
Abstract
Background:
Known possible consequences of proximal humerus fractures include impaired shoulder function, decreased independence, and increased risk for mortality. The purpose of this report is to describe the survival and independence of elderly patients with fractures of the proximal humerus, treated in our institution, relative to patient characteristics and treatment method.
Methods:
Retrospective cohort study from 2006 to 2012.
Setting:
Community-based hospital with level 1 designation.
Patients/Participants:
Three hundred nineteen patients ≥60 years who presented to the emergency department with an isolated fracture of the proximal humerus were either admitted to the inpatient ward for the organization and provision of immediate definitive care or discharged with the expectation of coordination of their care as an outpatient. Treatment was nonoperative or operative.
Outcome Measures:
One- and 2-year mortality.
Results:
Significant predictors of mortality at 1 year included Charlson Comorbidity Index (CCI; continuous, hazard ratio [HR] = 1.40; 95% confidence interval [CI]: 1.06-1.86), body mass index (BMI; <25 vs ≥25; HR = 3.43; 95% CI: 1.45-8.14), and American Society of Anesthesiologists (ASA) disease severity score (3-4 vs 1-2; HR = 4.48; 95% CI: 1.21-16.55). In addition to CCI and BMI, reliance on a cane/walker/wheelchair at the time of fracture predicted mortality at 2 years (vs unassisted ambulation; HR = 3.13; 95% CI: 1.59-5.88). Although the Neer classification of fracture severity significantly correlated with inpatient admission (P < .001), it was not significantly associated with mortality or with loss of living or ambulatory independence. Among admitted patients, 64% were discharged to a facility with a higher level of care than their prefracture living facility. Twenty percent of study patients experienced a loss in ambulatory status by at least 1 level at 1 year postfracture.
Conclusion:
In a cohort of elderly patients with fractures of the proximal humerus, patient characteristics including comorbidities, ASA classification, and lower BMI were associated with increased mortality. Specifically, those admitted at the time of fracture and treated nonoperatively had the highest mortality rate and, likely, represent the frailest cohort. Those initially treated as outpatients and later treated operatively had the lowest mortality and, likely, represent the healthiest cohort. These data are inherently biased by prefracture comorbidities but help stratify our patients’ mortality risk at the time of injury.
Keywords
Introduction
Proximal humerus fractures are the third most common fracture in patients over the age of 65. 1 Historically, these patients have been considered to be more robust than patients with hip fractures but frailer than patients with distal radius fractures. 2–3 Although the incidence of these fractures is rising, only sparse literature addresses the significance of this injury in elderly individuals, especially in frail elderly individuals. 4
During previous decades, the implication of hip fractures on morbidity and mortality has been well studied and has also driven care. Examples of this effect include the development of hip fracture protocols that prescribe immediate full weight bearing, surgical repair within 48 hours, and the stratification of risk relative to age and comorbidities. 5 –10 In contrast to this work in hip fracture care, relatively little analogous data exist to help counsel elderly patients regarding survival or living independence following a fracture of the proximal humerus.
The primary aim of this study was to identify risk factors for mortality in elderly patients with proximal humeral fracture. Secondarily, we investigated correlates in patient characteristics and patient outcomes. Specifically, we examined mortality in elderly patients with isolated fractures of the proximal humerus in relation to patient factors including comorbid conditions, body mass index (BMI), hospital admission status, treatment method, level of discharge facility, and level of prefracture patient independence.
Patients and Methods
The research was performed at a community-based hospital with level 1 trauma center designation. By searching Current Procedural Terminology and International Classification of Diseases, Ninth Revision codes, we identified 648 patients aged ≥60 years with fractures of the proximal humerus, treated between 2006 and 2012. Eligible study patients were ≥60 years old with an isolated and unilateral fracture of the proximal humerus. Exclusion criteria included polytrauma patients, bilateral fractures, shoulder dislocations, and pathologic fractures. Admission, at the discretion of the emergency department (ED), orthopaedic, or medical attending physician, was typically secondary either to a degree of social or medical dependence or to plans for early operative intervention. Fracture care was at the discretion of the treating senior author (JAS).
Three hundred nineteen patients aged 60 and over with isolated fractures of the proximal humerus met the inclusion criteria. Data were collected retrospectively from the electronic medical records (EMRs). The information obtained included general patient demographics, admission status, treatment method, length of stay, discharge facility, prefracture level of independence, residence at 1-year postinjury, ambulatory status at 1-year postinjury, and mortality at 1-year and 2-year postinjury. Comorbidities were captured using the Charlson Comorbidity Index (CCI) and American Society of Anesthesiologists (ASA) score. Changes in living and ambulatory status were ranked as “worse” or “same or better” (Figure 1). Fractures were classified according to both Neer and Orthopedic Trauma Association (OTA) classification schemes. 11,12 Mortality was captured from the EMRs when documented or from Ancestry.com, if date of death was not recorded in the EMRs or if clinical activity was not documented beyond 2 years of fracture. Those not identified as deceased at 1-year or 2-year postinjury by the EMRs or Ancestry.com were assumed to be alive at that point. 13,14
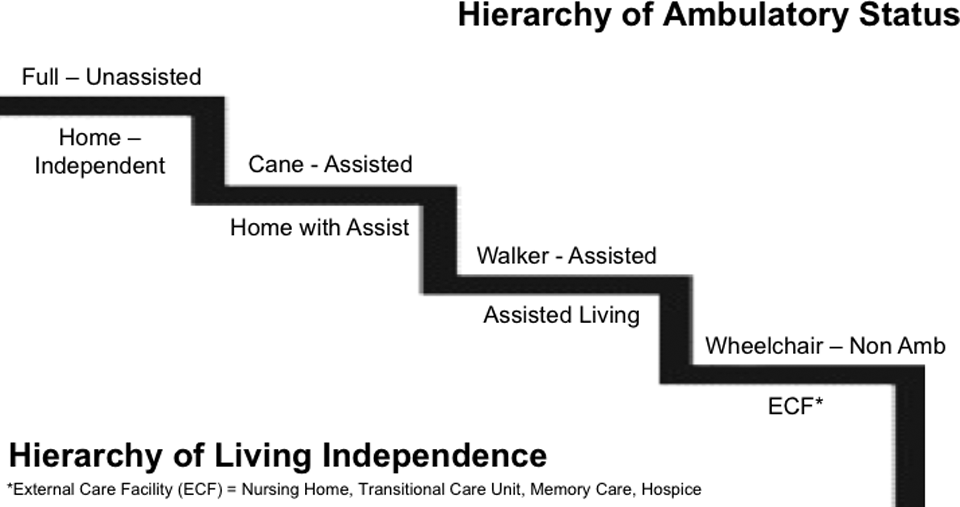
Illustration of ambulatory status and living independence levels.
Statistical Methods
Descriptive statistics were used to summarize the patient population as well as changes in living and ambulatory status pre- and postfracture. Cox proportional hazards regression analysis evaluated 1-year and 2-year mortality in relation to patient factors with results reported as hazard ratios (HRs) with 95% confidence intervals (CIs). For all other outcomes, we constructed multivariable generalized linear regression models to calculate β estimates (continuous outcomes) or odds ratios (ORs; binary outcomes). Independent variables for final adjusted models were chosen from a pool of a priori defined covariates using a stepwise selection algorithm. All statistical analyses were carried out with SAS (v9.4) software.
Results
A total of 319 patients, who were treated for fracture of the proximal humerus between January 2006 and April 2012, met study inclusion criteria. One hundred twenty-one (38%) were admitted as inpatients from the ED, while the remaining 198 were discharged from the ED. Patients in both groups were treated operatively and nonoperatively for their isolated proximal humerus fracture, as shown in Figure 2.

Study sample and clinical management.
The average age of the study cohort was 75 years (range: 60-97), and 76% were female. The majority of the patients (n = 196, 63%) were fully ambulatory (without assistance) prior to fracture and 72% (n = 227) lived independently in private homes without assistance. According to Neer classification, 35% of these patients were type 1, 52% were type 2, 9% were type 3, and 4% were type 4. According to the OTA classification, 57% were type A (extra-articular unifocal fracture), 35% were type B (extra-articular bifocal fracture), and 8% were type C (articular fracture). Due to incomplete radiographic records, 9 patients (3%) were not classified based on fracture type (Table 1).
Patient Demographics and 1-Year Mortality Stratified by Patient Characteristics.

A total of 109 patients (34%) were treated operatively, 61 were admitted directly from the ED. Forty-eight were discharged from the ED and scheduled to return for operative treatment. The mean length of stay for those admitted was 4.4 days (standard deviation [SD]: 3.1; range: 0-20). Of the 169 admitted patients, 163 had known discharge facility status. Of the 163 patients, 103 (63%) were discharged to a facility with a higher level of care than their prefracture living facility.
Pre- and postinjury ambulatory status were available for 280 (88%) of the 319 patients. A decrease in ambulatory independence (including death) at 1-year postfracture occurred in 57 patients (20%). Patients relying on a cane or walker for mobility at baseline had the highest proportion of decreased ambulatory status. Specifically, 41% of the individuals ambulating prefracture with a cane and 36% of the individuals ambulating with a walker lost at least 1 level of ambulatory status at final postfracture follow-up, while only 12% of individuals ambulating unassisted prefracture declined in ambulatory status at the final follow-up.
Death occurred in 27 patients (8%) within 1 year of clinical presentation and in 55 patients (17%) within 2 years. Prefracture unassisted ambulation and living independence were significant predictors of decreased mortality at 1 year, prior to covariate adjustment. Additional unadjusted correlates of mortality included older age, lower BMI, and comorbidities. Fracture classification status by either metric was not significantly associated with mortality (Table 2).
Baseline Characteristics by Survival Status at 1 Year.
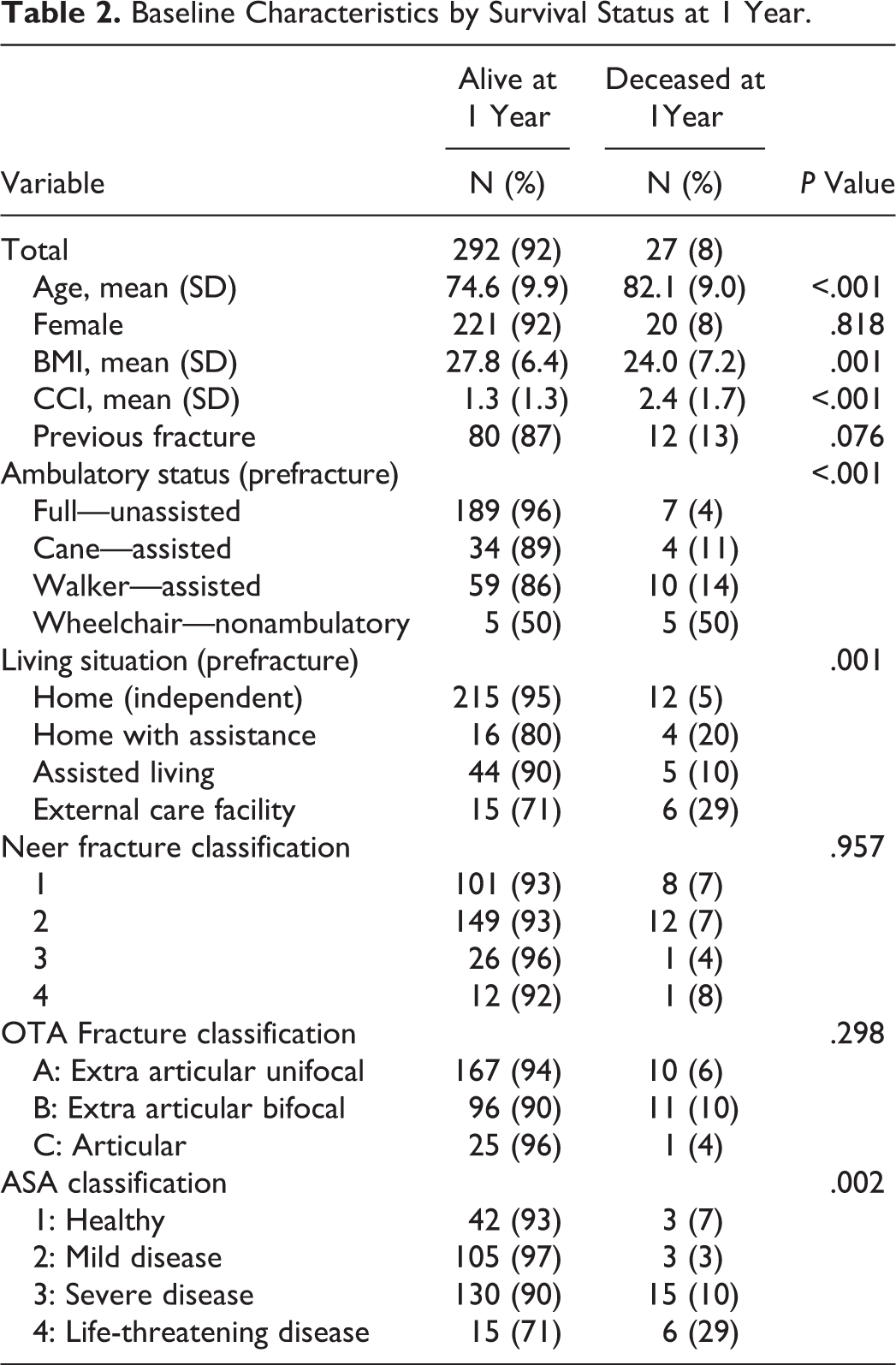
In an adjusted Cox regression model for survival at 1 year postfracture, variables representing patient frailty and/or comorbidity were predictive of mortality. Specifically, each 1-unit increase in CCI score was associated with a statistically significant 40% increase in the mortality rate (HR = 1.40; 95% CI: 1.06-1.86). Additionally, even after adjustment for CCI, an ASA disease severity score of 3 to 4 (severe disease) was significantly associated with a 4-fold increase in mortality rate (HR = 4.48; 95% CI: 1.21-16.55). Furthermore, BMI <25 (perhaps indicating frailty) was associated with a 3-fold increase in mortality rate (HR = 3.43; 95% CI: 1.45-8.14; Table 3).
Predictors of Patient Mortality within 1- and 2-Years of Humerus Fracture.
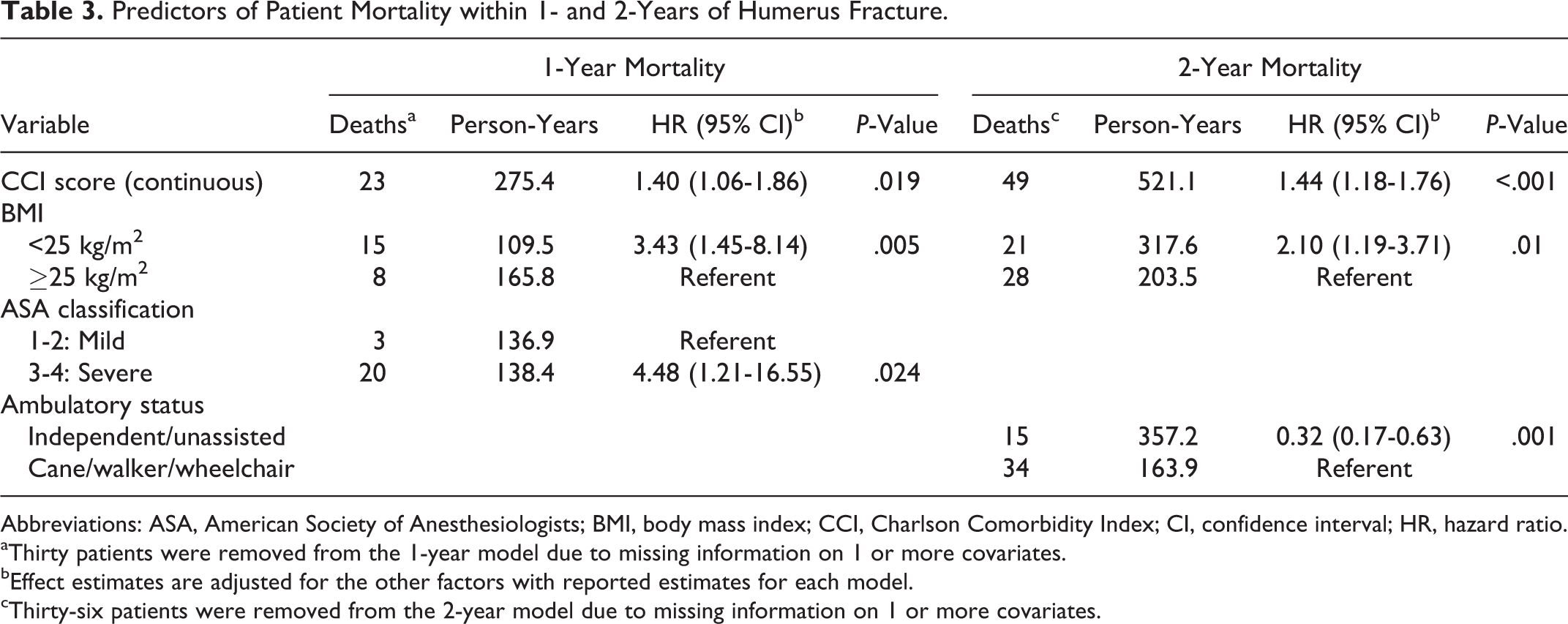
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; CCI, Charlson Comorbidity Index; CI, confidence interval; HR, hazard ratio.
aThirty patients were removed from the 1-year model due to missing information on 1 or more covariates.
bEffect estimates are adjusted for the other factors with reported estimates for each model.
cThirty-six patients were removed from the 2-year model due to missing information on 1 or more covariates.
Similarly, increasing CCI (HR = 1.44; 95% CI: 1.18-1.76) and BMI <25 kg/m2 (HR = 2.10; 95% CI: 1.19-3.71) were significant predictors of mortality at 2 years. The ASA classification was not a significant predictor of 2-year mortality in the adjusted model. However, full ambulatory status (unassisted) at baseline was protective for survival (HR = 0.32; 95% CI: 0.17-0.63), as compared to reliance on a cane, walker, or wheelchair (Table 3).
A Kaplan-Meier plot depicting survival at 1 year and 2 years by 4 categories of CCI is shown in Figure 3. A log-rank test for these survival trajectories (3 degrees of freedom) was statistically significant (P = .005).

Kaplan-Meier plot for 2-year survival by Charlson Comorbidity Index score category.
Finally, significant predictors of initial inpatient admission were Neer class (>1 vs 1; OR = 3.89; 95% CI: 2.14-7.04) and baseline ambulatory status (cane/walker/wheelchair vs full, OR = 3.17; 95% CI: 1.85-5.43). Patient factors associated with increased length of stay (in days) included CCI (continuous, β = 0.414; 95% CI: 0.096-0.733) and OTA class C (vs A/B, β = 1.376; 95% CI: 0.001-2.751). The parsimonious prediction model for likelihood of discharge to greater assistance included age (continuous, OR = 1.14; 95% CI: 1.08-1.21), reliance on a cane/walker/wheelchair at baseline (vs full ambulatory status, OR = 3.05; 95% CI: 1.19-7.81), length in days of inpatient stay (continuous, OR = 1.34; 95% CI: 1.10-1.63), and BMI (continuous, OR = 1.07; 95% CI: 1.00-1.15).
Discussion
The incidence of proximal humerus fractures in the elderly individuals is expected to triple over the next 30 years. 4 Many of these fractures will occur in individuals experiencing a declining health status. Therefore, further investigation into the effect of this injury is especially important in this population. To our knowledge, this is the first study of older patients with isolated proximal humerus fractures to correlate patient-specific characteristics such as CCI, BMI, prefracture living independence or ambulatory status with 1- and 2-year mortality as well as to 1-year outcomes of postfracture living independence and ambulatory status.
Our study population included 37% of individuals who required ambulation assistance or who were nonambulatory at the time of fracture (cane, walker, or wheelchair). This characteristic as well as living independence (28% requiring home care, assisted living, or skilled nursing) are likely predictors of the degree to which a proximal humerus fracture may be a sentinel event in the lives of these individuals. Court-Brown and McQueen previously described a series of patients with proximal humeral fractures. In this study cohort, 10% of patients were living at a care facility at the time of fracture. 3 The higher degree of dependence within our patient cohort (28% living in skilled nursing, assisted living, or with home assistance) provides an important opportunity to characterize outcomes in a frailer, elderly population (Table 1).
Olsson and Petersson stratified patients with proximal humerus fracture into those with no comorbidities, those with comorbidities, and those with severe illness. In their study, those with severe illness experienced a 40% mortality rate at 1 year, while those with fewer preexisting diseases had a mortality rate that was similar to sex and age-matched controls. 15 Similarly, in this report, we found that patient characteristics including comorbidities, ASA classification, and lower BMI were associated with increased mortality.
Interestingly, Neer and Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association (AO/OTA) fracture severity did not correlate with mortality in our study cohort. This lack of association may be due to the relative infrequency of OTA type C fractures (8%), Neer type 3 (9%), and Neer type 4 (4%) fractures in the setting of relatively low overall mortality (8% at 1 year and 17% at 2 years). 16 It is important to note that fracture severity did correlate with inpatient admission (initial and delayed). Length of stay was correlated with the loss of independent living at discharge and, perhaps, also serves as a surrogate for the overall injury severity or frailty. Early social work or case management should be prescribed for these patients. 17 –20
Center et al found that an incident fracture in an older cohort increases the risk of subsequent fracture for even up to 10 years postfracture, and Clinton et al found that proximal humerus fracture, in particular, predicts subsequent hip fracture (HR = 1.57), with the highest risk within 1 year. 21,22 This underlines the importance of fall risk evaluation and continued physical therapy as a means of fall prevention in these vulnerable patients. 23 Our patients experienced a drop in living and ambulatory independence postfracture. Of those patients living (with available data) at 1-year postinjury, we found that 20% (57/280) dropped at least 1 level of ambulatory independence and 17% (47/283) lost at least 1 level of living independence. While future investigations would ideally have a community control, to our knowledge this is the only study to show change in living and ambulatory independence following proximal humerus fractures.
Limitations of this investigation include its retrospective design that inherently allows bias in the study population. In spite of this, the data suggest that inpatient admission for this fracture, when at the discretion of the treatment team, may be a surrogate for frailty and/or comorbidity burden and, hence, mortality. Patient ASA score and CCI were used to account for premorbid differences between cohorts. This negates many of our associations with mortality but underscores the implication that admission decision, surgical decision, and mortality are all closely tied to physiologic frailty and comorbidities (CCI). These data allow us to describe mortality up to 2 years based on CCI at (0-1 or 2-7) at the time of injury (Figure 3). Although we searched the EMRs and Ancestry.com, it is theoretically possible that we considered patients to be alive at 2 years when they were in fact deceased. This situation could result in an underreporting of the actual mortality rate. Lastly, while ideal for this study, our community-based patient population may not be generalizable to all practices. Although there are inherent weaknesses of this retrospective cohort study, the goal was to appropriately describe our relatively large patient population but not to determine causality or to prognosticate.
Any fractures, including proximal humeral fractures, that occur in frail individuals are sentinel events that contribute to increased morbidity and mortality. In a cohort of elderly patients with fractures of the proximal humerus, patient characteristics including comorbidities, ASA classification, and lower BMI were associated with increased mortality, while operative intervention was associated with a lower 1- and 2-year mortality only when not accounting for comorbidities. Specifically, those admitted at the time of fracture and treated nonoperatively had the highest mortality rate and, likely, represent the frailest cohort. Those initially treated as outpatients and later treated operatively had the lowest mortality and, likely, represent the healthiest cohort. These data are inherently biased by prefracture comorbidities but help stratify our patients’ mortality risk at the time of injury.
Footnotes
Authors’ Note
Institutional review board approval was obtained to carry out this study. This work was presented in part at the International Geriatric Fracture Society Annual Meeting, Miami, Florida, on September 18, 2014. This work was also presented at the Minnesota Orthopedic Society Annual Meeting, Minneapolis, Minnesota, on May 8, 2015.
Acknowledgments
The authors would like to gratefully acknowledge the work of Lisa K. Schroder, BSME, MBA, and Logan Stuck, MS in the completion of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.