
Abstract
Background:
Many Wheelchair users experience adverse effects specific to their situation, some of which might be avoided if suspension systems are integrated into the wheelchair.
Objectives:
Our study aimed to compare the user experience using a novel wheelchair suspension system with normal wheels. We tried to quantify the user feelings and impressions while using the different wheels.
Study Design:
Double blinded comparative randomized study.
Methods:
The patients were randomized into 2 groups. One used shock absorbing wheels, and the other group had a set of standard wheels with the same exact wheelchairs. The patients were taken to a daily trip by the caregivers and given questionnaires in the second and fourth days. On the morning of the third day the wheels were interchanged, creating a cross over between the groups. We collected general and medical information from the participants. The main outcome measures were the questionnaires filled by the patients and the caregivers aiming to quantify the user experience with the suspension equipped wheels.
Results:
Statistical significance was reached in 2 questions referred to the patients: “In general—During the ride I didn’t feel the bumps” and “I feel very confident when riding the chair” and in one question referred to the caregiver—“It was easy to push the chair in suboptimal ground.”
Conclusions:
We conclude that the shock absorbing system provided a better user experience in the immediate term than standard wheels. Further study is needed to assess the long-term implications.
Keywords
Background
The use of assistive technology is a common and increasingly versatile way of adapting to a disability. 1 More than 3.3 million Americans or 1.5% of the adult population use wheelchairs or motorized scooters as their primary means of mobility and transportation. 2 Part of the increase in the use of assistive technology can be attributed to remarkable improvements in design, functionality and appearance. For example: there has been dramatic advancement in design options in wheelchairs in the last 2 decades including lighter weight wheelchairs, use of advanced building materials including carbon fiber and metal alloys, motorized wheelchairs and the ability to customize the fit of the seat and back support to the wheelchair rider. 3 With an ever increasing number of people with a disability in need of ambulation so are the requirements for a more maneuverable, faster and less energy consuming wheelchair. 4 All manual wheelchairs were not created equal and there are variations in the quality and performance of different designs and materials used. 5,6
While propelling a wheelchair users come across obstacles such as gravel, bumps, curbs, and uneven surfaces. Collisions with these obstacles cause obvious contusions and also vibrations on the wheelchair and, in effect—the wheelchair user, potentially causing adverse effects such as low-back pain, disc degeneration, muscle fatigue and other harmful effects. 7
The International Standards Organization (ISO) and the American National Standards Institute developed a standard for whole-body vibration measurement which includes the amplitudes of vibrations that are considered harmful and the exposure time for vibrations to be dangerous. The standard also discusses some of the physical effects that can occur from whole-body vibration exposure. 8 Van Sickle et al showed that wheelchair propulsion produces vibration loads that exceed the ISO 2631 -1 standards at the seat of the wheelchair as well as at the head of the user. 9 In another article he examined the relationship between the seating systems for manual wheelchairs and the vibrations experienced showing differences in how seating systems transmit or dampen vibrations. 10 Based on the exposure magnitudes of vibrations defined in the ISO-2631 standard, wheelchair companies added suspension to their wheelchairs to reduce the level of vibrations that are transmitted to wheelchair users including (among others) rear wheel suspension, seat suspension and frame suspension.
In an ongoing effort to reduce the vibrations some wheelchair companies have managed to reduce but not eliminate the problem. Cooper et al found that the addition of suspension caster forks reduced the amount of vibrations transferred to the user. 11 Wolf et al revealed that although suspension manual type wheelchairs visually reduce shock vibrations, the chairs are not yet ideal, possibly due to the orientation of the suspension elements 12 and later showed that suspension manual type wheelchairs are approaching significance in reducing the amount of shock vibrations transmitted to wheelchair users during curb descents. 13
Recently, a novel type of suspension was invented by Softwheel inc. (Tel-Aviv, Israel). This new suspension system is incorporated into the wheel itself potentially reducing the primary shock and also the following vibration magnitude, frequency and duration (Photo 1). The suspension was tested by the University of Pittsburgh Human Engineering Research Laboratories in Pittsburgh, PA (6/16/2015—Record ID-342), conforming with ANSI/RESNA WC Standards January 2009: WC-08. The following tests were performed (in order): impact tests, multi-drum test, curb drop test. The wheels passed all the relevant tests during this evaluation, with a few minor issues (small grease leakage during use, audible creaking noise that appeared to be connected to axial forces applied to the axle). The testers came up with the following conclusions: The results show a clear difference in jerk values over the entirety of the tests and in favor of the shock absorbing wheel. Other raw data of comparative tests were also analyzed and similar results were found. It is reasonable to assume that, as these tests involved only minor obstacles, other tests will include larger obstacles and the difference in jerk will be even greater and differences in accelerations will emerge due to the damping effect of the dampers.
To the best of our knowledge, this is the first study to compare user experience using the in-wheel suspension technology with a standard non-suspended wheelchair in a double blinded, prospective, randomized, control study. If indeed there is a clinical difference in User experience when using a suspension technology than wheelchair users would be encouraged to use it potentially preventing the harmful effects of the continuous seating position, i.e. lower back pain, neck pain, disc degeneration, muscle fatigue and others.
Methods
We conducted a randomized, cross-over, double blind study in the rehabilitation ward of our hospital. As required, all IRB and local Helsinki committee approvals were obtained. We recruited the patients voluntarily from the rehabilitation ward. All participants were chair bound when recruited and were not previously chairbound and could fill out a series of questions. After careful literature review we failed to find a validated questionnaire testing the user experience while using a wheelchair in the short period. Exclusion criteria were inability to answer the questionnaire, known Neurodegenerative disorder and moderate diabetic neuropathy. After participant approval and written consent participants were randomized into 2 groups using a sequential method supervised by the recruiting doctor. One participant was given a standard wheelchair (Service 3.6, Meyra GmbH inc. Kalletal-Kalldorf, Germany) equipped with shock absorbing wheels and the other the same standard wheelchair with a set of standard wheels using a 1 -1 allocation method. The manufacturer divided the shock absorbers into 3 groups according to the weight of the patient, allowing proper compression and timely extension of the cylinders, thus all patient’s weights were recorded and the proper absorbers were installed. All the wheels were covered so the patient and attending doctors did not know what kind of wheels were installed (Photo 2).
Once daily for the next 4 days the patient was taken for a short-standardized trip in the hospital by an attending doctor from the orthopedic ward (for safety and legal reasons). Aside from the rides the participants used the wheelchair normally throughout the day. The trip covered different kinds of surfaces: Smooth and even ground ∼ 40% of the ride. Even cobblestone road ∼ 20% of the ride. Smooth light slope ∼ 20% of the ride Tile road ∼ 20% of the ride. Two ascents and descents of curbs.
We timed the rides so the average speed was constant to minimize bias. The trip was measured to be roughly 800 meters long. All the drives were performed by only 5 doctors and we demonstrated and practiced with all of them before starting the study about how a standard ride should be performed. All the doctors that participated did not have a former experience pushing a wheelchair. On the second and fourth days the patient and the caregiver completed a short questionnaire immediately after the trip. Table 1 shows the complete questionnaires and results. All the questions were answered using a 1-10 Visual Analog Scale (1- I don’t agree with the statement, 10—I totally agree with the statement). The questionnaires were developed with the help of an expert rehabilitation physician, an expert physiotherapist and 2 resident orthopaedic surgeons in an attempt to quantify the subjective experience of the user and the caregiver and the rationale that the most common adverse reactions to wheelchair use are neck and back pain, tiredness and muscle pain 7 . On the morning of the third day, the wheels of the wheelchair were exchanged, creating the cross-over between the groups (Figure 1).
Demography, Background Diseases and Past Use of Wheelchair, by Order of Intervention.

Continuous/ordinal variables are presented with mean (SD) [median, range].
* Missing values: ethnicity (1), other (1). No product deficiencies or adverse effects were reported.
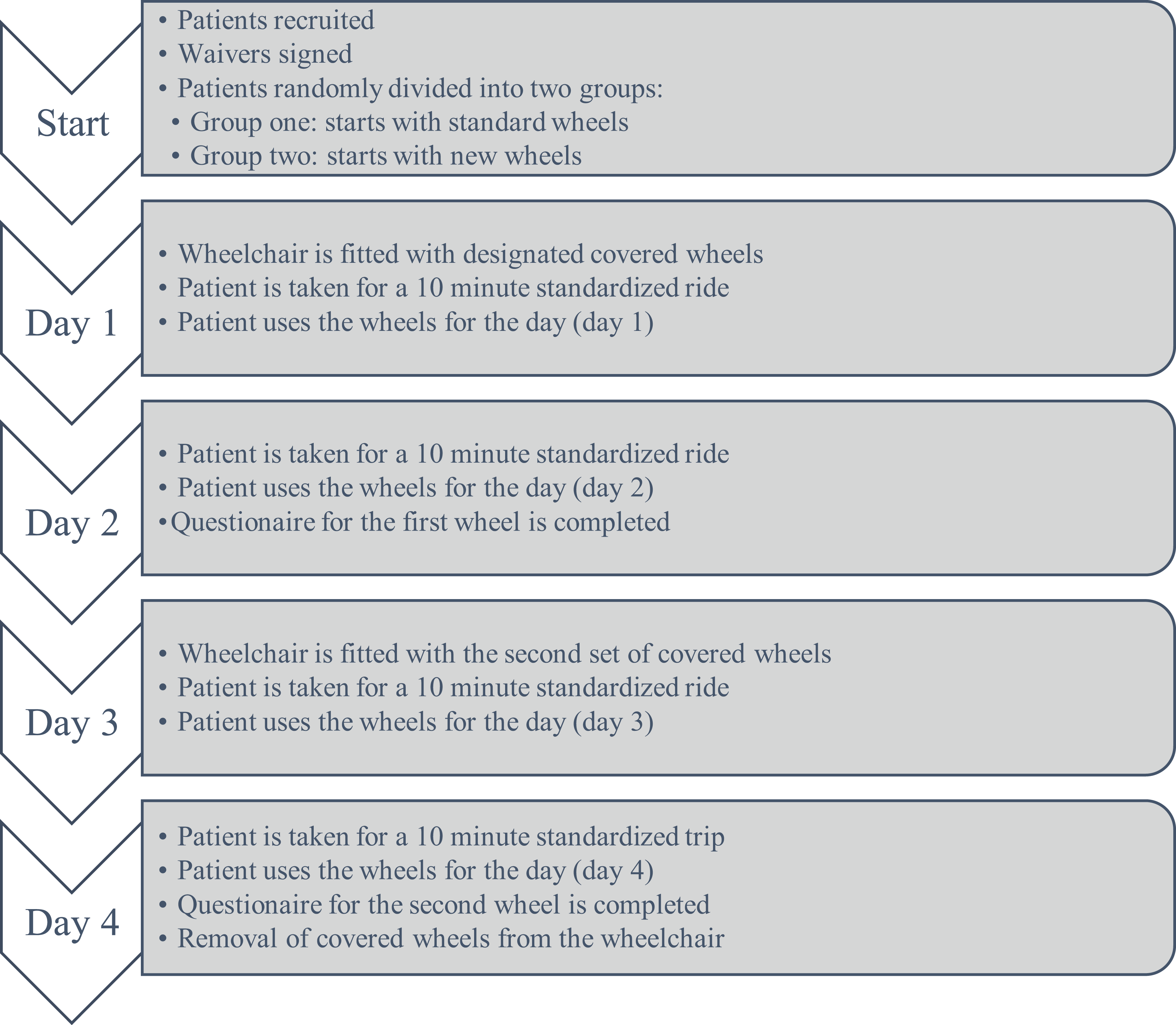
Study flow chart.
Statistical Analysis
Sample size was calculated using an estimate of 3-point effect size (on the analog visual scale of 1-10), alpha 5% and a 5-point standard deviation resulting in a total of 24 participants.
All the data were analyzed using SAS 9.4 software (SAS, Cary, USA). Categorical variables are represented using percentages, and continuous variables are represented by the standard distribution indices. Differences in continuous variables were tested using the paired T test or the Wilcoxon sign rank. McNemar’s test was performed for the categorical variables. Clinical difference was determined if the difference was ≥2 points. Equivalence of the wheelchairs was determined if the difference was between -1 and 1. Statistical significance was accepted to be p < 0.05.
Results
A total of 29 participants were enrolled, 24 completed the study and were included in the final statistics. Of the 5 participants who did not finish the study, one started walking before completion of the study, one had a personal wheelchair that was incompatible, one elected to stop participation for personal reasons and 2 participants were removed due to clerical errors (Figure 2).

CONSORT 2010 Flow Diagram.
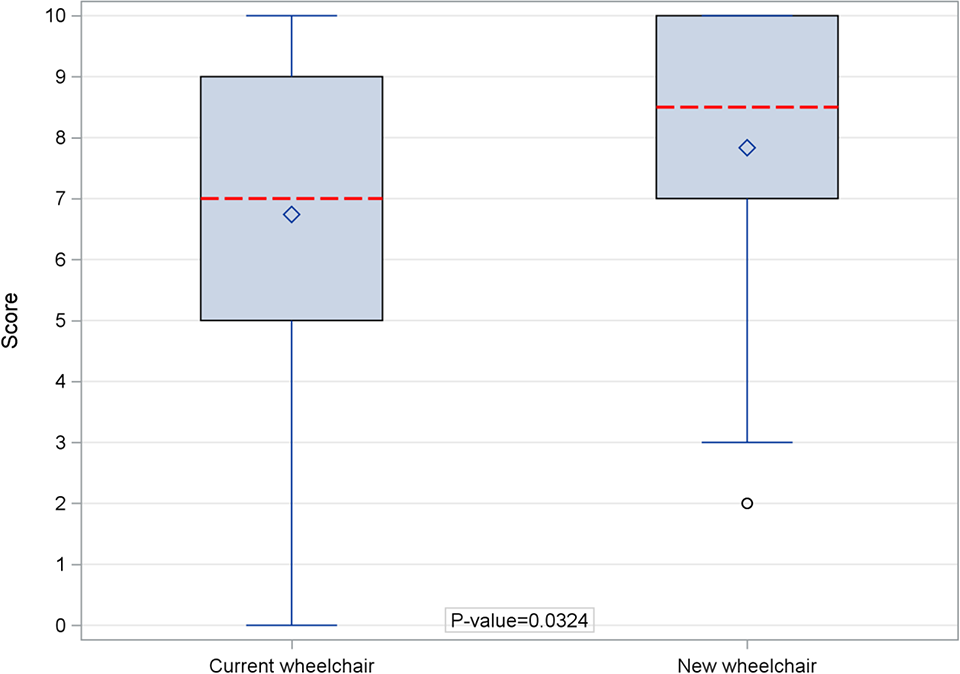
There were no significant differences between the groups in demographics, background diseases and past use of a wheelchair (Table 2). Statistical significance was reached in 2 questions referred to the participants (Table 1, Table 3): In general, “During the ride I didn’t feel the bumps” (6.95, 5.5, p = 0.0176) (Figure 3) and “I feel very confident when riding the chair” (9, 7.96, p = 0.0172) (Figure 4), and in one question referred to the caregiver: “It was easy to push the chair in suboptimal ground” (7.83, 5.74, p = 0.0324) (Figure 5). The following question reached near statistical significance: “During the travel on unpaved ground I didn’t fell the bumps” (6.67, 5.33, p = 0.0773). Eighteen (75%; 95%CI: 55%-88%) participants felt that the “new” (i.e. equipped with shock absorbing wheels) chair was equally/more comfortable and equally/more secure. 25% felt that the current wheelchair (non-shock absorbing) was better (Figure 6). No adverse effects were recorded.
Study Outcomes.

Continuous/ordinal variables are presented with mean (SD) [median, range]. ‡Missing values: Its very easy to autonomically commute in the chair (3), the rest had 1 missing value *Difference was calculated by subtracting the answers regarding the standard wheelchair from the new wheelchair. Thus, positive difference reflects higher score for the new wheelchair compared the standard wheelchair **P-value for the difference between the new and standard wheelchairs (Wilcoxon sign-rank test).
Study Outcomes (Categorical).
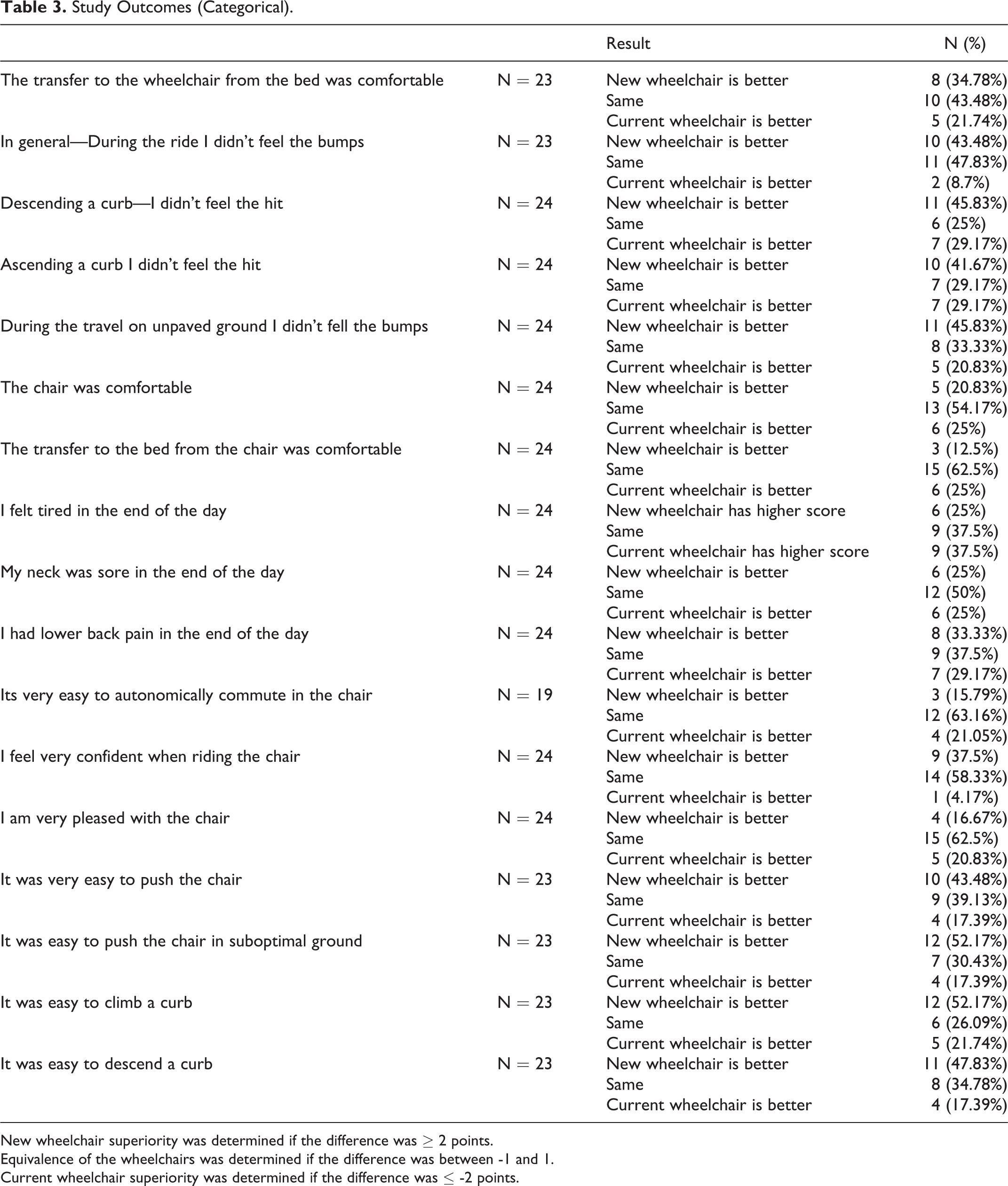
New wheelchair superiority was determined if the difference was ≥ 2 points.
Equivalence of the wheelchairs was determined if the difference was between -1 and 1.
Current wheelchair superiority was determined if the difference was ≤ -2 points.

In general—During the ride I didn’t feel the bumps.
I feel very confident when riding the chair.

It was easy to push the chair in suboptimal ground.

Stack comparison of comfort and sense of security.
Discussion
In this first-of-a-kind study, we tried to compare user experience with a wheelchair in a controlled environment. As user experience is subjective and may be influenced by different confounders, we tried to minimize the confounders by using the same chair for both wheels (the wheels were exchanged on day 3). The participants were taken on a daily trip using the same route consistently and at the same hours. The study was double-blinded and both the patient and caregiver did not know which wheel was installed.
We found statistically significant differences in the user experience between the 2 sets of wheels. When a participant reported that during the ride, they didn’t feel the bumps we can assume that the shock absorbers were active and absorbed the energy of the contusion releasing it slowly and gradually. Jianghong and Long 14 tested the comfort of a bus seat to provide recommendations to the manufacturer. Their results indicate that subjects were able to rate ride comfort reliably and could differentiate between seats. When a non-shock absorbing vehicle is used (bicycle, wheelchair, scooter etc.) each perturbation is transmitted to the user faster and the vibrations last for a longer period of time. In the case of a wheelchair the shockwave reaches the ischium and then the spine almost directly and the rider feels each and every obstacle, Hulshof and Zanten 15 reported a correlation between exposure to vibrations and an increase in developing low back pain. The ability of the shock absorbing wheels to effectively reduce the force transmitted to the user as well as the magnitude and duration of the vibrations might explain why the riders felt the bumps less but also why they felt more confident. Pope 16 examined the dynamic responses of individuals using 3 different cushion surfaces to establish a correlation between vehicle driving and low back pain. They found that soft cushions magnify the gain at the first natural frequency of the driver which amplifies the stress on the driver’s spine. As a wheelchair user commutes it is critical to be able to control the wheelchair safely. When the chair is felt to be more stable and not affected by every obstacle the patient reports higher confidence levels and hopefully that translates into a safer usage. DiGiovine and colleagues 6 reported that some subjects commented about feeling insecure when propelling a different wheelchair in a foreign environment. Other subjects indicated that they felt less secure in the test wheelchair than in their personal wheelchair, even when the test wheelchair was identical to their personal wheelchairs, they concluded that certain wheelchairs were rated higher than others for both ride comfort and ergonomics suggesting design and weight where translated into user experience.
Study Limitations
We recognize that the main fault of this study is the lack of a standardized and validated questionnaire regarding user experience with a wheelchair in the short period. To the best of our knowledge, there is no existing standardized, validated questionnaire for evaluation of user experience using a wheelchair (or any other assistive locomotive technology), most of the questionnaire was worded so that the higher the score the “better” the chair except for 3 questions, that might have confused the recruits. The second limitation is the small cohort size which was primarily due to the technical issues regarding the personnel required for the completion of the rides and follow-up.
Conclusion
The wheelchair equipped with shock absorbing technology provide better user experience in the immediate term than standard wheels. Further study is needed to assess the long-term implications. A lack of a standardized and validated questionnaire for evaluating user experience in a wheelchair hinders the possibility of further unified data collection and evaluation as well as asserting was is a valid MIC in such situation further study is necessary to formulate and validate such a questionnaire and establish the MIC.
Footnotes
Authors’ Note
The study was approved by the local ethical committee.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The trial was partially funded by the “Softwheel” Inc, Tel-Aviv, Israel. References