019-nCoV) was identified as the cause of Coronavirus disease 2019 (COVID-19) after a spike in pneumonia-like illness in Wuhan, China. 1,2 Soon after, the virus quickly spread to many corners of the world and, March 11th, 2020, was declared a pandemic by the World Health Organization (WHO). 3 As of January 2021, it has caused over 88 million confirmed cases and over 1.9 million deaths worldwide. 3
As the pandemic has spread, healthcare facilities have instituted many precautionary measures; hospitals rapidly expanded respiratory isolation units, emphasized telemedicine for patient evaluation, and implemented approaches to minimize room entry. 4 A large proportion of anesthetists and operating department practitioners were deployed to intensive care units, resulting in the reduction of operating room (OR) availability. 5 In orthopedic surgery, non-urgent diagnostic imaging was postponed, outpatient physical therapy and occupational therapy were decreased, and non-urgent elective procedures were postponed. 6,7
As a society, social distancing and travel restrictions have reduced the volume of patients experiencing trauma, while the amount of osteoporotic and fragility hip fractures have remained constant during the pandemic. 5,8 -13 There is compelling evidence that early surgery, prompt orthogeriatric care, a multidisciplinary approach, and early postoperative ambulation improves outcomes for patients with hip fractures. 14 -18 Although this patient-focused, algorithmic care has been shown to improve hip fracture outcomes in non-pandemic times, the vulnerability of the geriatric hip fracture population has made their treatment more complicated during COVID-19. Preliminary studies from various countries have noted increased mortality with hip fracture cases during this pandemic when compared to similar study cohorts in prior years. 19 -27 The shortage of personal protective equipment (PPE), reduced OR availability, lack of familiarity with the evolving COVID-19 protocols, visitor restrictions, and reduced physical and occupational therapy potentially negatively impacted the treatment of hip fracture patients.
Due to the developing nature of the COVID-19 pandemic, research into how it has impacted
Material and Methods
Study Design and Participants
A retrospective cohort study was approved by the institutional review board, and the study was conducted at a metropolitan community hospital in Minnesota. Included participants were patients ≥65 years of age presenting with a radiographic diagnosis of a proximal femoral fracture (31-A and 31-B according to the OTA/AO classification 28 ) from a low-energy mechanism, who were treated operatively over 24 weeks from January 17, 2020, to July 2, 2020. The World Health Organization (WHO) officially recognized COVID-19 as an international emergency on March 11, 2020. 3 Subsequently, on March 13, 2020, Minnesota’s Governor Walz declared a peacetime emergency to prepare for the COVID-19 pandemic in Minnesota. 29 We defined 3 phases of healthcare system response: pre-COVID-19, acute phase, and subacute phase. Pre-COVID-19 (period A) was defined as the 8 weeks preceding March 13. The acute phase (period B) was defined as 8 weeks after the peacetime emergency declaration and is characterized by new protocol development and frequent staff updates on rapidly evolving practices during the early stages of the crisis. The subacute phase (period C) was defined as 8 weeks after the acute phase and represents a timeframe with less frequent changes in practice and protocols.
Exclusion criteria included patients with high-energy trauma, periprosthetic or peri-implant fracture, greater trochanter or lesser trochanter fracture, age less than 65 years, non-surgical cases, or revision surgery for prior hip fracture.
Data Collection
Demographic, clinical, laboratory, treatment, and outcome data were extracted from electronic medical records by the site investigators with the use of a customized data collection form.
Variables
The primary outcome of this study was 30-day mortality. Demographic, clinical, and functional variables were extracted from the electronic medical record, including age at presentation, sex, body mass index, and comorbidities. We identified a set of commonly occurring comorbidities in the study population. 30 -32 The presence of the following comorbidities was registered: diabetes, hypertension, heart failure, cognitive impairment, cancer, metastatic cancer, chronic obstructive pulmonary disease (COPD), stroke, depression, Parkinson’s disease, and chronic kidney disease (CKD). In addition the Charlson Comorbidity Index (CCI) was calculated for each patient.
The diagnosis of COVID-19 was determined by a polymerase chain reaction (PCR) test from nares swab samples. Variables related to the timing of care were also collected, including the time to surgery (number of hours from the first presentation to the hospital to the time of surgery). Variables related to the injury and surgery were collected as well, including fracture type and mechanism of injury. Length of stay, time to start physical therapy after surgery, perioperative complications, delirium rate, hospice admission rate, discharge dispositions, readmission rate, and the reason for surgery delay were also assessed. Perioperative complications considered were acute kidney injury, myocardial infarction (MI), heart failure, deep vein thrombosis (DVT), pulmonary embolism (PE), anemia which required transfusion, gastrointestinal (GI) bleeding, surgical site infection, stroke, and respiratory failure. Further analysis on 30-days mortality, delirium rate, and perioperative complications to compare early surgery group <24 hours and delayed surgery group ≥24 hours were performed. The reasons for the surgery delay were also investigated.
Statistical Analysis
Continuous variables were presented as the mean and the standard deviation, and categorical variables were presented as the number and percentage. To compare the differences between 3 different treatment periods, a pair-wise comparison was performed. Statistical analysis of study outcomes was performed using the independent-samples t-test for continuous variables with normal distributions, while the Mann-Whitney U test was used for continuous variables that were not normally distributed. Categorical variables were compared using the chi-squared test. All analyses were performed with SAS software, version 9.4 (SAS Institute, Cary, NC). Statistical tests were considered significant at p < 0.05 (2 tails).
Results
There was a total of 125 patients who met inclusion criteria: 41 patients (32.8%) from period A, 39 patients (31.2%) from period B, and 45 patients (36.0%) from period C. Six patients did not have surgery and were excluded from this study: 4 from period A, 1 from period B, and 1 from period C. The 5 patients in periods A and B were not tested for COVID, but no respiratory or COVID symptoms were reported to influence treatment decisions. One hip fracture patient with a past medical history of severe dementia in period C was asymptomatic COVID positive. The patient was scheduled for hip fracture fixation within 24 hours of presentation, but canceled due to family/healthcare agent decision for non-operative care.
Table 1 shows a summary of the main demographic variables collected. Variables are described for the total number of included patients and separately for the number of patients among the 3 different periods. Their mean (SD) age was 83.6 (7.9) years with a minimum age of 65 years and a maximum age of 103 years. Women represented 74.4% of total cases, and 96.8% of patients were white. Mean BMI was 24.6 ± 6.0. Sixty-two fractures were intertrochanteric, and 63 fractures were femoral neck fractures.
Demographic Variables.

Abbreviation: BMI, Body Mass Index.
During the COVID-19 acute phase (period B), 84.6% of patients were not tested for COVID-19 upon admission and underwent surgery without the test. In the acute phase of the pandemic, the test was not widely available. Patients were not tested, because they did not have respiratory symptoms or fever, and therefore did not meet a criterion for being tested at that time. In period C, the test had become widely available, and new protocols were put in place to protect staff and patients. As a result, during this period, 44 out of 45 patients (97.8%) were tested for COVID-19 upon admission with the test result returning prior to surgery. There were no COVID-19 positive patients in any of the cohorts while inpatient during the research period.
The presence of the following comorbidities was registered: diabetes, hypertension, heart failure, cognitive impairment, cancer, metastatic cancer, chronic obstructive pulmonary disease (COPD), stroke, depression, Parkinson’s disease, and chronic kidney disease (CKD). In total, 82 patients (65.6%) had 3 or more comorbidities at baseline. The number of patients who had 3 or more comorbidities was highest in period C (N = 32, 71.1%) but was not statistically different across the 3 groups. The mean CCI for the entire cohort was 2.2 (range 0-10), with each period having a similar CCI mean and (range): A: 2.1 (0-7), B: 2.3 (0-9), C: 2.2(0-10).
Clinical outcomes are shown in Table 2 and 3. In total, 110 patients (88.0%) survived, and 15 patients (12.0%) died within the 30 days post-fracture. Primary outcome, 30-day mortality was the highest in period B (17.9%), followed by period C (11.1%) and 7.3% in period A, although this was not statistically different. One of the secondary outcomes, time to OR, was the longest in period C: mean 33.2 hours (SD 28.0), followed by period B: mean 24.9 hours (SD 16.5), and period A: mean 23.1 hours (SD 13.3) (period A vs. period C: p = 0.04). The mean (SD) time to surgery was 27.3 (21.0) hours. The length of hospital stay was longest in period C: mean 143.1 hours (SD 87.6), followed by period B: mean 129.9 hours (SD 35.3), and period A: mean 109.4 hours (SD 35.4) (period A vs. period C: p = 0.01).
Clinical Outcomes.
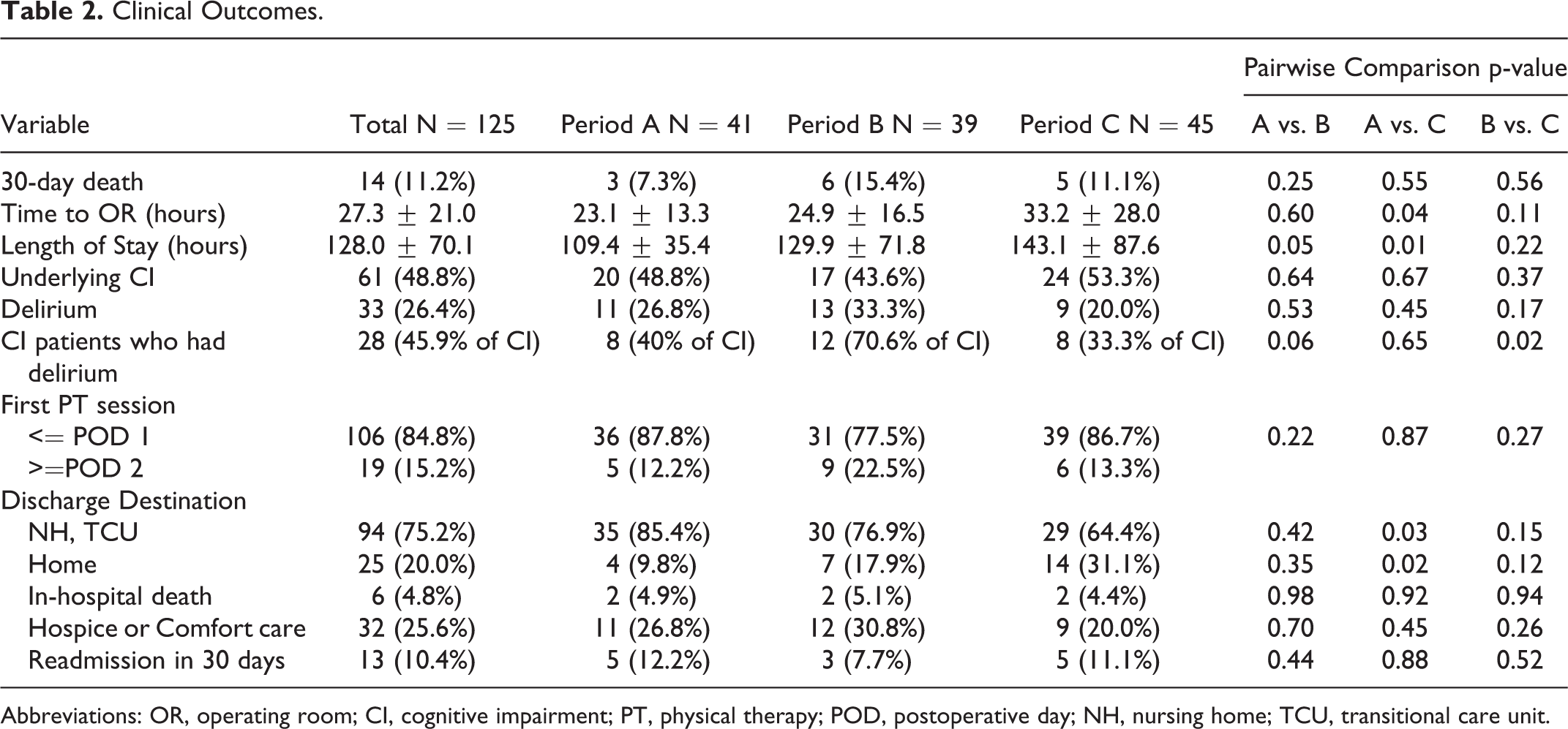
Abbreviations: OR, operating room; CI, cognitive impairment; PT, physical therapy; POD, postoperative day; NH, nursing home; TCU, transitional care unit.
Perioperative Complications.

Abbreviations: DVT, deep venous thrombosis; PE, pulmonary embolism; MI, myocardial infarction; GI, gastrointestinal.
A total of 33 patients (26.4%) had delirium during the hospital stay. The rate of developing delirium was highest in period B (33.3%), followed by period A (26.8%) and period C (20.0%), although the difference was not statistically significant. A total of 61 patients (48.8%) had underlying cognitive impairment (CI) upon admission. Among those who had underlying CI, 40.0% of patients had delirium in period A, 70.6% had delirium in period B, and 33.3% had delirium in period C (period B vs. period C: p = 0.02).
In total, 84.8% of patients had their first physical therapy (PT) session within one postoperative day (POD) and there was no statistical difference among the 3 groups regarding the timing of the first PT session after the surgery. Fourteen patients (31.1%) in period C were discharged to home care, compared to 9.8% from period A and 17.9% from period B (period A vs. period C: p = 0.02, period B vs. period C: p = 0.12). Fewer patients from Period C (64.4%) were discharged to nursing home (NH) or transitional care unit (TCU) when compared to 85.4% from period A and 76.9% from period B (period A vs. period C: p = 0.03). There was no statistical difference in the readmission rate (within 30 days) between these groups. In total, approximately one-fifth of patients were admitted to hospice/comfort care. No statistical difference in hospice admission was noted between the 3 groups. Table 3 shows perioperative complications. The anemia requiring transfusion was significantly higher in period C (22.2%), compared to period A (2.4%).
Figure 1 shows the length of stay for the patients who were discharged to NH/TCU vs. to home in period A, B, and C. The length of stay for those who were discharged to NH/TCU was longest in period C (mean 154.4 hours, SD 98.6), compared to period A (mean 112.8 hours, SD 34.9, p = 0.02) and period B (mean 125.1 hours, SD 52.9, p = 0.15). The length of stay who were discharged to home was also longer in pandemic periods (period B: mean 135.0 hours, SD 126.6 and period C: mean 115.6 hours, SD 55.4), compared to pre-pandemic (mean 75.7 hours, SD 21.0), although this was not statistically significant.

A line chart illustrating the length of stay comparison for operatively treated hip fracture patients discharged to nursing homes and transitional care units (NH/TCU) (blue) versus patients discharged to home (orange) for the 3 study periods.
Table 4 depicts a comparison between patients with time to OR< 24 hours vs. those with time to OR24 hours group. Sixty-one patients (48.8%) underwent early surgery and 64 patients (51.2%) underwent delayed surgery. There was no difference in the number of medical comorbidities at baseline between the 2 groups; a mean of 3.15 (SD 1.74) in the early surgery group was noted vs. a mean of 3.22 (SD 1.55) in the long wait group (p = 0.81). Of the 64 patients who underwent hip fracture surgery after 24 hours from admission, 11 patients (17.2%) died within 30 days vs 3 patients (4.9%) of 61 who underwent surgery within 24 hours (p = 0.03). Delirium was higher (29.7%) in the long wait group than in the early surgery group (21.3%, p = 0.28). The delayed surgery group had more postoperative complications, but they were not statistically significant.
Comparison between Time to OR< 24 Hours and 24 Hours.

Abbreviations: OR, operating room; DVT, deep venous thrombosis; PE, pulmonary embolism; MI, myocardial infarction; GI, gastrointestinal.
Table 5 describes the reasons for the surgery delay. For more than half cases in the delayed surgery group (57.8%), the surgery was performed on the day following admission. Surgery was delayed due to OR unavailability in 3 cases during period C. As a result of the COVID-19 pandemic, the OR was available on a restricted basis; there were other in-patient surgical cases deemed more emergent and there was a reduced OR staff. Surgery was delayed in 3 patients who were on direct oral anticoagulants (DOACs) in period C but none for period A patients. Patients who were on DOACs in period A had surgeries within 24 hours with general anesthesia. Those patients who waited for 48 to 72 hours for DOACs “washout” did so because spinal anesthesia was recommended per an anesthesia guideline during the COVID-19 pandemic at that time. Specialists were consulted for 1 case in period B (cardiology consult for atrial tachycardia) and 1 case in period C (gastroenterologist consult for cirrhosis and coagulopathy). Medical optimization was required for 1 patient in period A, 1 patient in period B, and 2 patients in period C (not statistically different). International Normalized Ratio (INR) reversal was required with FFP and vitamin K in 3 patients in period C. There was one patient whose family wanted to be present before surgery in period C.
The Reasons for Delayed Surgery.

Abbreviations: OR, operating room; DOACs, Direct oral anticoagulants; INR, International Normalized Ratio; FFP, Fresh Frozen Plasma.
Discussion
We investigated how the COVID-19 pandemic affected older adults undergoing hip fracture surgery. We found that the 30-day mortality rate was higher in the pandemic period compared to the pre-pandemic period as it has been reported by other studies, although the difference was not statistically significant in our cohort.
In our study, special attention was given to the time to OR and the reason for surgery delay during the COVID-19 pandemic. Previous research has reported that time to surgery of 24 hours is a threshold for increased risk of complications and high mortality. 14 -18 Our study also showed that those who had a longer wait time of ≥ 24 hours had acute complications and increased 30-day mortality rates. Since medically complex patients are predisposed to both complications and awaiting optimization before surgery, confounding factors likely present. However, the mean and SD of preexisting medical comorbidities were not different among the 2 groups (time to OR< 24 hours group vs. time to OR24 hours group), suggesting the differences in preoperative conditions were minimal. The time to OR was longest in period C, followed by period B and period A. We investigated the reason for surgery delay during the pandemic. Delayed surgery was due to a variety of reasons, although not because of waiting for the results of the COVID-19 test. COVID-19 test results were back within a few hours after the admission. There was also no difference in the number of patients who were too sick to undergo surgery and required medical optimization. Some of the surgery delays were related to OR unavailability due to reduced staff or rooms as a consequence of the COVID-19 pandemic. Given period C had the longest wait time, our result indicated that the adequate OR and staff resources were still not ensured in subacute phase of pandemic. Our study as well as previous studies 5,8 -13 showed that the number of fragility hip fractures has remained constant during the pandemic, therefore, it is important to ensure adequate resource availability, such as OR time and staff so that hip fracture patients may continue to receive rapid access to surgery.
Uncertainty regarding the anesthesia method for hip fracture patients who were on DOACs during the pandemic was another reason for delayed surgery. In period C, the surgeries of 3 patients were delayed due to taking DOACs, requiring time to washout DOACs. In the pre-pandemic period, those who were taking DOACs underwent early surgery with general anesthesia. However, during the subacute phase of pandemic (period C), regional anesthesia was recommended by the European and American Societies of Regional Anesthesia to decrease the risk of viral aerosolization. 33 Therefore, patients on DOACs had to wait 48-72 hours for washout before undergoing spinal anesthesia. 33,34,35,36,37,38,39 Which anesthesia (general endotracheal or spinal) is preferred during the pandemic is still controversial. The choice of anesthesia should be based on the patient’s overall situation, trauma condition, and needed surgical treatment. 40 At this point, further studies are needed to determine the preferred method of anesthesia.
Lastly, we observed an increased length of stay during the COVID-19 pandemic. We speculate that this is due to several factors. The length of stay was longest for patients who were discharged to NH/TCU in period C. When patients were discharged to other facilities, NH and TCU often required negative COVID-19 test results within 24-48 hours of transfer to accept new patients. This resulted in the need for repeat COVID-19 tests. It was also noted that when other residents in the facilities were diagnosed as COVID-19 positive, the facility could not accept new patients for at least a few days. Second, more patients were discharged to home in pandemic periods than pre-pandemic and the length of stay for patients who were discharged to home in pandemic was longer than pre-pandemic. Patients and their families requested to be discharged home with home health care support than to TCU or NH, presumably to avoid potential COVID-19 exposure. This increased the required hospital time for patients to be ready for discharge. Our research showed there was no increase in the readmission rate for those who were discharged to home. Being discharged to home is a good alternative to reduce COVID-19 exposure for those who have a robust support system at home.
Despite changes resulting from the COVID-19 pandemic, the management of patients with hip fracture should remain unchanged from that offered before the pandemic. Hip fractures should continue to be primarily managed surgically to reduce pain, restore mobility, and improve survival. We should still aim to promote prompt (less than 24 hours) surgical care when indicated to prevent perioperative complications while taking all precautions for the minimization of the risk of COVID-19 transmission. Additionally, immediate postoperative ambulation and rehabilitation should be prioritized in order to maintain optimal postoperative outcomes. Geriatricians need to be involved in patients care to medically optimize the patient without delaying surgery. A multidisciplinary approach remains the key to the management of these fragility hip fracture patients during the COVID-19 pandemic.
Strengths and Limitations
This study has multiple strengths. First, this is the first study to compare the effect of the acute and subacute phases of the pandemic on uninfected hip fracture patients. Second, to our knowledge, there has been no study conducted to analyze the reason for surgery delay for hip fractures during the acute and subacute phase of pandemic.
This study’s limitations include its retrospective nature, which is prone to the influence of potential confounders, and the exclusion the non-operatively treated patients, which would impact the reported 30-day mortality rates of all hip fracture patients. Other limitations include the limited study period and relatively small sample size due to the new and evolving COVID-19 pandemic. Thus, it could have affected the significance of the differences reported. More research with a larger number of patients is needed to further determine the impact this has on patient outcomes. Lastly, most of the patients were white, and our results therefore may not be generalizable to other ethnicities.
Conclusions
The COVID-19 pandemic has changed several health care scenarios. In the age of COVID-19, to provide the best care for the vulnerable geriatric orthopedic populations, the healthcare system must adopt new protocols. Appropriate management including COVID-19 infection-control precautions, widely available rapid COVID-19 tests, early orthogeriatric review, surgery within 24 hours, continuing delirium precautions, assuring OR and staff availability, and a multidisciplinary approach are warranted to minimize the risk of mortality and other adverse events in hip fracture patients during such a pandemic.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.