
Abstract
Background:
Expenditures for postacute care in total joint arthroplasty (TJA) have risen dramatically over recent decades. Therefore, efforts are underway to better identify cost savings in postacute rehabilitation centers, such as skilled nursing facilities (SNFs). The primary purpose of this study was to analyze gait training achievements in post-TJA patients in the interval between hospital discharge and the patients’ first 4 days at the SNF. Identification of potential losses in therapeutic progress may lead the way for improved patient care, outcomes, and cost savings. Our hypothesis is that patients discharged to an SNF will have a decline in gait achievements upon transfer from the hospital.
Methods:
A total of 68 patients who underwent TJA were included. The total distance ambulated during physical therapy (PT) was recorded for the last day of hospital therapy and the first 4 days at the SNF as well as the reported visual analog scale (VAS) pain scores.
Results:
There was a 73% decline in distance ambulated on SNF day 0 (Hospital: 138.6 ft vs SNF: 37.9 ft; P < .001) and a 50% decline on SNF day 1 (Hospital: 103.0 ft; SNF vs 51.1 ft; P < .001) compared to the last hospital session. There were no significant differences in distance walked on SNF days 3 and 4 relative to the last hospital session. The VAS pain scores did not significantly differ on SNF days 0 and 1 compared to the last hospital day but began to significantly decline on SNF day 3 (Hospital: 4.9; SNF: 3.3; P = .02) and day 4 (Hospital: 3.9; SNF: 2.3; P = .03).
Conclusion:
There was a significant decline in ambulatory proficiency in post-TJA patients on the day of and the day following hospital discharge to an SNF. These deficits cannot be attributed to heightened pain levels. Early and progressive ambulation is a recognized component of appropriate PT following TJA. This study therefore highlights the transition from hospital to SNF as a crucial and novel target for improvement in post-TJA care.
Keywords
Introduction
Total hip and knee replacements have proven to substantially improve quality of life in patients with hip and knee osteoarthritis. 1 Recent growth in patient demand for joint arthroplasty, attributed largely to an aging population with comorbidities, has heralded a surge in the number of total joint replacements performed annually. 2 The numbers of total hip and knee replacements are conservatively projected to increase over 2-fold and 6-fold, respectively, by 2030. 2,3 Concordantly, there has been a growing clinical interest in determining the optimal rehabilitation setting for postacute care for total joint arthroplasty (TJA) patients. 4 –8 However, there remains no definitive evidence to favor rehabilitation in a skilled nursing facility (SNF) over inpatient rehabilitation facilities, home health care, or outpatient settings. 2,9,10
Traditionally, patients who undergo TJA are admitted to the hospital after surgery and initiate a postoperative physical therapy (PT) regimen. After achieving functional and systemic stability, they are discharged home with or without home health care or to an extended care facility such as an SNF or inpatient rehabilitation facility. However, few measures are in place to ensure continuous and intensive PT during the transition from hospital to SNF. During this period, patients may be susceptible to significant losses in functional performance commensurate with their change in care and management.
Numerous publications affirm the need for early, rapid, and continuous mobilization with weight bearing in the postoperative period. 11 –14 Such measures promote joint viability, decrease risk of deep vein thrombosis, and protect long-term rehabilitation outcome. This concern is accentuated in patients destined for an SNF, as they tend to be older and have increased comorbidities, less favorable American Society of Anesthesiologists (ASA) physical classification scores, and lower preoperative functional performance scores than patients discharged to home. 15,16 Furthermore, patients who attend SNFs experience higher rates of hospital readmission than their counterparts who are discharged home or to an inpatient rehabilitation facility. 17,18 The SNF-bound patients therefore represent a vulnerable population, which merits additional study.
Given the relative uncertainty in postacute care outcomes, we sought to measure ambulatory achievements and subjective pain levels for post-TJA patients during the immediate interval following discharge from the hospital. The presence of discrepancies in PT achievements between hospital discharge and admission to the SNF may compromise long-term rehabilitation and therefore may serve as a crucial and novel target for improvement in post-TJA care. Our hypothesis is that patients discharged to an SNF following TJA will have a decrease in ambulatory achievements.
Methods
This study used a retrospective design that included patients who underwent TJA at our institution between November 2012 and July 2014. Patients were included in this study if they were discharged to an SNF following primary or revision total hip or knee replacement surgery. The study was approved by our Institutional Review Board.
Corresponding patient demographics and operative measures were obtained from hospital records and included gender, age, height, weight, insurance company, marital status, living status (with someone or alone), preoperative diagnosis, ASA physical status, and type of surgery. Patients were excluded from review if they had any immediate surgical complications. The following postoperative recovery and inpatient PT measures were also obtained: daily visual analog scale (VAS) pain scores, distance ambulated, weight-bearing status at discharge, and total length of stay (LOS) in the hospital.
We subsequently requested each patient’s medical file from his or her respective SNF. The following elements were abstracted from the patient’s SNF chart: daily VAS pain scores, distance ambulated during PT sessions, and total LOS in the SNF. Patients were excluded from the analysis if (1) their SNF file did not include PT evaluation notes, daily progress notes for the first week, or discharge summaries and (2) the patient left the SNF within the first 4 days at the SNF.
One hundred and thirty two patients were discharged from the hospital to an SNF during the study time period. After exclusion, the final study sample included 68 patients from 31 different sites. The majority of excluded cases were due to the lack of documentation at the SNF site. Forty-two of these patients underwent total knee arthroplasty (TKA) and 26 underwent total hip arthroplasty (THA).
Statistical Analysis
A 2-tailed paired t test was used to compare the distance ambulated by the patient and VAS pain scores at the time of hospital discharge versus days 0 to 3 after admission to the SNF. “Day 0” is defined as the day of hospital discharge and the day of admission to the SNF, “day 1” represents the day after hospital discharge (first full day at the SNF), and so on. Only a few patients had complete gait and pain records for each and every 1 of the 4 SNF days analyzed in this study. As a result, we conducted separate t tests for each day the patients were at the SNF and excluded patients from an analysis if they were missing data. For instance, a patient who had complete records for SNF days 0, 1, and 3 but lacked gait data on SNF day 2 was excluded from the analysis comparing ambulation in the hospital versus SNF day 2. However, the same patient would be included in the analysis comparing ambulation in the hospital versus SNF day 0. In addition, a secondary analysis was conducted to compare the percentage of difference in ambulation between hospital and SNF in TKA and THA subgroups. Bonferroni correction (α = .05/κ) was used to account for multiple comparisons in the primary study outcome. Data were analyzed using Microsoft Excel 2013 (Microsoft Corporation, Redmond, WA, USA).
Results
Table 1 describes the clinical, sociodemographic, and intraoperative characteristics of the patients included in this study. The average LOS at the hospital and SNF were 2.9 days (standard deviation [SD] ± 0.6) and 17.5 days (SD ± 13.8), respectively. Of the 68 patients included in this study, 20 (29.4%) began gait training at the SNF on the same day they were discharged from the hospital (day 0), usually as a component of their initial PT assessment. In contrast, 43 (63.2%) patients began gait training on day 1, and 5 (7.4%) began gait training on day 2.
Preoperative and Intraoperative Characteristics for Patients Discharged to an SNF Following TJA.
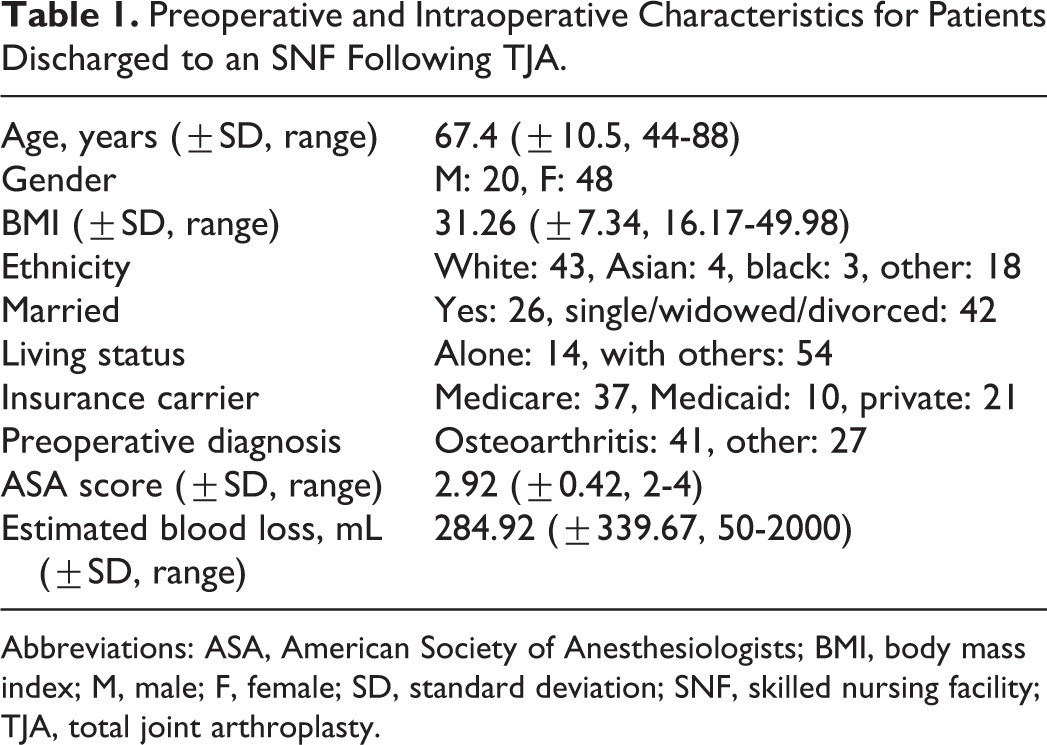
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; M, male; F, female; SD, standard deviation; SNF, skilled nursing facility; TJA, total joint arthroplasty.
Primary Outcome: Gait Training
Because of inconsistencies in data reporting between SNFs, very few patients had complete records of gait training for every single day of the first 4 days following admission to the SNF. Twenty-four (35.3%) of the patients had records of a single PT session at the SNF, 16 (23.5%) had records of 2 sessions, 26 (38.2%) had records of 3 sessions, and 2 (2.9%) had records of all 4 sessions. As previously discussed, we conducted serial paired t tests after matching patients based on their available data. Overall, there was a statistically significant reduction in the distance walked between the patients’ last recorded hospital PT session prior to hospital discharge and the distance walked at the SNF on days 0 and 1 (Table 2). These results are displayed graphically in Figure 1. Those who walked on SNF day 0 experienced a 73% decline (Hospital: 138.6 feet vs SNF: 37.9 ft; P < .001) in distance ambulated compared to their last hospital PT session. Similarly, a 50% decline (Hospital: 103 ft vs SNF: 51.1 ft; P < .001) in distance ambulated was observed in patients who underwent gait training on SNF day 1. There were no statistically significant differences in distance ambulated on SNF days 3 and 4 compared to the last hospital PT session. Similar trends were observed when patients were subdivided into TKA and THA groups. The TKA patients had a 79% decline (Hospital: 167.2 ft vs SNF: 35 ft; P = .003) in distance walked on SNF day 0 and a 53% decline (Hospital: 106.4 ft vs SNF: 50.6 ft; P < .001) on SNF day 1 compared to their last hospital PT session. On the other hand, the THA patients had a 58% decline (Hospital: 99.4 ft vs SNF: 41.9 ft; P = .003) on SNF day 0 and a 47% decline (Hospital: 95.9 ft vs SNF: 50.5 ft; P < .001) on SNF day 1 compared to their last hospital PT session.
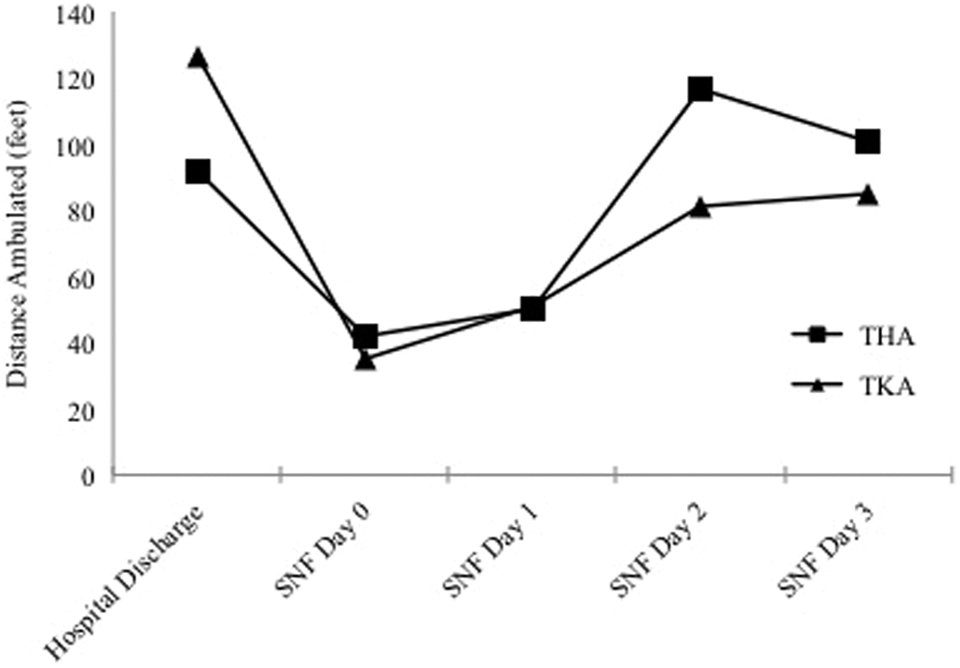
Average distance ambulated (feet) in THA and TKA patients following hospital discharge. SNF, skilled nursing facility; THA, total hip arthroplasty; TKA, total knee arthroplasty.
Distance Ambulated (Feet) and Percent Difference of Gait between Last Hospital PT Session and SNF Days 0 to 3.
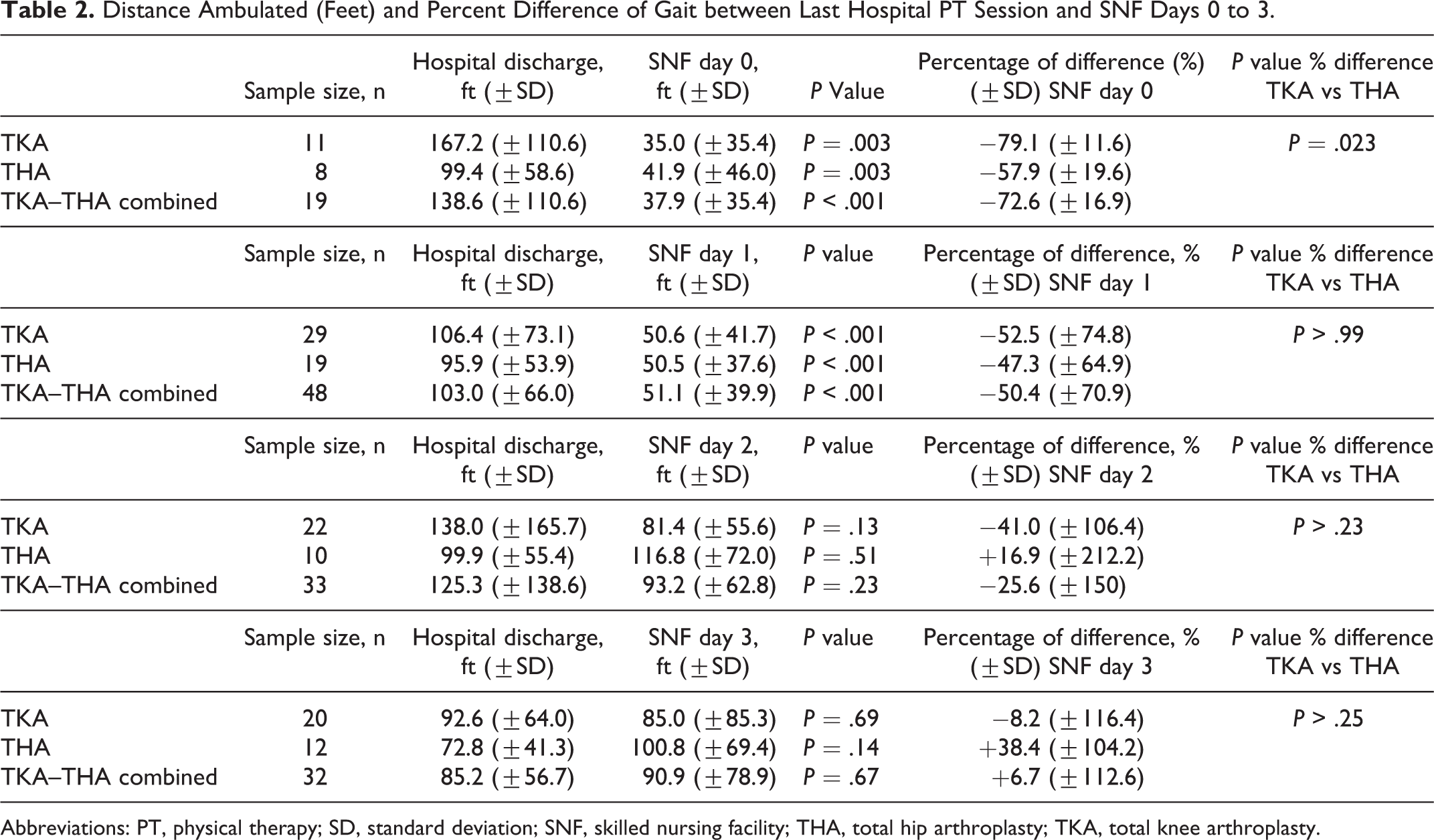
Abbreviations: PT, physical therapy; SD, standard deviation; SNF, skilled nursing facility; THA, total hip arthroplasty; TKA, total knee arthroplasty.
The percentage of differences in distance ambulated between hospital discharge and SNF days 0 to 3 were then calculated for TKA and THA subgroups (Table 2). It was found that, on day 0, the TKA group had a significantly greater decline in distance walked compared with the THA group (TKA: 79.1% vs THA: 57.9%; P = .023). However, on days 1 to 3, the TKA and THA groups did not significantly differ with respect to the proportion of decline in ambulation compared to their last hospital PT session.
We also sought to determine whether the timing of the last hospital PT session had an effect on distance ambulated on SNF day 0. There was no significant difference in the percentage of decline in distance walked between patients whose last hospital PT session was conducted the day before hospital discharge versus the day of hospital discharge (Table 3).
Effect of Last Hospital PT Session Timing on Decline in Ambulation on SNF Day 0.

Abbreviations: PT, physical therapy; SD, standard deviation; SNF, skilled nursing facility; THA, total hip arthroplasty; TKA, total knee arthroplasty.
Secondary Outcome: VAS Pain Scores
A similar analysis was conducted on VAS scores reported by patients in the days following discharge from the hospital. There were no statistically significant differences in VAS pain scores reported on SNF days 0 and 1 when compared to VAS scores reported in the hospital on the day of the hospital discharge (Table 4). However, the average VAS score was significantly lower on SNF day 2 (Hospital: 4.9 vs SNF: 3.3; P = .02) and SNF day 3 (Hospital: 3.9 vs SNF: 2.3; P = .03) compared to the hospital discharge day and SNF days 0 and 1.
Combined TKA–THA VAS Scores for Pain (of 10) During the First 4 Days Following Admission to SNF.

Abbreviations: SD, standard deviation; SNF, skilled nursing facility; THA, total hip arthroplasty; TKA, total knee arthroplasty; VAS, visual analog scale.
Discussion
Patient discharge to SNFs has garnered increasing attention as a source for improvement in both patient care and health care costs. This study approached the transition from hospital to SNF as a potential point of care during which patients lose ambulatory proficiency, which may lead to an increased LOS at the SNF and delayed return to function. We found in our study that there was a significant decline in gait achievements, as measured in ambulation distance, during the PT session on the day of and the day after the patients were transferred to an SNF. It was also noteworthy that, compared to the distance ambulated on the last hospital PT session, patients did not significantly improve on their gait training over the first 4 days at the SNF.
We considered the possibility that added pain during the transition to the SNF may have contributed to the functional decline. However, there were no significant differences in VAS pain scores between pain levels on the day of hospital discharge and the first 2 days at the SNF. There are a number of patient-sided factors that could have instead contributed to the decline in function, such as weariness from travel, lack of trust in the new SNF providers or institution, or a delay in acclimation to the new environment. Further work should be focused on these adjustable variables.
Nearly 30% of the patients in this study began gait training on the same day they arrived to the SNF, many of whom had also undergone PT at the hospital earlier that day. However, this study demonstrated no significant difference between ambulation performance for patients who conducted hospital PT on the day of hospital discharge and the day before hospital discharge. Therefore, same-day fatigue was not a major factor in the decline of performance seen at the SNF.
The functional loss demonstrated in this study could have a lasting impact on patient outcomes. First, it is widely believed that early and progressive ambulation is an integral part of a patient’s recovery from TJA. Pua and Ong demonstrated that even 1 day earlier ambulation in post-TKA patients was associated with reduced hospital LOS, improved knee function, and lower hospitalization costs. 14 Moreover, psychoemotional status is an important aspect to rehabilitating among post-TJA patients. 19 A halt in therapeutic progress may cause patients to be dissatisfied with their progress and lead to a lack of motivation in their rehabilitation.
Our findings are consistent with existing questions regarding the efficacy of rehabilitation in SNFs. DeJong et al 20 demonstrated that patients at SNFs participate in less intensive PT and had longer LOS than their counterparts at inpatient rehabilitation facilities. Similarly, Walsh and Herbold 21 reported that SNF patients had less favorable functional performance measures at discharge, including ambulation achievements, need for assistive devices, and stair negotiation, compared to patients at inpatient rehabilitation facilities.
There were several limitations in this study. First, there was a widespread variation in data reporting between different community SNFs. Many of the SNFs in this study documented daily gait achievements in compliance with the payer’s requisites, leaving many patients with incomplete gait training records. Implicit biases in data recording practices may therefore have had an effect on the results of this study. Second, our data collection did not extend beyond the first 4 days at the SNF. Therefore, this study did not define at what point patients began to significantly improve beyond hospital discharge. Future studies may seek to identify this moment in order to quantify the exact “time lost” post-discharge. Finally, this study utilized ambulation as a measure of therapeutic progress, which does not comprehensively reflect the patient’s functional capacity. However, there are as yet no universally accepted classification tools with which to characterize a patient’s holistic functional status. 22
Over the past 2 decades, there has been an across-the-board decline in length of hospital stay after TJA with a disproportionate rise in the use of postacute care resources and facilities, including SNFs. 23 The cost of postacute care represented the fastest growing spending category by Medicare between 1994 and 2009, accounting for approximately 73% of growth in expenditures for hip fractures. 24 In 2011, almost one-quarter of hospitalized Medicare beneficiaries were discharged to an SNF. 25 Spending in postacute care is therefore now considered the “next frontier” in health care savings and efficiency. This study identified a 4-day period during which post-TJA patients made no significant progress in their ambulatory function compared to their achievements on the day of hospital discharge. Poor ambulation during this time period may engender false expectations about the patient’s physical capacity and long-term potential at the SNF. Therefore, such deficits in therapeutic progress could potentially serve as an antecedent to longer SNF stays, reduced functional outcomes and patient satisfaction, and increased hospital readmissions.
Conclusion
Significant evolutions in the application of TJA for the treatment of osteoarthritis have simultaneously prompted the need for better and more cost-effective postacute care for patients undergoing TJA. This retrospective analysis of functional achievements in post-TJA patients has demonstrated a significant decline in ambulation following admission to the SNF compared to hospital discharge. This decline was proportionally worse for TKA patients than for THA patients. There were no significant differences in subjective pain levels during the 2 days following hospital discharge to account for the reduction in gait training achievements. Efforts to improve patient care and cost in TJA should aim to better understand the dynamics of PT following hospital discharge and admission to the SNF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.