
Abstract
Introduction:
According to the expected demographical changes, the number of elderly trauma patients will increase exponentially over the next decades. Different models of an interdisciplinary orthogeriatric care have been developed. But there is only limited evaluation of their benefit without clear and evidence-based results. In 2011, we monitored the results of our orthogeriatric combined management by conducting a 1-year follow-up.
Methods:
We treated 231 patients presenting a proximal femoral fracture on our orthogeriatric ward. We obtained the epidemiological data and the geriatric assessments from all these patients. One year after discharge, we sent them a written questionnaire. Primary end points were the mortality and the functional outcome, measured by Barthel score, the requirement of care, and the residential status.
Results:
One hundred sixty-seven (72%) of the 231 patients completed the follow-up. The average age at admission was 81.5 years (70-99 years). The mortality rate was 2.4% during hospital stay and 31.4% after 1 year. The average Barthel score was 44 points at the time of admission, 55 points at discharge, and 72 points after 1 year. Forty-five percent of the patients were in requirement of care at the time of their admission. At the 1-year follow-up, 63% of the patients had some form of care, thus showing an increase of 18%. At the moment of the fracture, 77% of the patients were living in their own home and 23% in a nursing home. After 1 year, the surviving patients show nearly unchanged conditions (75% own home vs 25% nursing home). Eighty-six percent of the patients coming from their own home were able to continue living there independently.
Conclusion:
The orthogeriatric care is successful in reducing the short-time mortality without showing any effect on 1-year mortality. But the surviving patients seem to benefit from an improved functional outcome.
Keywords
Introduction
Proximal femoral fractures of the elderly people are typical, osteoporosis-associated, and so-called geriatric or fragility fractures. In our institution, they represent one-third of all inpatient treatments for patients older than 70 years. In most cases, fractures are caused by a low-energy trauma; nevertheless, the consequences are severe. Fragility fractures are accompanied by an increased rate of complications 1 and an excessive mortality (up to 35% after 1 year 2 ). The most serious concern is the loss of independence after the fracture and the subsequent requirement for care, 2 -6 resulting not only in medical but also in socioeconomic problems. 7
This situation will worsen over the next decades as the number of geriatric patients with those kinds of fractures is expected to increase rapidly. 8,9 There are prognoses estimating that the number of patients older than 80 years with proximal femoral fractures will double by 2050. 10
To cope with the problems, associated with those geriatric patients, different types of cooperations have been established between orthopedic trauma surgeons and geriatricians. Some also include other specialties such as anesthesiologists or physiotherapists.
11
The different models of cooperations differ in the grade of complexity and the intensity of collaboration: In some cooperation models, for example, the patients are transferred from the surgical ward as soon as possible (normally around the fourth postoperative day) to a specialized geriatric ward. In the “network-model,” during the entire length of their stay, the patients are treated on a regular trauma ward, while receiving additional treatment from a geriatrician composed of periodical ward rounds. The most complex degree of cooperation is represented by the “ward model”: Fragility fracture patients are transferred to a ward, providing a specialized setup and a multidisciplinary team of physicians, nurses, physiotherapists, and social workers during the whole stay. The daily ward round is performed together by the trauma surgeon and the geriatrician.
So far there is no survey comparing one of these models with regular treatment on surgical ward alone and showing an evident benefit, despite the additional effort and expenses. 12
In 2008, we started to establish a specialized geriatric trauma unit in our institution and increased their capacity step by step up to 44 beds, representing one-third of all trauma beds in the hospital.
In 2011, we monitored the results of the interdisciplinary treatment by conducting a 1-year follow-up study of all geriatric patients treated, including those having a proximal femoral fracture.
Materials and Methods
Since 2009, all trauma patients in our hospital who are older than 70 years and have typical geriatric comorbidities detected by a geriatric assessment (“fragility fracture patients”) are treated on a specialized orthogeriatric ward, representing the complex “ward model.” The patients are treated by a multidisciplinary team consisting of trauma surgeons, geriatricians, specially trained nurses, physiotherapists, ergotherapists, and social workers. Besides the daily interdisciplinary ward round, there are regular team meetings to discuss the therapeutic strategy for each patient. The patients receive activating care by the nurses and physiotherapy at least twice a day. The training is focused on the preservation of the activities of daily living (ADLs) and their independent mobility.
A standardized geriatric assessment is performed for each patient at the time of admission and at the time of discharge in order to uncover mental or physical deficits to be treated.
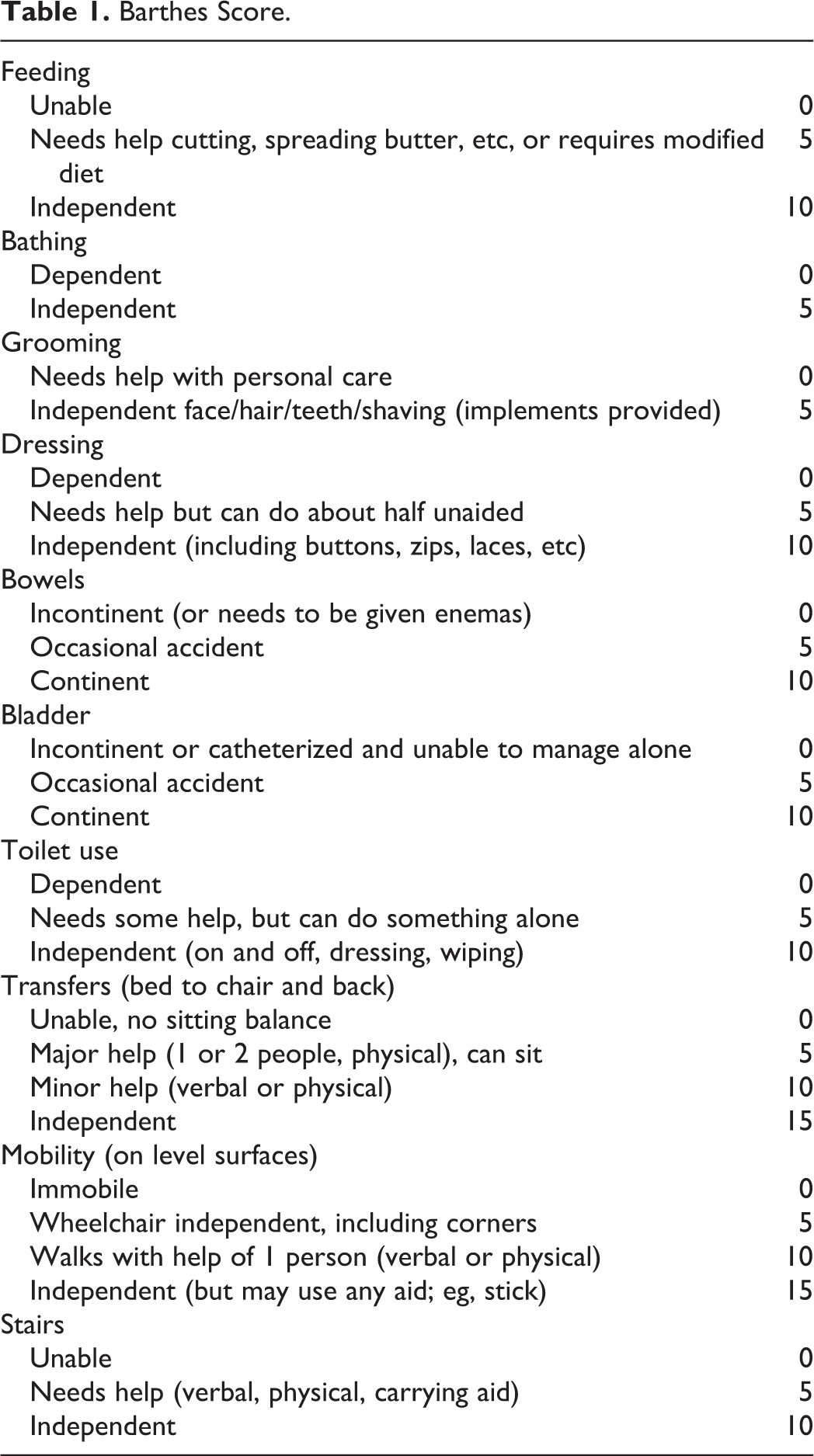
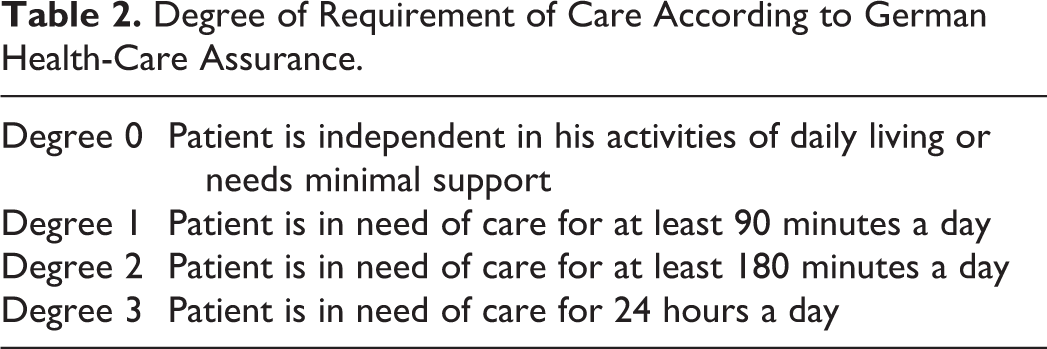
In 2011, all 231 patients with hip fractures (femoral neck and pertrochanteric fractures) treated on our geriatric trauma ward were enrolled in the follow-up study. The geriatric assessments (eg, Barthel score; Table 1), comorbidities, the course of treatment, living situation, and the requirement for care were all recorded. In the German health-care system, the degree of requirement for care is defined by the amount of time per day that a patient is dependent on professional help in his ADLs (Table 2) and is assigned by the health-care insurance. At a 1-year interval, all patients were asked to fill out a questionnaire about their current situation.
Barthes Score.
Degree of Requirement of Care According to German Health-Care Assurance.
The actual residential status, their requirement for care (Table 2), and Barthel score (Table 1) were all requested. In the case of a missing answer, 5 attempts to contact the patient, his relatives, or his general practitioner via telephone were done by 1 study nurse in order to complete the questionnaire.
The obtained data were also aligned with hospital documentation system. For the calculation of mortality rate, all proven events of death—via questionnaire or hospital documentation system—were included. Approval of the national ethic committee was obtained before starting the survey.
Results
We were able to obtain the complete data set of 167 (72%) of the 231 patients. The average age at admission was 81.5 years (70-99 years). We had 75% female and 25% male patients, and the mean length of hospitalization was 17.5 days (6-134 days).
Mortality
The mortality during the hospital stay was 2.4% and another 29% in the following year, resulting in an overall 1-year mortality rate of 31.4%.
Hospital Readmission
Within the first year, 26% of the patients had to be treated in the hospital again, 53% of those even several times. The reason for readmission was in 11% (that means 3% of all patients) a second fracture. In another 11% (3% of all patients), the readmission was a complication of the first fracture. One patient (0.6% of all patients) had to be treated because of persisting pain. Readmitted patients had the following complications: 2 implant failures (1.2% of all patients), 1 postoperative seroma, and 1 chronical infection (0.6% of all patients each). Seventy-eight percent of the readmissions were due to nonsurgical indications (see also Figure 1)

Reasons for readmission.
Functional Outcome
Barthel score
At the time of admission, the mean Barthel score was 44 (0-70) points. That score increased to 55 (0-90) points at the time of discharge and up to 72 (0-100) points after 1 year (Figure 2).

Changes of the Barthel score.
Requirement of care
Forty-five percent of the patients needed support in their ADLs before the hospitalization, of those 63% degree 1 (Table 2), 37% degree 2, and none of them degree 3. After 1 year, 63% of the patients needed support, of those 58% degree 1, 40% degree 2, and 2% degree 3. We saw an increase in the number of patients who needed support for the ADLs by 18%, without significant differences between the different degrees of requirement of care (see also Figure 3).
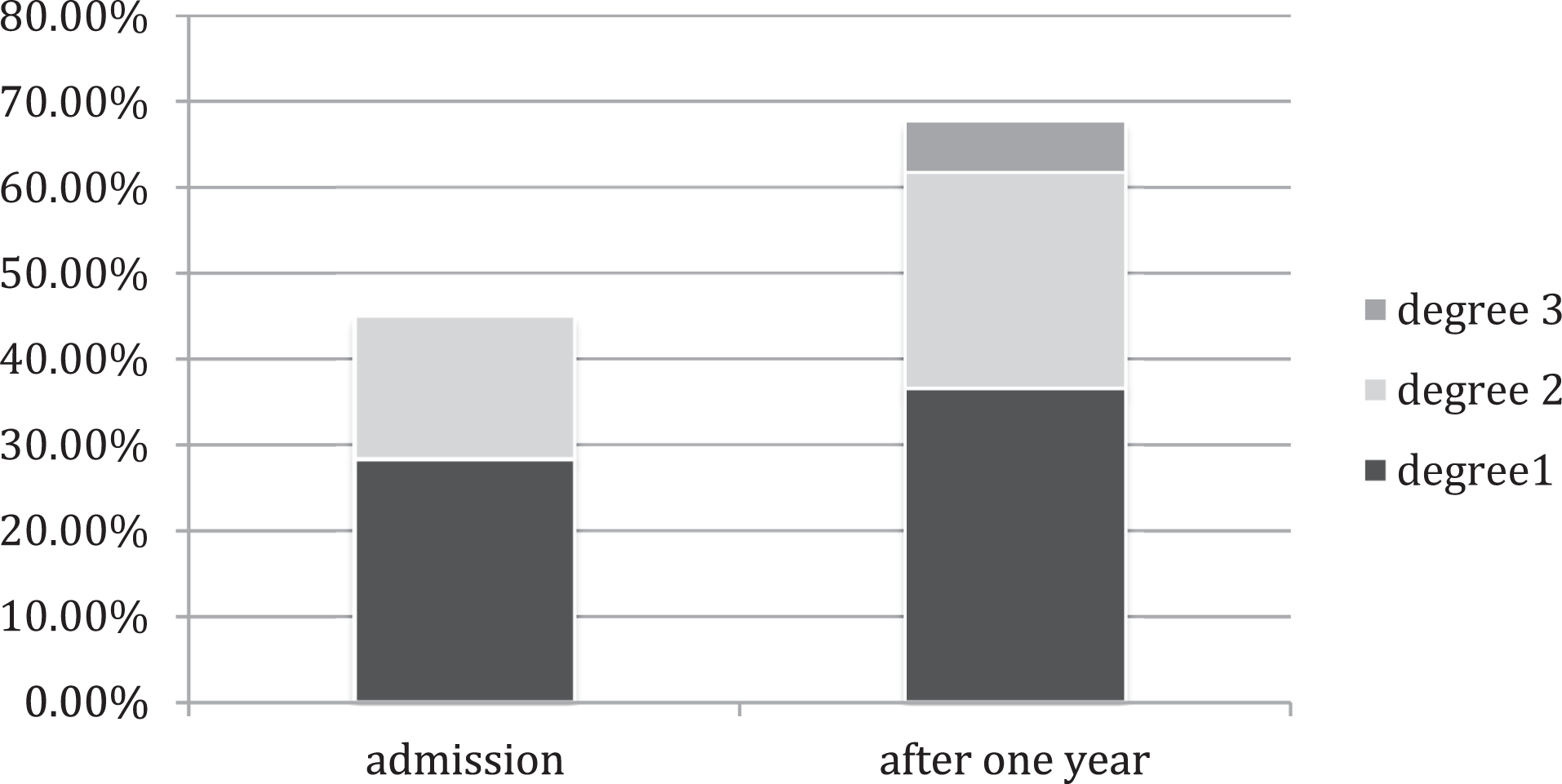
Degree of requirement of care at the time of admission and after 1 year.
Residential status
At the time of hospitalization, 77% of the patients lived in their own homes and 23% in a nursing home. After 1 year, 75% were still living in their own homes and 25% in a nursing home. Eighty-six percent of the patients who lived in their own homes prior to hospitalization remained there 1 year after the fracture (Figure 4).

Changes in the residential status.
Discussion
The goal of this study was to obtain the short- and long-term results of a specialized orthogeriatric treatment in a “ward model” for patients with proximal femoral fractures. Until today, there is no clear evidence for superiority in comparison with regular treatment 12 by trauma surgeons exclusively without support by geriatricians.
Considering the high average age of these geriatric patients and the kind of study based on a written questionnaire, the return rate of 72% is a satisfying result. We might have obtained a higher return rate by a face-to-face examination on our 1-year follow-up, but the required effort would have been unreasonably high. Due to privacy policy, we couldn’t gain access to health-care insurance or governmental data. Nevertheless, the loss to follow-up of 28% of all patients could influence the results as the mortality rate or the change in resident situation and requirement of care could be higher than reported.
We sent out a simple questionnaire with objectives and clear criteria (mortality: yes/no, degree of requirement of help according to the German health care’s insurance 0/1/2/3, living situation: own home/nursing home). In our opinion, high-quality data are able to be obtained via written questionnaire or telephone interview. However, for the Barthel score determination, there is a slight chance for inaccuracy when using those methods.
Another limitation of our follow-up is the absence of a control group with conventional treatment on a regular trauma unit without geriatric support. Unfortunately, we didn’t collect comparable data before implementing our orthogeriatric trauma unit. Since we are very convinced of the benefit of this interdisciplinary treatment, conducting a study with the conventional control group would not be ethical in our opinion and in our situation nearly unfeasible. Comparing our results with studies from other countries is not meaningful due to the different settings and different health-care systems. The mean age and the gender ratio in our study population are comparable to other studies on geriatric trauma patients. 5
The mean length of stay at the hospital for our patients was 17.5 days, which is 3 days longer than the mean stay for those kind of fractures in Germany 13 and twice as long as described by Suhm et al for a “network model” (8.6 days). 14 But contrary to many other orthogeriatric cooperation models, it was explicitly not our goal to reduce the length of stay. In fact, Suhm et al 14 could show recently that an orthogeriatric combined managed care using a “network model” is able to reduce the length of stay (8.6 vs 11.3 days) without influencing the mortality or the functional outcome in a negative way. This is a remarkable result and, from the economic point of view, certainly an interesting approach. As we know the inherently pure functional outcome after femoral fractures in the elderly patients, 2 we don’t want to content ourselves with maintaining this low level. In our opinion, a prolonged length of stay is reasonable, if the patient benefits from a better functional outcome, if the society benefits from reduced consequential costs, or if at the best the patients and society both do benefit. Therefore, our aim is the best functional outcome for the patient to protect him or her from loss of independency and to enable him or her to return to his previous living situation.
Mortality
In the 2 years before implementation (2006 and 2007), the in-house mortality for this special group of patients was 3.6% and 5.4% in our hospital. Regarding the prolonged length of stay, the in-house mortality in our study of 2.4% is very low, also compared to rates twice as high in other studies with a similar group of patients. 13,15,16 Despite that the 1-year mortality is comparable to other studies based on conventional treatment. 2,5,17 -19 Other studies regarding orthogeriatric multidisciplinary treatment 11,14,18,20,21 show similar results without significant reduction in the long-time mortality rate. Also, a meta-analysis in 2013 12 couldn’t show a significantly reduced long-term mortality rate by the use of interdisciplinary treatment. Despite the different multidisciplinary orthogeriatric approaches for patients with proximal femoral fractures over the last few years, the overall mortality rate stayed nearly the same. 22,23 Nevertheless, this could be interpreted as an improvement, since the mean age of the patients increased over the same period. The proximal femoral fracture of the elderly people seems to be a more complex and multifactorial entity or consequence of a multifactorial than an isolated disease pattern. Therefore, even an optimized medical treatment for 2 weeks in a geriatric trauma unit is not able to reduce the long-term mortality. According to those findings, other “fragility fractures” such as osteoporosis-associated fractures of the vertebral column also go along with an increased mortality rate. 4 The fact that almost 80% of the readmission in our study occurred due to other medical problems and only 10% due to complications of the surgery underlines the role of the multimorbidity in those patients.
Functional Outcome
The Barthel score could be improved during the hospital stay. One year after discharge, the patients achieved an average score of 72 of 100 points. Of course, one shouldn’t jump to conclusions by this abstract number, but with this result, one can assume a high degree of independency and ability to handle activities of daily life.
Because of the different assessments, the difficulty of measurement, and the small number of studies, 11,12 it is very difficult to compare our results to other studies. Nevertheless, it seems that an orthogeriatric multidisciplinary treatment, especially in a “ward model,” is able to achieve a better functional outcome, even if the results have not always shown statistical significance so far. 19,21,24 -26 But recently, a prospective, randomized trial 27 comparing orthogeriatric and usual orthopedic care after hip fractures in elderly people could show statistically significant better functional outcome after 4 and 12 months (measured by Short Physical Performance Battery and Instrumental ADLs) for the orthogeriatric group.
It is important to note the small increase in the number of patients in requirement of care, with only 18% in our study. An investigation of German health-care insurance data 5 including almost 8000 patients of a comparable cohort with hip fracture showed in contrast an increase in requirement of care after 1 year in every second patient. Besides the benefit for the patient, this could be a significant financial benefit for the health-care system and possibly help finance the additional costs of such a orthogeriatric cooperation, especially under the described “ward model” conditions. For the Norwegian health-care system, such an effect could be proven recently. 27
In the end, all those questions are rather unimportant for the patients themselves, since each patient is much more interested in whether he can keep his independent living situation and whether he is able to perform all his ADLs without further support. To reach this goal, a good functional outcome is an indispensable necessity. In this context, the high percentage of patients still able to live in their own homes after 1 year is very encouraging. It is remarkable that only 14% of the patients coming from their own home have to move into a nursing home after the fracture.
As mentioned before, there are not many studies about the long-term effects of hip fractures in the elderly patients, but there is one study with 1000 patients which investigated the living situation of patients after a conventional treatment of a femoral fracture. 28 Their study population was comparable to ours but showed a significantly smaller number of patients still living in their own homes 1 year after surgery (65% vs 75%). Table 3 summarizes some of the results in comparison with existing data.
Comparison of Our Results to Previous Data.

Conclusion
Despite some limitations of our study due to the lack of comparison data before implementation of our orthogeriatric comanagement and a loss to follow-up of 28%, we could achieve very promising results in accordance with the existing literature. Due to the orthogeriatric multidisciplinary treatment in a “ward model,” we were able to reduce the in-house mortality rate but not the 1-year mortality rate compared to our preimplementation status and existing surveys. 2,17 -19,21 The existing data are indicating that the patients do benefit from an orthogeriatric management with regard to their functional outcomes, measured by Barthel score, the requirement for care, and the living situation; after 1 year, the patients achieve an average Barthel score of 72 of 100 points and the percentage of patients in requirement of care increases only by 18%. Eighty-six percent of the patients coming from their own home are able to still live there independently.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was conducted with financial sponsorship by DePuy Synthes.